Midterm 2 - Developmental Psychopathology
1/159
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
160 Terms
Covert Conduct Problem
The more interpersonal manifestations of aggression related to conduct problems
rises till adolescence (These problems see highest peaks in early adolescence → not to say younger children can’t present just less normal)
heritability estimate lower than overt
Covert Conduct Problem Examples
lying, stealing, substance abuse, truancy (skipping school)
Overt Conduct Problem
The often physical manifestations of aggression related to conduct problems. "more observable and noticeable"
peaks early, recedes after preschool (early, toddler/preschool, peaks in early childhood, as children get older it decreases)
higher heritability than covert
Overt Conduct Problem Examples
physical aggression, argues, temper tantrums
Conduct Problems (Definition)
Age-inappropriate actions and attitudes of a child that violate family expectations,societal norms, and the personal or property rights of others
Dimensional Approach to Conduct Problems
Measuring: aggression on a spectrum
Overt vs covert debate
Aggression categorized in relational vs physical or reactive vs proactive
Categorical Approach to Conduct Problems
Diagnosably: ODD, Antisocial Personality Disorder; NOT threshold of symptoms like dimensional approach
May use categorical approach to give diagnosis, but use continuous/dimensional approach to assess specific symptoms
**Both approaches coexist**
Physical subtype of aggression
Behavioral subtype of aggression, generally more present in boys
Presentation of physical subtype of aggression
hitting, pushing, or kicking
Relational subtype of aggression
Social subtype of aggression, more prevalent in girls, boys tend to have high levels of both → but girls in general higher level
Presentation of relational subtype of aggression
tell other kids that they won't like them or be their friends just to hurt them or get their own way
heritability differences in covert vs overt
Genetics play a stronger role in explaining the variability in overt conduct problems
Proactive Aggression
Conscious and planned act, used for personal gain or egocentric motives. Also known as "premeditated", "instrumental" aggression
presentations of proactive aggression
"Used force to obtain money or things from others", "Yelled at others so that they would do things for you", "Vandalized something for fun"
Reactive aggression
An emotionally charged response to provocations or frustration. Also known as "impulsive", "affective" aggression
presentations of reactive aggression
"Become angry or mad when you do not get your way",
"Damaged things because you felt mad",
"Hit others to defend yourself"
Oppositional Defiant Disorder
a pattern of angry/irritable mood, argumentative/defiant behavior, or vindictiveness
Requirements for diagnosis of ODD
Behavioral pattern exhibited for at least 6 months as evidenced by at least 4 symptoms
exhibited during interaction with at least one individual who is not a sibling
Causes impairments (flashcard 19)
Differential diagnoses ruled out
Impairments of ODD
behavioral disturbance is associated with distress in the individuals or others, or negatively impacts child's functioning
Categories of symptoms in ODD
1) Angry irritable Mood
2) Argumentative/Defiant Behavior
3) Vindictiveness (revengeful)
Angry/Irritable Mood (ODD Symptom)
Often loses temper
Is often touchy or easily annoyed
Is often angry and resentful
Argumentative/Defiant Behavior (ODD Symptom)
Often argues with authority figures or adults
Often actively defies or refuses to comply with requests from authority figures or with rules
Often deliberately annoys others
Often blames others for his/her mistakes/misbehavior
Vindictiveness (revengeful)
Has been spiteful or vindictive at least twice within the past 6 months
Conduct Disorder
a repetitive and persistent pattern of behavior in which the basic rights of others or major age-appropriate societal norms or rules are violated
Requirements for diagnosis of Conduct Disorder
Symptom threshold reached: manifested by the presence of at least 3 of the 15 criteria in the past 12 months from any of the categories below, with at least 1 criterion present in the past 6 months
+ Impairments
+ Differential diagnosis is ruled out
Impairments of conduct disorder
behavioral disturbance causes clinically significant impairment in social,academic, or occupational functioning
Categories of symptoms of conduct disorder
1) Aggression to people and animals
2) Destruction of property
3) Deceitfulness or Theft
4) Serious violation of rights
Aggression to people and animals (CD Symptom)
Often bullies, threatens, or intimidates others. Often initiates physical fights.
Has used a weapon that can cause serious physical harm to others (e.g., a bat, brick, broken bottle, knife, gun).
Has been physically cruel to people.
Has been physically cruel to animals.
Has stolen while confronting a victim (e.g., mugging, purse snatching, extortion, armed robbery).
Has forced someone into sexual activity.
Destruction of property (CD Symptom)
Has deliberately engaged in fire setting with the intention of causing serious damage.
Has deliberately destroyed others' property (other than by fire setting).
Deceitfulness or theft (CD Symptom)
Has broken into someone else's house, building, or car.
Often lies to obtain goods or favors or to avoid obligations(i.e., "cons" others).
Has stolen items of nontrivial value without confronting a victim (e.g., shoplifting, but without breaking and entering;forgery)
Serious Violation of Rules (CD Symptom)
Often stays out at night despite parental prohibitions,beginning before age 13 years.
Has run away from home overnight at least twice while living in the parental or parental surrogate home, or once without returning for a lengthy period.
Is often truant from school, beginning before age 13 years.
Antisocial Personality Disorder
a pervasive pattern of disregard for and violation of the rights of others
requirements for diagnosis for ASPD
Symptom threshold reached: occurring since age 15 years, as indicated by 3 (or more) symptoms
Age: the individual is at least 18 years
Age of onset: there is evidence of conduct disorder with onset before age 15 years.
