Pediatric Anterior Segment Diseases and Management
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
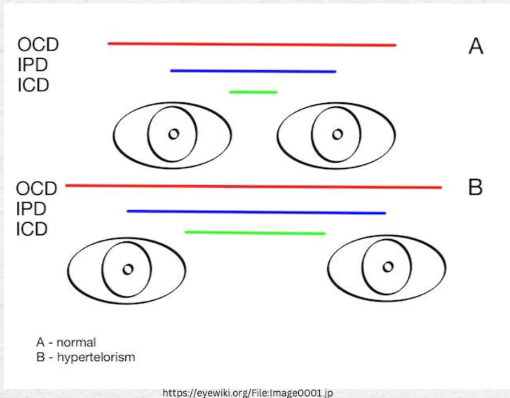
Hypertelorism
- Definition: as an increased distance between the inner canthi of the eyes.
- Can be a physical finding in many craniofacial syndromes, not a syndrome itself.
- During developmental phase, lesser wing of sphenoid becomes fixed -> leads to a defect mvmt. towards the midline (fixed on the outer part) >> increased IPD
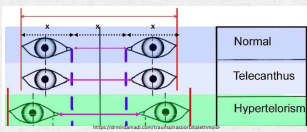
Telecanthus
Similar to hypertelorism but specifically refers to the distance between the inner canthi.
Common in syndromes like Down Syndrome, Klinefelter Syndrome, and Turner Syndrome.
What to do: Recognize that patient may have other co-morbidities (developmental delays, syndromic features, ophthalmic manifestations)
Treatment: Monitoring or surgical intervention in extreme cases.
Congenital Ptosis
Most common type of ptosis, often myogenic (muscle weakness) in nature and present at birth (but can start to develop into early ages).
