Cranial Nerves XI and XII + Brainstem Blood Supply
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
20 Terms
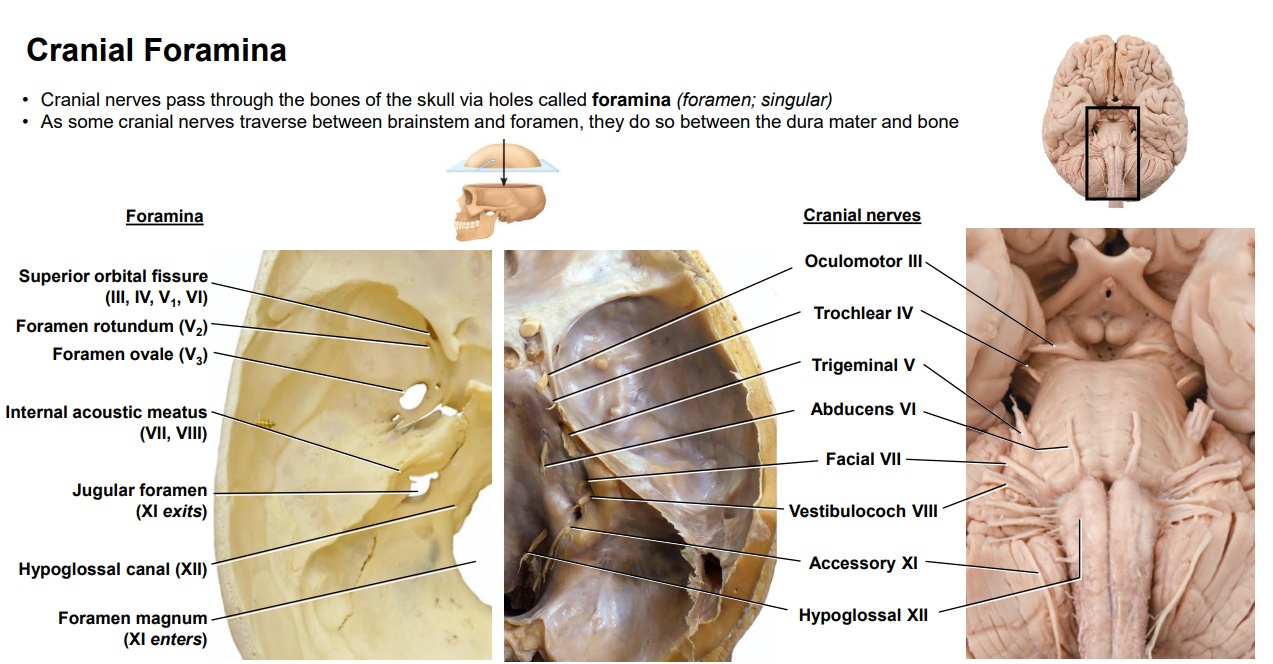
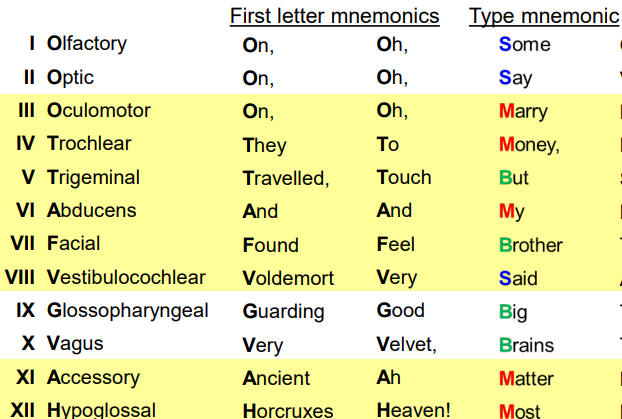
List the Cranial Nerves and their associated Foramina
Olfactory - Cribiform Plate
Optic - Optic Canal
Oculomotor - Superior Orbital Fissure
Trochlear - Superior Orbital Fissure
Trigeminal
Opthalmic - Superior Orbital Fissure
Maxillary - Foramen Rotundum
Mandibular - Foramen Ovale
Abducens - Superior Orbital Fissure
Facial - Internal Acoustic Meatus
Vestibulocochlear - Internal Acoustic Meatus
Glossopharyngeal - Jugular Foramen
Vagus - Jugular Foramen
Accessory - Jugular Foramen
Hypoglossal - Hypoglossal Canal