+Differential diagnoses ruled out
Categories of symptoms to ASPD
1) Failure to conform to social norms and laws
2) Deceitfulness
3) Impulsivity or failure to plan ahead
4) Irritability and aggressiveness, as indicated by repeated physical fights and assaults
5) Reckless disregard for safety of self and others
6) Consistent irresponsibility
7) Lack of remorse
transitory
Many problems experienced by adolescents are
relatively _______ in nature and are resolved by the
beginning of adulthood, with few long-term
repercussions
occasional
We need to distinguish between __________
experimentation and enduring patterns of dangerous
or troublesome behaviors
origins and onset
We need to distinguish between problems that have
their _________ during adolescence and those
that have their roots in earlier periods
key developmental changes in adolescence
Parent-adolescent relationships
Peer relationships
Development of self and identity
Pubertal development
Brain development
Adolescent susceptibility to substance use problems
Increased sensitivity to reward
Increased sensation seeking and risk taking
Increased gradual development of top down cognitive control
Increased sensitivity to social signals
> peer evaluation and peer influences
Increased stressors
> puberty, parent-adolescent conflict, peer/social
stress
parent-adolescent relationship changes
Independence, collapse of authority, growth in defiance
peer-adolescent relationship changes
Deeper connections, same gendered play groups to cross gender, developments in social anxiety
More complex conflicts and dynamics
