Test #2: Intubation in Dogs and Cats:
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
Intubation Definition:
placement of flexible plastic tube into trachea to maintain an open airway or to serve as a conduit through which to administer certain drugs
Benefits of Intubation:
assist in maintaining open airways
prevents aspiration of saliva or regurgitated gastic contents
seals respiratory system and breathing circuit
Indication of Intubation:
respiratory and cardiac arrest
general anesthesia
heavy sedation
any procedure or disease that compromises the airway
endotracheal washes
decreased level of consciousness
periodontal therapy
upper airway obstructions
Intubation Equipment:
3-12 mL syringe to inflate cuff
endotracheal tubes in varying sizes
gauze squares
laryngoscope
oxygen
sterile lubricant
supplies to secure endotracheal tube
Types of Endotracheal Tubes:
Material:
Silicone
Red Rubber
Polyvinyl Chloride (PVC)
Types:
Plain/uncuffed
Cuffed
Types of Endotracheal Tubes: Plain: Cole
cuffed ET tube <3.0mm
besst choice: avians, pediatric animals or exotic pets
birds must complete tracheal rings— cuffed ET can lead to pressure necrosis if cuff is inflated too much
excellent pressure flow, provides less resistance
shoulders form an airtight seal at the entrace to larynx
Types of Endotracheal Tubes: Cuffed:
used in all species
2 purposes:
prevent gas leaks around the tube'
