2130 unit 5
1/145
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
146 Terms
What are seven different functions of the kidney?
(1) Regulation of ECF volume & BP
(2) Regulation of osmolarity
remove extra solutes to maintain balance
(3) Maintenance of ion balance
examine each ion to conserve OR excrete ions not needed
(4) Maintenance of body pH
keep body in narrow range otherwise die (work w/ lungs to regulate)
(5) Excretion of wastes
remove waste from blood plasma (urea, ammonia, creatinine)
recover essential substances → glucose, AAs, water, ions, Na, Cl
waste can accumulate BUT X = death
(6) Production of hormones
make erythropoietin (EPO) → helps RBC maturation
make vit D → activated by kidney
(7) Gluconeogenesis
makes new glucose molecules from non carb sources
What is the most important function of the kidney?
Regulation of total body water and salt balance (of blood plasma in ECF)
w/o = X survive if ECF, osmolarity & ions dissolved in plasmas unregulated
EX → INC H2O intake = INC ECF volume = INC blood plasma volume = INC BP & need to remove CDF to DEC BP to normal
What are three ways the kidneys contribute to homeostasis?
Balance ECF volume
regulate osmolarity
maintain ion balance
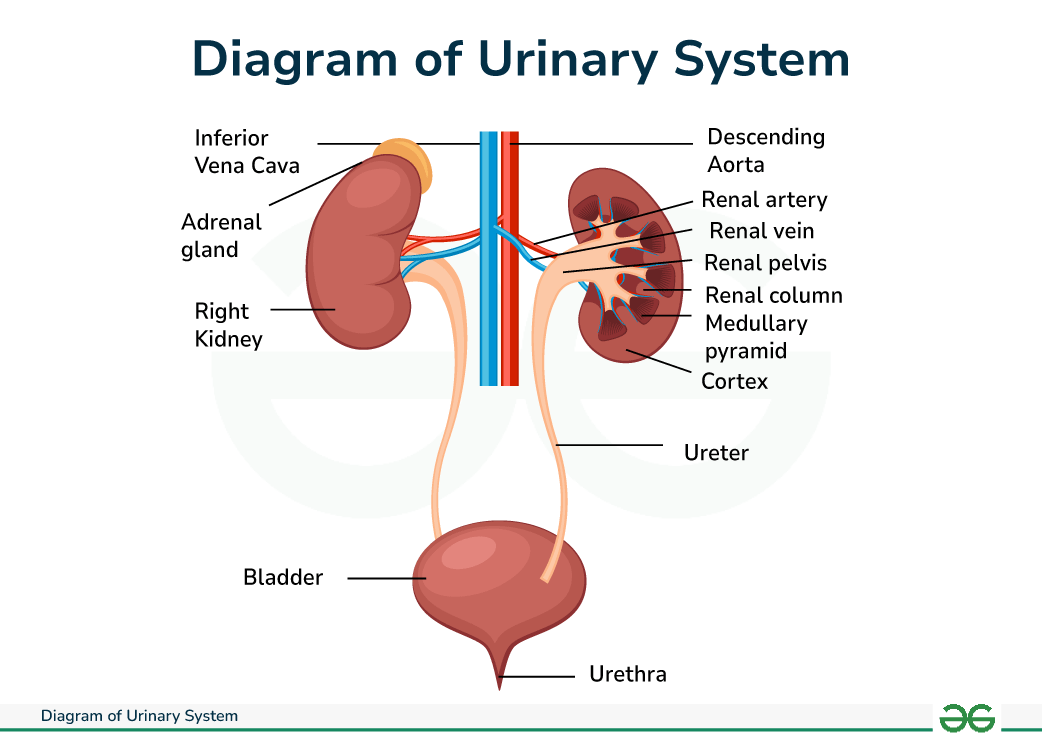
urinary system anatomy
kidney → filter blood, process it & unabsorbed items excreted via urine
renal artery → 1 on inner concave side of each kidney, big blood vessel brings O2 blood inside
renal vein → 1 on inner concave side of each kidney, send blood to body w/ nutrients to conserve/return to blood
ureter → 1 on each kidney, filter blood X absorbed & take urine out
bladder → collects urine made from both kidneys
urethra → tube releases urine from body (INC length M)
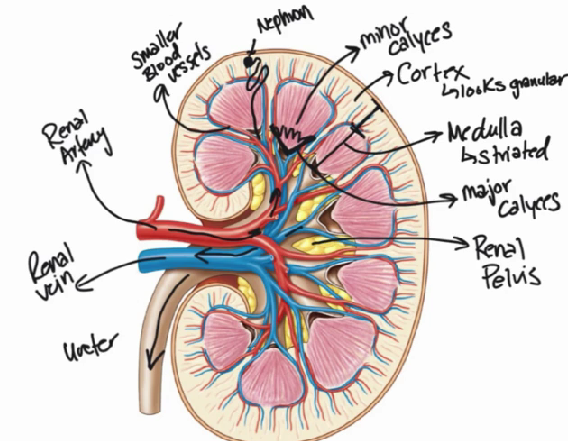
kidney anatomy
renal vein → blood sent back to body to be used
renal artery → brings in blood & flow thru smaller blood vessels to cortex
cortex → outer layer, granular b/c of nephron
medulla → inner layer, straited b/c of nephron
nephron → structures filter blood, make urine, collected in minor calyces & collected to rental pelvis
calyces minor → in medulla & collects urine from nephron & funnel into calyces major
calyces major → funnel in urine from minor calyces & send to renal pelvis
renal pelvis → center of kidney, hollow, collects urine & leave via ureter
ureter → bring urine to bladder & out of body
How are the kidneys positioned?
retroperitoneally → outside abdominal cavity & btwn membrane lining of abdomen & back bone/muscles
posterior to abdomen each side of spine @ 11/12th rib
What happens at the inner concave side of the kidney?
