Case 7: Luke Tomczak - Pneumonia
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
Lung Protective Mechanisms
Physical barriers
Reflex barriers
Chemical barriers
Cellular barriers
Lung Physical Barriers
Epithelial cells
Cilia
Cell junctions
Mucus
Pattern recognition receptors
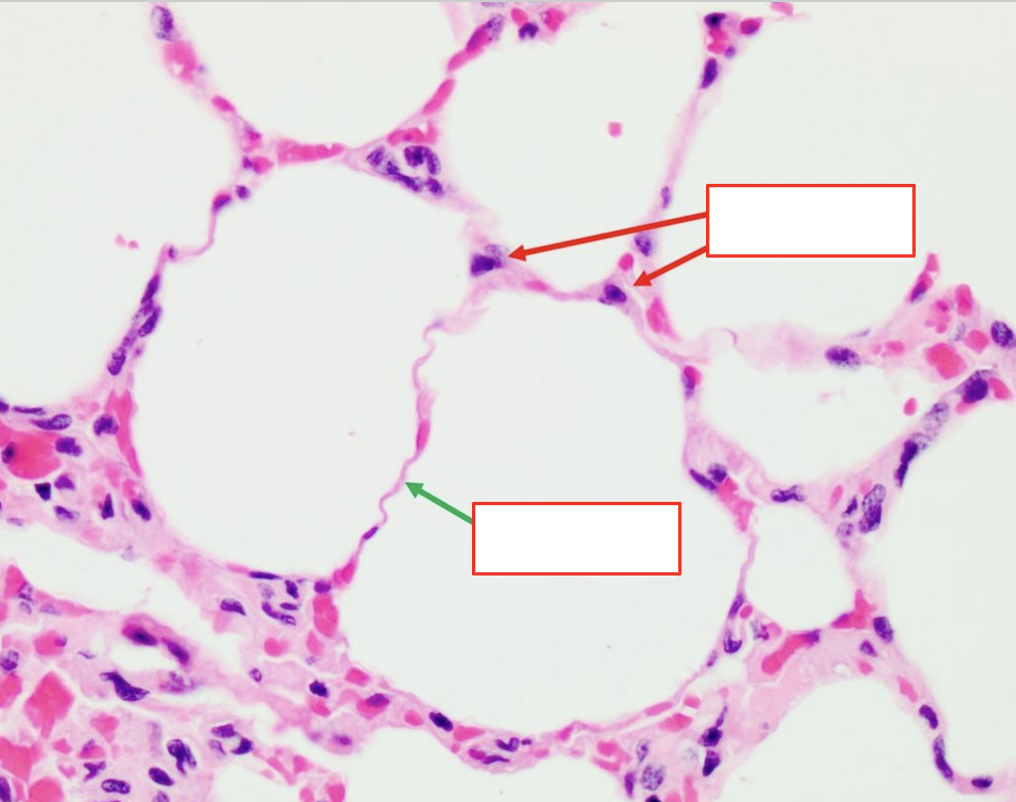
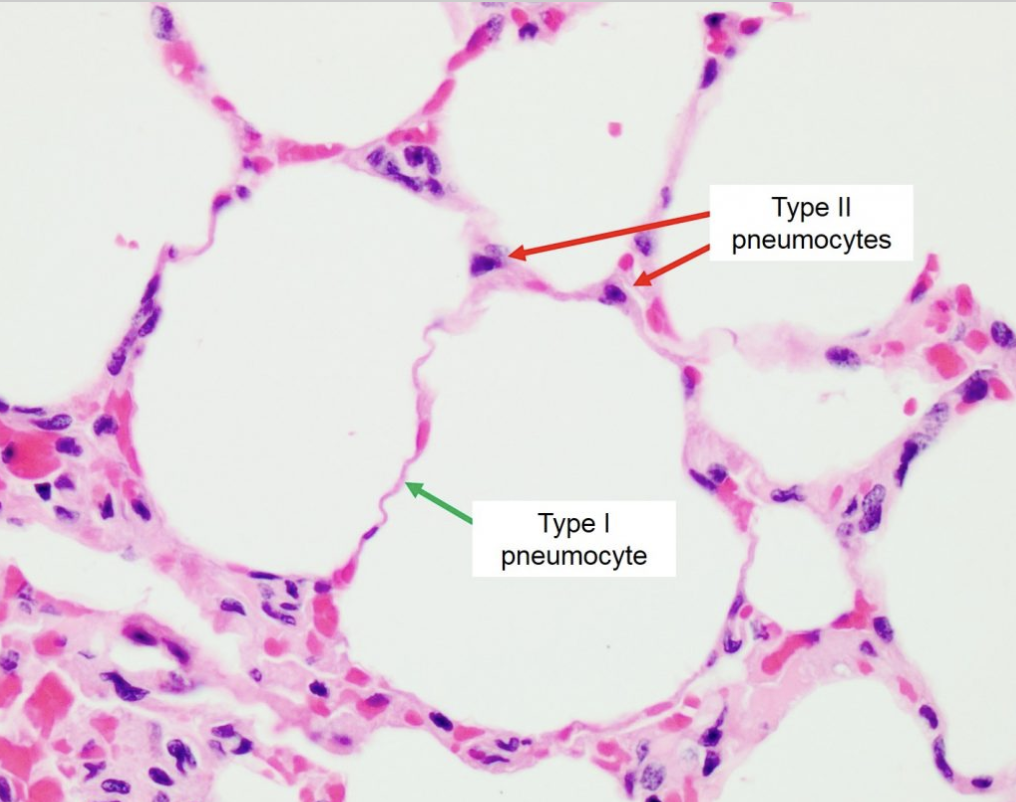
Physical Barrier: Epithelial Cells
Type 1 and 2 pneumocytes (alveolar cells)
Type 1:
Squamous cells
Gas exchange
Maintain ion/fluid balance
Type 2:
Produce and secrete pulmonary surfactant (decrease surface tension)
Express immunomodulatory proteins
Transepithelial water movement
Regenerate pneumocytes
Physical Barrier: Cilia
In resp tract (not alveoli)
Push mucus to pharynx (mucociliary clearance)
Physical Barrier: Cell Junctions
Apical junctional complex
Tight and adherens junction proteins between epithelial cells
Prevent foreign particle entry into tissues
Physical Barrier: Mucus
Secreted by mucous glands and goblet cells in epithelium
Trap foreign particles for mucociliary clearance
Physical Barrier: Pattern Recognition Receptors (PRRs)
In airway and alveoli
Detect pathogens and initiate innate immune response
Lung Reflex Barriers
In Edwin McKenzie
Cough
Sneeze
Gag
Lung Chemical Barriers
Antimicrobial peptides (AMPs)
Chemical Barrier: AMPs
In mucus
Neutralize/kill pathogens
Ex: Defensins, lysozymes, lactoferrin, IgA, collectins
AMPs: Collectins
In alveoli
Secreted by type 2 pneumocytes
Surfactant Protein A (SP-A) and Surfactant Protein D (SP-D)
Bind sugar patterns on pathogens for phagocytosis
Lung Cellular Barriers
Immune cells
