Pharmacodynamics
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
Articles used for use in the diagnosis, cure, mitigation, treatment or prevention of disease in man or other animals
Drugs
What is Pharmacodynamics?
The effects of drugs on the body
What is Pharmacokinetics?
The study of how the body interacts with drugs
What are the 3 different ways that drugs can be named? Describe each
Chemical Name
Describes the drug using chemical nomenclature
Generic (Non-Proprietary) Name
The name of the drug by the producing company
Ex: Acetaminophen
Trade (Proprietary) Name
Names that are owned exclusively by one company
Ex: Tylenol (a type of Acetaminophen)
T/F: Once manufacturers choose a trade name for a drug, they cannot rebrand that drug
False, they can, even if they. change the drug into an entirely new product they do not have to change the name
What are receptors?
They are molecules that bind to endogenous or exogenous ligands
What is Allosteric Binding?
Ligands that alter a receptors confirmation by binding nearby to it
What are the 4 major types of receptors? What is the main function of each?
Ligand-gated ion channels
Regulate ion flow through cell membranes
G-protein coupled receptors
Send 2° messengers into cells to trigger a certain outcome (stimulatory/inhibitory)
Tyrosine Kinase receptors
Activation (phosphorylation) of cellular enzymes and proteins
Mostly used by hormones/growth promoters
Intracellular Receptors
Alters DNA transcription
Ligands are lipophilic (steroids/thyroid hormones) and can enter the cell and bind to receptors within the cell
Response can take days
A receptor that allows Na+ into and out of the cell would likely be what type?
Ligand Gated Ion Channel
A receptor that is activated by thyroid hormones within the cell is likely what type?
Intracellular Receptor
When a Drug binds to a receptor on an enzyme, what are the 3 potential outcomes?
Block/Activate normal enzyme function
Produce false metabolites
Activate a prodrug
When a Drug binds to a transmembrane receptor, what are the 3 potential outcomes?
Mimic/Block the normal effect of endogenous molecules
Indirectly affect endogenous molecule concentration at receptors
Change endogenous molecule uptake
Two important terms of drug-receptor interactions are affinity and intrinsic activity, define both terms, describe the difference between the two
Affinity
Describes the tendency of a drug to bind with its target receptor and the strength of its connection
Intrinsic Activity
Occurs after the drug binds to the receptor
It describes the amount of response that occurs when a drug binds to the receptor
The most ideal drug is specific and selective, what does this mean? Is this feasible?
Specific means it binds to one or a few receptors
Selective means the drug only has its intended effects (ie no side effects)
This is achieved by the drug only binding to its intended receptor and not any others
This is rare, most drugs bind to multiple receptors with a stronger affinity for one of them
Which is more likely to cause side effects, non-specific drugs or specific drugs? Why?
Non-specific drugs
They bind to a wider range or receptors with less affinity for one particular receptor
This gives them the greatest probability to cause side effects
What is the difference between efficacy and intrinsic activity?
Efficacy describes the ability of the drug to produce the maximal desired effect
Intrinsic activity describes the ability of the drug to cause a response at the receptor (cellular) level
T/F: Receptors can have variable intrinsic activity, why or why not?
True
If the receptor can take multiple ligands, then it has the potential to send out one or more 2° messengers, resulting in different cellular responses
What are stereoisomers and what role do they play in pharmacokinetics?
They are chemicals that share the same molecular formula but vary in their 3D shape
The main type are Enantiomers
These are chemicals that are mirror images of each other (Think of it like holding out your L and R hand and making an L in both)
Drugs are made with racemic mixtures, meaning they have both variants (L and R) that can bind to to the different variants of receptors
What risk do racemic mixtures of drugs pose?
They can bind to different receptors and cause very different effects or side effects
What are the 3 different theories of dose-response quantification? Briefly describe each theory
Occupancy Theory
The response of a tissue/organ is proportional to the # of receptors bound and activated by a drug
Two-State Model
Receptors exist in a dynamic equilibrium between active (tensed) and inactive (relaxed)
Agonists bind to the receptors in their active state which shifts the equilibrium towards active
Inverse Agonists bind to receptors in their inactive states and shift equilibrium towards the inactive
Rate Theory
Receptors can be bound or unbound by a ligand but neither causes a reaction
The reaction stems from the binding of the ligand to the receptor (the important part is the initial contact between ligand and receptor)
What are the 4 important characteristics of the drug-concentration relationships?
Efficacy
Potency
Slope
Variablity
Define Efficacy
The ability of a drug to produce the desired effect
It is more important for a drug to be ______ than potent
Efficacious
Define Potency
The concentration of a drug required to elicit the desired effect
What is a drug-response curve used to represent?
How close the relationship is between effectiveness of a drug and toxicity in relation to the dosing
If a dose-response curve has overlying lines, what does that indicate about the dosing range of the drug?
It indicates that there is not a very safe dosing range between effectiveness and toxicity
T/F: All drugs work the same for every animal of the same species
False, they can vary wildly
What factors can contribute to the variable responses to a certain drug in patients?
Administration route
Drug concentration at the receptor site
Drug interactions
Disease type and severity
Age
Tolerance
Gender
What is the difference between an Agonist and an Inverse Agonist?
An Agonist mimics the effects of endogenous substances when they bind to a receptor, the “activate“ receptors
An Inverse Agonist binds to inactive receptors and stabilizes them in the inactive confirmation, preventing activation
What is the difference between a partial agonist and a full agonist?
