CC7 - Fluency - Chapter 10 (Assessment of Preschool Children Who Stutter) & Chapter 11 (Assessment of School Age Children, Adolescents, and Adults Who Stutter)
1/55
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
56 Terms
Clinical Questions
Stuttering or normal disfluency?
If stuttering, what are the disfluencies like in various situations, and how does it change over time?
What are the child’s responses? Emotions?
What are the family’s concerns, expectations, etc.?
Treatment options—none, waiting, indirect, direct?
Language, articulation, and voice age appropriate?
Any issues for which referral needed?
Initial Contact
Usually on telephone
Listen carefully and respond to level of concern
Make appointment as appropriate
Provide suggestions to give parents useful ways to start helping child
Video Recording
Helpful to get video of child speaking spontaneously at home
Five to ten minutes of parents playing with child is usually adequate, unless stuttering is highly variable, in which case, more than one sample may be needed
Provides important sampling of stuttering that may be worse at home than at clinic
Parents can leave camera on stand for several days to get child used to it before filming
Parent-Child Interaction
Done first to get unbiased sample
Opportunity to observe child’s stuttering and awareness of it
Opportunity to observe parent’s style of interacting with child
What are key elements to observe?
Video record for later analysis
Parent Interview #1
Interview with child present or not—what are the pros and cons of each?
Begin with open-ended questions about what parents’ concerns are
Careful, nonjudgmental listening is important
Leave time at end of parents’ questions
Get a sense whether parents blame themselves for the child’s stuttering. Explore this. At an appropriate time during the interview, let them know the latest scientific information about possible etiology of stuttering.
Parent Interview #2
Gather information about
Child’s birth and development
Family history (stuttering and other disorders)
Onset of stuttering and changes over time
Child’s awareness and response to his stuttering
Parents’ response to child’s stuttering; their ideas about the cause
Previous treatment
Child’s personality and environment
Parents’ questions
Clinician-Child Interaction #1
Opportunity to observe child’s stuttering and his response to various stimuli
If child is quite fluent, clinician may speak rapidly and ask many questions to see if stuttering appears
If child is stuttering, clinician may experiment with fluency facilitating interaction, such as speaking slowly
If child is aware, discuss with parents the benefit of talking to child about stuttering.
Clinician-Child Interaction #2
Clinician can ask child if he ever gets stuck on words or has trouble talking. Should be done very acceptingly
Children usually relieved by open, reassuring discussion of stuttering
If child is reluctant to talk or play with clinician, it’s important not to push; clinician can play with an appealing toy and talk to self, and eventually child may join.
Speech Sample Analysis #1
Obtain sample from home and sample from clinic—at least 200 (300 if possible) syllables each
General observations to make from sample:
Frequency of disfluency
Types of disfluency
Nature of repetitions, prolongations, and blocks
Starting and sustaining airflow and phonation
Physical concomitants • Word avoidances
Speech Sample Analysis #2
SSI-4: Assess child’s severity (see Chapter 8)
Speech rate: syllables per minute (see Chapter 8)
Feelings and attitudes
Ask parents
Observe child’s reactions to his stuttering
Talk to child directly about his stuttering
Feelings and attitudes can range from being totally unaware to highly frustrated and afraid
May change from time to time.