Immune Cells
Epithelial cells
Neutrophils
Monocytes
Macrophages
Dendritic cells
Innate lymphoid cells
NK cells
Immune Cells: Epithelial Cells
Ciliated in airways for mucociliary clearance
Produce mucus, AMPs, and cytokines (inflammation and immune cell recruiting)
Immune Cells: Neutrophils
Phagocytes
Recruited by chemotaxis from inflammation
Enter alveolar spaces
Immune Cells: Monocytes
From bone marrow
Immature phagocytes in blood
Cannot fight infection
Recruited by chemotaxis from inflammation
Become macrophages in tissues
Immune Cells: Macrophages
Phagocytes
Etherocytosis: Resolution = Macrophages phagocytose neutrophils + self
Alveolar and interstitial macrophages
Alveolar Macrophages
In alveoli (no cilia) = Rely on macrophages to phagocytose pathogens
Migrate to bronchioles and deposit
Cilia carry to pharynx
Toll-like receptors (TLRs) bind PRR recognizing pathogen-associated molecular patterns (PAMPs)
Cause phagocytosis and secrete pro-inflammatory cytokines + chemokines
Interstitial Macrophages
In lung interstitium
Express MHC 2 proteins = Bind and present antigens to CD4+ T-cells
Produce immunosuppressive cytokines and chemokines
Regulate immune cell activity and tissue-damaging inflammation
Immune Cells: Dendritic Cells
APC
Surface MHC 1 and 2 proteins
Bind and present antigens to T-cells in lymph nodes
Initiate adaptive immune response
Produce cytokines for viral infection
Immune Cells: Innate Lymphoid Cells
Respond to distress cytokines from epithelial cells
Regulate inflammation and tissue repair
Main: ILC2
Immune Cells: NK Cells
Target abnormal host cells (virus-infected, transformed)
