Week 3:Postural Control & Primitive Reflexes
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
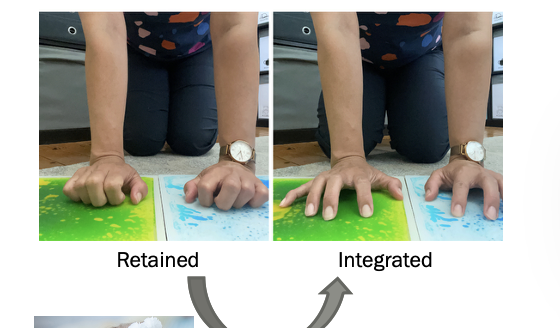
Integration
•Typically integrate in 1st year of life
•When a reflex is “integrated” it has developed into a more mature movement pattern.
•The reflex is no longer present
Persistence
RETAINED
May indicate atypical development
The reflex is still present
The more mature movement pattern has not developed
Child did not experience enough movement related to that reflex and the response.
Palmar Grasp Reflex
Onset: Birth
Integration: 5-6 Months
Voluntary Grasp replaces it
Automatic flexing fingers to grab objects
Retained Reflex:
Poor manual dexterity
Poor pencil grip
Messy handwriting,
Increased Oral Overflow

Palmar Grasp: Strategies to Integrate
Promote proximal stability & strength: activities that encourage stability of joints and strengthening of muscles
Provide proprioceptive input to promote weight bearing to the palm.
Activities to help promote gross grasp, strength and release
In Hand manipulation activities
Promote integration of Extension of Index finger in (grasp)
Pincer grasp
Open Web Space
Radial Digital Grasp
Case Example of palmar grasp reflex
10m old female baby with PMH of torticollis and low tone.
OT referral: Increased flexion of digits when crawling
Standardized Assessment: PDMS-2
Grasping Standard score 6; VMI standard score 7 (Below average)
Grasp
Immature grasp with ulnar side of hand; gross raking without thumb, no clear open web space
Index finger not integrated with grasp; pincer grasp not observed
VM:
Poor precision with Put in tasks (removing pegs) Poor graded control (placing cubes in cup)
Intervention: WB with full wrist and digit extension; Promote radial digital grasp, Graded control with grasp and release (put in tasks), Pincer grasp,