New types of activities (no longer play dates)
Peer pressure becomes present; Teens more selective of their peers
development of self and identity
Start to develop their own values aside from parents values and expectations
Start to develop and refine their identity, not just who I am as a person but in different domains: athletics, academics, culture, social, ethic exploration of identity (shapes their interactions with individuals from different groups)
pubertal development
Changes happening in social cognition and body
Conceptions of relationships
brain development
Involves the development and structure of self regulation
Dual system theory:
1) motion driven control-happy = "go for it"
2) Top-down control = executive function, less emotion driven and more planned and effortful (but this develops later); imbalanced, emotion driven is present and executive functioning is developing
heterotypic continuity
sequential development of different disorders across development
e.g. One type of anxiety disorder can develop into another type of anxiety disorder (separation anxiety in middle school → generalized anxiety in high school; symptoms can be sporadic not categorizable)
homotypic continuity
continuity of same disorder or symptoms over time (emerges in middle childhood and later); not in early childhood
trait impulsivity
most common risk factor for externalizing spectrum disorders. Heritable but also shaped by environment. Good evidence for dimensional approach to diagnosis as its shares commonality for many conduct problems and then disorders
Etiology of conduct problems (level 1)
environmental/genetic factors
Multiple genes, polymorphism related to trait impulsivity
Environmental: poverty, adversity, positive parenting, prosocial peers (can be protective or vulnerability factors)
Etiology of conduct problems (level 2)
biological/personality factors (Endophenotype)
Explain association between environmental genetic risk and risk
Behavior level → personality, coping styles, temperament, emotional affect
Brain organization
Molecular indicators
Etiology of conduct problems (level 3)
psychopathology/phenotype
polymorphism
refers to the role of common genetic variations in influencing an individual's susceptibility to psychiatric disorders
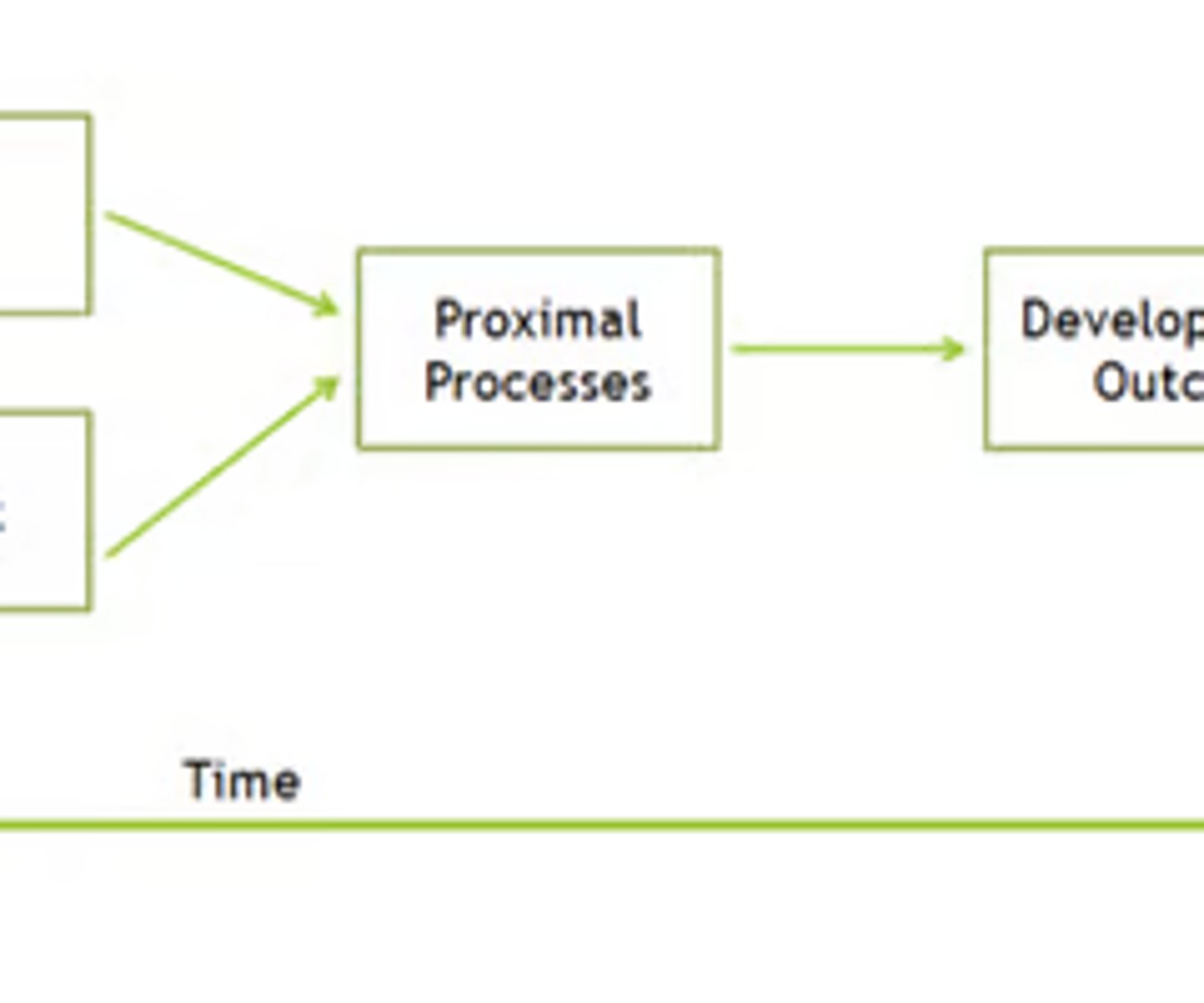
proximal process
The complex reciprocal interactions between the child and their immediate external environment e.g., parent-child interactions, child-child activities, group or solitary play, reading, digital media use
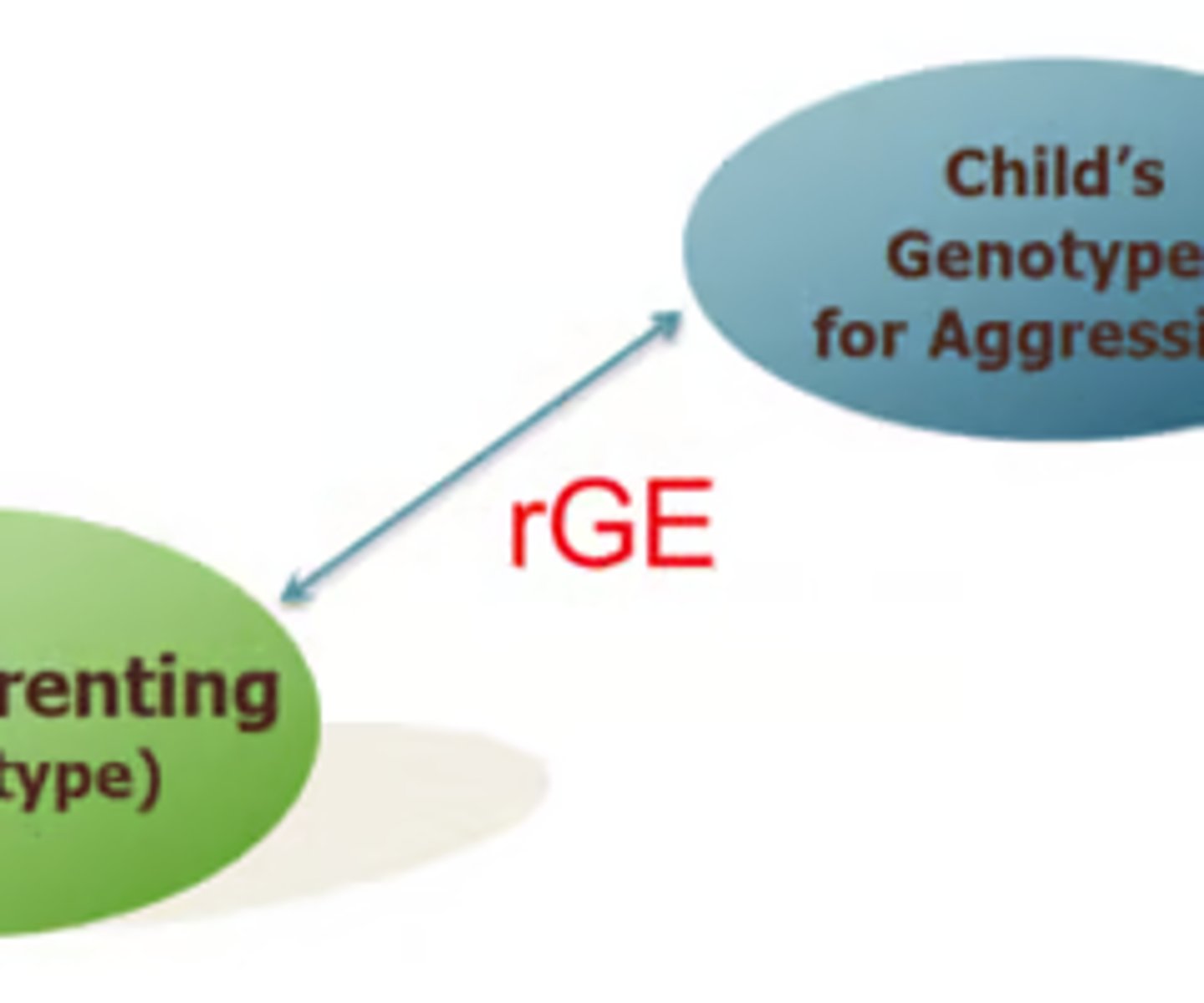
gene environment correlation
The correlation between the child's genotype and the child's environment
If you measure children's genotype for aggression → measure parenting (found with children with genotype with aggression, parents are more likely to be harsh → rGE = correlation)
gene x environment
Genotype moderates the effect of an environmental risk factor on a disorder, different from rGE

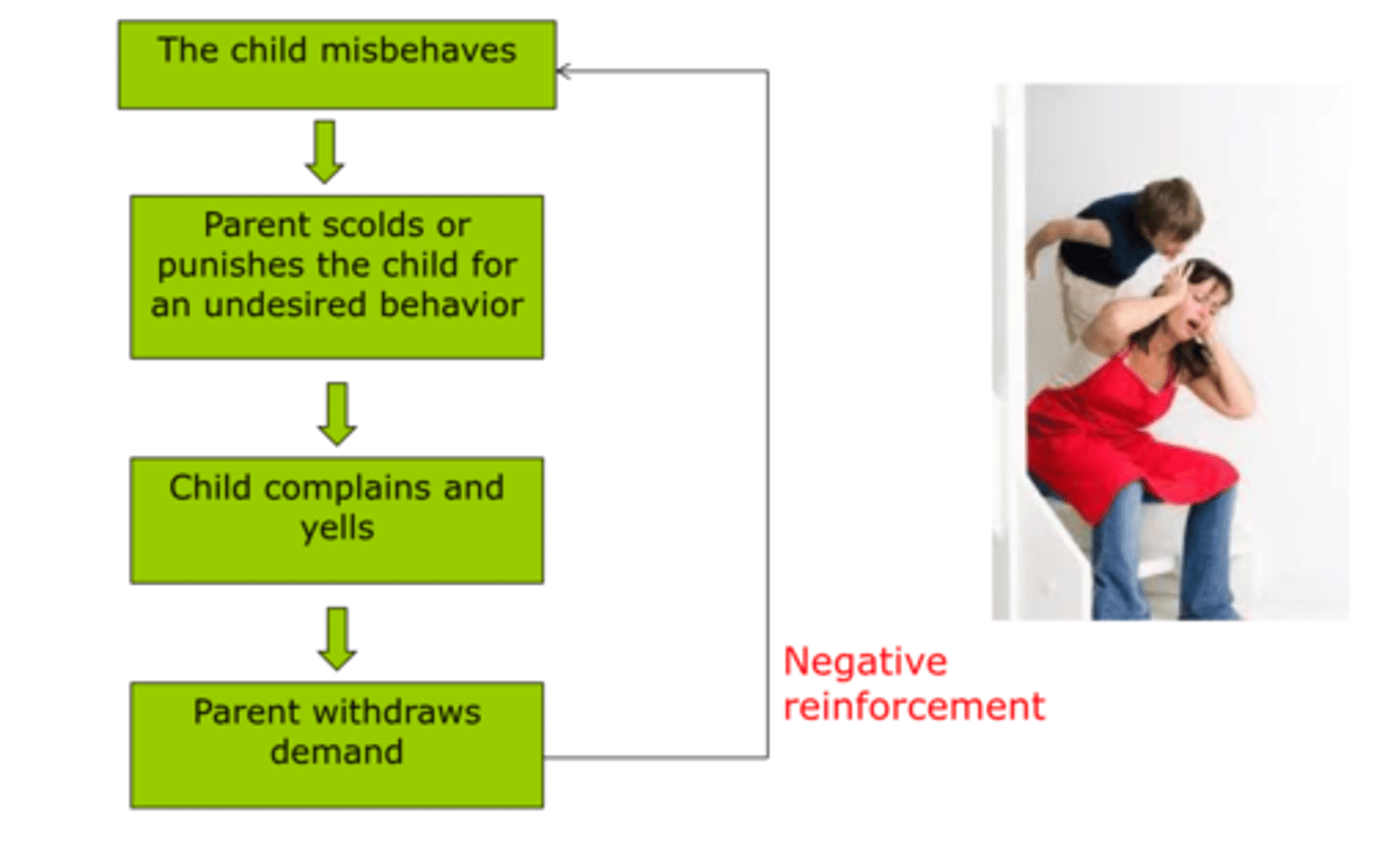
coercive exchange
Children throwing temper tantrum when parent tries to discipline, parent relinquishes discipline in order to appease/calm down child becoming negative reinforcement