List the Cranial Nerves and their associated Function (Motor or Sensory)
Olfactory - Sensory
Optic - Sensory
Oculomotor - Motor
Trochlear - Motor
Trigeminal - Both
Abducens - Motor
Facial - Both
Vestibulocochlear - Sensory
Glossopharyngeal - Both
Vagus - Both
Accessory - Motor
Hypoglossal - Motor
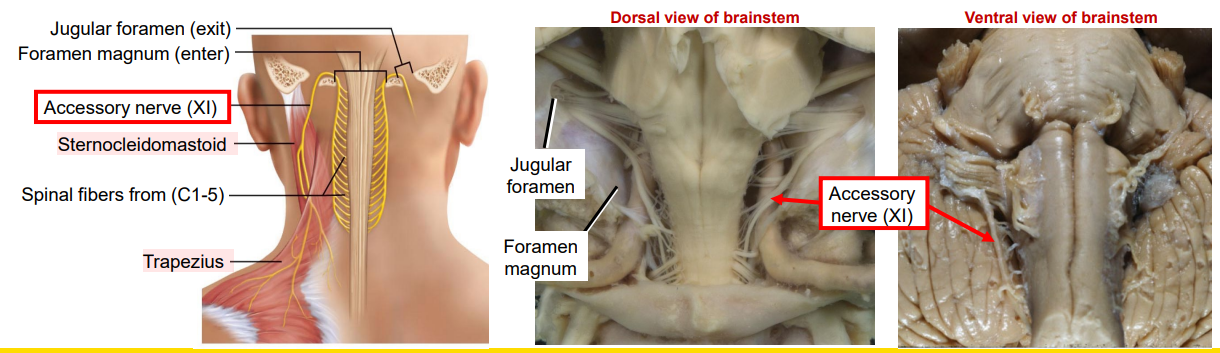
Accessory Nerve (CN XI) - Location of nerve and nuclei, innervations
Nerve Location: Upper Cervical Segments C1 - C4/5
Nuclei Location:
Nucleus Ambiguus: Caudal medulla within the reticular formation (hard to see)
Spinal Accessory Nucleus: Upper cervical cord and spinomedullar junction, located where normally the ventral horn would be
Synapse with UMNs from Corticobulbar Tract (bilateral)
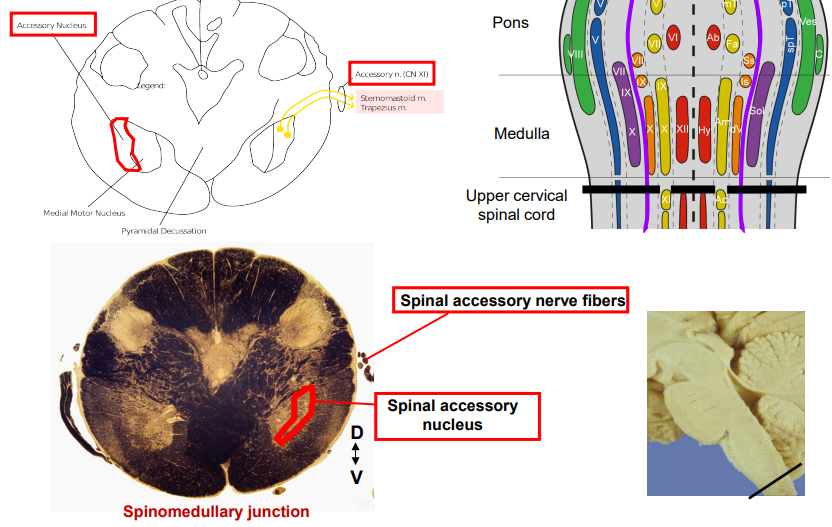