Where blood supply enters w/ renal artery and exists via renal vein
What is the function of the ureter?
Where urine produced by kidneys is removed
located on the inner concave side of the kidney
What is the function of the bladder?
Collects urine produced by both kidneys
Stores the urine until it is full and triggers the urge to urinate
What is the urethra?
tube where urine exits the body from the bladder
kidney stones
precipitation & crystallization of INC than regular [minerals] = stones
occur in diff locations on urinary tract → renal pelvis, ureter & urethra
renal pelvis → if VV big, stuck here & hard exit kidney via ureter
EX → oxalate, P, Ca, uric acid
TREATEMENT
lithotripsy = E waves pulverize stones to smaller parts
ureteroscopy = use laser break apart & grab out of ureter
surgery
nephron
functional unit of kidney
each kidney = 1M nephrons
IRL = twist on itself & covered in blood vessels
(1) renal corpuscle
(2) tubule (proximal, loop of Henle, distal convoluted tubule, collecting duct)
What is the renal corpuscle?
filters blood
makes filtrate & it travels through tubule
(1) Bowman's Capsule → where fluid filters into
(2) Glomerulus → specialized leaky capillaries
(3) Juxtaglomerular Apparatus (JGA) → junction of tubule & arterioles around bowman’s capsule
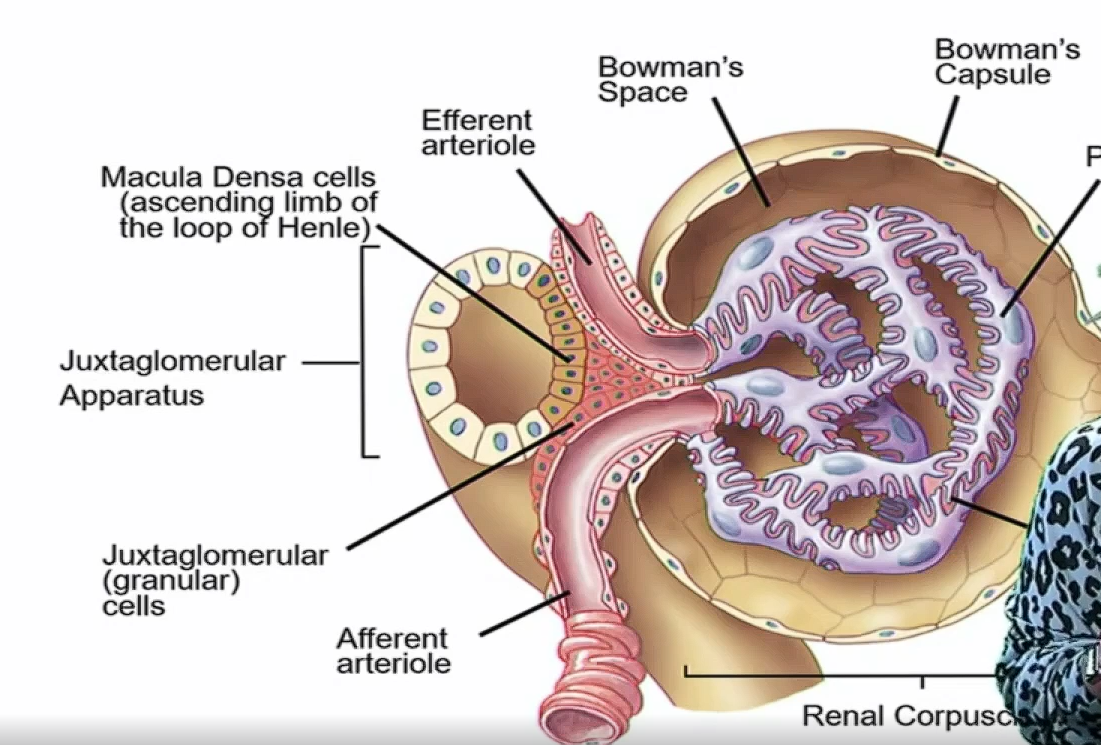
What is the Bowman's Capsule?
fluid filled ball hollow structure
surround glomerulus & connects to proximal tubule
(1) bowman’s/capsular space → inside of capsule, where filtrate collects
(2) epithelial cells → outside
(3) podocytes → contact glomerulus
What are podocytes?
cells that wrap around the glomerulus
stop excess leaking & filters fluid from blood → bowman’s space (all has to go thru this)
What is the function of the glomerulus?
leaky capillaries bed 4 filtration from blood → bowman’s space
blood enter = Afferent arteriole
blood leave = Efferent arteriole (X all blood filtered b/c moving & exits)
What is the juxtaglomerular apparatus (JGA)?
junction of =
(1) late ascending limb of Henle (touches corpuscle)
macula densa cells → detect [Na] & [Cl] & speed filtrate pass
(2) arterioles → afferent (IN) & efferent (OUT)
limb passes thru these blood vessels
around Bowman's Capsule
secretes renin from granular/juxtaglomerular cells
what is the afferent arteriole?