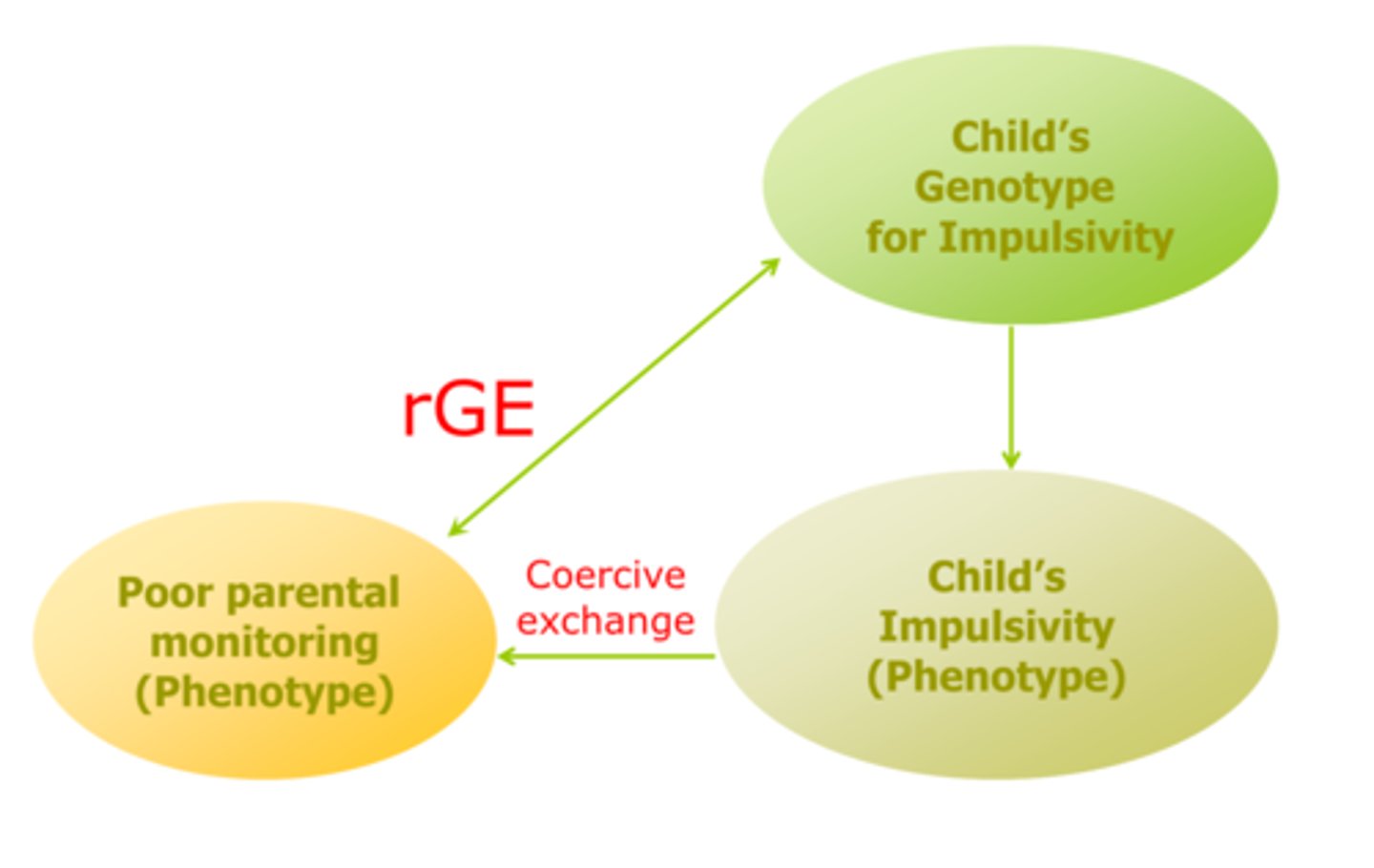
evocative gene environment correlation
Child's genetic risk for impulsivity, (high levels of impulsivity, low self control) → tends to engage in coercive exchange process that escalates their behavior parents withdrawal demands, and parents give up on monitoring child's behavior
Genetic risk for impulsivity leads to genetic risk factor
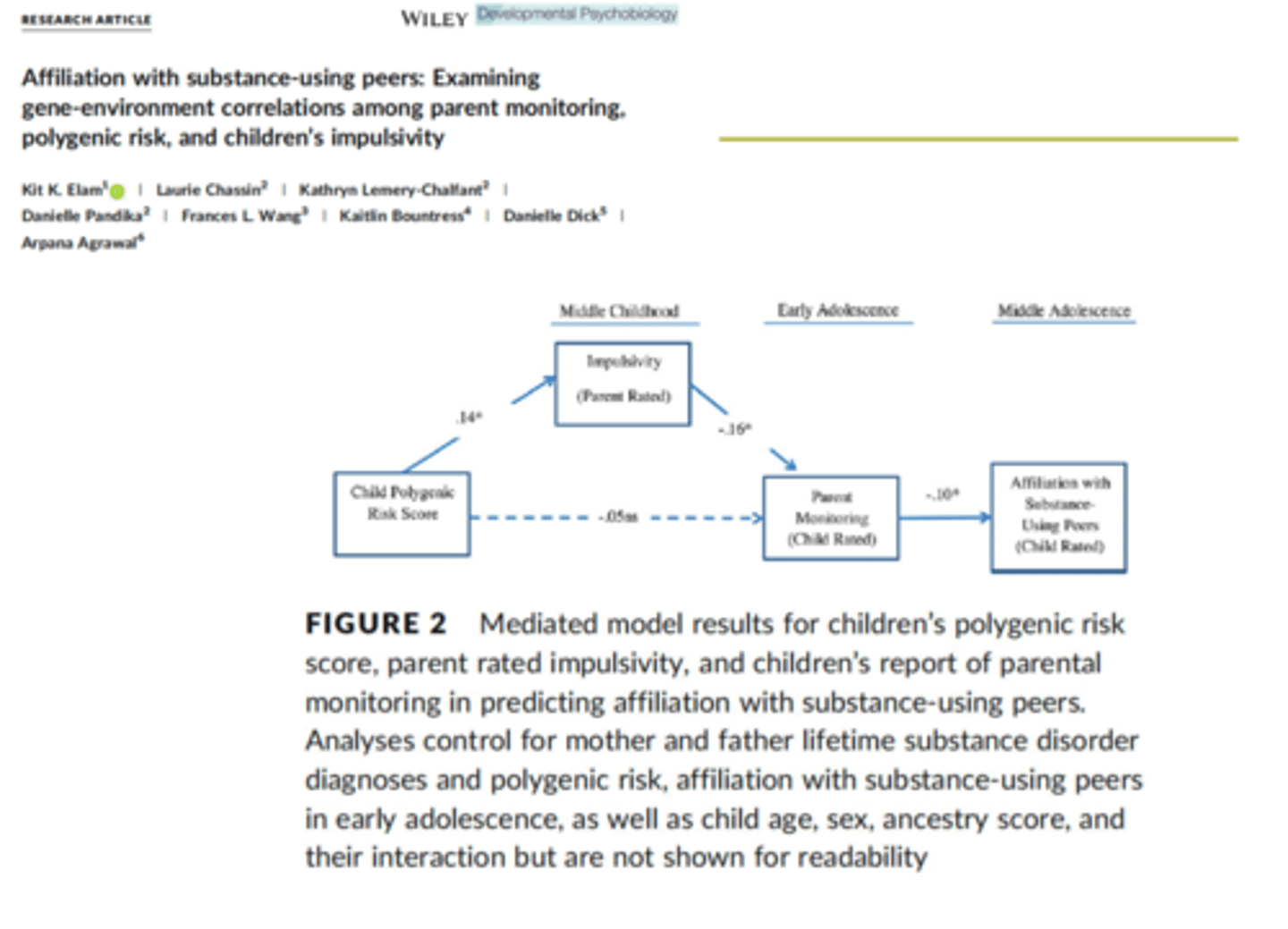
Examining gene environment correlations in parent monitoring, polygenic risk, and children's impulsivity
Lack of monitoring leads to risk of association with deviant peers (originally associated with polygenic risk, but impulsivity in the model makes that direct path no longer significant) → no longer moderates genetic risk with parental monitoring
Who (Conduct Problem Intervention)
Target population of your intervention
When (Conduct Problem Intervention)
developmental stage of children
How (Conduct problem intervention)
intervention context/setting and intervention strategy
Incredible Years Parent Training Program
Parent training, teacher training, child conduct training
Intervention originally developed to target children who were 3-9 years old at high risk for conduct problems and their parents (who have a hard time managing children' s behaviors)
For this specific intervention-parent training groups, 12 week program (parents come to the clinic, 8-12 parents per group with two facilitators-different formats, video, group discussion, discussion→ teaching effective management to stop the negative cycle of child misbehaving and how parents intervene
