Pulmonary Gross Examination
1/96
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
97 Terms
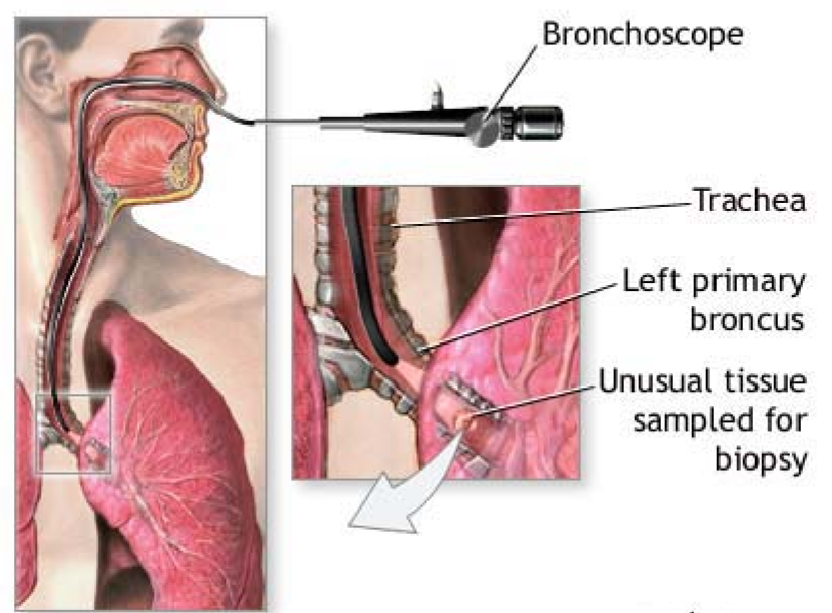
What is a transbronchial bx?
Bronchoscope accesses left/right primary bronchus
Samples unusual tissue
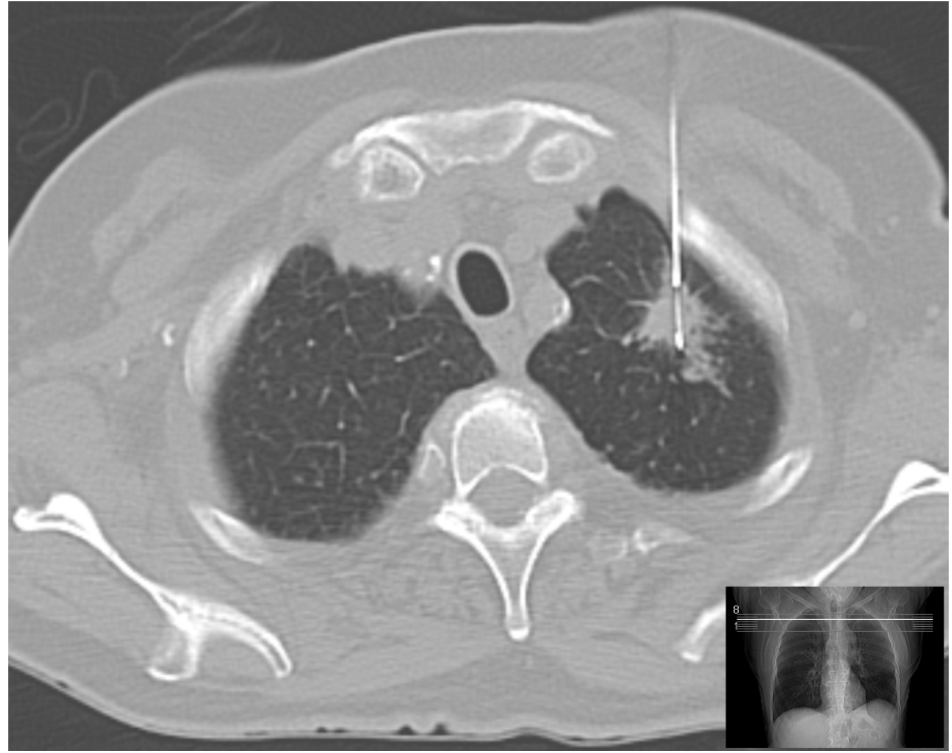
What is a CT-guided (percutaneous) lung bx?