bring blood from renal artery → each nephron’s afferent arteriole → glomerulus (travels to bowman’s space OR out w efferent arteriole)
juxtaglomerular/glandular cells → behind macula densa, make & release renin
what is the efferent arteriole?
blood exit from renal corpuscle
What is the tubule?
tube-like structure made up of a single layer of epithelial cells
wraps around itself & forms JGA
process & modifies fluid → varies based on each part
(1) proximal tubule = close to corpuscle
(2) loop of Henle = descending & ascending limbs
(3) distal convoluted tubules
(4) collecting duct = connects w/ many nephrons on 1 collecting duct
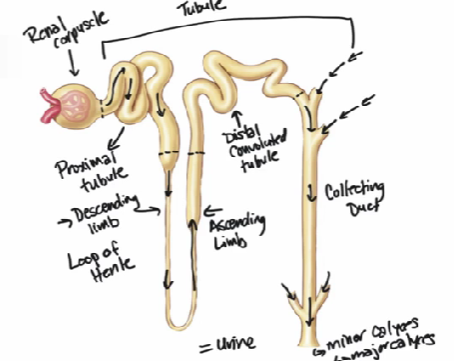
What is the direction that filtrate travels?
renal artery → smaller blood vessels → nephron [ Renal corpuscle → proximal tubule → descending limb of Henle → ascending limb of Henle → distal convoluted tubule → collecting duct] → minor calyces → major calyces → renal pelvis → ureter → bladder → urethra
where are nephrons found?
within layers of cortex & medulla in kidney
fits with smaller blood vessels branches (1M nephrons in 1 kidney)
from renal artery surrounds medulla & fills in cortex
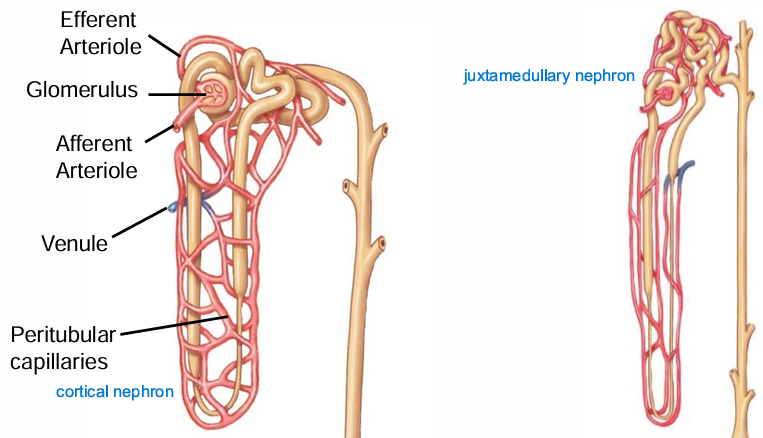
what are the types of nephrons?
based on position & anatomical differences BUT → filter blood, process fluid same as tubules
cortical nephron
80% of all
short loop of Henle
renal corpuscle upper part of cortex
peritubular capillaries → reabsorb filtrate
juxtamedullary nephron
20% of all
longer loop of Henle
renal corpuscle next to medulla
vasa recti capillaries → reabsorb filtrate & [] urine
![<p>based on position & anatomical differences BUT → filter blood, process fluid same as tubules </p><ol><li><p>cortical nephron</p><ul><li><p>80% of all </p></li><li><p>short loop of Henle</p></li><li><p>renal corpuscle upper part of cortex </p></li><li><p>peritubular capillaries → reabsorb filtrate</p></li></ul></li><li><p>juxtamedullary nephron</p><ul><li><p>20% of all</p></li><li><p>longer loop of Henle </p></li><li><p>renal corpuscle next to medulla</p></li><li><p>vasa recti capillaries → reabsorb filtrate & [] urine</p></li></ul></li></ol><p></p>](https://assets.knowt.com/user-attachments/ba083b7f-8421-4b0f-a61d-d85e2e900ddd.png)
What are peritubular capillaries?
Capillaries next to cortical nephrons that help reabsorb filtrate.
What are vasa recti?
Capillaries next to juxtamedullary nephrons that help reabsorb filtrate and concentrate urine.
In the renal corpuscle, what are the layers that connect the blood vessels to Bowman's capsule?
Podocytes
How much cardiac output is sent to the kidneys?
20%
then filtered in nephrons
large amt needed b/c → keep blood V & efficient ion balance
components of blood sent to kidney?
(1) PLASMA → H2O, proteins, glucose, hormones, CO2, O2, ions
(2) RBC
(3) WBC
What is the order of blood vessels in and around the nephron?