Feelings and Attitudes #1
Obtain information about the child’s feelings and attitudes from the case history, parent interview, and my own interactions with the child
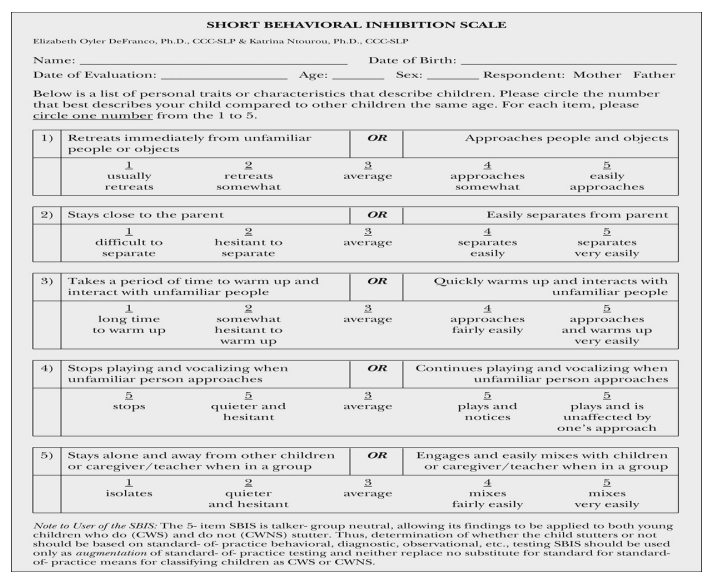
The Impact of Stuttering on Preschoolers and Parents questionnaire
However, if the child shows signs of struggle and tension when they stutter, or if the parents indicate that the child is aware through various examples of their frustration with their stuttering, I explore with the child their feelings about getting stuck on words
Feelings and Attitudes #2
Assessment of the feelings and attitudes can determine whether the child:
Is unaware of their disfluencies
Is occasionally aware of them and, even then, is seldom and only transiently bothered by them
Is aware and frustrated by them
Is highly aware, frustrated, and afraid of them
In addition, the questionnaire for parents described earlier in this chapter and shown in Figure 10.3—SBIS (Ntourou et al., 2020)—can be used to learn about how sensitive the child is.
Short Behavioral Inhibition Scale
Other Speech and Language Behaviors
Parents reports and observations of child’s speech and language may reveal other problems
Formal tests for phonological or language problems may indicate need for treatment concurrent with or following stuttering treatment
Compare syntax with vocabulary scores; disparity may be of concern
Also observe speech-motor and other fine motor skills
Hoarse voice may indicate laryngeal tension associated with stuttering.
Other Factors
Physical development
Cognitive development
Social-emotional development
Speech and language environment
Determining a Diagnosis, Prognosis, and Planning Treatment
Typical disfluency: greater than 10 disfluencies per 100 words; multisyllable word and phrase repetitions; greater than 3 iterations in reps that are slow and regular temple; child unaware
Borderline: more than 10 disfluencies per 100 words; part-word and whole-word repetitions; more than two iterations in many repetitions; little or no tension; minimal awareness of stuttering
Beginning: tension and hurry in stuttering; awareness and frustration; escape behaviors; possibly some avoidance
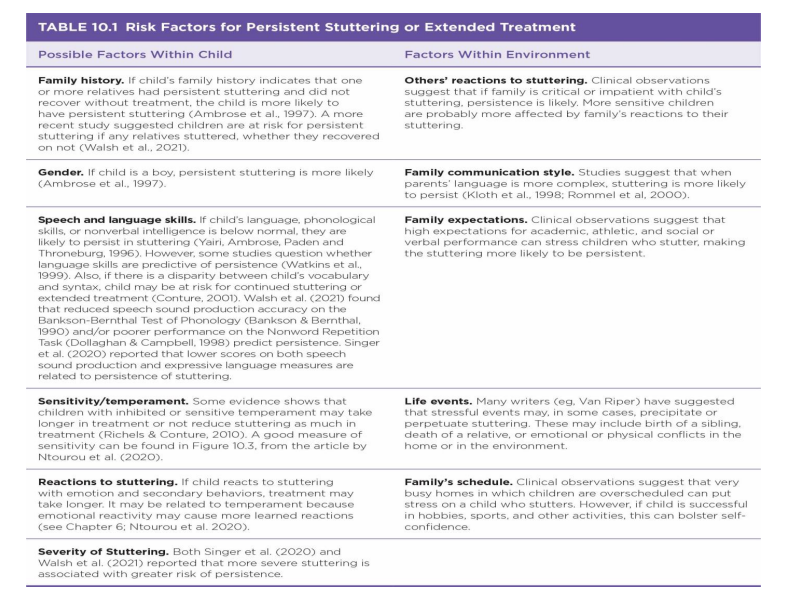
Risk Factors for Persistent Stuttering
Factors that may be associated with persistence of stuttering:
Stuttering does not decrease during 12 months after onset.
Stutterer is male.