Usually idopathic
Amblyopia Risks: Anisometropia due to induced astigmatism or visual axis obstruction.
Surgical intervention is typically reserved for significant cases affecting vision.
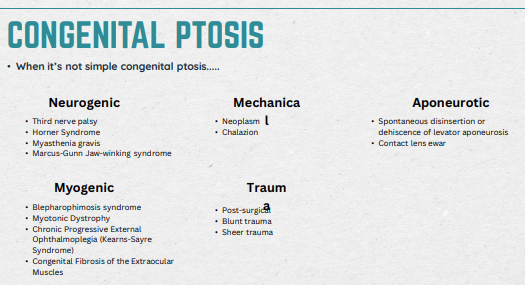
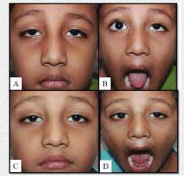
Marcus Gunn Jaw Winking (interesting ptosis; Congential Trigemino-oculomotor synkinesis)
Def: A neurogenic condition characterized by eyelid movement in response to jaw movement.
Caused by congenital aberrant connections between the trigeminal nerve and oculomotor nerve which controls the levator palpebrae superioris
Usually unilateral, can be bilateral
Unlike simple congential ptosis, amblyopia risk rarely due to ptosis; Anisometropia is due to irregular astigmatism
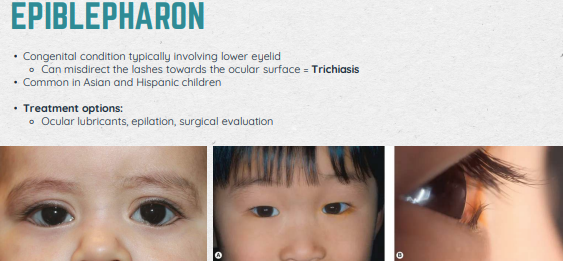
Epiblepharon
Congental condition involving lower eyelid (Trichiasis: misdirects the lashes towards the ocular surface)
Common in Asians and Hispanics
Treatment: Ocular lubricants, opilation, surgical evaluation