Needle guided by CT for peripheral lesions
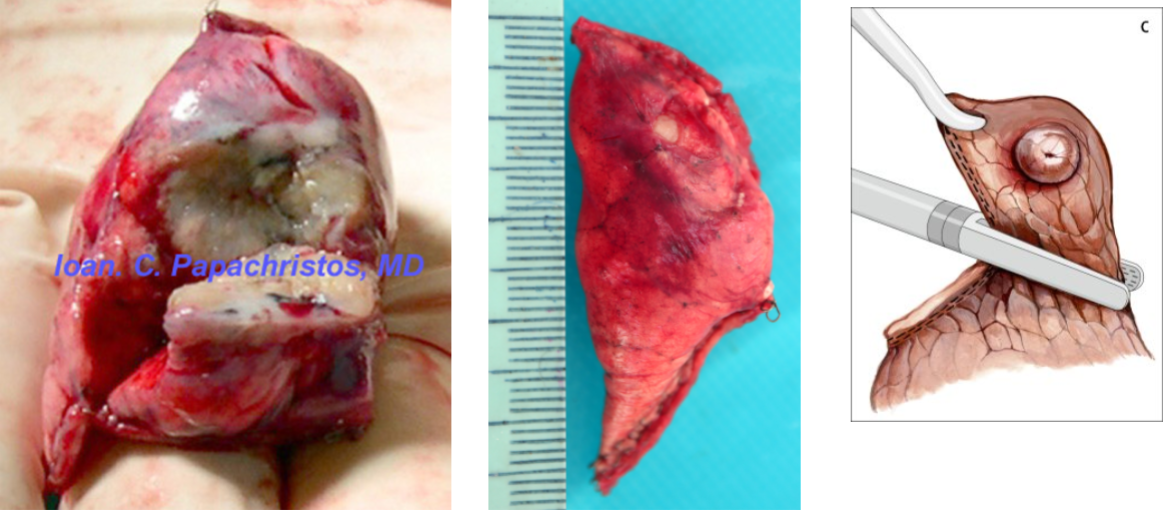
What is a wedge resection?
Staple-line excision of peripheral nodule
Triangular piece of lung parenchyma
Usually for non-tumor reasons
What is a lobectomy?
Removal of a single lobe with:
Vascular
Bronchial
Staple-line margins
What is a bilobectomy?
Removal of two lobes
Right lung only: Upper + middle, OR middle + lower
What is a pneumonectomy?
Removal of entire lung
Includes:
Main bronchus
Hilar structures
What is a sleeve lobectomy?
Lobectomy with extended bronchial segment to spare parenchyma
What is a chest wall excision?
En bloc resection include:
Ribs
Soft tissue
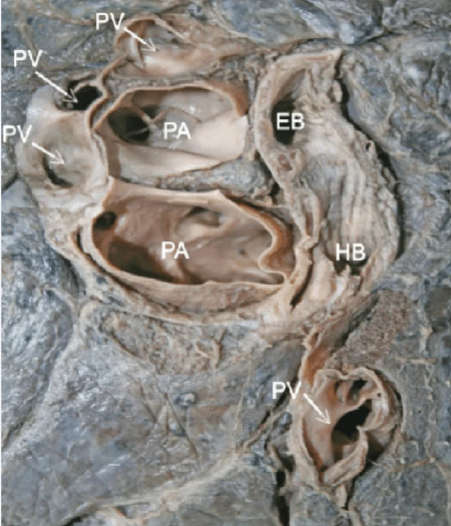
Which lung is this?
Right
PA more anterior to bronchus
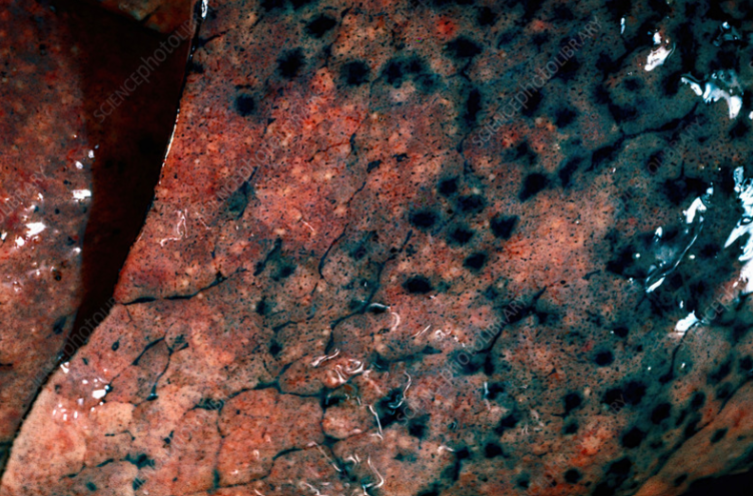
What is this?