Renal artery --> afferent arteriole --> glomerulus (capillary bed) --> efferent arteriole --> peritubular capillaries/vasa recti --> venule --> renal vein
difference from rest of body = go to 2 diff arterioles & capillaries before venules & veins
impt bc both can contract & dilate
peritubular capillaries/vasa recti = reabsorb glucose back to body
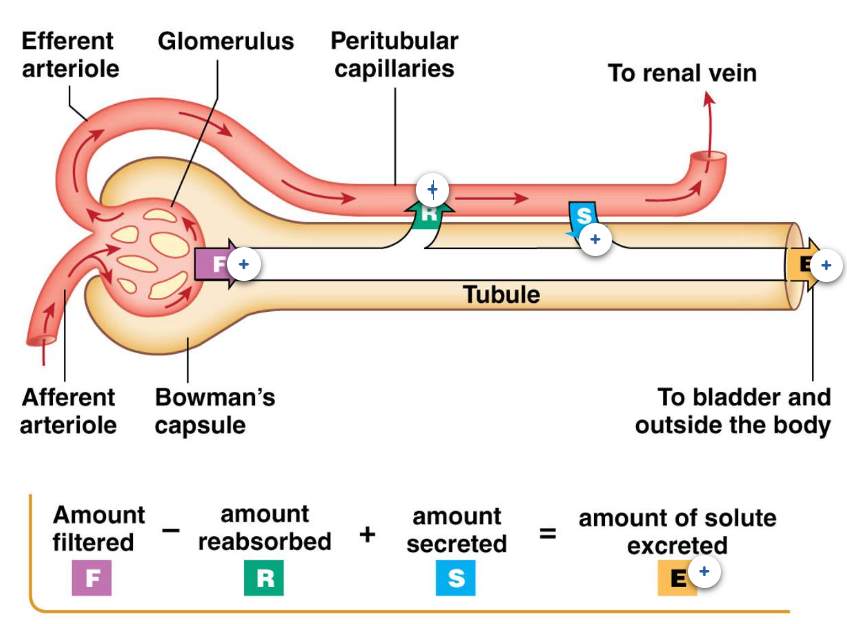
what is the process of the nephron?
most of filtrate reabsorbed back in body → 180L make, 1.5-2L urine
PROCESS
(1) F = filtration
(2) R = reabsorption
(3) S = secretion
(4) E = excreted
What is filtration?
movement of fluid & items dissolved in blood
from glomerulus → Bowman's space (filtrate enters)
ONLY IN RENAL CORPUSCLE
What is reabsorption?
movement of items from filtrate within tubules → surrounding capillary bed (peritubular capillaries/vasa recti capillaries)
most filtered fluid reabsorbed
reabsorbed filtrate = H2O, ions, glucose, AAs
What is secretion?
movement of items dissolved in blood from capillary bed → filtrate in tubule
things dissolved in blood & X filtered in corpuscle
What is excretion?
amount of solute excreted in urine
filtrate collected in renal pelvis → collect to bladder = urine
What is the formula for excretion?
E = F - R + S
solute excreted = filtered - reabsorbed + secreted
what are the filtration barriers?
glomerulus capillary bed has many FENESTRATIONS (pores)
THUS → leaky & everything filters into bowman’s space
THUS → barriers in corpuscle so proteins X filtered
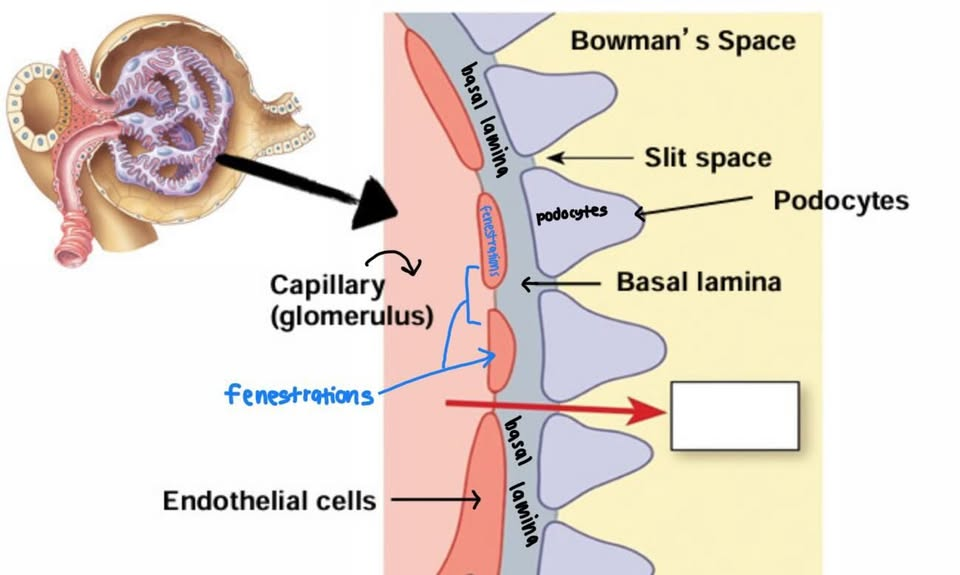
How does the glomerulus serve as a filtration barrier?
has endothelial pores (fenestration) → holes on endothelial cells & spaces btwn endothelial cells
USE → size filter items filter out b/c leaky everything except proteins
How does the basal lamina serve as a filtration barrier?
spaces in btwn fibers = further filter & exclude plasma proteins enter Bowman's capsule
FORM → collagen & (-) charged glycoproteins structure connect endothelial cells of glomerulus to podocytes
How do podocytes serve as a filtration barrier?
use pedicels → wrap & interlace glomerulus w narrow slits
narrow slits btwn each podocyte → narrow or widen & limit SA 4 filtration
THUS → only 20% blood entering glomerulus filtered in bowman space
how does the filtration in the renal capsule work?
blood ENTER renal capsule & nephron via afferent arteriole to make filtrate→
glomerulus’ fenestration sizes + spaces btwn endothelial cells
basal lamina’s space in btwn fibers
podocytes’ spaces in btwn
THEN → blood not filtered exit via efferent arteriole to kidney & to main circuit
What are three methods used for urinalysis measurement?
