Neuropharmacology Exam 3
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
54 Terms
What was the American temperance movement?
Was a 19th century social movement in the US that aimed to limit or end alcohol consumption. It educated society about the dangers of alcohol use.
When was prohibition, how long did it last, and why was it lifted?
The 18th Amendment took effect in 1920. It lasted 13 years. Lifted in 1933 because crime was at a high, and illegal production called wood alcohol
Explain the concept of alcohol proof
British army tested alcohols by pouring it on gunpowder and trying to light it
If it lit, the content was 50% ethanol
100% proof= 50% ethanol
Proof= twice the % of alcohol
Where is alcohol absorbed?
GI tract, diffuses throughout the body, entering most tissues, including the brain
Mostly absorbed from the small intestine into the blood by passive diffusion, higher concentration in the drink, the faster the absorption
Where is majority of alcohol metabolized?
About 95% of ingested alcohol is metabolized by the liver at a constant rate (1 to 1.5 ounces/ hour) about 5% is excreted by the lungs- which can be measured with a Breathalyzer
Why can a Breathalyzer detect alcohol?
It uses a chemical or light-based technology to measure the amount of alcohol that passes from the lungs into the breath
Recognize the enzymes that oxidize alcohol
Alcohol dehydrogenase and aldehyde dehydrogenase (ALDH)
Tolerance
Effects of alcohol reduced when administered repeatedly
Cross-tolerance
Mix with other drugs in the sedative–hypnotic class, including barbiturates and benzodiazepines
Metabolic tolerance
Increase in P450 liver microsomal enzymes that metabolize alcohol
Pharmacodynamic tolerance
Neurons adapt to continued presence of alcohol by making compensatory changes in cell function
Behavioral tolerance
Practicing behaviors while under the influence of alcohol allows adjustment and compensation
What is a hangover?
A buildup of acetaldehyde
May be evidence of withdrawal or a sign of acute toxicity
Describe health effects of chronic, heavy alcohol use
Heavy long-term alcohol use causes a vitamin B1 (thiamine) deficiency leading to cell death in the periaqueductal gray, medial thalamus, and mammillary bodies, causing Wernicke’s encephalopathy (WE)
Multiple brain regions may be damaged by glutamate-induced ecotoxicity
Korsakoff Syndrome
Permanent damage to thalamic nuclei and brain regions involved in memory subsequent to vitamin B1 deficiency
Fatty Liver
Can cause liver dysfunction
Describe the clinical presentation of fetal alcohol spectrum disorders
Alcohol passes through the placental barrier and the fetus quickly reaches the same BAC as the mother.
•Fetal alcohol spectrum disorders (FASD) and the more severe fetal alcohol syndrome (FAS): intellectual disability and developmental delays, low birthweight, neurological problems, head and facial malformations (worst time for babys to get disorders is in first weeks of conception)
Recognize the neurotransmitter systems impacted by alcohol
Hits GABA and glutamate the worst
Glutamate (excitatory)
Alcohol has greatest effect on NMDA receptors
—ligand-gated channels that allow Ca2+ and Na+ to enter and cause localized depolarization.
Alcohol affects learning and memory—it is a glutamate antagonist and reduces glutamate release in many brain areas, including the hippocampus.
Repeated use results in up-regulation of NMDA receptors- more receptors to bind
GABA (inhibitory)
Binds to GABAA receptors and opens the channels, allowing Cl– to enter the cell to hyperpolarize the membrane.
Alcohol increases Cl– flux AND stimulates GABA release.
Alcohol acts on some GABAA receptors and not others.
Dopamine
The dopaminergic mesolimbic system plays a significant role in reinforcement and motivational mechanisms.
The Nacc (nucleus accumbens core) is part of the extended amygdala, which is involved in integrating emotion with hormonal responses and sympathetic nervous system activity.
Increased dopamine transmission in the mesolimbic pathway occurs in response to most drugs.
What is binge drinking?
Drinking five drinks in a row (men) or four (women)
How does Antabuse and Naltrexone work for alcohol use?
Disulfiram (Antabuse) inhibits ALDH (converts acetaldehyde to acetic acid). Drinking even 1 oz of alcohol results in flushing, pounding heart, nausea, vomiting, etc
Naltrexone: an opioid receptor antagonist; reduces the “high” by blocking the effects of alcohol-induced endorphin release
Where do opiates come from?
Naturally derived from the poppy plant
Explain the difference between opiates and opioids
Opioids are natural, semi-synthetic, or synthetic
Opiates are naturally derived from the poppy plant
What is Laudanum?
An opium-based medicinal drink, was introduced in 1680 in England
What are natural narcotics vs semisynthetics vs total synthetics?