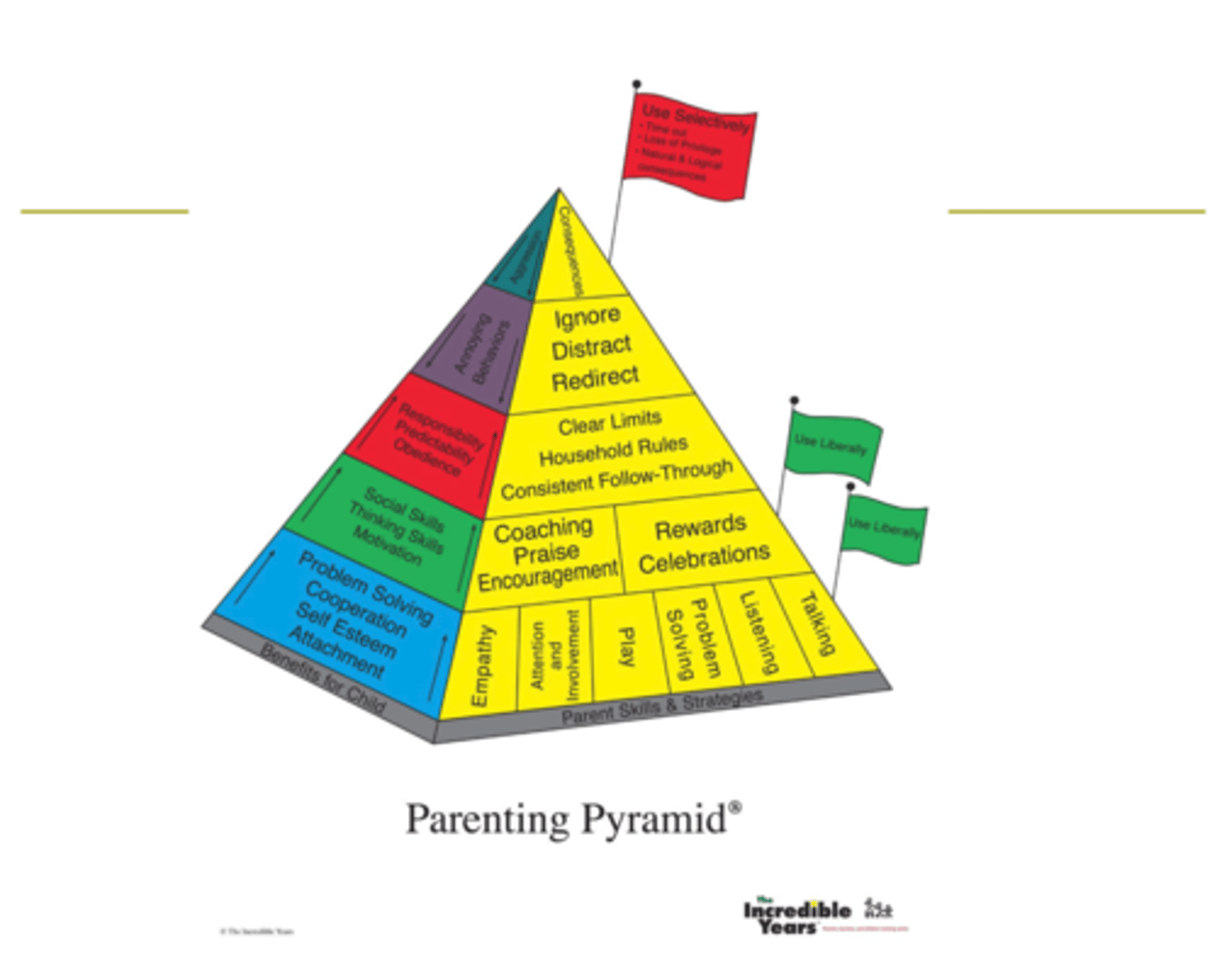
Parenting Pyramid
Shows different types of skills that parents use to intervene with the child
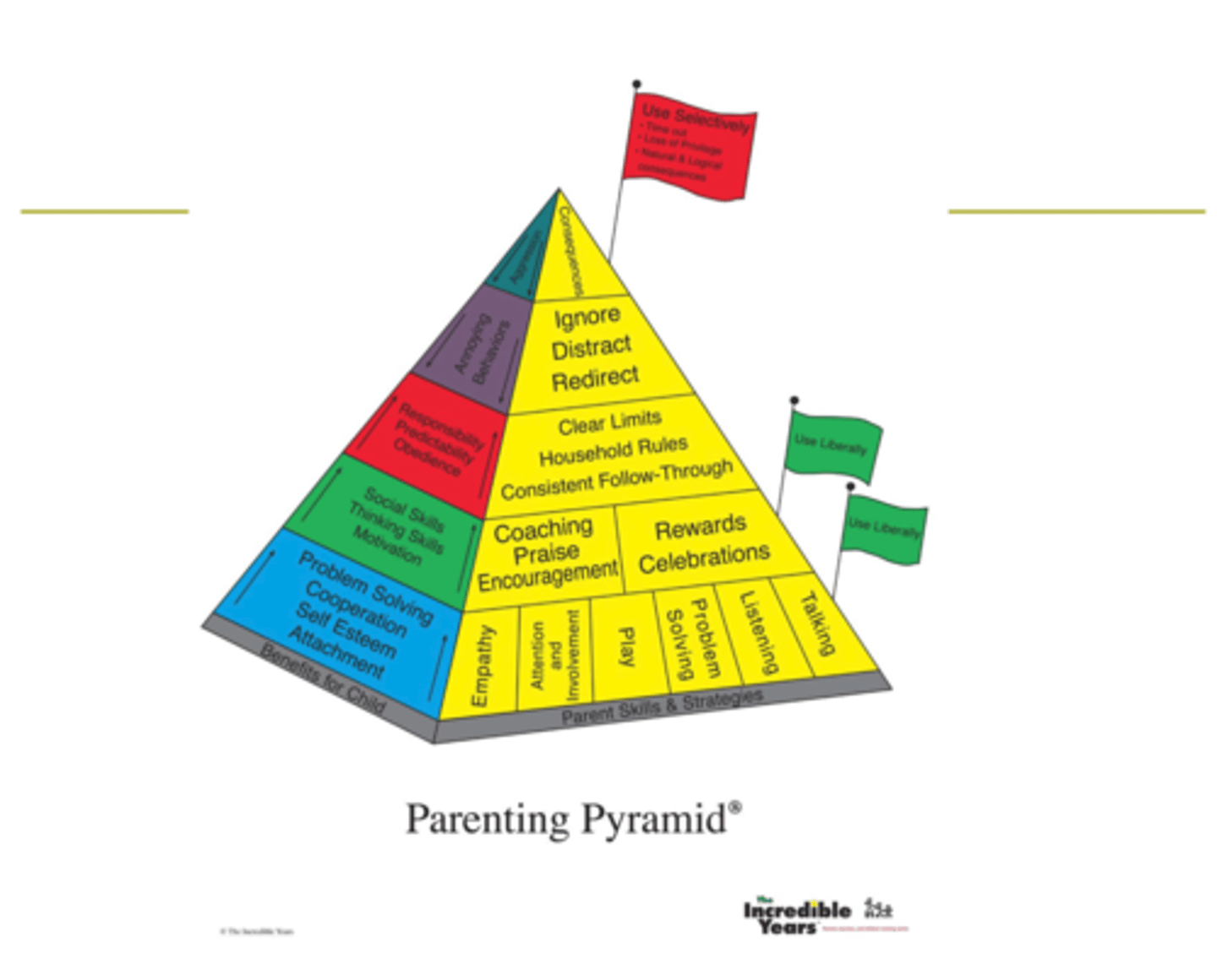
Parenting Pyramid (base)
positive parenting behaviors (encouraged to use unlimited-ly)
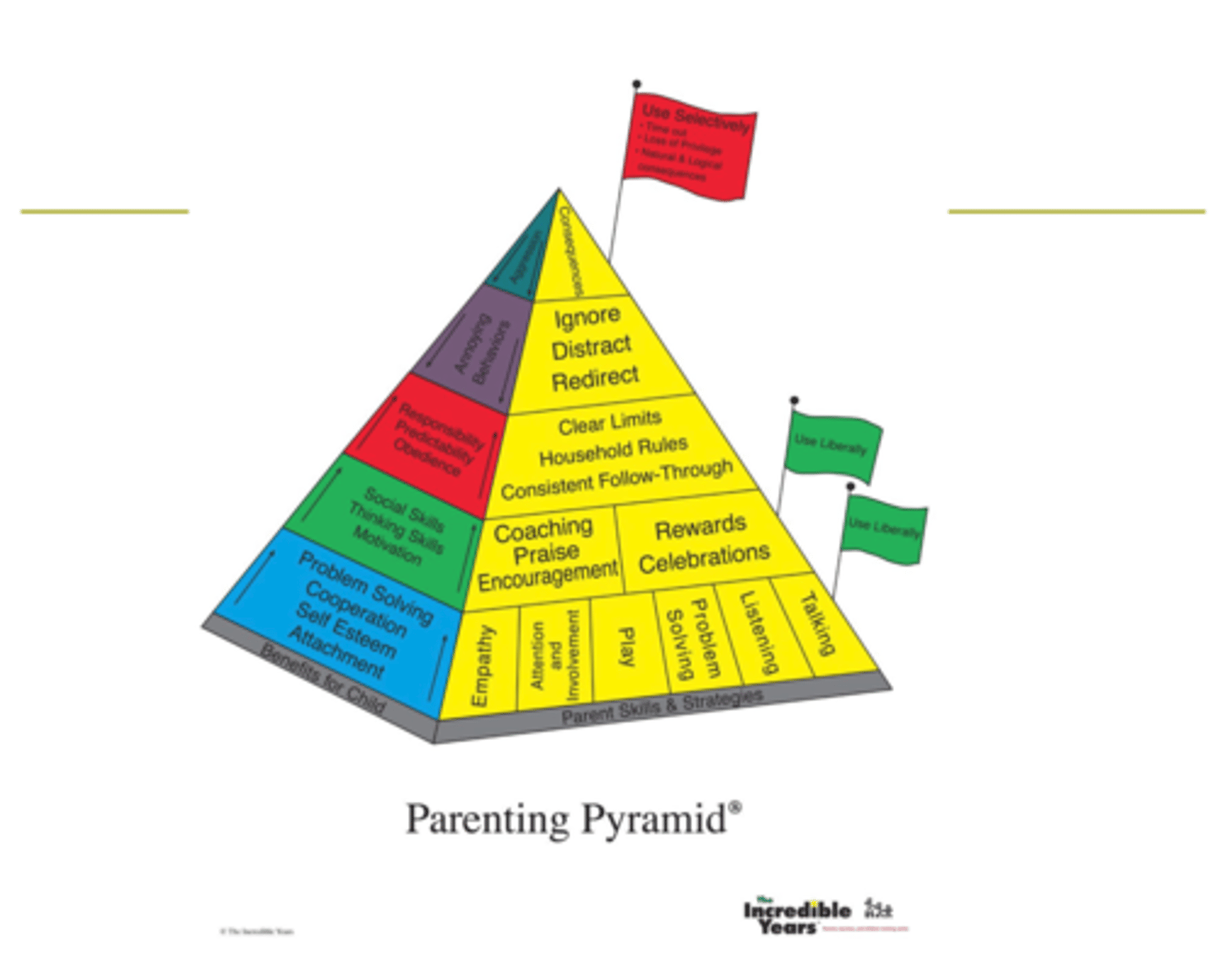
Parenting Pyramid (up from base)
Up the base, using reward instead of punishment → but using only liberally because they want them to clean their room without having to need a reward for doing so
Behaviors that they want parents to select: “Clear limits household rules consistent follow-through”
Parenting skills that target negative behaviors of a child (whining, disobedience) → parents encouraged to use strategies cautiously “ignore, distract, redirect”
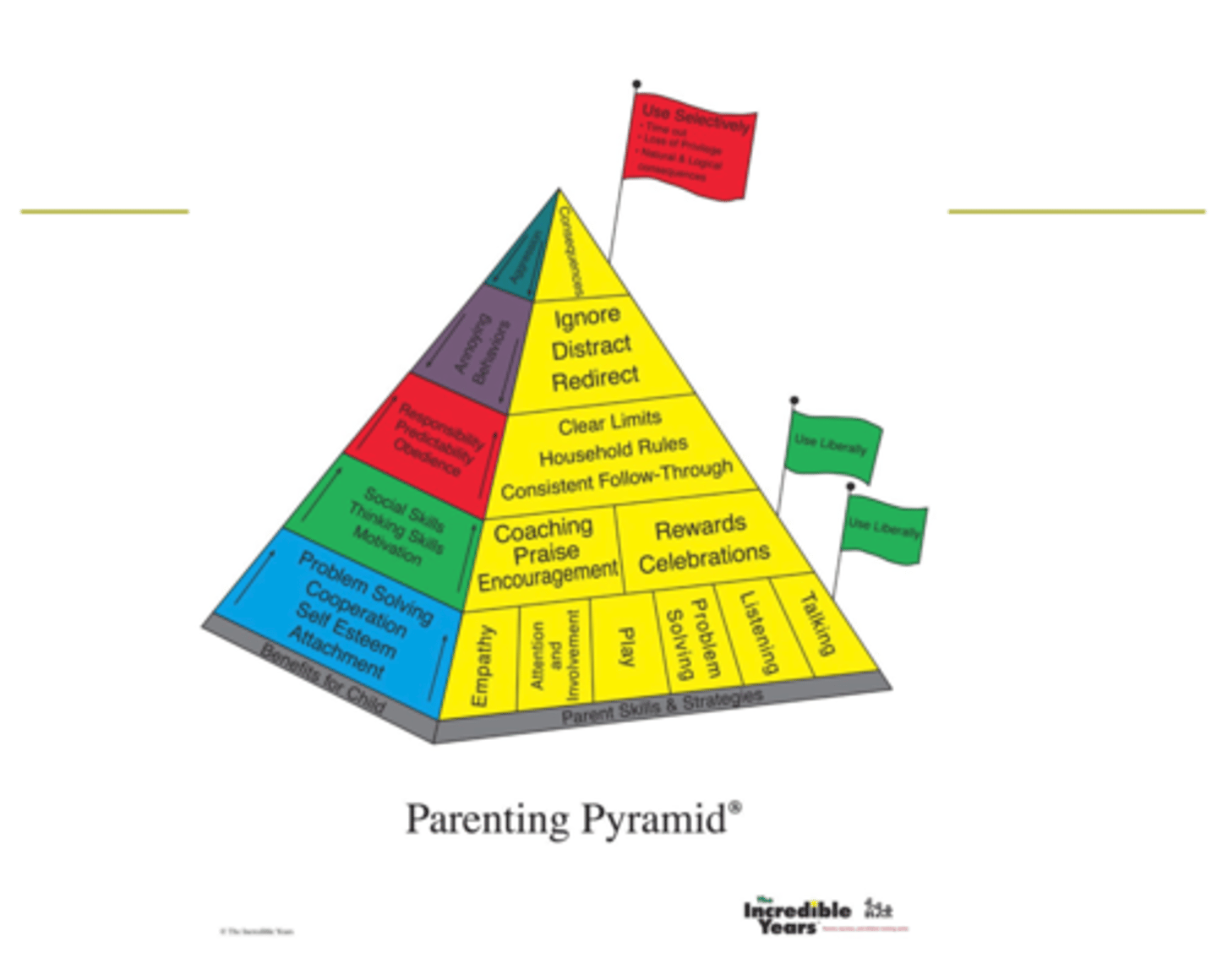
Parenting Pyramid (top)
At top: not that parents should never use but they have to use it extremely cautiously "use selectively"
externalizing liability
predicts development of all disorders, manifest in different behaviors
early intervention
best intervention, even beyond parent training (Incredible Years), school-based, or child specific (one on one therapy sessions)
"Peer Influences on Adolescent Risk Taking"
fMRI study
• While being observed by peers, adolescents showed greater activation in reward-
related brain regions (ventral striatum & orbitofrontal cortex)
• Activities in reward-related brain regions predicted subsequent risk-taking behaviors
• Adults showed no differences in activations in reward-related regions as a function of social context (peers vs. no peers)
Chein et al. (2011).