to reduce risk of aspiration of gastric and oral secretions
2 types:
high pressure, low volume
high volume, low pressure: less damage to tracheal mucosa
Cuffed ET Tubes: Murphy
most common
oval opening (murphy eye) across from bevel of tube
Murphy Eye: emergency opening if the distal end of lumen of tube becomes clogged
Cuffed ET Tubes: Magill
does NOT have the murphy eye but similar otherwise
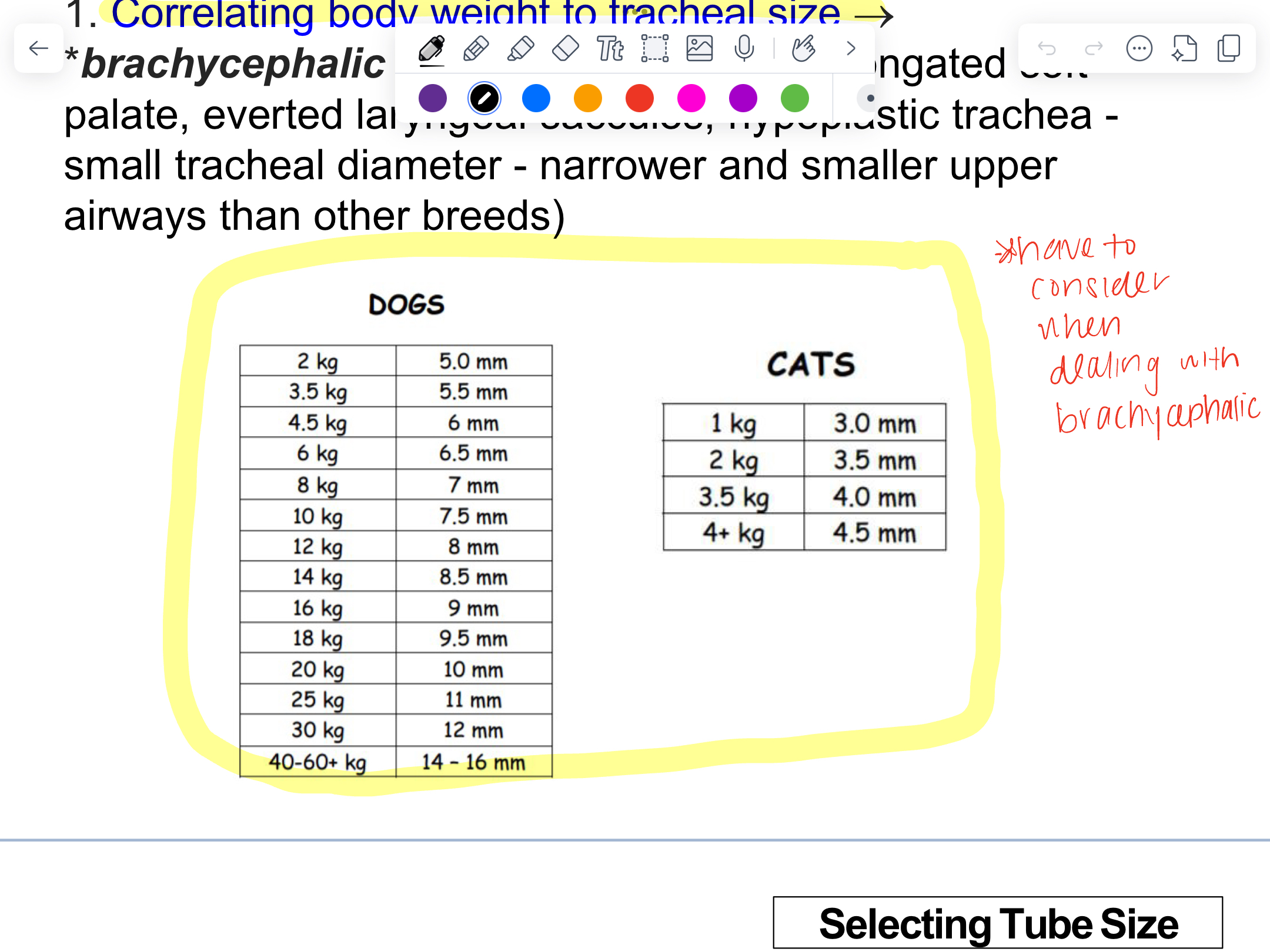
Selecting Tube Size:
rapid intubation
minimize tracheal trauma
ensure that airway is appropriately protexted
too large: airway trauma
too small: leaks around the cuff/airway protection be compromised
always choose 3 tubes
Selecting Tube Size: Correlating Body Weight tp Tracheal Size
brachycephalic breeds have smaller tracheal diameter, narrower and smaller upper airways than other breeds
Selecting Tube Size: Evaulating Width of Nasal Septum:
ET tube should be held up to narrowest point between the nares
21% effective
Selecting Tube Size: Palpation of the Width of Extra Thoracic Trachea Just Above Thoracic Inlet
46% effective
Selecting Tube Size: Proximal End & Distal End
proximal end: not extend past the incisor teeth
distal end": not extend past point of shoulder
Stylets:
in cases of smaller or extremely flexible ET tubes
provides support to faciliate intubation
cats with laryngospasm
ensure tip of stylet does not protrude beyond tip pf ET tube to minimize injury to the larynx and trachea