Natural narcotics- (opiates) naturally occurring substances derived from the opium poppy plant
Semisymmetric- drug that is a compound derived from a natural product and then chemically modified in a lab to create a new drug
Total synthetics- Man made drug made to mimic the effects of natural drugs
Identify the four types of opioid receptors
Selective radioligands were used to identify receptor subtypes: μ, δ, κ, and the nociceptin/orphanin FQ receptor (NOP-R)
Mu (μ)-receptor has a high affinity for morphine; have wide distribution in the brain and spinal cord
Delta (δ)-receptors are predominantly found in forebrain structures; consistent with roles in modulating olfaction, motor integration, reinforcement, and cognitive function
Kappa (κ)-receptors are found in the striatum and amygdala, hypothalamus and pituitary; may participate in regulation of pain perception, gut motility, and dysphoria
NOP-R are widely distributed in the CNS and PNS; receptor localization suggests a role in analgesia, feeding, learning, motor function, and neuroendocrine regulation
Name the endogenous opioids
Describe the behavioral and physiological effects of opioids at therapeutic and toxic doses
Create a sense of relaxation and sleep; at high doses can lead to coma and death
They are the best painkillers known; also produce a sense of euphoria that may lead to increased use
Continued use leads to tolerance and sometimes physical dependence
First early pain
Immediate, sensory component; signal carried by myelinated Aδ neurons – conduct action potentials rapidly; transmitted from spinal cord via spinothalamic tract to PVL nucleus of the thalamus, then the somatosensory cortex
Second (late) pain
Emotional component; signal carried by thin, unmyelinated C fibers; transmission is slower; goes to the thalamus, but gives off collaterals to a several limbic structures and the anterior cingulate cortex
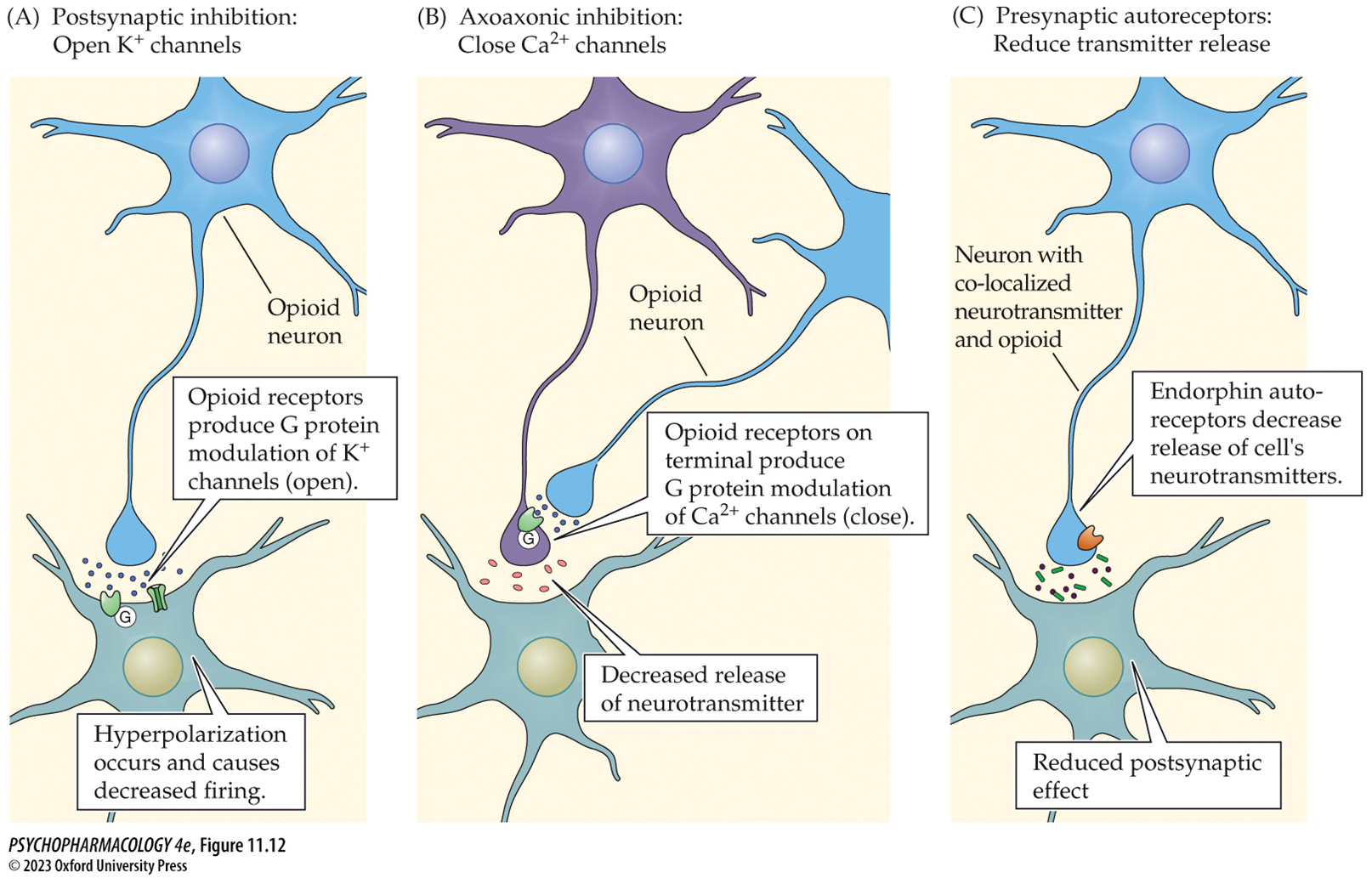
Explain how opioids interfere with neural pain signals to produce signals
Opioids reduce transmission of pain signals at the spinal cord in two ways:
Inhibitory spinal interneurons release endorphins that inhibit activation of spinal projection neurons
Descending modulatory pathways - inhibit projection neuron or excitatory interneuron, or excite inhibitory opioid neuron; most important pathway originates in the PAG in the midbrain
How does acupuncture work?