Accessory Nerve (CN XI) - Function
Function: MOTOR
Nucleus Ambiguus: Muscles of the pharynx for speech and swallowing
Spinal Accessory Nucleus: SCM and Trapezius motor function
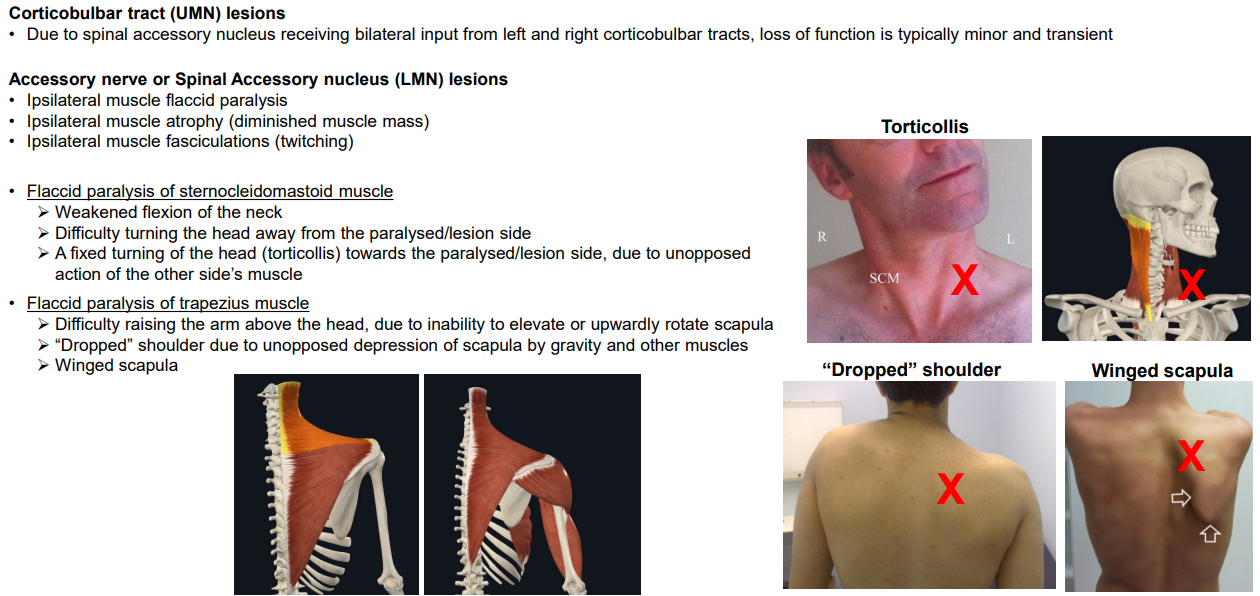
What are some signs of an Upper or Lower motor neuron lesion affecting the Accessory nerve or nucleus?
UMN lesion: Damage to a Corticobulbar Tract does not cause many issues, due to bilateral input from the other side
LMN lesion: Damage to the Accessory nerve or its nuclei can lead to ipsilateral LMN lesion symptoms
Flaccid paralysis
Atrophy
Fasiculations
Only affecting SCM and Trapezius
SCM damage:
Poor flexion of the neck (head usually tilts contralaterally to damage)
Poor rotation away from lesion
Trapezius damage:
Difficulty raising arm above head due to poor scapular rotation
Ipsilateral dropped shoulder
Winged scapula
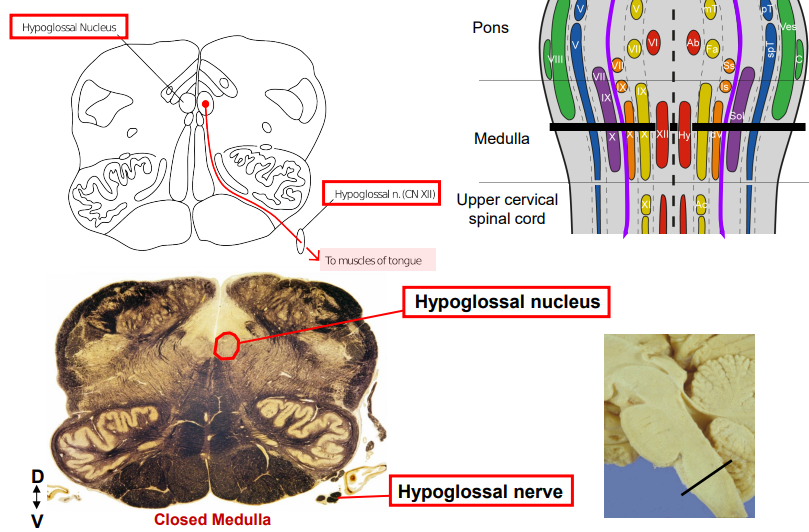
Hypoglossal Nerve (CN XII) - Location of nerve and nuclei, innervations
Nerve Location: Medial medulla between the olives and pyramids
Nuclei Location:
Hypoglossal Nucleus: Medulla, near the midline and superior to the medial longitudinal fasiculus
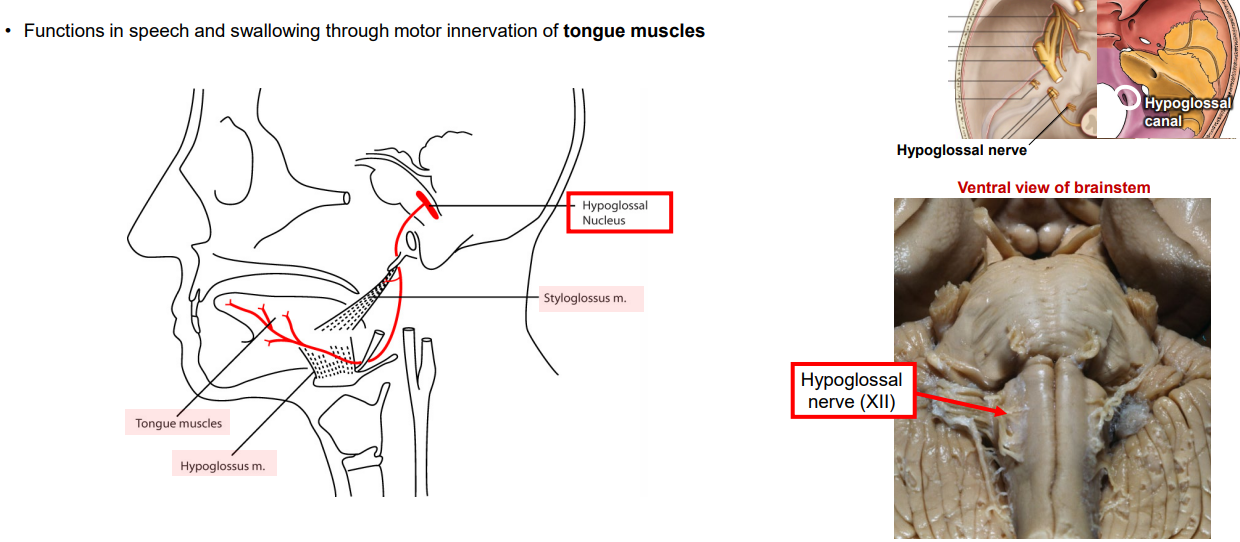
Hypoglossal Nerve (CN XII) - Function
Function: MOTOR
Hypoglossal Nucleus: All intrinsic tongue muscles and most extrinsic tongue muscles (except palatoglossus - CN X)
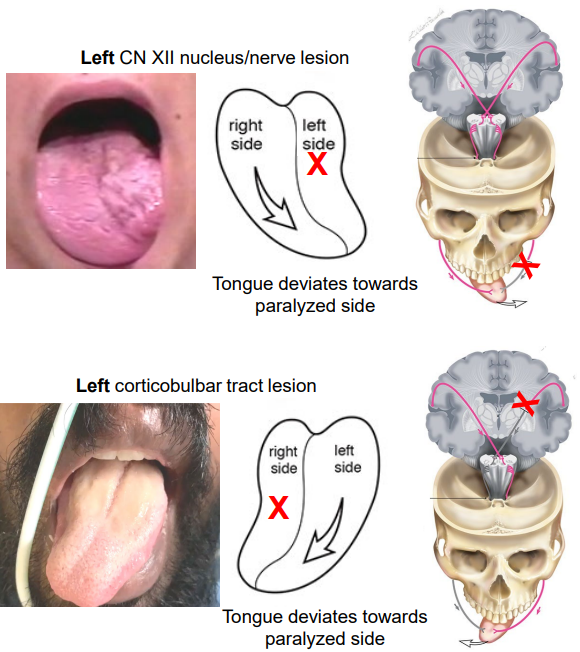
What are some signs of an Upper or Lower motor neuron lesion affecting the Hypoglossal nerve or nucleus?