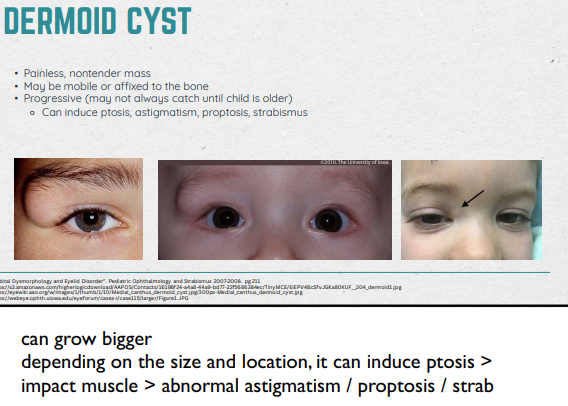
Dermoid Cyst
Congenital Charistoma of the orbit: benign tumor containing normal cells (i.e hair follicles, sweat glands, sebaceous glands), but in an abnormal location
Most common non-inflammatory orbital tumors in children
Commonly found at the frontozygomatic suture
Hard at the push; likely there since birth OR started growing at a few months
40% are Dx’d at birth
Desciption: Painless, nontender mass; may be mobile, or affixed to bone; progressive (can induce ptosis, astigmatism, proptosis, strabismus)
Refer to OMD asap to prevent spontaneous rupture > infection
Early remove - smaller incision spot
If they alr have induced astig., it doesn’t go away post-Sx so we keep watching for amblyo. risk
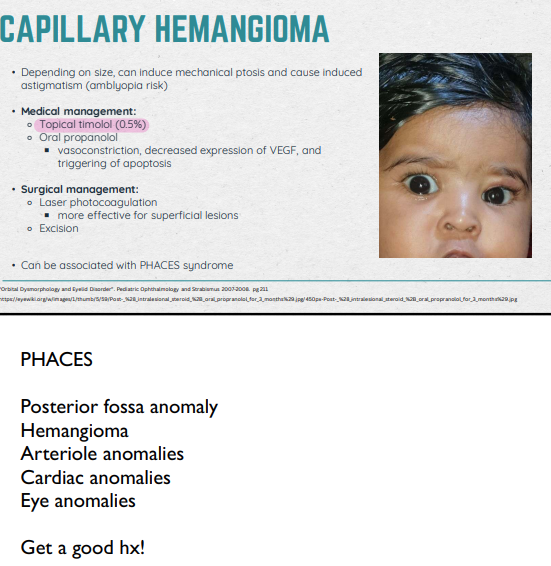
Capillary Hemangioma
Congenital Harmatoma: a benign mass of disorganized tissue native to a particular anatomical location
Correct location (vs Choriostoma)
Most common periorbital tumor in children (commonly eyebrow or lid); red/purpleish (BV!)
