18.3 excitability in the myocardium (AP in contractile cardiomyocytes)
1/6
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
7 Terms
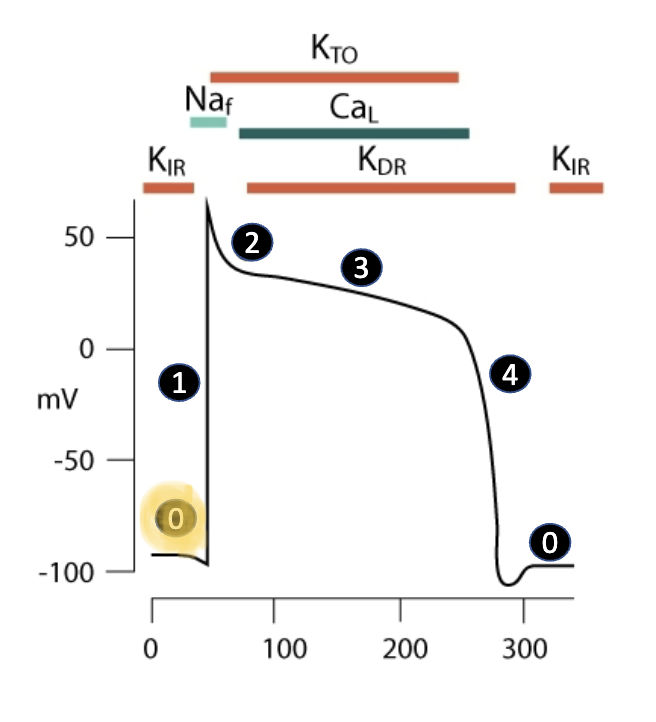
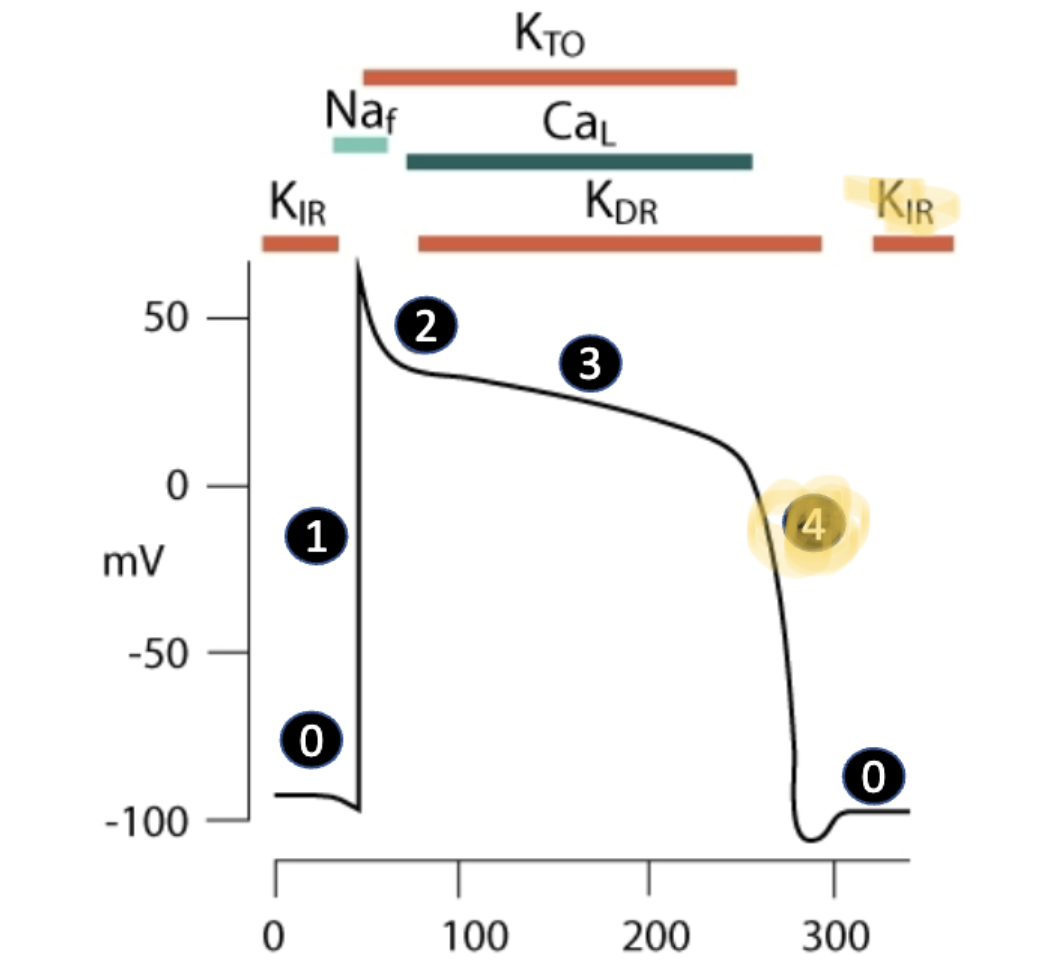
0 phase (resting membrane potential)
typically betw. -80mV and -90mV
resting membrane more negative due to protective/more intentional than skeletal muscle (no twitches)
created from continuous EFFLUX (moving out) of K+ through inward rectifier potassium channels (KIR) (keeps membrane potential low)
small amount of Ca+2 and Na+ permeability
Na/K/ATPase serves to maintain concentration gradients
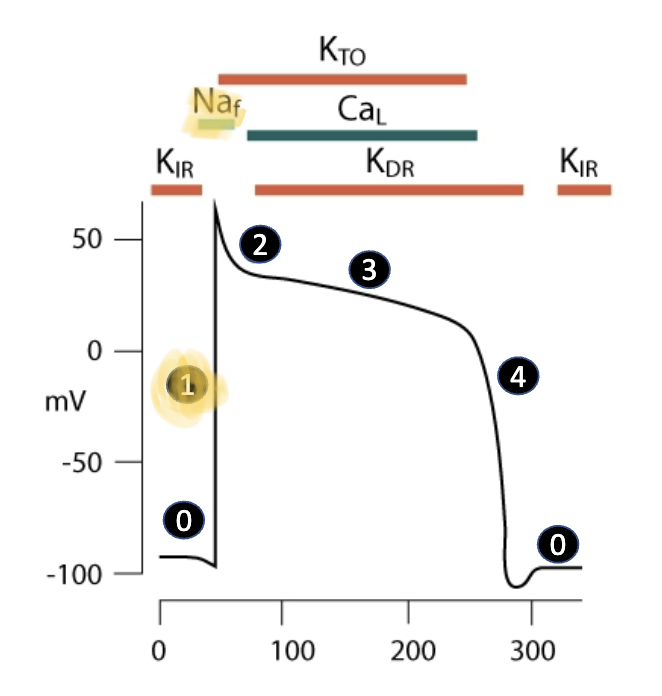
depolarization
similar process in skeletal muscle