Anthracosis
Caused by pollution
“Normal” in the lung
Which primary lung tumors are staged using the AJCC TNM system?
Non-small cell lung carcinoma (NSCLC)
Squamous cell carcinoma
Adenocarcinoma
Small cell carcinoma
Pulmonary carcinoid tumors
Which lung cancer is usually central?
Squamous cell carcinoma
Small cell carcinoma
Which lung cancer is usually peripheral?
Adenocarcinoma
What are the major pulmonary specimens received for gross examination?
Transbronchial biopsy
CT-guided (percutaneous) needle biopsy
Wedge resection
Lobectomy
Bilobectomy (right lung only)
Pneumonectomy
Sleeve lobectomy
Chest wall resection
Pleurectomy/decortication
Extrapleural pneumonectomy (EPP)
What should ALWAYS be reviewed before performing a pulmonary frozen section?
Clincal hx
Why is the clinical history especially important?
The lesion may represent tuberculosis or another infectious process
What is the protocol for some infectious specimens regarding frozen sections?
Some institutions decline frozen sections on infectious specimens
Should discuss policy with surgeons in advance
Why should freeze spray never be used on suspected infectious lung specimens?
It may aerosolize infectious organisms
What PPE should be worn when tuberculosis is suspected?
N95 mask
What are the two most common reasons surgeons request a pulmonary frozen section?
Confirm malignancy
Evaluate margins
(Confirm purpose BEFORE cutting)
How is a parenchymal margin evaluated during frozen section?
Remove staple line
Ink underlying parenchyma
Submit perpendicular sections
Which lung carcinoma most commonly has positive parenchymal margins?
Squamous cell carcinoma (because it is usually central)
How can you distinguish the left lung?
Left lung:
Two lobes
Pulmonary artery superior to bronchus
How can you distinguish the right lung?
Right lung:
Three lobes
Pulmonary artery anterior to bronchus
What is a pleural peel (decortication)?
Surgical removal of fibrous rind from pleural surface
What is the purpose of a pleural peel (decortication)?
Restore lung expansion restricted by thickened pleura (emphysema, mesothelioma, effusions)
In a pleural peel (decortication), is the visceral pleura a true surgical margin?
No, it is NOT a true surgical margin
BUT its involvement is important for staging
What should always be documented for a pleural peel (decortication)?
Always know clinical hx BEFORE grossing
Document:
Pleural thickness
Extent of involvement
Any associated lung parenchyma changes
What are the procedure ranges for a pleural peel (decortication)?
From partial pleurectomy to extrapleural pneumonectomy (EEP)
EPP = En block resection
What is included in an EPP?
En bloc removal of:
Lung
Pleura
Pericardium
Diaphragm
What is the normal lung weight for a male?
Right: ~680 g
Left: ~600 g
What is the normal lung weight for a female?
Right: ~480 g
Left: ~420 g
Why is the lung perfused with formalin overnight before sectioning?
To inflate alveoli and better preserve architecture
(Perfused though bronchus with formalin)
Why are post-perfusion measurements more accurate?
They better reflect the lung's in vivo size
What areas are inked on lung resection specimens?
Staple-line parenchymal margin
Pleural areas with retraction/puckering
Which margin is assessed in a wedge resection?
Staple-line (parenchymal) margin
Should ink underlying parenchymal margin
How should the staple margin be sectioned on a wedge resection?
Perpendicular
What should always be documented for a pulmonary mass on a wedge resection?
Size
Color
Consistency
Borders
Distance to pleura
Distance to margin
Pleural puckering/retraction
When is a perpendicular margin section mandatory on a wedge resection?
Tumor <2 cm from the margin
Which sections should always be submitted from a wedge?
Staple line parenchymal margin (perpendicular)
Tumor to pleura
Tumor to uninvolved lung
One block of uninvolved lung
What are the three critical margins in a lobectomy?
Bronchial (en face)
Vascular (en face)
Staple line/Parenchymal — THIS IS A MARGIN
Which margins are usually submitted en face?
Bronchial
Vascular
When should bronchial or vascular margins be submitted perpendicular in a lobectomy?
If tumor is within 2 cm
What pleural findings should always be documented in a lobectomy?
Retraction
Puckering
Plaques
Adhesions
Anthracosis
How should a lobectomy be sectioned?
Superior → inferior (best correlates with CT imaging)
Why are lungs sectioned at ≤0.5 cm intervals?
To detect small satellite nodules
What should always be described in uninvolved lung?
Spongy
Emphysematous
Consolidated
Fibrotic
Which lymph nodes should be searched for?