GOAL = test if healthy based on whats in urine
Visual inspection (colour & clarity)
clear = overhydration
bright yellow = excess multi vitamins (B2)
dark yellow = dehydration
brown = liver/kidney disease, antibiotics, drugs, malaria
frothy = proteinuria, meds (INC BP)
particles/frothing = bacteria, proteins & kidney stones
microscopic evaluation
test if seen w/o microscope, crystal, cell types
small crystals = kidney stones
bacteria, RBC = UTI
RBC = UT cancer
chemical analysis
pH, density w colorimetric strip
WBC/leukocytes = infection
glucose = DM
bilirubin = liver disease/ gallstones (excrete digestive normally)
net filtration pressure
healthy = 10 mmHg
collection of 4 forces that control amt of fluid filtered into bowman’s space
What are the four pressures in the renal corpuscle that contribute to net filtration pressure?
Hydrostatic Pressure of Glomerular Capillaries (PGC)
Colloid Osmotic Pressure of Glomerular Capillaries (πGC)
Hydrostatic Pressure of Bowman's Capsule (PBC)
Colloid Osmotic Pressure of Bowman's Capsule (πBC)
What is the formula for NFP?
NFP = (PGC + πBC) - (PBC + πGC)
What is Hydrostatic Pressure of Glomerular Capillaries (PGC)?
heart’s pressure push blood → leaky glomerular capillaries → capsule space
FAVOURS filtration
#1 force promotes filtration
What is Colloid Osmotic Pressure of Glomerular Capillaries (πGC)?
water's pressure from its affinity 4 proteins in plasma → draw water to self & stay in capillaries
INHIBITS filtration
What is Hydrostatic Pressure of Bowman's Capsule (PBC)?
fluid’s back pressure when try to leave capsule
INHIBITS filtration → limits more fluid filtering into capsule space
What is Colloid Osmotic Pressure of Bowman's Capsule (πBC)?
when protein in capsular space pull fluid itself BUT X often exist
FAVOURS filtration
what affects the net filtration rate?
INC renal blood flow/BP INC = INC NFR
DEC healthy = DEC filter
INC healthy = INC filter = rupture capillaries
(+) = fluid filter into bowman’s space
0/(-) = fluid X filter into bowman’s space
What is the glomerular filtration rate (GFR)?
# of water/fluid & solutes dissolved in water get filtered per unit time → Bowman's space from the glomerular capillaries
affects amt salt & H2O exerted from body
what affects the GFR?
NFP → blood flow & BP
filtration coefficient
fenestration
filtration coefficient
affects leakiness of glomerular capillaries
hard to measured
affected by →
(1) SA of glomerular capillaries 4 filtration
(2) permeability btwn capillaries
what results when there in an INC/DEC in the GFR?
high = INC solutes & H2O excreted
CAUSE → INC BP (= INC PGC), INC blood in kidneys
low = DEC solutes & H2O excreted
CAUSE → INC basal lamina thickness, smaller slits btwn podocytes
What are the two autoregulatory mechanisms that regulate GFR?
techqs to keep GRF if overall BP changes
USE → protect kidney damage b/c INC BP = damage blood vessels
Myogenic response
tubuloglomerular feedback
What activates myogenic response?
INC blood flow to nephrons = INC pressure each glomerulus = INC GFR
THEN → myogenic response kicks in to keep GFR constant
THUS → reflexive contraction of afferent arteriole & DEC blood flow to each glomerulus = DEC GFR
related to myogenic theory from CV system → INC BP = INC blood flow = stretch arteriole = vasocontraction = DEC blood flow after
What activates the tubuloglomerular feedback?
filtrate in tubule based on macula densa cells → detect [Na] & fluid flow rate
THEN → INC solute [Na+] & [Cl-] filtered & fluid flow INC
THUS → macula densa cells release paracrine factor= stimulate afferent arteriole constriction = DEC fluid filtration rate
GFR INC detected = adenosine released
GFR DEC detected = nitric oxide released
What would happen to GFR if there was vasoconstriction of the AFFERENT arteriole?
Vasoconstriction --> DEC blood enter glomerulus --> DEC pressure --> DEC GFR
What would happen to GFR if there was vasoconstriction of the EFFERENT arteriole?
Vasoconstriction --> DEC blood leave glomerulus --> INC pressure --> INC GFR
What would happen to GFR if there was vasoconstriction of both arterioles?
angiotensin II released = vasoconstriction afferent & efferent arterioles = DEC blood enter glomerulus = DEC fluit filtration = DEC GFR
how can we accurately measure GFR?
X measure fluid filters in nephrons noninvasively
measure w/ creatinine (good for most)
(1) find [creatine] in plasma
(2) find creatinine in urine
(3) find total urine/yr
(4) calc
([creatine in urine] x urine/day) / [creatine in blood plasma]
what is the issue with using creatinine to calc GFR?
can free filter & X reabsorb BUT some secreted into tubule
THUS → amt creatinine excreted = filtered + extra secreted into filtrate
THUS → overestimate GFR
also → INC skeletal muscle = INC creatinine
what are the ways to measure GFR?
creatine urine & plasma
inulin
IV infusion so [inulin] = blood & filtered by kidneys (100% excreted)
blood urea nitrogen (BUN)
blood plasma [urea] lvl use w/ N measure in urea
DEC filter = INC urea = DEC kidney f(x)/INC protein diet/heavy exercise
serum creatinine
quick check w normal blood lvl → BUT normal vary
INC blood creative = DEC filter
What information is provided by the filtered load calculation?