Produce cytokines
Failure of Respiratory System Pathways
Poor physical clearance
Disrupted mucociliary function
Impaired phagocytic and inflammatory cells
Resp System Failure: Poor Physical Clearance
No cough
Weak diaphragm and expiratory muscles
Poor epiglottis function
Resp System Function: Disrupted Mucociliary Function
Viral infections causing structural damage
Primary ciliary dyskinesia (poor cilia function)
Smoking
Resp System Failure: Impaired Phagocytic and Inflammatory Cells
Alveolar macrophage deficiencies
Viral infections, smoking, alcohol
Lung Infection Effects on Ventilation
Edema
In Airway: Increase resistance = Decrease airflow
In Pleura: Decrease compliance and lung distension = Decrease VC
Insufficient pressure to draw air in
Lung Infection Effects on Gas Exchange
Low V/Q: Decrease gas exchange (particularly CO2)
Alveolar Edema: Increase alveolar-capillary barrier space = Prevent O2 diffusion
Hypoxia
Low O2 reaching tissues
From pO2
Hypoxemia
Low O2 in blood
From SPO2
PaO2/FiO2: Indicate when patient needs O2
Low ratio = Severe shunting
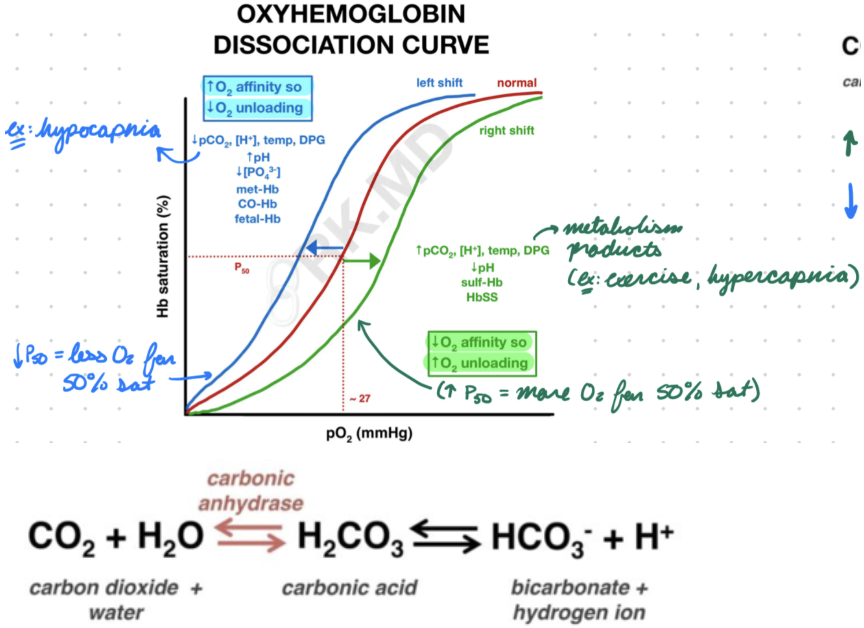
Oxyhemoglobin Curve
Hemoglobin affinity for O2
Plateau at 60-70 mmHg
Oxyhemoglobin Curve: Right Shift
Decreased hemoglobin affinity for O2
More O2 unloading into tissues
Increase P50
50% sat at higher-than-normal PO2
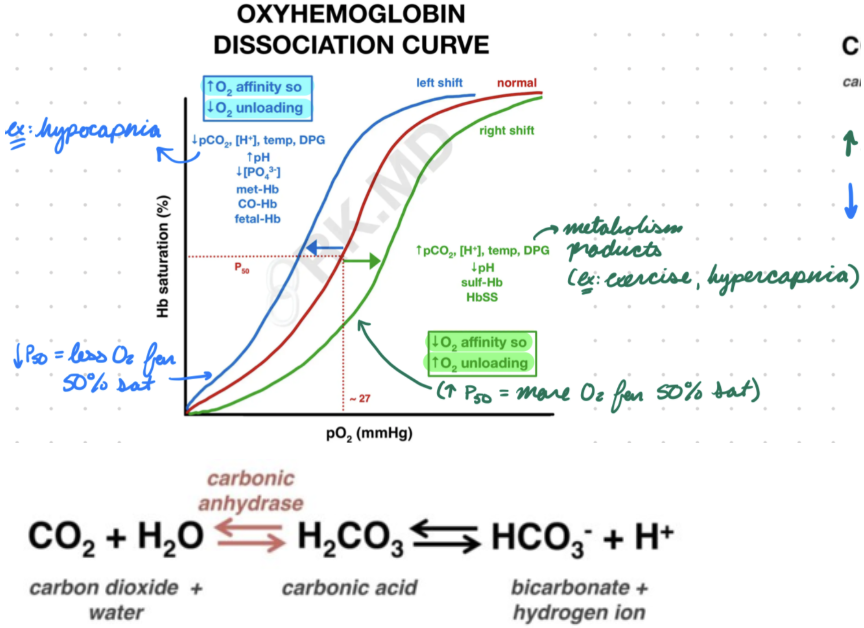
Oxyhemoglobin Curve: Left Shift
Increase hemoglobin affinity for O2
Less O2 unloading into tissues (hemoglobin bind tighter)
Decrease P50
50% sat at lower-than-normal PO2
Chest Pain Indications
Changing during Resp: Lung pathology