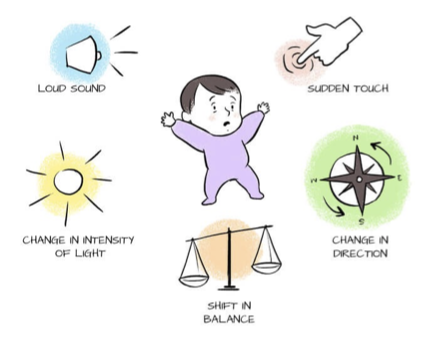
Primitive Reflexes : MORO Reflex
Onset: 28 Weeks Gestation
Integration: 4-6 Months
Occurs in response to unexpected changes
Function: Flight or Fight Response
Test: Rapidly Drop Head Backwards
Response
Phase 1: Arm Extension & Abduction
Phase 2: Arm Flexion & Adduction
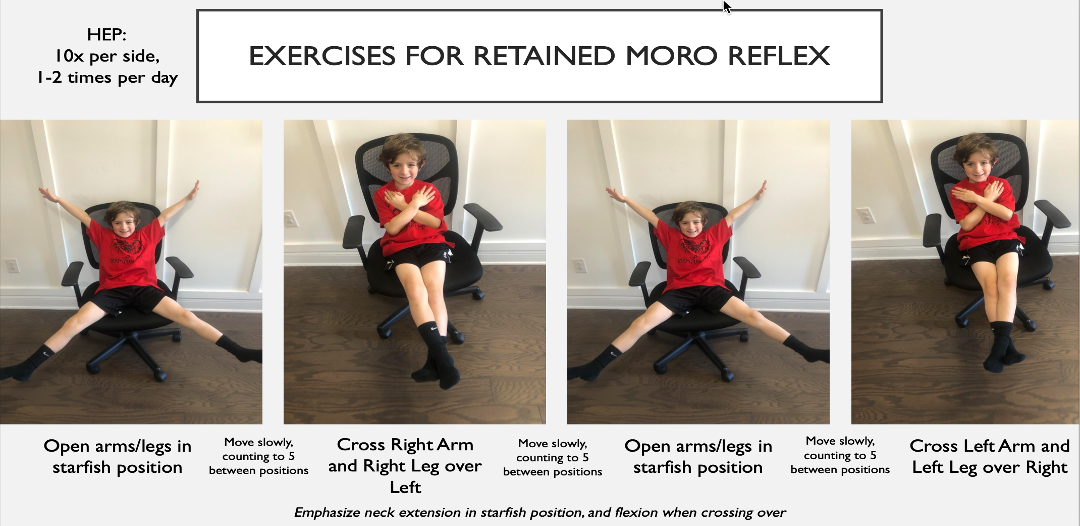
Strategies to Integrate Moro Reflex
Target Vestibular System
Rocking, rhythmic activities
Element of surprise
Sudden shifts in proprioceptive input (on standing surface)
Adapt Environment
Tummy Time
Swaddling Transition

Moro Reflex: Additional Interventions
Vestibular Input via Climbing Courses
Consider Change in
Direction
Speed
Angle
Orientation
Primitive Reflexes: Asymmetrical Tonic Neck Reflex (ATNR)
Onset: 37 Weeks Gestation
Integration: 4-6 Months
Function: Precursor to Hand Eye Coordination
Rolling over stomach
Crawling
Reading/writing
Test: Position Baby in Supine & Rotate Head to 90 Degrees.
Response
Face Side: Arm Extension
Skull Side: Arm Flexion
Persistence Effects of ATNR
Unable to Cross Midline (eyes/hands)
impacts creeping and crawling
Poor Reading Comprehension
Poor Visual Tracking & Eye Pursuits
Poor Handwriting
Poor Hand Eye Coordination
Poor bilateral coordination
Writing compensations: tight pencil grasp, turning paper, decreased fluency, extended arm, writing w/ slant, letter reversals
ATNR Strategies
Crawling in tunnel
Tummy time
Crossing Midline activities
Passing ball to each other and child watches as it swings side to side

ATNR Goal
Promote Head and UB dissociation
Consider variability in practice
Supine
Prone
Tall kneel
Four point
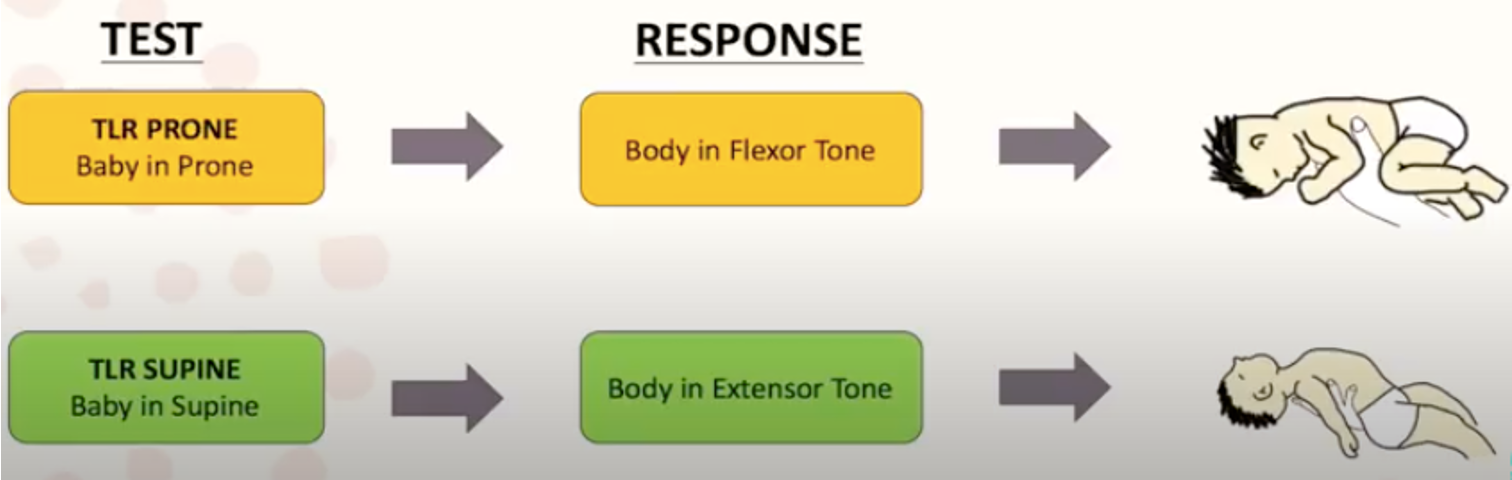
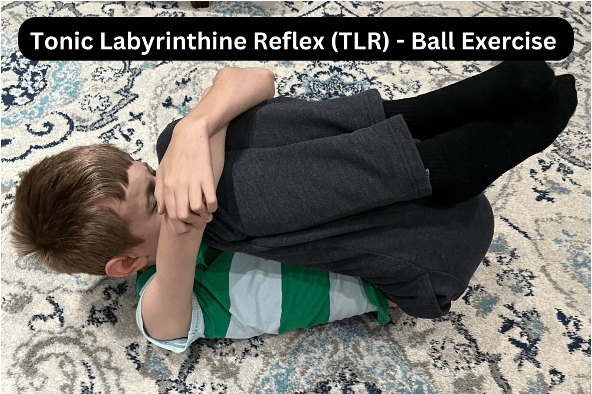
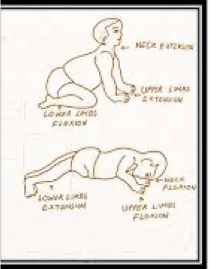