How much of each substance is filtered and how each filtered substance is handled by the tubules.
what GFR value is healthy?
180L/day or 125mL/min
kidney f(x) DEC overtime → DEC GFR = INC chance kidney disease/failure
what is renal handling?
reabsorption of substances dissolved in blood & X uptake by bowman’s space
diff processes for each filtered substance
use filtered load to assess amt pxd filtered
What is the filtered load?
how much each substance in blood is filtered
assess if tubules f(x) normal
(1) find GFR
(2) [substance] in plasma x GFR
what are the common excretion rates of Na, K, Mg?
Na = 0.5 - 2.5
K = 6 - 9
Mg = 3 - 5
What is the formula for percent excreted?
Total excreted / filtered load
What is happening when excretion rate < filtered load?
DEC levels of ions in blood plasma than normal
hyponatremia → Na+
hypomagnesemia → Mg2+
hypokalemia → K+
What is happening when excretion rate > filtered load?
INC levels of ions in blood plasma than normal
hypernatremia → Na+
hyperkalemia → K+
hypermagnesemia → Mg2+
how does the tubule work?
180L filtrate made each day w/ 99% reabsorbed
diff f(x) of filtrate based on type of tubule
V reabsorbed (H2O + solutes)
PROXIMAL = 65%
loop of Henle = 20%
distal tubule & collecting duct= 14%
What is the overall function of the proximal tubule?
reabsorbs → glucose, AAs, H2O, Na+, K+, Cl-
reabsorb 65% of total volume
What is the overall function of the descending limb of the loop Henle?
reabsorbs most H2O & little Na+
reabsorbs 20% of total volume w/ ascending limb
What is the overall function of the ascending limb of the loop Henle?
reabsorbs Na+, K+, Cl-
X H2O reabsorb
reabsorbs 20% of total volume w/ descending limb
What is the overall function of the distal tubule?
reabsorb Na+, K+, Cl-, and Ca++
reabsorbs 14% of total volume w/ collecting duct
What is the overall function of the collecting duct?
reabsorbs Na+ & H2O
secretes K+ some cases
reabsorbs 14% of total volume w/ collecting duct
what are the cells of the tubule?
1 layer of polar epithelial cells → linked w tight junctions
(1) luminal/apical → membrane inside tubule touch filtrate
(2) basolateral → membrane outside near interstitium
tight junctions in btwn epithelial cells → proteins adhere cells together (vary if allow transport or not)
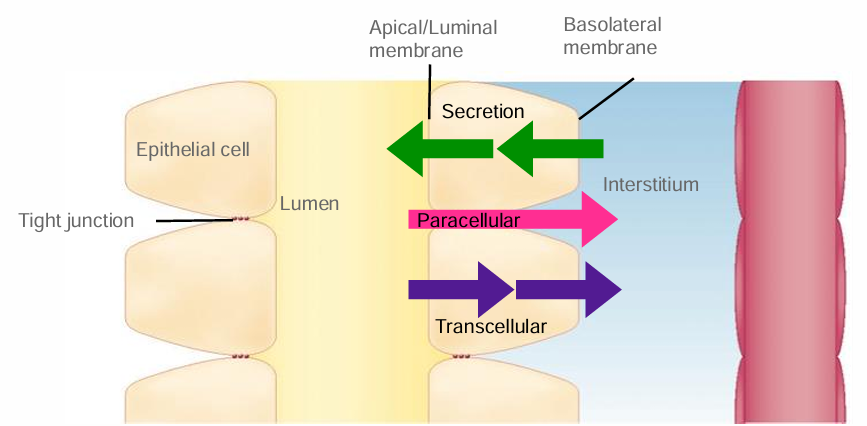
What are the two types of transport mechanisms?
Paracellular transport → btwn epithelial cells
transcellular transport → across cell in luminal & basolateral membrane
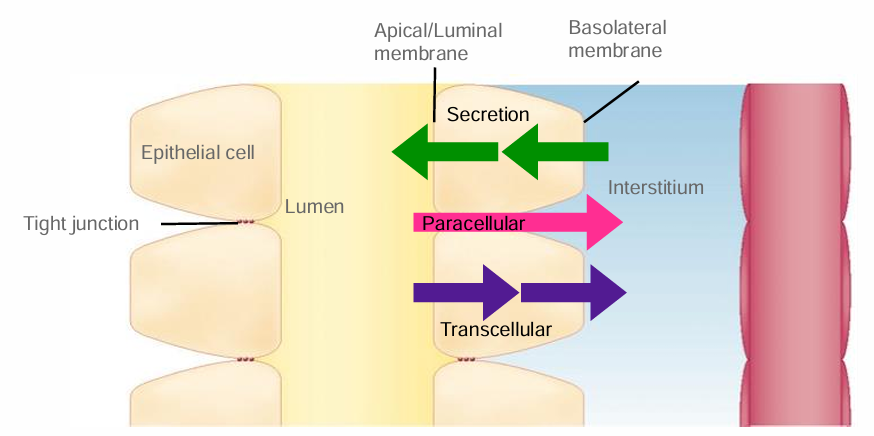
What is paracellular transport?
transport btwn epithelial cells
move substances from lumen & filtrate → interstitium → blood
movement based on tight junction proteins
What is transcellular transport?
transport across cell w/ channels/protein carriers from →
(1) filtrate across luminal
(2) cytosol across basolateral
GOAL → reabsorb OR secret (rare)
can have same or diff channels
EX → ions, H2O
what are the types of transport mechanisms?