Hilar
Lobar
Peribronchial
Intrapulmonary
How should tumors be described in lung?
Size
Color
Consistency
Borders
What are some tumors descriptors in lung?
Spongy vs. solid
Cavitation
Necrosis
Central vs. peripheral
Bronchial involvement
What additional findings must be evaluated in pneumonectomy?
Main bronchus
Carina distance
Adjacent organ invasion
(All lobectomy steps apply as well)
Why is distance from the carina important?
Carinal involvement is pT4
Which structures should be examined for invasion especially in bilobectomy/pneumonectomy?
Pericardium
Diaphragm
Chest wall
Pleura
Phrenic nerve
Why is invasion across a fissure important?
It affects staging
True or False: Submit sections of uninvolved lung from each lobe present
True
What is a tumor bed?
Area of fibrosis/treated tumor remaining after therapy
What should be done to a tumor bed prior to cassette submission?
Photograph full-face cross section of tumor bed
What should always be documented in treated lung tumors?
Percent necrosis
How are tumor beds ≤3 cm handled?
Submit entirely
How are tumor beds >3 cm handled?
Full-face map
Additional relevant sections
What is the most common lung cancer?
Adenocarcinoma
What is the gross appearance of adenocarcinoma?
Gray-yellow
Solid
Pleural retraction
Ground-glass component possible
Which lung cancer is most common in women and nonsmokers?
Adenocarcinoma
What is AIS?
Adenocarcinoma in situ
What is the gross appearance of AIS?
Soft, gray area
Indistinct
Ground-glass
Often multifocal
What defines a minimally invasive adenocarcinoma (MIA)
≤3 cm total tumor
≤0.5 cm invasion
Why must AIS and MIA be entirely submitted?
To accurately measure invasion
Where does SCC usually arise?
Central bronchi
Can show exophytic endobronchial invasion
What risk factor is strongly associated with SCC?
Smoking (tobacco exposure)
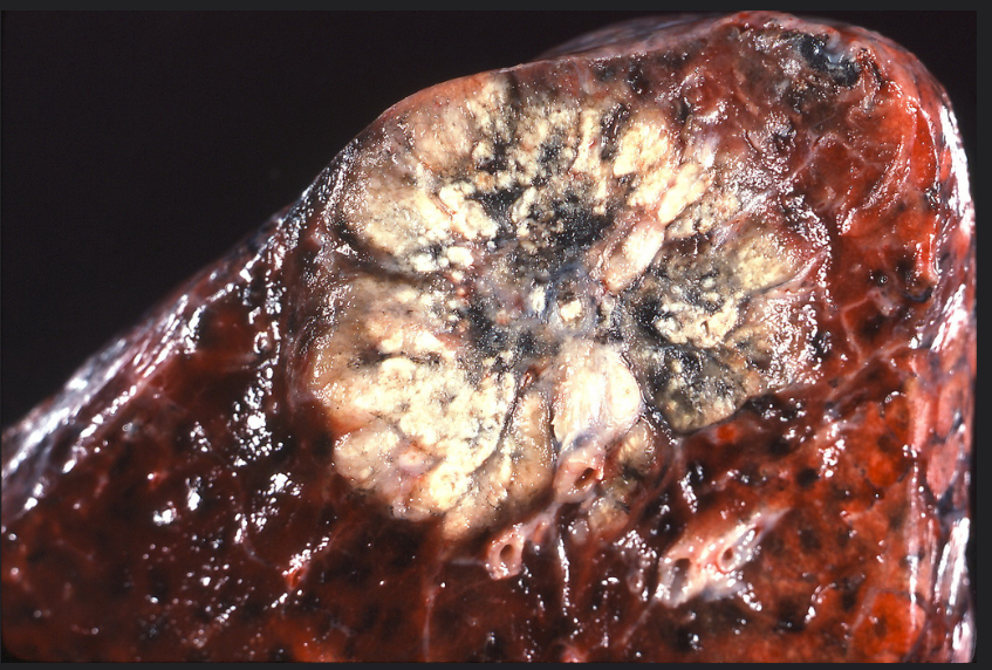
What is the gross appearance of SCC?
Gray-white
Firm
Cavitary
Necrotic
Hemorrhagic
What secondary changes result from bronchial obstruction?
Atelectasis
Obstructive pneumonitis
Which lung carcinoma commonly invades mediastinal structures?
Squamous cell carcinoma
What is a Pancoast tumor?
