The Older Adult Learner and Cognitive Aging
1/37
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
38 Terms
Cognitive Aging
Cognitive aging occurs over time and varies among individuals
Changes in cognitive functioning are not specifically caused by aging, factors such as general health, education, life-style, genetics, socioeconomics, and socialization can cause changes in individuals
The stereotype that older adults have fewer cognitive skills can lead to assumptions in relationships that could be less than ideal
Factors that Impact Cognitive Health
Lifestyle
Education
Socioeconomic status
Access to health care
Cognitive Processes Include
Attention
Memory
Problem-solving
Decision-making
Reasoning
Judgment
Language
Speed of processing
Attention
The ability to focus on stimuli for the purpose of processing information
Requires effort and the ability to filter relevant and irrelevant stimuli
The ability to successfully make decisions, problem-solve, or think through an issue requires attentional resources
Sustained (or focused) Attention
The ability to direct attentional resources to a single task or activity
Example: Concentrating on reading a book
Selective Attention
The ability to direct attentional resources to a task or activity while simultaneously directing attention resources to ignore distracting information
Example: Listening to a story someone is telling while others are talking around you
Alternating Attention
The ability to direct or switch attentional resources between two or more tasks or activities
It is conceptually distinct from divided attention because tasks are performed one at a time with attentional resources switching back and forth between tasks
Example: When cooking, a person attends to stirring on item and then letting it cook, while they work on chopping and prepping another item; the person then shifts back and forth depending on the instructions.
Tips for practice
Minimize all distractions; remove unneeded equipment, ensure privacy
Consider speed of processing. Slow the instruction if client needs more time to process
Know the client’s sensory processing abilities to ensure the client is understanding and seeing what you are doing; asking the client for feedback is one way of checking their understanding
Explain to the client your goal for the session and ask what they would like to get from the session; this can build meaning and set expectations
Actively engage the client in the treatment; this can emphasize the meaning and relevance to the client
Use a “teach-back” method of instruction, asking the client to explain what was said and ask their opinion
Repetition. Engage in problem-solving for the client’s learning
Once the occupation has been performed safely, you may introduce distractions to challenge the client and simulate a realworld environment, such as a busy home