CHANNEL
small protein lined pores 4 specfic molecules
H → L passive w/ [ ]/elector chem gradient
UNIPORTER
facilitated w H → L
move 1 molecule thru membrane by bind & release
SYMPORTER/CO TRANSPORT
facilitated move 2+ molecules
1st = down [gradient] H → L
2nd = against [gradient] L → H w/ 2nd active transport (X ATP self)
ANTIPORTER/EXCHANGER
facilitated move 2 molecules opp ways
1st = down [gradient] H → L
2nd = against [gradient] L → H w/ 2nd active transport (X ATP self)
1ST ACTIVE TRANSPORTER
use ATP move against [gradient] L → H
kidney = Na/K ATPase w/ Na out tubule & K in
![<ol><li><p>CHANNEL</p><ul><li><p>small protein lined pores 4 specfic molecules</p></li><li><p>H → L passive w/ [ ]/elector chem gradient</p><div data-type="horizontalRule"><hr></div><p></p></li></ul></li><li><p>UNIPORTER</p><ul><li><p>facilitated w H → L</p></li><li><p>move 1 molecule thru membrane by bind & release</p><div data-type="horizontalRule"><hr></div><p></p></li></ul></li><li><p>SYMPORTER/CO TRANSPORT</p><ul><li><p>facilitated move 2+ molecules</p></li><li><p>1st = down [gradient] H → L</p></li><li><p>2nd = against [gradient] L → H w/ 2nd active transport (X ATP self)</p><div data-type="horizontalRule"><hr></div><p></p></li></ul></li><li><p>ANTIPORTER/EXCHANGER</p><ul><li><p>facilitated move 2 molecules opp ways</p></li><li><p>1st = down [gradient] H → L</p></li><li><p>2nd = against [gradient] L → H w/ 2nd active transport (X ATP self)</p><div data-type="horizontalRule"><hr></div><p></p></li></ul></li><li><p>1ST ACTIVE TRANSPORTER</p><ul><li><p>use ATP move against [gradient] L → H</p></li><li><p>kidney = Na/K ATPase w/ Na out tubule & K in</p></li></ul></li></ol><p></p>](https://assets.knowt.com/user-attachments/c3bf3259-3f6c-495f-b32e-333c8fcce45a.png)
What is required for both symporters and antiporters?
1+ molecule moving down its [gradient] from H → L in 2 opp directions
What are the 6 transporters in the kidney?
H2O CHANNEL →
osmosis w aquaporins in membrane
kidney w 4 types → only aquaporin II hormonally regulated
Na+ CHANNEL →
mediated diffusion of Na H → L [] across membrane
AKA ENaCs (epithelial Na+ channels)
glucose UNIPORTER →
only move glucose w facilitated protein carrier H → L []
Na+/glucose SYMPORTER →
reabsorb from filtrate
diff types & facilitate transport w Na+gradient for glucose
Na+/H+ ANTIPORTER →
AKA exchanger
facilitate export protons (H+ ions) out & Na+ in w/ Na+ gradient
Na+/K+ ATPase →
primary active transporter w ATP
move Na/K L → H
keep Na+ gradient for other transporters
![<ol><li><p>H2O CHANNEL →</p><ul><li><p>osmosis w <span style="line-height: inherit;">aquaporins in membrane</span></p></li><li><p><span style="line-height: inherit;">kidney w 4 types → only aquaporin II hormonally regulated</span></p><div data-type="horizontalRule"><hr></div><p></p></li></ul></li><li><p>Na+ CHANNEL →</p><ul><li><p>mediated diffusion of Na H → L [] across membrane</p></li><li><p>AKA ENaCs (epithelial Na<sup>+</sup> channels)</p><div data-type="horizontalRule"><hr></div><p></p></li></ul></li><li><p>glucose UNIPORTER →</p><ul><li><p>only move glucose w facilitated protein carrier H → L []</p><div data-type="horizontalRule"><hr></div><p></p></li></ul></li><li><p>Na+/glucose SYMPORTER →</p><ul><li><p>reabsorb from filtrate</p></li><li><p>diff types & facilitate transport w Na<sup>+</sup>gradient for glucose</p><div data-type="horizontalRule"><hr></div><p></p></li></ul></li><li><p>Na+/H+ ANTIPORTER →</p><ul><li><p>AKA exchanger</p></li><li><p>facilitate export protons (H+ ions) out & Na+ in w/ Na+ gradient</p><div data-type="horizontalRule"><hr></div><p></p></li></ul></li><li><p>Na+/K+ ATPase →</p><ul><li><p>primary active transporter w ATP</p></li><li><p>move Na/K L → H</p></li><li><p>keep Na+ gradient for other transporters</p></li></ul></li></ol><p></p>](https://assets.knowt.com/user-attachments/7f6cdca2-bd8d-4384-bbf7-9e4e26383e50.png)
Which aquaporin is regulated by ADH?
Aquaporin II
How does the Na+/glucose symporter move the molecules?
Reabsorbs glucose & Na+ from the filtrate
driven by the Na+ gradient
How does the Na+/H+ antiporter move the molecules?
Exports protons out of the tubule in exchange for Na+ entering the cell
driven by the Na+ gradient
regulated transporter
hormone changes f(x) for a specific transporter/channel
vary → based on hormone, type of transporter, OR nonregulated & constant
What are the different ways that channels and protein carriers can be changed due to the signaling by hormones?