Relatives who have not recovered from stuttering
Below-average nonverbal intelligence scores
Sensitive temperament.
Risk Factors for Persistent Stuttering or Extended Treatment
Closing Interview: Recommendations and Follow-up #1
Some information is available for closing interview: for example, home video, case history and interview, observations of child’s stuttering
Other information will be available later for report: for example, analysis of clinic video
Need to develop hypothesis about:
Child’s current developmental/treatment level
Important risk factors
Treatment approach
Closing Interview: Recommendations and Follow-up #2
Describe positive aspects of child and parents’ response to stuttering
Describe stuttering in appropriate, clear terms
Discuss treatment options
Respond to questions and implied concerns
Possible to give family a brief description of your findings that you compose just before the closing interview (see next slide for an example)
Closing Interview: Recommendations and Follow-up #3
It may be helpful to give family a brief description of your findings when you do the closing interview
A full report will be sent to them in a few days, but an immediate description of findings may give them something to take away, think about, and share with others.
Recommendations: Typical Disfluency
Give information about normal disfluency
If parents are concerned, set up another appointment in several weeks to reevaluate if disfluency persists or worsens
If needed, recommend changes in environment that may help all children: for example, turn-taking, careful listening, appropriate speech rates
Recommendations: Borderline or Beginning Stuttering
Use risk factors and duration of stuttering since onset to determine if treatment should be direct or indirect
Teach parents to use severity rating (SR) scale and have them begin to use it
Borderline (usually younger preschool children):
Discuss option of indirect treatment or watchful waiting
Provide video Stuttering and the Preschool Child or link to videos on Stuttering Foundation website
Have parents share weekly results of SR scale
Recommendations: Borderline or Beginning Stuttering
Beginning (usually older preschool children)
Discuss indirect versus direct treatment
Have parents begin to use SR scale and share with you on a weekly basis
For both levels: answer questions and provide contact information so parents can stay in touch if needed before next appointment
Clinical Questions
What are characteristics of student’s stuttering?
What are student’s feelings and attitudes about speaking?
How does it affect him at school and home?
Is he eligible for services, according to state regulations?
Public School Considerations
Individuals with Disabilities Education Act (IDEA) and state laws set procedures for evaluation and treatment of students who stutter
When child is referred for stuttering, SLP makes discreet observation in classroom; confers with teacher and special education administrator
Child’s parents are contacted, permission for an evaluation is obtained, and evaluation is carried out
Team of SLP, teacher, special education administrator, and parents discuss treatment options
Initial Contact With Parents #1
In school setting, call to get permission to evaluate child
Describe how student was identified and what characteristics of student’s stuttering are
Let parent know school’s desire to help student become a more effective communicator
Find out if family has noticed stuttering
Maintain a caring, accepting attitude
Explain evaluation process
Ask them to fill out a case history form
Try to obtain a video from home (may be more effective to wait until SLP obtains permission from child)
Initial Contact With Parents #2
In clinic setting, a telephone call to the family can let them know what to expect in the evaluation
Let them know you’ll be sending a case history and perhaps other forms to complete
May be helpful to talk to the student on the phone to describe the procedures and obtain permission for a home video
Case History Form
Important information:
Changes in stuttering since onset
Student’s own reaction and family’s reaction to stuttering
Past treatment
Impact of stuttering on school performance
Video recording may be more stuttering at home or school than in clinic, so this is an important sample
Parent-Child Interview
Observe the student’s speech with his parents while they are involved in an activity that promotes speech, such as how their favorite sports team is doing or describing a book or movie that they liked
Video record this with the participants’ permission for later analyses and then pay close attention to both the student’s stuttering behaviors and the parents’ responses and interaction style.
Parent Interview
Let parents know you support them and their child
Fill in gaps from case history (see section on areas to discuss with parents of preschool child)
Ask about how stuttering affects student in school (eg, participating, teasing, teacher responses, etc.)
Try to determine if there are factors that would hinder recovery (eg, parent’s anxiety or negative attitude about stuttering, student’s sensitivity, motivation, etc.)