Prevalence of Adolescent Substance Use Problems in the U.S.
Study conducted in Michigan, but sampled across the nation
Rural and urban areas (trying to be representative of the whole population)
Longitudinal study: but new–looking at 50,000 8th, 10th, and 12th grade every year (not same kids but same environments)
Latest Findings of "Prevalence of Adolescent Substance Use Problem in the U.S"
• Most forms of drug use showed steep and
atypical declines in 2021 (the largest and
broadest declination in 46 years)
• Marijuana: the most prevalent form of illicit drugs
used by teens, showed a sharp decline (24% -
27%) in lifetime, annual, and 30-day prevalence
from 2020 to 2021
• Vaping: nicotine vaping had the highest annual
prevalence of substances other than alcohol in
2020, but it dropped by 29% in 2021
• Drugs with no change in annual prevalence in
2021: inhalants, hallucinogens other than LSD,
crack cocaine, heroin, Oxycontin, Vicodin, Ritalin
Substance Use Disorder (SUD)
A cluster of cognitive, behavioral, and physiological symptoms indicating that the individual continues using the substance despite significant substance-related problems
Substances SUD can be applied to
1) alcohol
2) cannabis
3) hallucinogens
4) inhalants
5) opioids
6) sedatives
7) hypnotics
8) anxiolytics
9) stimulants
10) tobacco, and other (unknown) substances
Alcohol Use Disorder (AUD)
A problematic pattern of alcohol use leading to clinically significantimpairment or distress
Requirements for diagnosis of AUD
manifested by at least two symptoms occurring within a 12-month period
Categories of symptoms in AUD
Impaired control over substance use
Social impairment related to substance use
Risky use of substance (failure to abstinence despite risks)
Pharmacological effects
Impaired control over substance use
1. Taken in larger amounts or over a longer period than was intended
2. Persistent desire or unsuccessful efforts to obtain and use alcohol
3. A great deal of time spent to obtain or use alcohol, or recover from its effects
4. Craving, or a strong desire or urge to use alcohol
Social impairment related to substance use
5. Failure to fulfill major role obligation
6. Continued use despite social or interpersonal problems caused/exacerbated by alcohol
7. Important social, occupational, or recreational activities given up/reduced because of alcohol
Risky use of substance (failure to abstinence despite risks)
8. Recurrent alcohol use in physically hazardous situations
9. Continued use despite knowledge of physical or psychological problems caused by alcohol
Pharmacological Effects
tolerance and withdrawal
Tolerance
a. A need for markedly increased amounts of alcohol to achieve intoxication or desired effects
b. A markedly diminished effect with continued use of the same amount of alcohol
Withdrawal
a. The characteristic withdrawal syndrome for alcohol (e.g., autonomic hyperactivity, hand tremor, insomnia...)
b. Alcohol (or a closely related substance) is taken to relieve or avoid withdrawal symptoms
contextual factors for decline of substance use post-2020 (Macrosystem)
Parents home, helping children with self worth, mediates substance use as that "beneficial" factor
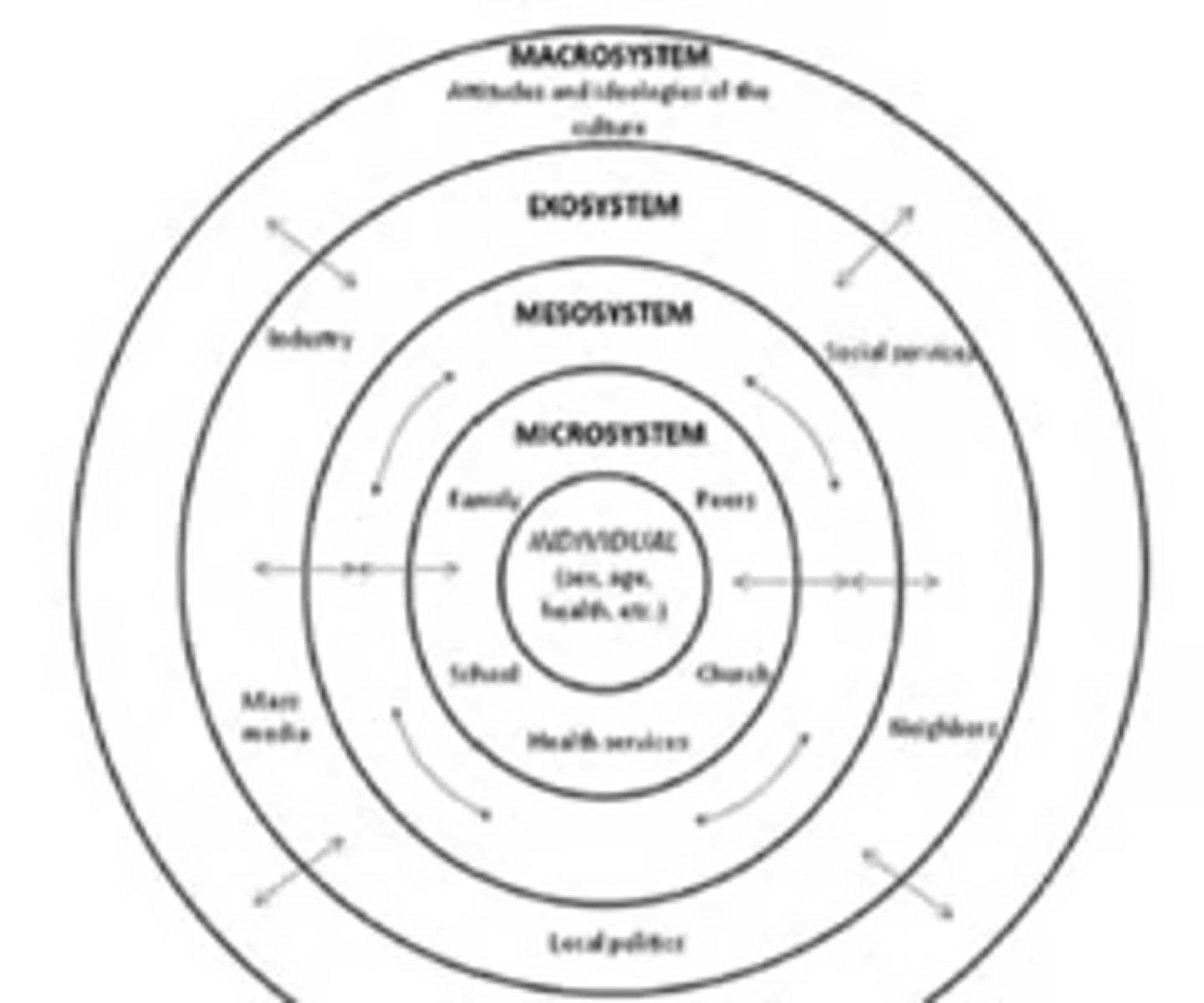
Microsystem
First layer of Bio-ecological model
a pattern of activities, social roles, and interpersonal relations experienced by the developing person in a given face-to-face setting with particular features...
e.g., mother-infant dyad, teacher-child interactions, child-peer interactions at playground...

Mesosystem
Second layer of Bio-ecological model
The relationships between two or more microsystems
e.g., parents' influences on children's peer network, parent involvement in children's schooling, family's relationships with neighbors...