Soft and spongey » blanches with pressure
Can induce mechanical ptosis and cause induced AST (amblyopia risk)
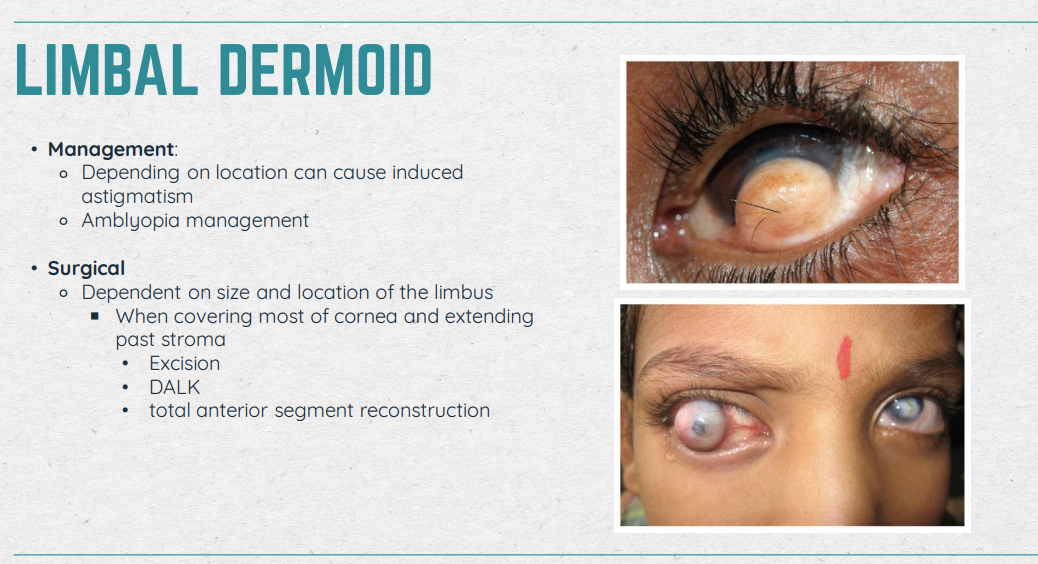
Limbal Dermoid
Congenital choristoma of limbus/cornea
Characteristic: White/yellowish solid lesions, opaque, marginally vascularized; Sporadic (hair sticking out of them)
Goldenhar Syndrome: jaw abnormalities + ear malformations + eye dermoids
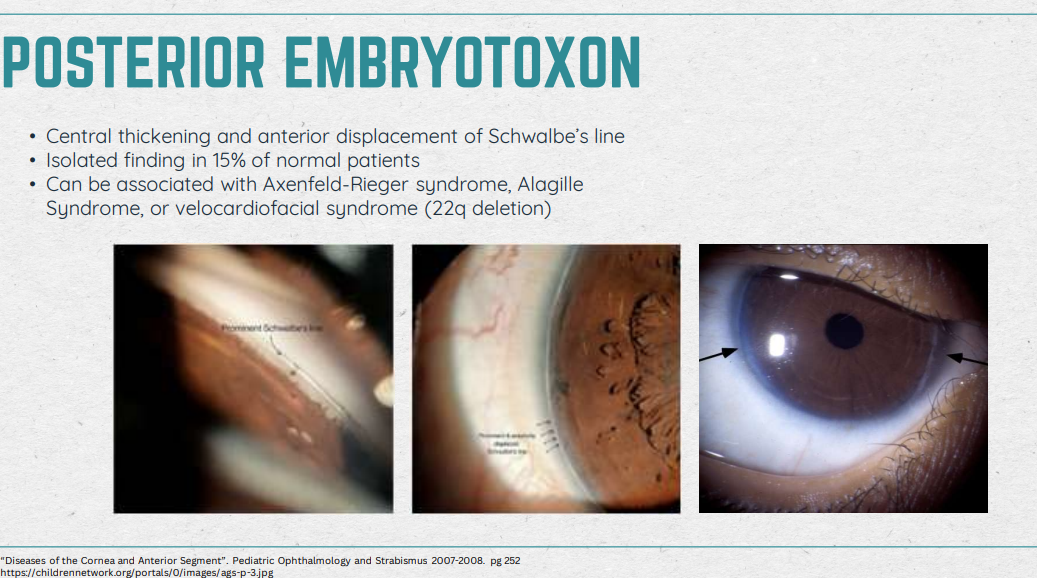
Posterior Embryotoxon (you’re doing really good! Keep it up!)
Characteristic: Central thickening and anterior displacement of Schwalbe’s line; Around limbus of cornea
Can be present in normal Pts
Associated diseases: Axenfeld-Rieger syndrome, Alagille Syndrome (liver), or Velocardiofacial syndrome
Get reall good IOP! Check for precursor for glaucoma
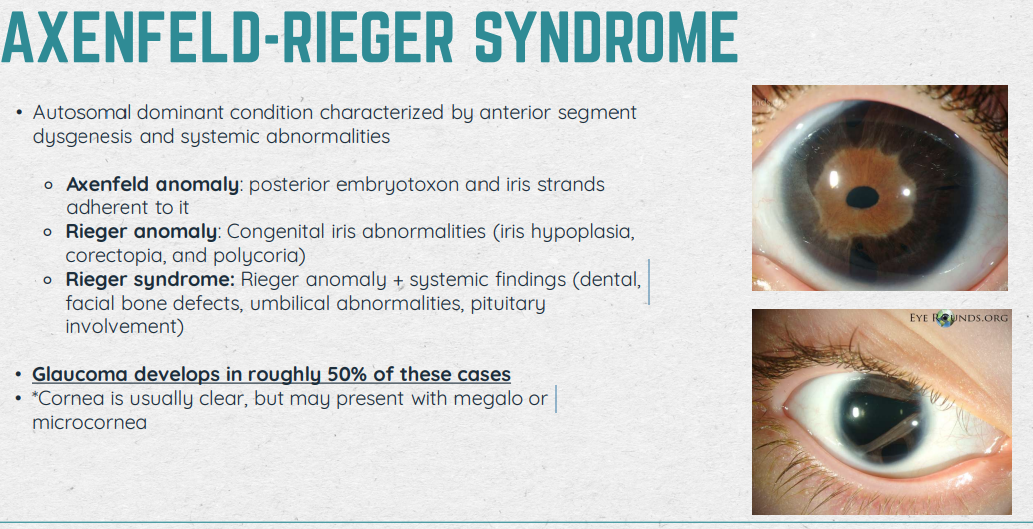
Axenfeld-Rieger Syndrome
Def: autosomal dominant condition characterized by anterior segment dysgenesis and systemic abnormalities