One produces a maximal response and the other produces a sub-maximal response (lower intrinsic activity)
What is the term that goes with this description?
Agonists that bind to receptors (mainly GPCRs) that can stimulate different pathways/responses but are favorable towards one particular pathway
Biased Agonists
What is the term that goes with this description?
The interaction between two drugs that results in the response of one being decreased when the other drug is present
Antagonism
What are Receptor Antagonists and what role do they play in receptor activation/inactivation?
They are ligands that have an affinity for a recpetor but when they bind they do not change the confirmation of the receptor to active/inactive
They reduce the effect of other agonists/ligands by competing for the
T/F: Receptor Antagonists have no clinical effect if no Agonist/Ligand is present
True
What are the 3 different types of Antagonists? Describe each
Reversible Competitive Antagonist
Don’t bind permanently to the receptor
Bind to the same site on the receptor as the ligand
Surmountable (If there is more agonist it can be overcome)
Irreversible Antagonists
Competitive/Non-Competitive forms
Form permanent bonds with receptors
Non-Competitive Antagonists
Bind allosterically to receptors, preventing agonist from binding
T/F: Antagonists alter the receptor equilibrium (active/inactive), but Agonists don’t
False, it’s reversed
What is the difference between a Physiological and a Chemical Antagonist?
A Chemical Antagonist prevents the Agonist from binding to a receptor by modifying/sequestering the Agonist so that it can no longer bind to the receptor
A Physiological Antagonist just cancels out the effect of another drug (similar to the definition of Antagonism )
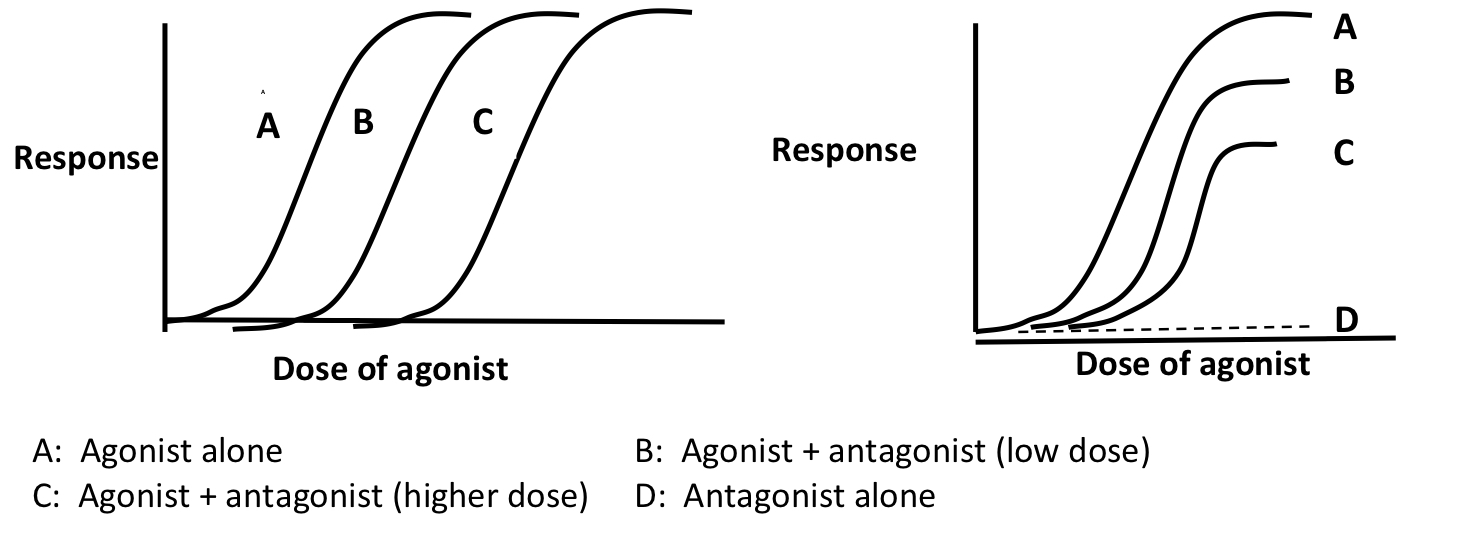
What type of Antagonism is depicted on the L and R?
L
Competitive Antagonism
R
Non-Competitive Antagonism
Decreases each time because as the Antagonist increases, the response decreases because the Agonist can’t fight the antagonist for a spot since the antagonist binds allosterically
T/F: Drug action can change over time
True!
Refractory
Loss of therapeutic efficacy over time
Tolerance/Tachyphylaxis
Loss of efficacy of a drug due to continuous/repeated use
What is Receptor Attenuation? What can cause it?
The loss of receptor response
The desensitization of receptors
Receptors remain in cell membrane but are deactivated
Down-regulation of receptors
# of receptors decreases either by decreased synthesis or internalization
What are some causes of increased responsiveness to a drug?
Altered pharmacokinetics (how the body interacts with the drug) leading to a greater concentration of drug at the target site
Increased # of target receptors
What is the Therapeutic Index?
A measure of a drugs safety
It’s a comparison of the average dosage that produces toxicity and the average dosage that produces the desired response
There is no such thing as a perfect drug, but what are the 10 properties of an ideal drug (in order of importance)?
Efficacy
Safety
Specificity
Reversible Actions
predictability
Ease of administration
Freedom from drug interactions
Inexpensive
Chemical Stability
Generic product available