Primitive Reflexes: Tonic Labyrinthine Reflex (TLR)
Onset: 37 Weeks Gestation
Integration: 6 Months
Function:
Development of Balance, Body Position & Stability
Balances Flexion and Extension Tone
Head Neck Alignment and control
Body/Head Trunk Dissociation
there are 2 aspects of TLR: TLR PRONE and TLR Supine.
Retained: TLR: prone flexion and supine extension
persistence effects of TLR
Difficulty with Prone Extension (Increased Flexor Tone)
Difficulty with supine to sit (Increased Extensor Tone)
Poor Posture (W sit)
Poor Coordination
Impacts Auditory Processing
Impacts Visual Perception
Low muscle tone
Decreased chin tuck (impacts feeding)
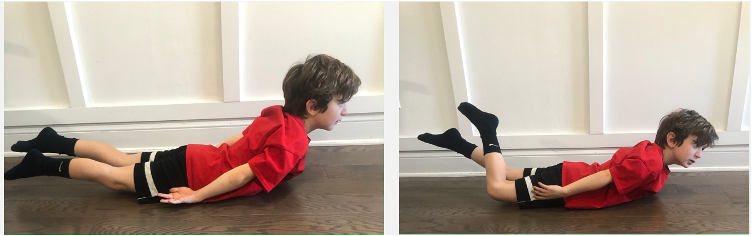
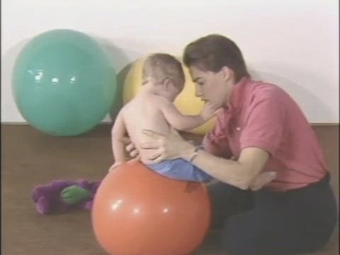
strategies of TLR
Anti-gravity Movement Exercises
Prone Extension
Supine Flexion
Landau reflex
Symmetrical Tonic Neck Reflex (STNR)
Onset: 4-6 months
Integration: 8-12 Months
Function: Precursor to Crawling – (Static Quadruped Position)
disassociation of the upper and lower body
Persistence Effects of STNR
Difficulty sitting up from supine
Poor muscle tone and posture (W-sit)
Impacts Focus
Postural Control
Foundation for movement
Postural stability allows for distal mobility
Ability to control center of mass in relation to base of support
Postural Reflexes
Supine Flexion
Prone Extension
Postural Control and Function
Developmental positions
Functional mobility
Transitions
Seated Posture
Impacts reach and FM milestones
Driven by Occupation

Facilitating Functional Movement
Observe what child can do in each functional position
Stationary and Dynamic
Start by Promoting Alignment
Example
Goal: Pt will demonstrate improved postural control by sitting upright in chair without compensations (trunk lean, UE support) during 5 minute activity with minimal cueing in 4/5 trials.