Convey acceptance of family; comment on positive things they have done
Teacher Interview
Make an alliance with the teacher
Find out about child’s communication in class, if stuttering interferes with communication, how teacher responds to child’s stuttering, and if other children tease child about his stuttering
What information might you want to give to the teacher about stuttering?
Classroom observation
Arrange a time with teacher to unobtrusively observe student when he may be talking in class
Note how much he talks, to what extent he avoids, and how others react to his stuttering.
Student Interview
Get to know student first—his likes, dislikes, family, etc.
Discuss stuttering in a direct but accepting manner
Make sure child experiences you as interested in him and accepting and curious about his stuttering
Explore when he stutters the most, least
What he does when he stutters (have him teach you)
His feelings about his speaking
Others’ reactions, teasing, parents’ responses
Avoidances.
Speech Sample #1
Preliminaries
Ask student’s permission to video record
Record 300 to 400 syllables of student’s conversation (10 minutes)
Obtain 200-syllable reading sample
Offline: analysis of disfluencies; observe degree of tension, struggle, escape, avoidance; and estimate developmental/treatment level
SSI-4
Speech rate: compare with normal for age
Trial Therapy #1
Have student catch clinician’s pretend stutters
Have student put in pretend (or real) stutters, and have clinician catch student and reward him
Have student control length of clinician’s pretend stutters (eg, by having student squeeze fist and keep clinician in stutter as long as student is squeezing fist)
Roles reverse, and clinician signals student to make stutter longer and end it slowly and loosely (much reward when student is able to do this!)
Can student hold onto stutter, reduce tension, and release stutter slowly with clinician’s coaching? On his own?
Feelings and Attitudes
Methods of assessing:
Informally by observation and discussion with student
Informally with materials (eg, “worry ladder” from workbook by Chmela & Reardon, 2001)
Use formal assessment with discussion: CAT or A-19 and/or OASES for schoolage children
Other Speech and Language Disorders
Observe articulation and language; test if needed
Physical: Are there motor problems? Delay?
Cognitive: Learning disability? Attention/activity problem? Intelligence?
Social-emotional: Able to make friends? Highly sensitive or anxious?
Academic adjustment: Academic performance problems? Reading problems?
Diagnosis and Closing Interview
Developmental/treatment level
Factors influencing persistence
Closing interview in clinical setting
Begin with positive aspects of child and family
Be clear and direct when describing level of stuttering and implications for treatment
Address family’s concerns about student’s future
Discuss treatment options including family’s role
Public School Setting
After evaluation, clinician writes brief report in lay terms
Report should discuss affective, behavioral, and cognitive aspects of student’s stuttering and school performance
IEP team meets to consider the severity of child’s stuttering and its impact on education including extracurricular activities
Does student participate fully in school activities, or does stuttering limit him or her?
Can student meet school’s curriculum objectives, especially those related to speaking?
If IEP team determines child is eligible, measurable goals and short-term objectives are developed
Services to meet these goals and objectives are determined.
Preassessment #1
Clinic versus school assessment
This evaluation described as though it is in a clinic
When evaluation is in school, IEP process is followed
IEP process gets input from students when they are 14 or older and eventually involves not only school-based treatment but transition plans as well
Adolescents in school can fill out themselves with help from parents.
Preassessment #2
Attitude questionnaires
Sent to client several weeks before evaluation so they can be analyzed prior to interview
Typically used: S-24, SSRSS, Locus of Control, OASES
Also send “Personal Aims for the Stuttering Treatment” form AV recording
Crucial to have recordings from out of clinic; best if difficult situation, like talking on the phone
Analyze prior to evaluation.
Interview/Conversation
Learn about adolescent’s strengths and interests
Begin by letting client know what will take place in the evaluation
Ask open-ended question like “Why don’t you begin by telling me about your stuttering?”
After client has finished an initial description of concerns, ask about onset, development, and early experiences
How would you elicit this information?
Ask about current stuttering and how it affects social, occupational, and academic situations
Explore feelings—use results of questionnaires (S-24, etc.) as a basis to explore further
Explore client’s awareness of current stuttering including escape and avoidance behaviors
Does client have questions?