Review the session, address questions and concerns, and ask the client if the session met their expectations and what more is needed
Handouts can be helpful to enhance learning
What factors can impact a person’s attention while performing a task?
environmental factors/distractions
medication (e.g., drowsiness)
stress
fatigue
relevance to the task (e.g., is it meaningful?)
motivation (e.g., depression)
Memory
A generic term used to describe type of memory including
Sensory memory
Short-term memory
Working memory
Several long-term memory systems (including declarative and procedural long-term memory)
Sensory memory
The processing of information through the vestibular, visual, auditory, and tactile systems
Short-term memory
2 Forms
1. new information is stored based on sensory inputs
2. memories that have been stored and retrieved through cueing such as smelling an odor and recalling a feeling or conversation
Working memory
Demands attention and requires the intentional use of strategies to manipulate, store, and maintain information
Serves a vital role in facilitating higher-order cognitive processes such as language production and comprehension, decisionmaking, problem-solving, and learning
Procedural or Non-Declarative Memory
Nonverbal-based memory system that stores information for motor-based skills and behaviors (e.g. muscle memory), habits, emotional associations, priming, and classical conditioning
Retrieval of nondeclarative memories can occur with little effort or even conscious awareness
Examples: how to play a musical instrument, ride a bike, or perform a habitual task, such as brushing your teeth
Prospective memory
Enables individuals to remember future-oriented or scheduled tasks without the use of external memory aides (e.g. a written note or list)
Examples: remembering to take medications twice daily, wearing a brace to bed, stopping at the grocery store, or buying a birthday card for a friend
Semantic memory
The knowledge of language including words, phrases, definitions, and grammar
Understanding language and memory for facts is considered crystalized intelligence and remain relatively stable with aging
However, age-related differences can be found in the production of speech
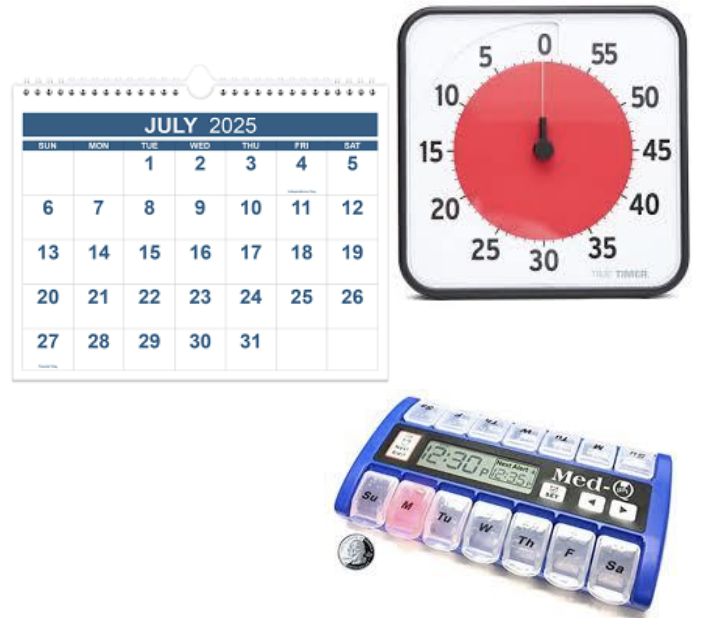
External Memory Aids
• Alarms/Timers
Notebooks/Datebooks
Calendars
Audio messages
Pillboxes
Internal Memory Aids
Association
e.g., “everytime i cook dinner, I will also have to give my son his medication”
Organization
knowing where things are meant to be
Visualization
Imagination
Executive Functioning
Refers to higher-order cognitive processes such as reasoning, decision-making, problem-solving, judgment, abstract thought, cognitive flexibility, initiation (i.e., beginning a task), and inhibition (e.g., having no filter)
Underlies a person’s ability to engage in everyday activities
Intelligence Abilities
Fluid Intelligence:
the ability to use abstract reasoning, flexibility to shift one’s mental set, and initiate and complete purposeful action
it includes creative and flexible thinking required in novel situations and can be directly affected by physiological structure changes
Crystallized intelligence:
the accumulation of knowledge, experience, and acculturation that is highly representative of individual differences
older adults can learn new things stil!!- just may take more time
knowledge of facts, rules, and verbal skills rely on crystallized intelligence
Implicit and Explicit Processing
Two types of cognitive processes used to learn (or transfer) information from short-term to long-term memory and to retrieve information from long-term to short-term memory
Implicit: unintentional, occurs without awareness, and is effortless, requiring minimal cognitive resources
e.g., remembering a song from just listening to it a lot
Explicit: intentional, occurs with awareness, and is effortful, requiring moderate to substantial cognitive resources
e.g,. remembering a song b/c you practice reading the lyrics
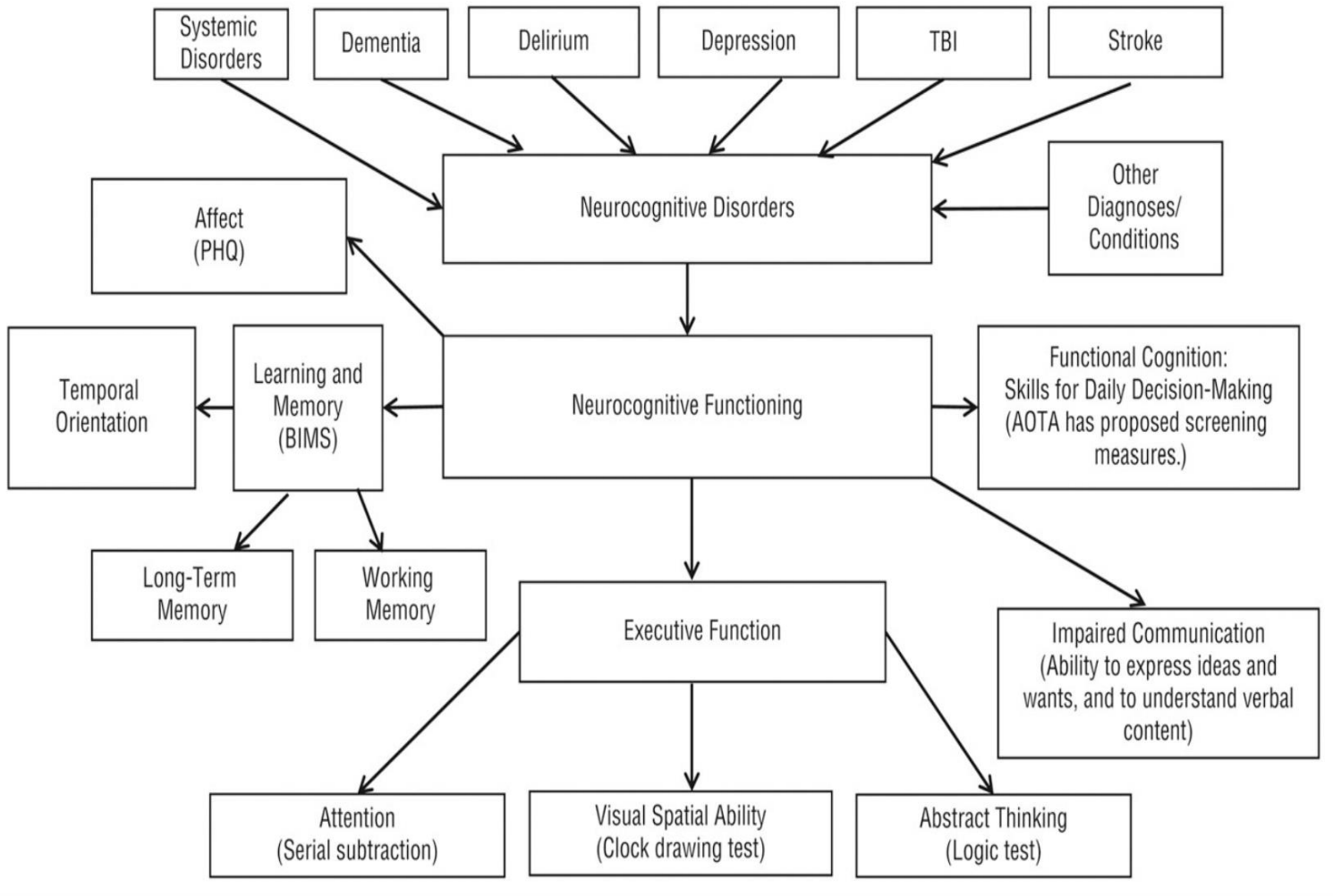
Functional Cognition
The cognitive ability to perform B(basic)ADLs and IADLs, incorporating the cognitive processes previously discussed
Should be assessed in the natural, real-world context in which the task is performed, rather than a laboratory setting using standardized measures
performance-based assessments (^ tasks being performed in a natural, real-world context) have much better psychometrics than self-report measures
Performance-based Executive Function Assessments (specific to OT)
Assessment of Motor and Performance Skills (AMPS; Fisher, 1995)
Cognitive Performance Test (CPT; Burns et al., 1994)
Complex Task Performance Assessment (CTPA; Wolf et al., 2008)
Multiple Errand Test (MET; Shallice & Burgess, 1991)
Performed Direct Assessment of Functional Status (modified) (PDADS; Rankin & Keefover, 1998)
Executive Functional Performance Test (EFPT; Baum, 2011)
The Kitchen Task Assessment (KTA; Baum & Edwards, 1993)
Large Allen’s Cognitive Screen-5 (LACLS-5; Allen et al., 2007)
Menu Task (Edwards et al., 2019) • Performance Assessment of Self-Care Skills (PASS; Holm & Rogers, 2008)
Weekly Planning Calendar Activity (WPCA; Toglia, 2015)
Need for Functional Cognitive Screening
Neuropathologies and Impact on Cognitive Functioning in Older Adults
Delirium
Mild Cognitive Deficits
Dementia
CVA
TBI
Mental disorders
Delirium
A syndrome with an acute onset of changes in attention, awareness, and cognitive functioning
Onset is rapid as 1 or 2 hours and can last for day to months
Can be caused by a medical condition not related to a preexisting neurocognitive disorder
Causative factors include
Frailty, infections (e.g. urinary tract infections), prolonged illness, low sodium, medication reactions, alcohol, and surgery with anesthesia
UTIs are very big in causing cognitive deficits!!