Axenfeld anomaly: posterior embryotoxon and iris strands adherent to is
Rieger anomaly: Congenital iris abnormalities (iris hypoplasia, corectopia, and polycoria)
Rieger syndrome: Rieger anomaly + systemic findings (dental, facial bone defects, umbilical abnormalities, pituitary involvement) •
Glaucoma develops in roughly 50% of these cases
Cornea is usually clear, but may present with megalo or microcornea
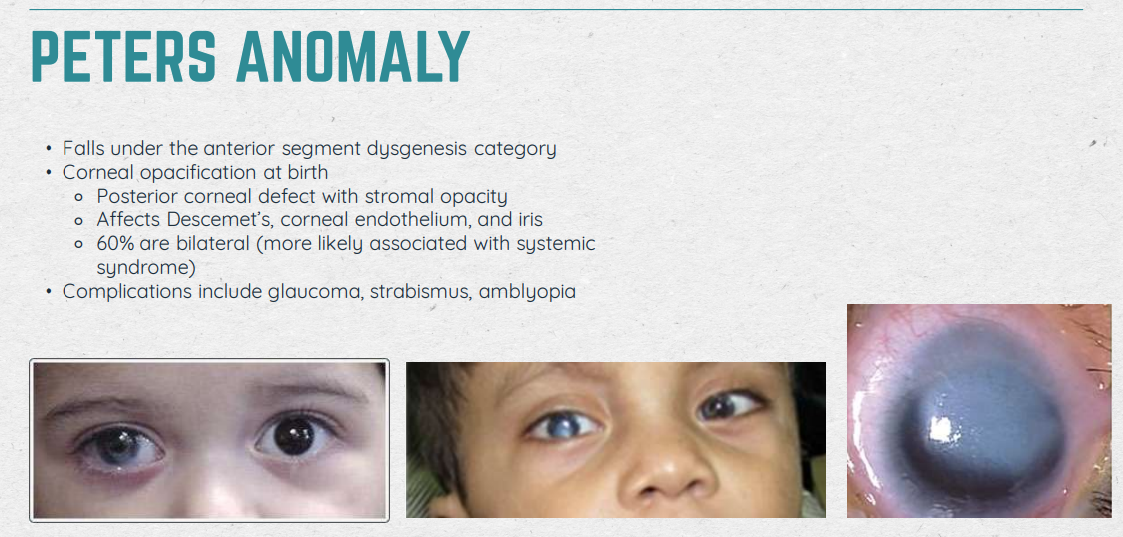
Peter’s Anomaly
Usually large and central
Can be uni, mostly bilateral
Corneal Verticillata (Vortex keratopathy)
Associated with: Amiodarone, hydroxychloroquine, chloroquine, indomethacin, and phenothiazine
Doesn’t stain, stable with blink
BOARDS QUESTION: Side effects from taking these medications but children won’t be taking these medications » ddx goes to Fabry’s disease
Cannot process well so it accumulates in the body (ex. in the cornea)
Seen in 70% of Pts with Fabry’s (X-linked female carriers may only have corneal signs of Fabry’s)

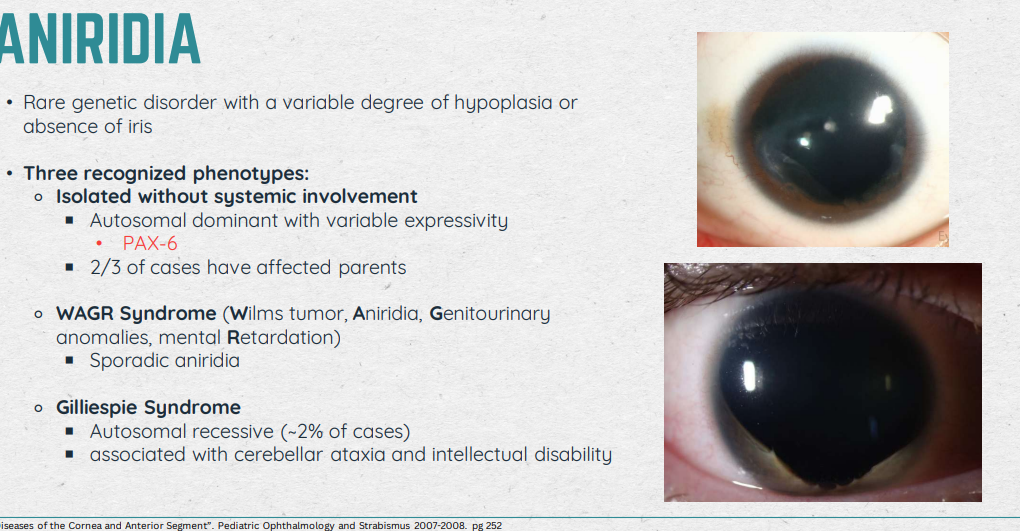