Speech Sample #2
Use video recording of client talking about a familiar topic such as school of work, 300 syllables or more
Reading sample at appropriate level
Also sample from outside clinic; if none available, record client making a phone call
Analyze with SSI-4
Speech rate
Pattern of stuttering
Trial Therapy #2
Have client freeze a moment of stuttering, maintaining posture and tension; client should get sound flowing even with posture stopped
This may require some coaching, especially on stop sounds
Have client become aware and describe what he’s doing as he stutters
Show your accepting curiosity as you help child feel what he’s doing as he stutters
Trial Therapy #3
Have client stay in posture and become comfortable in the posture with sound flowing, via your coaching
When client is comfortable, tension will reduce
Then client should finish the word loosely and slowly
See if client can do this (staying in stutter and releasing slowly) on his or her own after some clinician-guided practice
Interview: Family of Adolescent
Convey sincere acceptance of family’s viewpoint and concerns
Give family opportunity to express their concerns and emotions and to get their view of the adolescent’s stuttering
Give some time for adolescent to express views and feelings privately
In closing interview with adolescent and family, give principle role in treatment to adolescent, but involve family as much as adolescent is comfortable with
Diagnosis
Determine if this is “developmental” stuttering rather than normal disfluency, cluttering, neurogenic, or psychogenic stuttering
How do you differentiate these?
Intermediate stuttering
Younger than age 14
Blocks, repetitions, and prolongations
Escape and avoidance behaviors
Negative attitudes about speaking
Advanced stuttering
14 years or older
Symptoms as above but more entrenched
Closing Interview
Focus on positive aspects first
Describe stuttering behaviors, feelings, and attitudes, and provide explanation as far as possible
Describe therapy options, and give recommendations
Provide client with assignments to start
Set up next appointment if appropriate.
Preassessment #3
Case history form sent to adults several weeks prior to evaluation
Attitude questionnaires
Sent to client several weeks before evaluation so they can be analyzed prior to interview
Typically used: S-24, SSRSS, Locus of Control, OASES
Also send “Personal Aims for the Stuttering Treatment” form which is available in Chapter 9
AV recording
Crucial to have recordings from out of clinic; best if difficult situation, like talking on the phone
Analyze prior to evaluation.
Interview
Begin by letting client know what will take place in the evaluation
Ask open-ended question like “Why don’t you begin by telling me about your stuttering?”
After client has finished an initial description of concerns, ask about onset, development, and early experiences
How would you elicit this information?
Ask about current stuttering and how it affects social, occupational, and academic situations
Explore feelings—use results of questionnaires (S-24, etc.) as a basis to explore further
Explore client’s awareness of current stuttering including escape and avoidance behaviors
Does client have questions?
Speech Sample
Use video recording of client talking about a familiar topic such as school of work, 300 syllables or more
Reading sample at appropriate level
Also sample from outside clinic; if none available, record client making a phone call
Analyze with SSI-4
Speech rate
Pattern of stuttering
Trial Therapy #4
Have client freeze a moment of stuttering, maintaining posture and tension; client should get sound flowing even with posture stopped
This may require some coaching, especially on stop sounds
Have client become aware and describe what he’s doing as he stutters
Show your accepting curiosity as you help child feel what he’s doing as he stutters
Trial Therapy #5
Have client stay in posture and become comfortable in the posture with sound flowing, via your coaching
When client is comfortable, tension will reduce
Then client should finish the word loosely and slowly
See if client can do this (staying in stutter and releasing slowly) on his or her own after some clinician-guided practice
Other Speech and Language Behaviors
Informally screen or formally assess language, articulation, voice
Screen hearing
Other factors
Intelligence
Psychological and vocational adjustment
Diagnosis
Determine if this is “developmental” stuttering rather than normal disfluency, cluttering, neurogenic, or psychogenic stuttering
Determine what treatment level is appropriate
Advanced stuttering
14 years or older
Symptoms as above but more entrenched
Closing Interview
Focus on positive aspects first
Describe stuttering behaviors, feelings, and attitudes, and provide explanation as far as possible
Describe therapy options, and give recommendations
Provide client with assignments to start
Set up next appointment if appropriate.