Exosystem
linkages and processes taking place between two or more settings, at least one of which does not contain the developing person, but in which events occur that indirectly influence processes within the immediate setting in which the developing person lives
e.g., parents' work environment, industry, school board, local policies, neighborhoods, social services

Macrosystem
The general prototypes, existing in the culture or subculture that set the pattern for the structure and activities occurring at the concrete level
e.g., education or school systems, healthcare laws, immigration laws, societal attitudes/ideologies of cultural groups, the COVID-19 pandemic....
general development trend of SUD
1) Typically children start initiating in middle school and peaks in emerging adulthood, and decreases in mid to late adulthood
2) Use of gateway drug (alcohol and nicotine) "weed' other illegal drugs
3) Abstinence → experimental use → early abuse → abuse → dependence
Early-onset subtype (SUD)
differing by when they start to use, and change in use pattern when they start
Includes:
Children who initiate substance use quite early
Stronger association with family risk factors (genetic predisposition to substance abuse) / worse prognosis and outcomes
Late onset subtype (SUD)
initiation in late adolescence or emerging adulthood
Associated with different prognosis and risk factors
Tends to be associated with environmental factors, deviant years and coexisting with periods of autonomy
Questions: Because limited in adolescence (expecting substance use to decrease after adolescence) we expect their substance use to decrease, instead with LOS it continues
"Two hypothetical trajectories of antisocial behaviors"
1) Childhood-onset or life-course-persistent trajectory
2) Adolescent-onset or adolescence-limited trajectory
"Developmental trajectories of conduct problems"
Followed over 17,000 children (male and female) nationally representative sample, born between 2000-2002
For this study they used 6 waves of data, measured parents reporting symptoms of children (9 months, 3 years, 5 years ,7 years, 11 years, and 14 years) → reported by mothers
Reported (1) conduct problems and (2) risk factors, (3) family risk factors and (4) socioeconomic risk factors
(1) Conduct Problems
temper tantrums, obedient (-), fights/bullies, lies/cheats
(2) Child Risk Factors
co-morbid inattention/hyperactivity, peer problems, and emotional problems
(3) Family Risk Factors
non-intact family, large family size, parental depression, poor parental physical health
(4) Socioeconomic risk factors
low parental education, low household income, parental worklessness, social housing
Graph "Developmental trajectories of conduct problems"
Low-level CP: about 50% have 0 conduct problems
High level persistent CP: 7% of children in the sample
Childhood limited: age 3-4 relatively high levels of CP but then decrease in CP after preschool and into elementary school periods, by the time they are in middle school = very low CP (23%)
Adolescent onset: moderate to low levels of CP in childhood, but in elementary school = stars to increase ; by age 14 they have higher CP
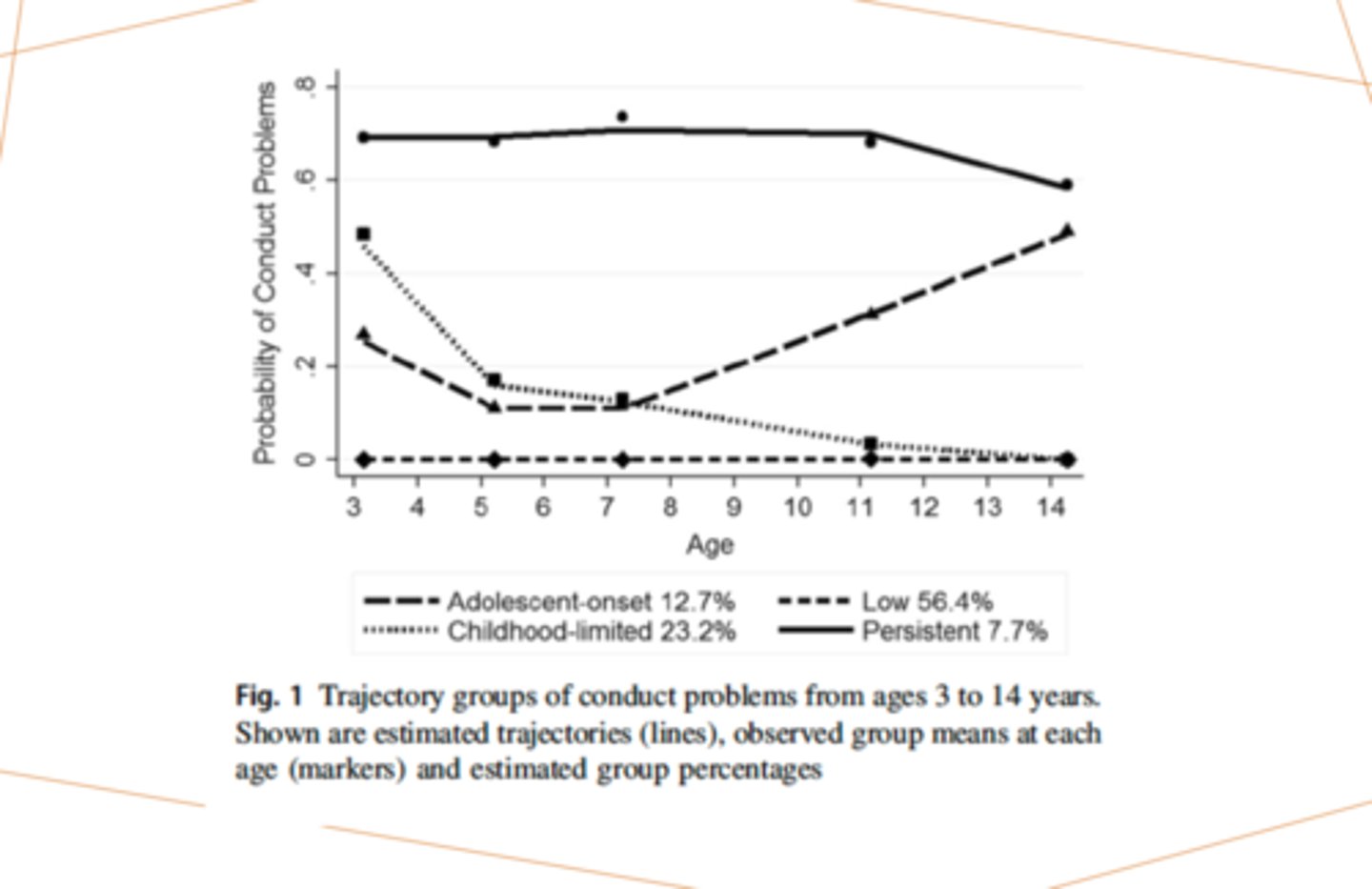
Findings in "Developmental trajectories of conduct problems"
Out of three problematic trajectories: high level of early socioeconomic, child, and family risks
For childhood-limited pathway, exposure to family SES, and child risk factors receded after childhood
For adolescent onset and persistent pathways, exposure to family and child risks continued through adolescence
We need to make treatment plans specific to “trajectories”
Etiological models to AUD
1) Deviance Proneness Pathway
2) Negative Affect (Externalizing Pathways)
Deviance Proneness Pathway
Starting point → family history of alcoholism = largest risk factor
Some shared mediators: for ultimate deviant = association with deviant peers
Ineffective parenting practices and temperament (bi-directional, mediator)
dis inhibition and deficits in executive function = academic failure → developmentally will lead to association with deviant peers (been established in a lot of literature do poorly at school)
Parenting is a moderator → not all children who have failure at school have association with deviant peers (more active parents = not continued pathway to alcoholism, similarly parenting can moderate temperament to associate with deviant peer (if parents are warm and supporting and high levels of monitoring that can prevent them)
Association with deviant peers
Ultimate mediator to AUD in adolescents
Parental alcohol dependence was positively associated with children's affiliation with substance-using peers and siblings,which in turn predicted greater alcohol use in emerging adults
Impulsivity at age 9 positively predicted peer deviance at age 12, which in turn predicted adolescents' alcohol use at age 15