UMN lesion: Corticobulbar tract damage will lead to few symptoms due to bilateral input
However, genioglossus (involved with protruding the tongue) has unilateral innervation
Hence, tongue deviates to paralysed side when protruded as genioglossus undergoes atrophy and flaccid paralysis
LMN lesion: Damage results in ipsilateral atrophy, paralysis and fasciculations of all tongue muscles
Tongue deviates to paralysed side when protruded
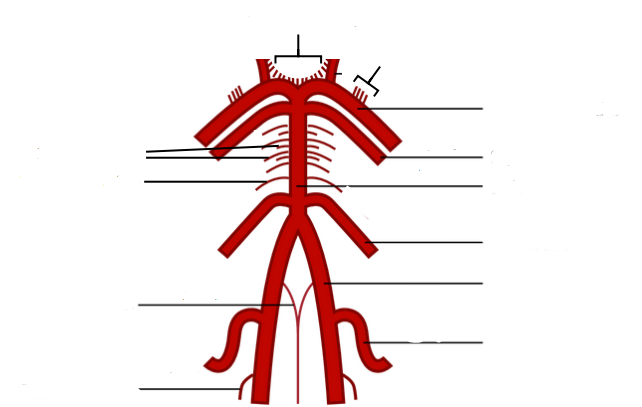
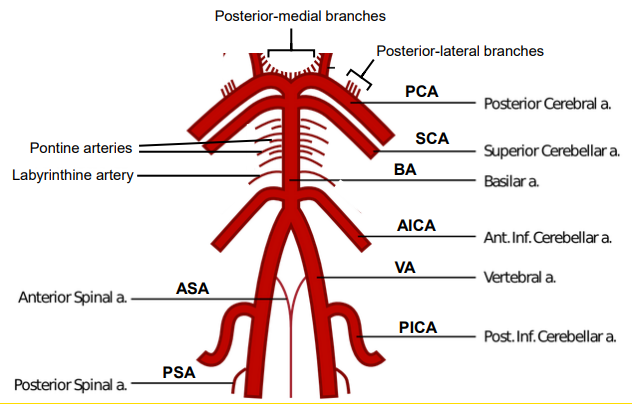
Name each of the main arteries in the posterior circulation chain
From Rostral to Caudal:
Posterior medial and lateral branches
Posterior Cerebral Artery
Superior cerebellar Arteries
Pontine Arteries
Labyrinthine Artery (not needed)
Basilar Artery
Anterior Inferior Cerebellar Artery
Vertebral Artery
Anterior Spinal Artery
Posterior Inferior Cerebellar Artery
Posterior Spinal Artery
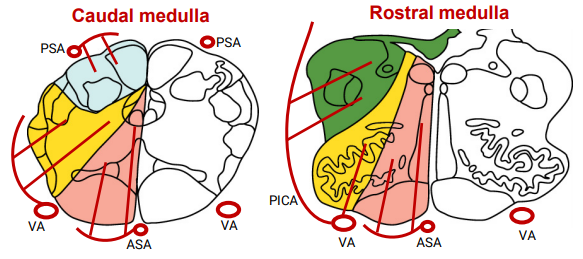
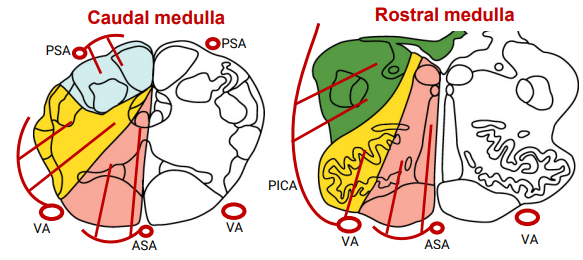
What are the arteries involved with the blood supply for the Medulla?
Anterior and Posterior Spinal Arteries:
Branch off the vertebral artery to supply the anterior and posterior medulla respectively
Also supply respective regions of the spinal cord
Vertebral Arteries:
Supply the lateral aspect of the Medulla
Posterior Inferior Cerebellar Arteries
Branch off the vertebral artery at rostral medulla to supply the posterior-lateral aspect of the rostral medulla
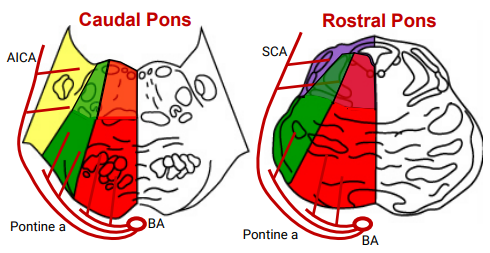
What are the arteries involved with the blood supply for the Pons?