voltage-gated fast sodium channels (Naf) are activated, allowing influx of positively charged sodium ions
cells are becoming more positive (depolarization)
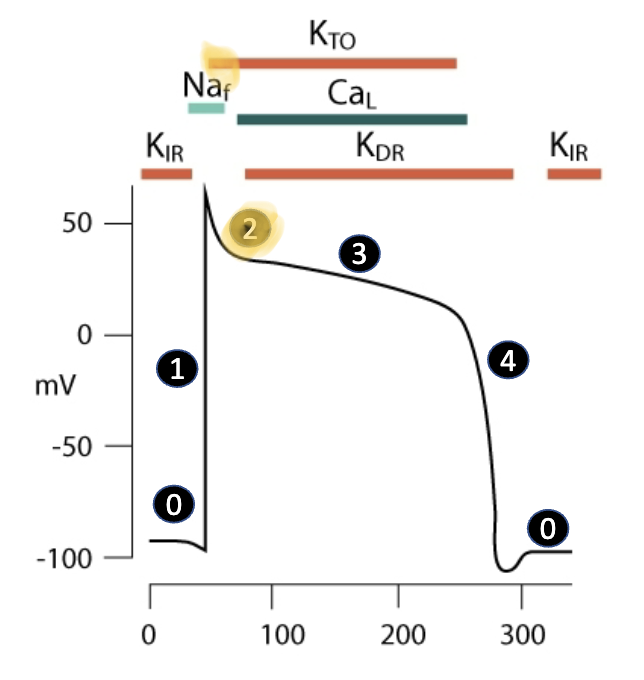
transient repolarization
voltage-gated sodium channels rapidly inactivate at the peak of AP
sodium permeability decreases since it’s TOO positive
cardiomyocytes go into refractory period
membrane potential begins to hyperpolarize due to transient outward current from K channels (K channels help maintain refractory)
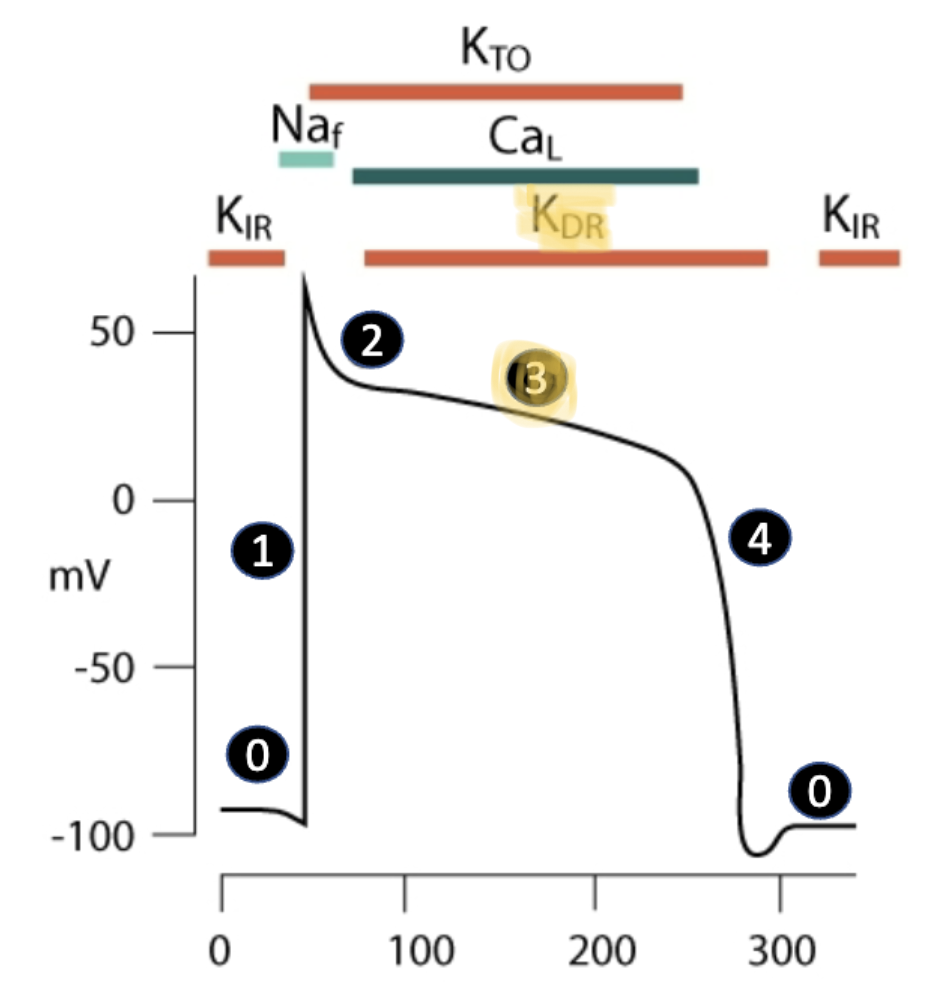
plateau phase
voltage-gated L-type calcium channels (CaL) OPEN, bringing postively-charged Ca2+ ions into cell
this is opposed by the efflux of K+ ions through delayed rectifier potassium channels (KDR)
two opposite electrical forces create plateau in membrane potential
rapid repolarization
L-type calcium channels close
efflux of K+ continues through voltage gated potassium channels
membrane potential repolarizes to resting state
excitation contraction coupling
couples together the excitation of cardio myocytes with the contraction (AP traveling thru the muscle)
calcium induced calcium released (CICR)
the Ca+ goes through the LTCC (L-type calcium channel, voltage gated), is enough to open the “door” (Rynodine receptor, RyR) and is enough to induce Ca+ release from the sarcoplasmic reticulum, but NOT ENOUGH TO STIMULATE A CONTRACTION