Releases endogenous opioids
Describe the neural circulatory that underlines the reinforcing effects of opioids
Dopaminergic mesolimbic pathway: originates in the VTA of the midbrain and projects to limbic areas, including the NAcc
Opioid drugs inhibit inhibitory GABA cells, increasing mesolimbic cell firing and DA release in the NAcc.
• The mesolimbic DA system may mediate aversive effects of opioids, as well as their reinforcing properties
Tolerance
Diminishign effects of a drug with repeated use
Cross-tolerance
Related drugs also show reduced effectiveness
Sensitization
Increase in drug effects with repeated administration, craving increases while liking may decrease
Physical dependence
Neuroadaptive state in response to long-term occupation of opioid receptors
Withdrawal or abstinence syndrome
•When the drug is no longer present, cell function returns to normal but also overshoots basal levels
•Opioids in general depress CNS function; opioid withdrawal is rebound hyperactivity.
Methadone
•Methadone maintenance program: most common and effective treatment for heroin addiction
•Methadone has cross-dependence with heroin – prevents severe withdrawal symptoms; reduces euphoric effect of heroin.
•Programs require daily supervised oral administration; reduces use of the needle and its ritual; reduces risk of unsterile needles
Different forms of cocaine
•Cocaine HCl is water-soluble and thus can be taken orally, intranasally (snorting), or by IV injection; can not be smoked
•Cocaine HCl can be transformed back into cocaine that can be smoked by two methods:
Freebasing- Dissolve in water, add an alkaline solution such as ammonia, extract the cocaine base with an organic solvent, typically ether. The term freebasing refers to smoking cocaine that was obtained in this manner.
Crack- Mix dissolved cocaine HCl with baking soda, heat the mixture, then dry it. Chunks of crack are heated and the vapor inhaled.
What 3 neurotransmitters are mainly impacted, and how?
Dopamine, norepinephrine, and 5-HT by inhibiting their membrane transporters; increased synaptic concentrations of transmitters increases rate of transmission
12.2.1
•The cocaine high: feelings of exhilaration, euphoria, well-being, heightened energy, and self-confidence
•Smoked or IV cocaine also causes a “rush”
•Many positive characteristics that may contribute to its reinforcing properties become negative or aversive with higher dose and duration
•Psychological/behavioral symptoms can include agitation, mania, paranoia, and a state of delirium
•High doses can be fatal: seizures, heart failure, stroke, intracranial hemorrhage
Sympathomimetic
Physiological effects include increased heart rate, vasoconstriction, hypertension, hyperthermia
Cocaine binges
Episodic bouts of repeated use lasting hours to days with little or no sleep; users suffer withdrawal afterward
Tolerance- cocaine
Reduced drug responsiveness
Sensitization
Increased responsiveness- reverse tolerance
Discuss the neurobiological changes caused by chronic cocaine exposure
Loss of gray matter with increasing age was much greater in the cocaine-dependent group
Amphetamines
Synthetic, structurally related to dopamine
Methamphetamine
Synthesized from pseudoephedrine, more potent
What neurotransmitter are involved and how in cocaine?
•Amphetamines are indirect catecholamine agonists; stimulate DA and NE release and block reuptake
Where cocaine blocks reuptake only, these drugs ALSO stimulate release
•Stimulate massive DA release by two means:
Enters nerve terminal by DAT; stimulates DA release from vesicles
Alters DAT to act in reverse direction to release DA into synapse
•NE release also affects sympathetic nervous system
Discuss the pharmacology of methylphenidate (Ritalin)
Activates catecholamine transmission by blocking DAT and NET reuptake - increases extracellular levels of DA and NE
No enhancement of GPA
Background of Tabacco, nicotine
•Nicotine is an alkaloid found in tobacco leaves
•Tobacco and nicotine were unknown to Europeans until Columbus’s expedition to the New World; quickly became popular in Europe
•Cigarettes became popular in the mid-19th century
•e-cigarettes: the device heats and vaporizes a solution of nicotine, producing an aerosol that is inhaled
Discuss the mechanisms of nicotine action on nicotinic acetylcholine receptors
Nicotine activated nicotinic cholinergic receptors
Ionotropic- produce rapid excitatory responses
Green Tabacco illness
Nicotine exposure in field workers
Mechanisms of caffeine action
(Dose dependent): inhibition of cAMP phosphodiesterase, blockade of GABAA receptors, stimulation of Ca2+ release in cells, and blockade adenosine receptors
Blockade of adenosine receptors, particularly A2A subtype, underlies caffeine-induced behavioral stimulation