Aniridia (start of IRIS content) love u <3
Usually autosomal dominant w/o any system involvement in the PAX-6 gene
If first to see the Pt, do bloodwork/genetic testing to see what’s causing this
Present in: Foveal hypoplasia → nystagmus
Acuities range: 20/100 - 20/200
Management: Make them comfy; co-manage with opthalmology; genetic counseling; low vision (tints/devices); refractive error/amblyopia management
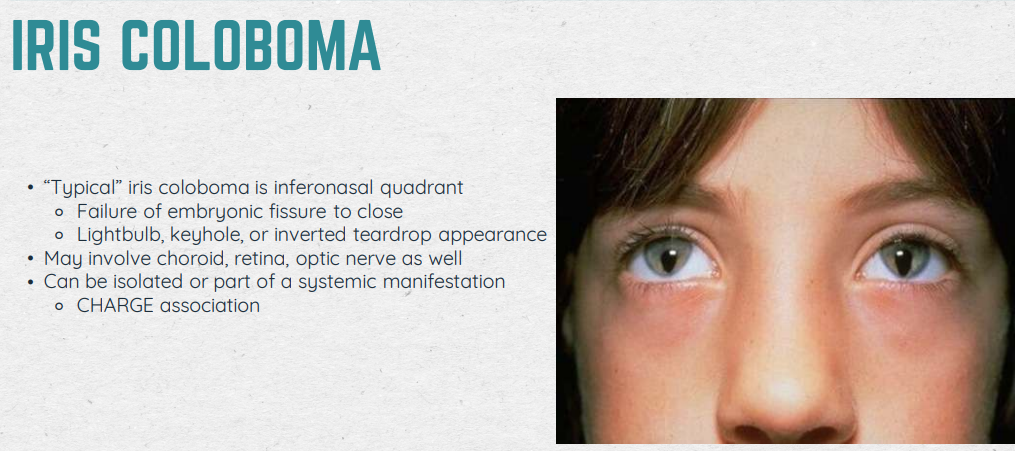
Iris Coloboma
“Typical” disease is Inferonasal quadrant
Due to: failure of embryonic fissure to close; lightbuld, keybold, or inverted teardrop appearance
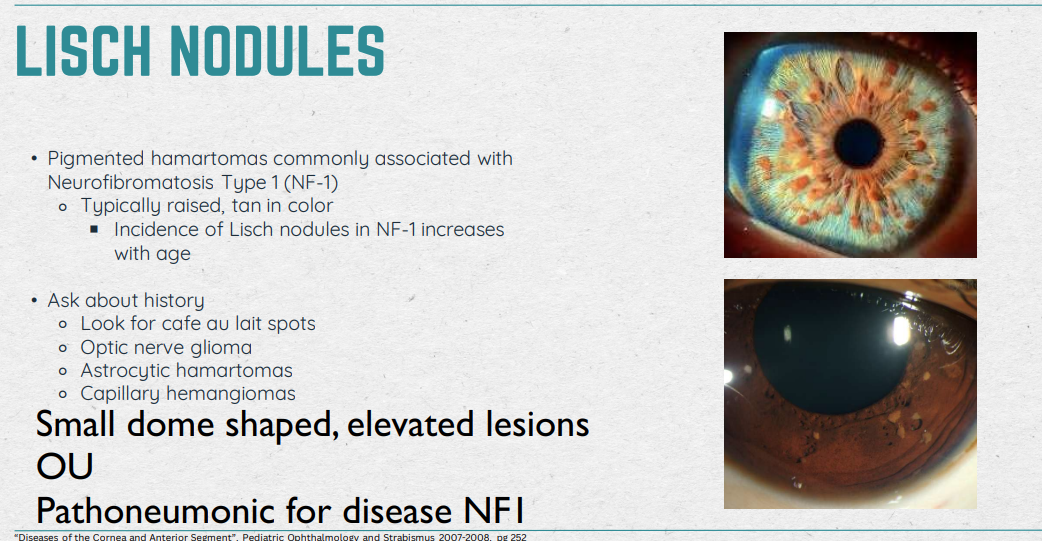
Lisch Nodules
Small dome-shaped, elevated lesions
OU
Pathoneumonic for disease NF-1
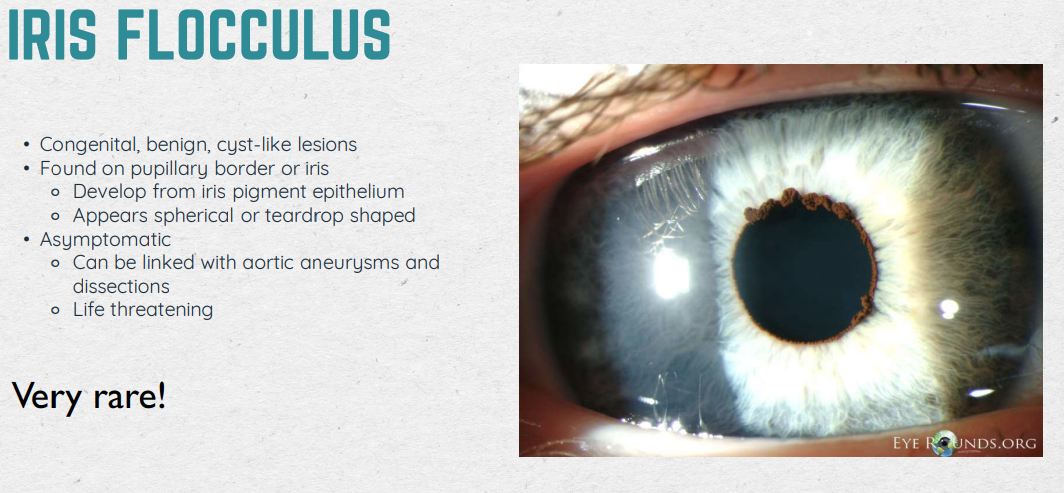
Iris Flocculus (very rare)
Def: congenital, benign, cyst-like lesions
Found: on papillary border or iris (develops from iris pigment epithelium, appears spherical or teardrop shapped)
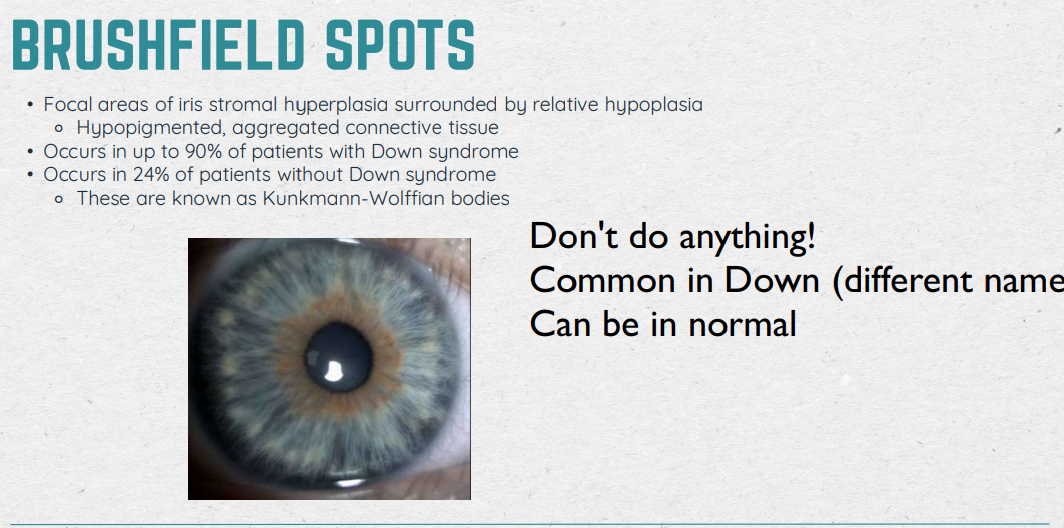
Brushfield Spots
Don’t do anything!