Unchanged during Resp: Suspect MI
Pneumonia: Description
Acute LRT infection
Acquisition:
Community: Infection outside hospital
Nosocomial: Infection in hospital setting
Location:
Lobar: In pulmonary lobes (single or multi)
Interstitial: Inflammation and fibrosis in interstitium and parenchyma
Pneumonia: Epidemiology
Very common
Risk Factors:
Younger and older age
Comorbidities (aspiration, COPD, chronic lung/heart diseases)
Viral resp infection
Smoking and alcohol
Pneumonia: Etiology
Viruses (more common) and bacteria
Viruses:
Influenza A and B
Coronavirus
Rhinovirus
Parainfluenza virus
Adenovirus
Bacteria:
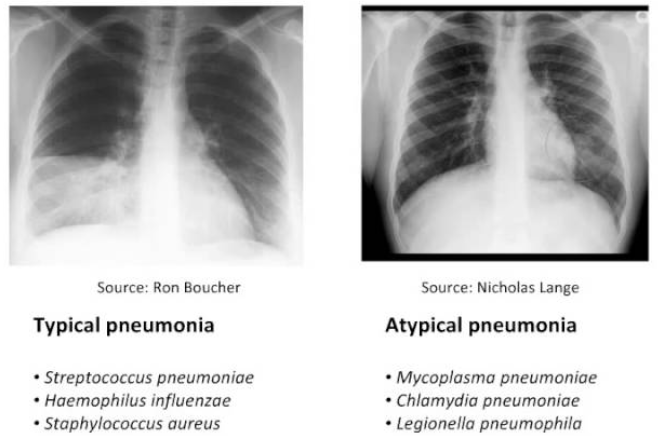
Typical:
Streptococcus pneumoniae (most common)
Group A streptococci
Atypical: Resist beta-lactams, cannot identify with traditional techniques
Legionella
Mycoplasma pneumoniae
Pneumonia: Pathogenesis
Alveolar infection
Pathogen enter LRT (droplets, aerosol)
Compete against lung microbiome
Colonize nasopharynx and alveoli
Immune system cannot clear pathogen = Inflammation
Pus in parenchyma = Decrease compliance + shunt
Immune cells increase inflammation and neutrophil chemotaxis
Pneumonia: Investigation
X-ray
Pulmonary infiltrate (opacity) → Air bronchogram (darker air-filled bronchioles on top)
Typical: Opacity in 1 lobe
Atypical: Reticular (radiating) opacity
Severe: Identify pathogen + evaluate treatment
CBC
Sputum gram stain + culture
Urinary antigen test
Pneumonia: Clinical Presentation
Fever
Resp symptoms:
Cough
Dyspnea/SOB
Chest pain
Pneumonia: Treatment/Management
Antibiotics: Target S. pneumoniae
Amoxicillin + macrolide
Abscesses: Drain + longer treatment