Basilar Artery: Gives rise to Pontine Arteries
Pontine Arteries:
Supplies medial and lateral pons
Anterior Inferior Cerebellar Arteries:
Branch off the basilar artery at the level of the caudal pons to supply the posterior-lateral aspect of caudal-to-mid pons
Superior Cerebellar Arteries:
Branch of the basilar artery at the rostral pons level to supply posterior-lateral region of rostral pons
What are the arteries involved with the blood supply for the Midbrain?
Posterior Cerebral Artery: Gives rise to medial and lateral branches
Posterior-medial branches supply medial aspect of midbrain
Posterior-lateral branches supply lateral aspect of midbrain
Collicular branches supply the posterior aspect of the midbrain
PCA continue posteriorly to supply occipital lobe
What are the clinical presentations that might be seen by damage to the Vertebral artery
Main arterial output to the posterior circulatory system. Damage could be life threatening
What are the clinical presentations that might be seen by damage to the Anterior Spinal Artery
Medial Medullary Syndrome
Hypoglossal nucleus: Ipsilateral tongue atrophy and paralysis, deviation to side of damage
Medial lemniscus: contralateral body loss of fine touch, vibration and conscious proprioception
Corticospinal tract: contralateral body muscle weakness/paralysis
What are the clinical presentations that might be seen by damage to the Posterior Spinal Artery
Ipsilateral body loss of fine touch, vibration and conscious proprioception sensations
Carries fibres from cuneate and gracile fasiculi and/or nuclei
These fasiculi cross AFTER reaching the medial lemniscus
What are the clinical presentations that might be seen by damage to the Posterior Inferior Cerebellar Artery
Lateral Medullary Syndrome:
Vestibular nuclei: Nystagmus (repetitive eye movements) and vertigo (dizziness)
Nucleus Ambiguus (CNXI) : Difficulty speaking (dysarthria), and difficulty swallowing (dysphagia)
Cuneo & Spinocerebellar tracts and cerebellum: Ipsilateral loss of motor coordination (ataxia)
Spinal trigeminal nucleus and tract: Ipsilateral loss of pain and temperature in face
Spinothalamic tract - contralateral body loss of pain and temperature sensations
What are the clinical presentations that might be seen by damage to the Anterior Inferior Cerebellar Artery
Vestibular nuclei: Nystagmus (repetitive eye movements) and vertigo (dizziness)
Cerebellum: Ipsilateral loss of motor coordination (ataxia), nystagmus and vertigo
Spinal & Principal Trigeminal nuclei: Ipsilateral face loss of pain and temperature & fine touch and vibration, respectively
What are the clinical presentations that might be seen by damage to the Superior Cerebellar Artery
Cerebellum: Ipsilateral loss of motor coordination (ataxia), nystagmus and vertigo
What are the clinical presentations that might be seen by damage to the Pontine Arteries
Motor Nuclei and Tracts
Abducens nucleus: Ipsilateral eye loss of abduction
Facial motor nucleus: Paralysis to entire ipsilateral side of facial expression muscle
Trigeminal motor nucleus: Paralysis of ipsilateral muscles mastication
Pontine nuclei: Contralateral loss of motor coordination (ataxia) *masked by paralysis
Corticospinal tract: Contralateral body muscle weakness/paralysis (hemiparesis/hemiplegia)
Corticobulbar tract: Tongue deviation away from the side of the lesion
Sensory Nuclei and Tracts
Medial lemniscus: Contralateral body loss of fine touch, vibration and conscious proprioception sensations
Spinothalamic tract: Contralateral body loss of pain and temperature
Trigeminothalamic tract: Contralateral face loss of pain and temperature, & fine touch and vibration
What are the clinical presentations that might be seen by damage to the Posterior Cerebral Artery
Weber’s Syndrome: hemianaesthesia, loss of vision, and paralysis on contralateral side of body
Oculomotor & Edinger Westphal nuclei: Ipsilateral eye “down and out” deviation, dilated pupil, closed eyelid, (ptosis), difficulty focusing
Occipital lobe - Loss of vision
Sensory tracts - contralateral loss of all sensation from body and face (hemianesthesia)
Medial lemniscus
Spinothalamic
Trigeminothalamic
Cerebral peduncle (motor tracts)
Corticobulbar tract - paralysis to contralateral side lower quarter of face (i.e. below the eye), tongue deviation away from side of the lesion
Corticospinal tract - contralateral body muscle weakness/paralysis (hemiparesis/hemiplegia)
Corticopontine tract - contralateral ataxia *masked by paralysis