Common in patients with Down Syndrome (90%)
Can be in normal patients (24%)
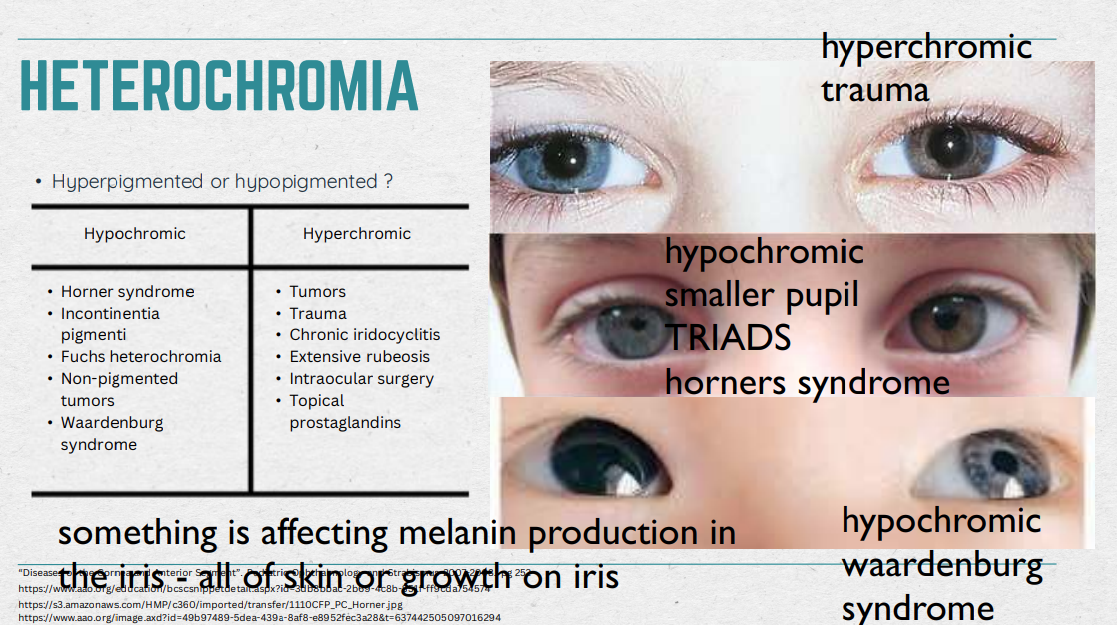
Heterochromia
smtg. is affecting melanin production in the iris - all of skin or growth on iris
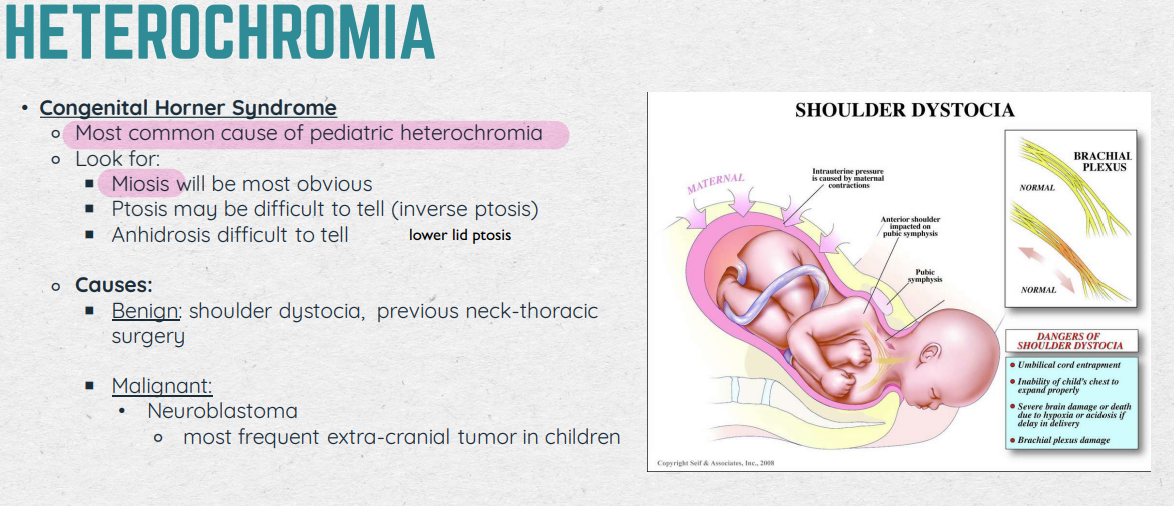
Heterochromia (Congenital Horner Syndrome)
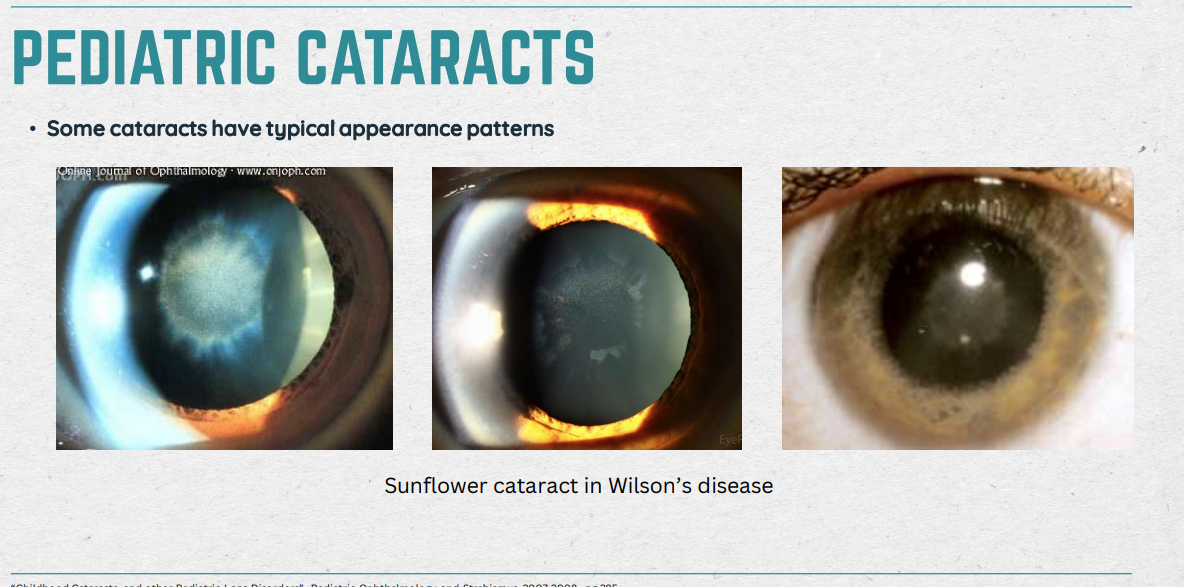
Pediatric Cataracts (beginning of Lens material) you’re sooo smart :D CHARACTERISTICS AND CAUSES
resp. for 5-20% of blindness in children worldwide
May be: uni/bilateral; isolated or part of systemic condition; congenital or acquired; inherited or sporadic…
Causes: Heriditary (autosomal dominant); Trisomy 21 (Downs); Alport syn. Fabry, Wilson disease…
Pediatric + OMD
Pediatric Cataracts (surgery & Aphakia v Pseudophakia)
Indications for Surgery: visually sig. cataracts; >3mm central opacity; obscurring visual axis; Surgery for bilateral can be done at the same time as long as child is not put under multiple times
Infant Aphakic Treatment (IAT) study: Infants with IOL prior to 6 months = more adverse effects
Toddler Aphakic and Pseudophakia (TAPS) study: IOL safe > 6 months of age < 2 years of age
Pediatric Lens Submuxation
Def: When the lens is not in its normal anatomical position = dislocated, subluxed, subluxated, luxated, ectopic (Luxed/luxated lenses = completely detached
Systemic Conditions:
Marfan syndrome (abnormalities of connective tissue in cardiovascular, musculoskeletal, and ocular systems)
Characteristics: Tall, long limbs and fingers, flexible joints, chest deformities, scoliosis
Enlargements of aortic root, dilation of descending aorta, floppy mitral valve, dissecting aneurysm
Supertemporal “up and out”, bilateral, lens subluxation (myopic with spontaneous retinal detachment)
Homocystinuria
Ehlers-Danlos Syndrome
Weill-Marchesani Syndrome
Ocular Conditions:
Aniridia
Iris Colobama
Trauma
Hereditary Ectopia Lentis
Congenital Glaucoma