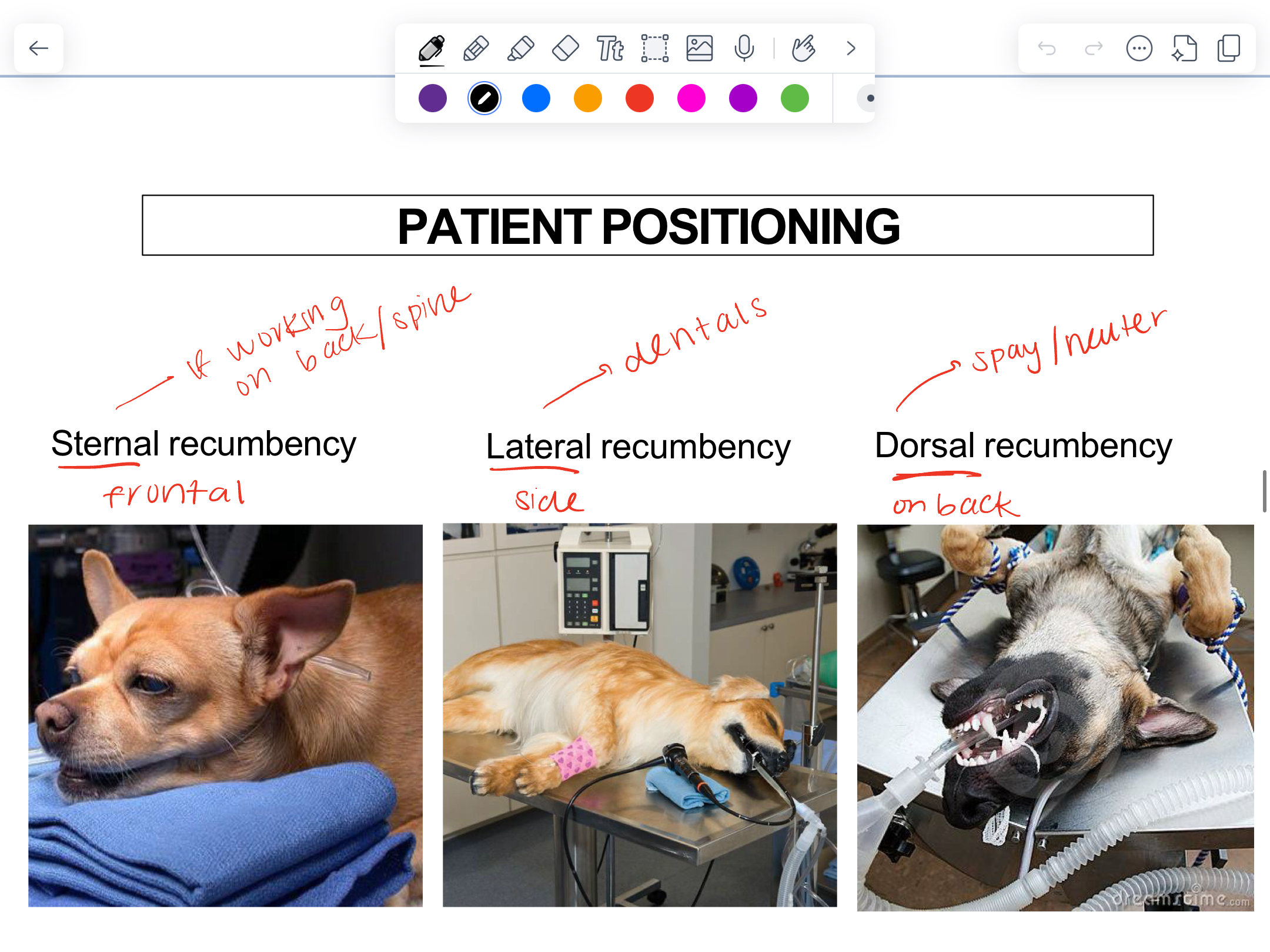
Patient Positioning:
Procedure in Cats:
same as dogs
laryngospasm: arytenoids to remain closed
use 1 drop of 2% lidocaine into each arytenoid
cats sensitive to lidocaine
Techniques to Confirm Tracheal Intubation:
Visual Confirmation: ET tube passing between arytenoids only definitibe way of confirming correct placement
Cough: ET tube is advanced into trachea
Condensation: clear tube on exhalation— air movement
Palpation of the Ventral Cervical Region: should reveal one rigid structure
Monitoring Under Anesthesia:
Circulation
electrocardiography (ECG)
oscillometric blood pressure measurement
Ventilation:
Capnography: measurement of CO2 in patient’s exhaled breath
Oxygenation:
pulse oximetry
Body Temperature:
thermometer
Depth of Anesthesia:
anesthetic gas analyzer
Extubation:
ONLY after confirmation that the pharyngeal reflex is reestablished
Before:
Check—- excessice secretions; aspirate
Cuff should be fully deflated
After:
Monitored
Head: be kept elevated to avoid aspiration from regurgitation
Flow-by O2 should be administered
Respiration and oxygenation should be monitored until animal fully awake
Types of Injections:
Injections can be delivered into:
Muscle (IM)
Tissue under skin (SQ)
Veins (IV)
Skin (Intradermal)
Body Cavities: abdominal cavity or thoracic cavity
Bone (intraosseous)
Most Common:
SQ
IM
IV