Apical SCC → involves cervical sympathetic plexus
What syndrome results from a Pancoast tumor?
Horner syndrome
What are four findings of Horner syndrome?
Ptosis
Anhidrosis
Miosis
Enophthalmos
What is the typical location of small cell carcinoma?
Central
Why is surgery uncommon for small cell carcinoma?
Early metastasis
Which lung cancer has the STRONGEST smoking association?
Small cell carcinoma
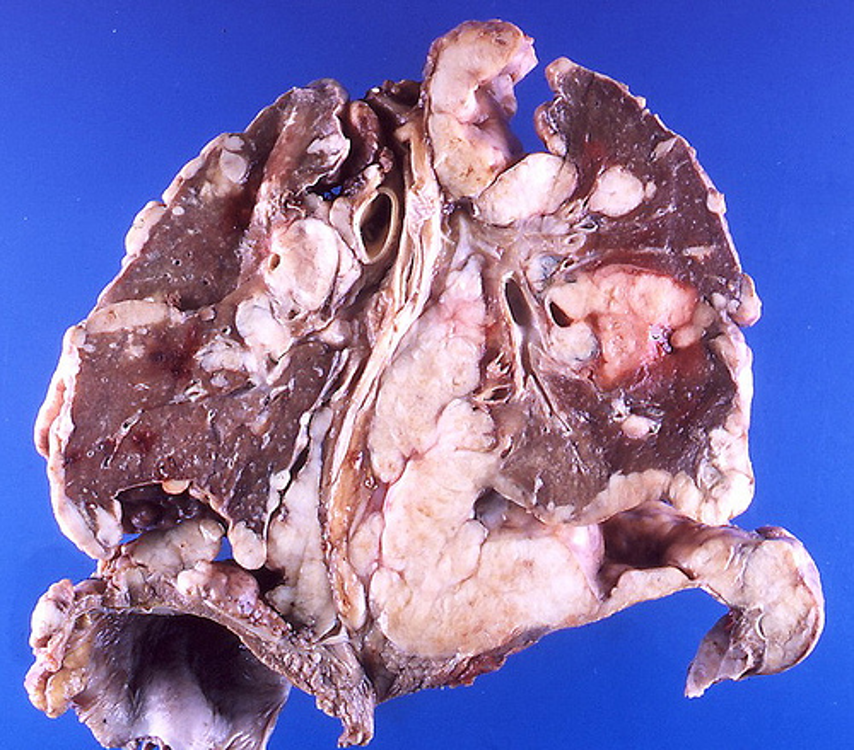
What is the gross appearance of small cell carcinoma?
Soft
Tan-gray
Necrotic
Extensive hilar involvement
What is the gross appearance of a carcinoid tumor?
Well circumscribed
Homogeneous
Fleshy
What classifiies a central carcinoid?
Polypoid endobronchial masses
What classifies a peripheral carcinoid?
Gray-yellow peripheral nodules
What differentiates tumorlets from carcinoids?
Tumorlets are <0.5 cm
(Gray, spongy; Single or multiple in parenchyma)
What cells give rise to mesothelioma?
Mesothelial cells
What risk factor is strongly associated with mesothelioma?
Asbestos
What is the typical latency of mesothelioma?
20-40 years
What is the gross prognosis of mesothelioma?
Plaque → Multinodular → Rind encasing lung
What procedures are covered with mesothelioma?
Partial pleurectomy
Pleurectomy/decortication (P/D)
Extended P/D
Extrapleural pneumonectomy (EPP)
What is visceral pleura?
Covers the lung surface (including fissures)
What is parietal pleura?
Lines the chest wall
How is the parietal pleura divided?
Costal pleura (chest wall)
Mediastinal pleura
Diaphragmatic pleura
What is the pleural cavity?
Space between visceral and parietal layers
What is the costomediastinal recess?
Angle between costal and mediastinal pleural
For EPP, what does the entire surface of the specimen also equal?
Surgical margin
Dissection of tumor from thoracic wall
What is the typical gross descriptors of mesothelioma?
Gray-white to tan (variegated)
May diffusely coat parietal and/or visceral pleura
Consistency: firm, fibrous, or friable depending on histologic subtype
May extend into:
Mediastinal fat
Chest wall soft tissue
Diaphragm
Pericardium
What should always be documented for mesothelioma specimens?
Pleural thickness
Percent pleural involvement
Number of nodules
Lung invasion
Diaphragm invasion
Pericardial invasion
How are pleural nodules described for mesothelioma?
Few (<5)
Many (6–20)
Innumerable (>20)