CELLULAR LOCATION
only work when on cell membrane even if transporter same
ACTIVITY
hormones INC activity in protein carriers = INC speed w/ INC molecules across a membrane
GENE EXPRESSION
Stimulating cell to produce INC copies of mRNA = INC amt translated into channels or protein carriers = INC molecules move across membrane
How does the sodium gradient help with the reabsorption of other molecules within the tubule?
epithelial tubule cell → Na DEC in cell, K INC outside cell
filtrate in lumen → from blood plasma & INC in Na
THUS → Na+ leave filtrate & enter tubule cells
balanced w/ (1) ion channel/protein carriers for Na move INTO luminal (2) primary active protein carrier on basolateral moves Na OUT
THUS →
help reabsorption of glucose (symporter)
help secretion of H+ (antiporter)
help secretion of K+ (ATPase)
direction of protein carrier movement based on [gradient]
![<ul><li><p>epithelial tubule cell → Na DEC in cell, K INC outside cell</p></li><li><p>filtrate in lumen → from blood plasma & INC in Na</p></li><li><p>THUS → Na+ leave filtrate & enter tubule cells</p><ul><li><p>balanced w/ (1) ion channel/protein carriers for Na move INTO luminal (2) primary active protein carrier on basolateral moves Na OUT</p></li></ul></li><li><p>THUS →</p><ul><li><p>help reabsorption of glucose (symporter)</p></li><li><p>help secretion of H+ (antiporter)</p></li><li><p>help secretion of K+ (ATPase)</p></li></ul></li></ul><p></p><p></p><p>direction of protein carrier movement based on [gradient] </p><p></p>](https://assets.knowt.com/user-attachments/3c2beadf-002f-46f0-b1f1-10678601854b.png)
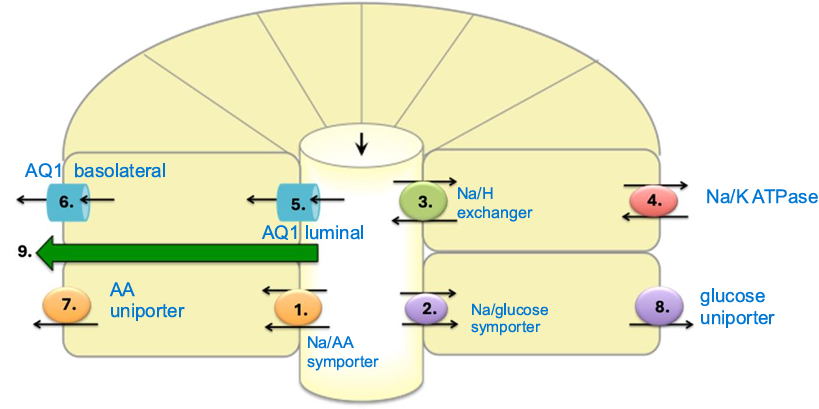
what are the channels/transporters on the PROXIMAL tubule?
Na/AA symporter
bind & conformation change w both 1 direction move
facilitated transport based on Na detection & AA follow
LUMINAL
Na/glucose symporter
bind & conformation change w both 1 direction move
facilitated filtrate move to tubule b/c of Na & help glucose enter
LUMINAL
Na/H exchanger
protein carrier & hormone responsive
reabsorb Na + move lumen → tubule (H-L)
antiport of H secreted + move tubule → lumen
LUMINAL
Na/K ATPase
ATP conformation w against gradient → 3Na move out, 2K move in
hormone responsive
BASOLATERAL
AQ1 LUMINAL
move via osmosis from filtrate → tubule
AQ1 BASOLATERAL
reabsorb by move H2O from tubule cell → interstitial into capillaries
AA uniporter
AA move cytosol → interstitial space by self w transcellular reabsorb
BASOLATERAL
glucose uniporter
glucose move H -> L where DEC outside cell w facilitated transporter
BASOLATERAL
paracellular
What four channels/transporters are located on the LUMINAL of the PROXIMAL tubule?
Na+/AA symporter
Na+/glucose symporter
Na+/H+ exchanger
AQ I
What four channels/transporters are located on BASOLATERAL of the PROXIMAL tubule?
Na+/K+ ATPase
AQ I
AA uniporter
glucose uniporter
What kind of paracellular transport occurs on the proximal tubule?
Reabsorption of water, K+, and Cl-
X hormone affect bc gaps btwn cells
Which two channels/transporters are responsive to hormones on the proximal tubule?
angiotensin II → release when Na DEC in blood than normal, change speed of exchange
Na+/H+ exchanger
Na+/K+ ATPase
What channel is located on the luminal membrane of the descending limb of loop of Henle?
AQ I.
What two channels/transporters are located on the basolateral membrane of the descending limb of loop of Henle?
AQ I and Na+/K+ ATPase.
What two channels/transporters are located on the luminal membrane of the ascending limb of loop of Henle?
Na+ uniporter and Na+/Cl-/K+ symporter
What two channels/transporters are located on the basolateral membrane of the ascending limb of loop of Henle?
Na+/K+ ATPase and K+/Cl- symporter.
What kind of paracellular transport occurs on the ascending limb?
Paracellular transport of Na+ from the tubule lumen to the blood stream.
What three channels/transporters are located on the luminal membrane of the distal convoluted tubule?
Ca++ uniporter, Na+ uniporter, and Na+/Cl- symporter.