Facilitation of Reach
Facilitate weight bearing on forearms or hands
Facilitate efficient weight shift and equilibrium responses
Improve control of isolated & dissociated extremity movements
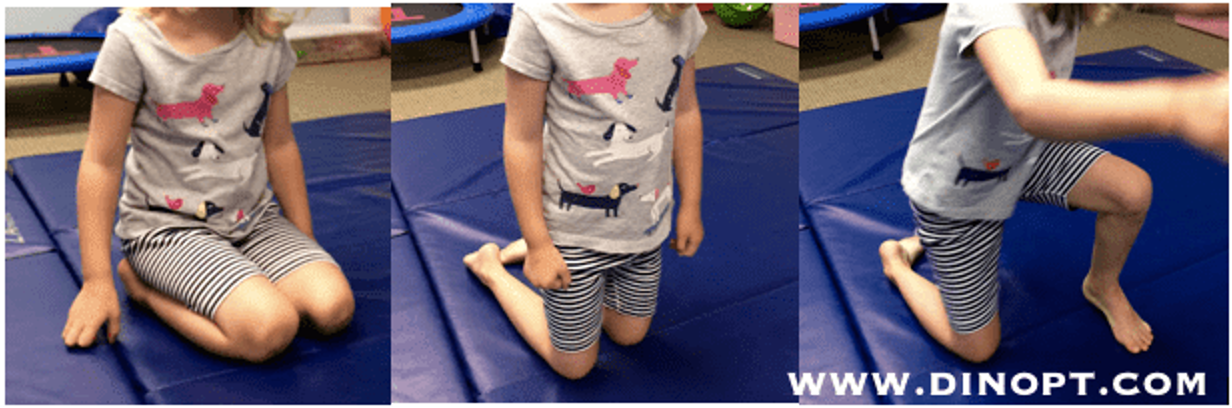
transitional (dynamic) movement
Prone to Sit
Sit to 4 point
4 point to Tall Kneel
Tall kneel to stand
Neurodevelopmental Therapy (NDT)
Can help children adapt movement when they lack variety in movement or show compensatory patterns
Primarily designed for children with CP; Utilizes concepts from MC/ML
Lack of adaptability in movt. patterns to accommodate task demands & environmental constraints leads to motor dysfunction
Meaningful engagement in wide variety of activities can help develop posture and core muscle control for coordinated movement
Engaging children in Typical Movement with Therapeutic Handling Techniques
Primary focus- inhibit spasticity & primitive reflexes and facilitate normal movement patterns
Ex. Increased Internal rotation at shoulder, pronation, wrist flexion adduction versus External rotation, supination, horizontal abduction, & wrist extension.
Examples of intervention techniques typically used using this model-
Facilitate weight bearing on forearms or hands
Facilitate efficient weight shift and equilibrium responses
Improve control of isolated & dissociated extremity movements
No evidence demonstrating use of NDT techniques to improve hand function of children with CP
Studies have shown that specific handling techniques used in NDT does not improve function in children with CP
Motor Learning is more effective than NDT for retention of motor function (Khanna et al. 2023)
Ideas & concepts from NDT have “deepened therapists’ understanding of CP and other muscle tone impairments” (Case-Smith & Exner, 2015, p. 239)
proximal points of control
Downward Pressure at Pelvis to guide Transition
from side sit to short sit'

Stabilizing Trunk to Promote Selective
UE reach
Distal Points of Control

Facilitating Alignment FOR Function
Stationary tasks
Consider use of equipment
Points of Control
