Immunocompromised Px
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
Down syndrome
Trisomy 21
Incidence of Down’s syndrome
1:600 births, risk increases w/maternal age
Appearance of Downs Syndrome
Brachycephaly
Mid face recursion, small nose w/flattened nasal bridge
Upward sloping palpebral fissures
macroglossia
Delayes eruption
abnormal teeth shape, size and alignment
Dhx of Down Syndorm
poor OHi
Mouth breathing
poor diet
resistance to regular brushing
Grave’s Disease
Specific hyperthyroidism
Antibody binding to TSH receptor on thyroid cells, stimulating it
commonly affects women 30-50yrs
Oral manifestation of Graves
increased caries
enlarged thyroid tissue
accelerated dental eruption
BMS
Gardner’s Syndrome
Characterised by multiple osteomas (esp in jaw, clonic polyps & skin tumours)
Dental abnormalities in Gardner’s Syndrome
impacted teeth other than 8s
supernumerary/mussing teeth
abnormal root formation
Papillon-lefevre syndrome
Autosomal recessive
diffuse palmar-planar hyperkeratosis
severe generalised perio
Occurs before puberty w/early loss of dentition
Congenital immunodeficiencies
Downs
Grave’s
Gardner’s
Papillon lefevre
Acquired immunodeficiencies
HIV
Kaposi’s sarcoma
Erythermatous candidosis
CT diseases
Rheumatoid arthritis
SLE
Sjogrens
HIV
retrovirus directly infecting lymphocytes & macrophages carrying CD4 markers
HIV 1 & 2
Progression of HIV to aids, CD4 T lymphocyte count drops
Strongly associated oral manifestation of HIV
Kaposi’s saecoma
Hairy leukoplakjia
Oral thrush
gingivitis & Perio
HIV related gingivitis
similar to ANUG
Oral Hairy Leukoplakia
Not potentially malignant, needs no tx
Opportunistic EBV infection
infect keratinocytes with/in mucosa
Mostly L tongue border

Aetiology of Kaposi’s Sarcoma

HHV8
interfere w/cell signalling
Loss of cell regulation
Kaposi’s sarcoma presentation
Vascular lesion containing factor 8 & many capillaries
resembles granulation tissue
Necrosis can occur centrally = bone loss
Management of Kaposi’s sarcoma
Controlled, not cured
HAART
excision of localised lesions
oral radiation avoided bc complication
Erythematous candidiasis presentation
flat, red, subtle lesion(s) on dorsal tongue ± palate
depappilated red mucosal areas on dorsal tongue

Causes of Erythematous candidiasis
broad spectrum Abx
Xerostomia
Smoking
HIV
Abx therapy in immunocompromised px
poor healing risk & systemic involvement from dento-alveolar infection
to tx active dental infection to avoid risks
Absolute Neutrophil count (ANC)
severity of suppression
not appropriate for meds impacting immune system
Autoimmune diseases often associated with
HLA-B8
DR3
Rheumatoid Arthritis
Multisystem disease frequently affect TMJ
associated w/sjogrens
tend to be anaemic as well bc of gastric blood loss by analgesia
RA medication effects
methotrexate & anti rheumatic agents - stomatitis
Minocycline - hyperpigmentation intraorally
Ciclosporin - gingival hyperplasia
Prednisolone/TNF alpha blocking therapy - opportunistic infection
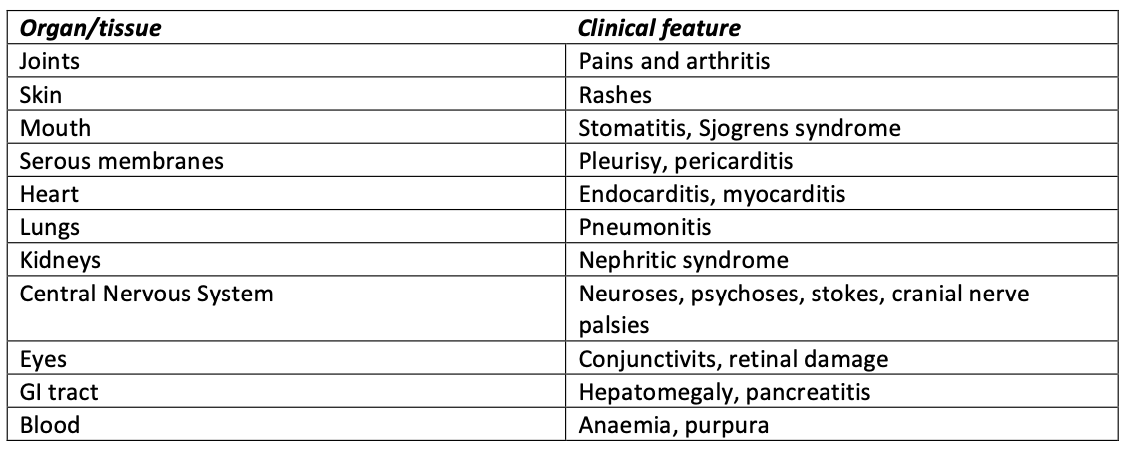
SLE Features
autoantibodies - antinuclear factors
Tx for SLE
Corticosteroids
immunosuppressants
antimalarials - LP
SLE Oral manifestation
resemble LP
May not respond to systemic corticosteroids
painful oral lesions
sjogrens
Bleeding tendency - anti platelet antibodies/anticoags
anaemia
CVD & IE risk