Often presents during daytime and worsens at night
Being in an unfamiliar environment can exacerbate delirium
Treatment: discovering the cause and intervening
UTI —> treatable but you must catch in time or they’ll become septic (full-body infection)
Multi-intervention approaches including OT and PT have been effective in reducing the number of days with delirium
D.E.L.I.R.I.U.M. Mnemonic
Encompasses the key elements of current best practice in managing delirium
Drugs
removing drugs that might make people, e.g., narcotic
Environment
make sure it’s safe
Light
natural light appropriate for day vs night (e.g., limiting light at nighttime)
Initiate Cognitive Tasks
practice meaningful, stimulating tasks in therapy
Routine
using clocks, schedules (24-hr method), etc.
Integrate an Interprofessional Team Approach
OT, PT, speech, pharmacology, etc.
Under hydration/nutrition
food and fluid intake is sufficient + incorporate that into a routine
Mobility
incorporate movement into daily routine (e.g., exercise)
Mild Cognitive Impairment (MCI)
Affects 10-15% of adults over the age of 65
MCI is a transitional stage between healthy aging and dementia
The prevalence of MCI in older adults increases with age, lower level of education, and sex (higher in men)
Diagnoses of MCI include:
Client history and cognitive testing
The progression is defined by the presence of amnesia and the number of areas affected by the amnesia, including attention, language, visuospatial, and executive functioning
Current medications are shown to only slow progression- doesn’t get rid of it completely
Persons with MCI benefit from inclusion in
Exercise
Client-centered activities
Cognitive stimulation
Socialization
Client and family education
Memory strategies
Dementia
A syndrome of cognitive impairment affecting cognitive processes and significantly affects a person’s ability to independently perform BADLs and IADLs and participate in meaningful and fulfilling activities
Risk Factors for Dementia
Less education
Hypertension
Hearing impairment
Smoking
Obesity
Depression
Physical inactivity
Diabetes
Excessive alcohol consumption
TBI
Air pollution
Low social contact
Types of Dementia
Alzheimer Disease
Vascular Dementia
Dementia with Lewy Bodies
Frontotemporal Dementia
Alzheimer Disease
most common type of dementia, accounting for 60% to 70% of cases
Vascular Dementia
Second most commonly diagnosed form of dementia
Caused by an overall inefficient supply of oxygenated blood in the brain which may be caused by small transient ischemic attacks, major strokes, or untreated high blood pressure
Individuals with vascular dementia may not experience progressive cognitive changes across time, but instead will typically experience daily fluctuations in their cognitive abilities, with symptoms becoming worse over the course of the day
symptoms can be similar to Alzheimer’s, but are more localized
also more inconsistency in cognitive processes
life expectancy: 5 years post-onset of symptoms
Dementia with Lewy Bodies
A progressive dementia and represents two related diagnoses
Dementia with Lewy bodies
Parkinsons disease dementia
up to 80% of people with Parkinsons disease dementia with also develop Lewy bodies
Up to 85% of people with dementia with Lewy bodies experience motor difficulties
Dementia with Lewy bodies is diagnosed as early as 50 years old, and life expectancy is 5 to 7 years after initial onset of symptoms
Persons present with a range of cognitive changes including
Attention
Executive functions
Visual perceptual symptoms
Neuropsychiatric symptoms (hallucinations)
Sleep disorders
Autonomic symptoms (syncope, dizziness)
can only truly know this diagnosis from an autopsy after a person dies
Frontotemporal Dementia
A hereditary neurodegenerative disorder (30% of cases have a strong family history)
Characteristics include changes in behavior (personality), language (progressive aphasia), and motor function (ALS or PD (parkinson’s disease))
Characterized by abnormal amounts of forms of tau and TDP-43 proteins accumulating inside neurons in the frontal and temporal lobes
Optimizing Cognitive Functioning in Older Adults
Cognitive Reserve: the amount of cognitive resources available after an individual engages in a task
the more cognitive reserve, the better someone will age
Factors such as participation in cognitively stimulating activities, physical activity and exercise, and socialization have been linked to facilitating enhanced cognitive reserve
Cognitive and Mental Stimulation
Participating in mentally stimulating and novel activities can include increasing the difficulty of cognitive tasks during therapy and educating patients to challenge themselves at home with new and unfamiliar tasks, such as learning a new language or activity
To be considered mentally stimulating, tasks should be novel and mentally challenging, as new learning facilitates neural growth, development, and plasticity
Socialization
Paramount for healthy cognitive aging