lab med | Quizlet
1/153
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
154 Terms
Which of the following conditions is not characterized by eosinophilia?
A. Atopic dermatitis
B. Trichinosis
C. Bronchial asthma
D. Cushing syndrome
E. Scarlet fever
D. Cushing syndrome
Which of the following tends to decrease in the course of hemolytic anemia?
A. Albumin
B. Ceruloplasmin
C. C-reactive protein
D. Transferin
E. Haptoglobin
E. Haptoglobin (page 63 in Viggs notes)
After a hemolytic episode haptoglobin concentration falls, since it is all used up, as haptoglobin cleans free hemoglobin in the bloodstream.
Which of the following laboratory tests is not recommended for the periodic assessment of the metabolic condition of a patient diagnosed with type 1 DM?
A. TSH
B.Lipid profile
C. Autoantibodies to GAD65
D. Albuminuria
E. HbA1c
C. Autoantibodies to GAD65
(this is only a diagnostic tool)
A 35-year-old diabetic woman is diagnosed with autoimmune hemolytic anemia. What is the test recommended for the monitoring of diabetes control in that case?
A. Glucosamine
B. HbA1c
C. HbS
D. Fructosamine
E. HbC
Fructosamine
(need help verifying. HbA1c cannot be used because of the low erythropioesis that occurs during anemia)
What is the most probable pattern of MCV and RDW values in a 69•year•old woman diagnosed with anemia of iron and vitamin B12 deficiency?
A. MCV 84 fL; RDW 13,0% no
B. MCV 79 fL; RDW 17,5% no
C. MCV 102 fL; RDW 10,0% no because mcv is normal
D. MCV 118 fL; RDW 16,5%
E. MCV 88 fL; RDW 18,5%
E. MCV 88 fL; RDW 18,5%
• Iron-deficiency anemia usually presents with increased RDW and low MCV.
• Folate and vitamin B12 deficiency anemia usually presents with normal RDW and high MCV.
• Mixed-deficiency (iron + B12 or folate) anemia usually presents with high RDW and variable
MCV
Which of the following statements concerning paraneoplastic syndrome is true?
A. It is caused by decreased ACTH secretion in lung cancer patients
B. It is a remote effect of malignancy
C. It is caused by acute tumor lysis syndrome
D. It is caused by compression of growing tumor on surrounding tissues
E. It does not cause SIADH
B. It is a remote effect of malignancy
Which of the following statements concerning fecal occult blood test (POBT) is not true?
A. It is a screening test for colon cancer
colon cancer or polyp in the colon/rectum)
B. Requires diet modification
C. It is recommended to perform the analysis once a year after 45 years
D. It is a screening test for anemia
E. It can produce false-positive results
D. It is a screening test for anemia
What is the recommended screening for prostate cancer?
A. Human chorionic gonadotropin
B. Alpha fetoprotein
C. Prostate biopsy
D. Prostate specific antigen and transrectal ultrasound
E. Prostate specific antigen
D. Prostate specific antigen and transrectal ultrasound
What is a tumor marker used for the monitoring of colorectal cancer patients after surgery?
A. Calcitonin
B. Human chronic gonadotropin
C. CA 19.9
D. Alpha fetoprotein
E. Carcinoembryonic antigen
E. Carcinoembryonic antigen (CEA)
"Monitoring the patient after gastric cancer surgery
with both: CEA and CA 19-9 is the gold standard
What is the best answer describing skeletal and mineral metabolism in a 62-years- old uremic male?
A. Calcium normal, phosphate high, 25 hydroxyvitamin D normal, 1.25 - dihydroxy vitamin D low, PTH high
B. Calcium low, phosphate normal, 25-hydroxyvitamin D low, 1.25 - dihydroxy vitamin D normal, PTH high
C. Calcium low, phosphate high, 25-hydroxyvitamin D normal, 1.25 - dihydroxy vitamin D low, PTH high
D. Calcium high, phosphate low, 25-hydroxyvitamin D normal, 1.25 - dihydroxy vitamin
D low, PTH high
E. Calcium normal, phosphate low, 25-hydroxyvitamin D normal, 1.25 - dihydroxy vitamin D high, PTH high
C. Calcium low, phosphate high, 25-hydroxyvitamin D normal, 1.25 - dihydroxy vitamin D low, PTH high
n uremic patients, especially those with chronic kidney disease, the kidneys have difficulty converting 25-hydroxyvitamin D into the active 1,25-dihydroxyvitamin D. This leads to low levels of 1,25-dihydroxyvitamin D, and since calcium absorption is dependent on active vitamin D, the calcium level may be low. The body compensates by increasing parathyroid hormone (PTH) to raise calcium levels by mobilizing calcium from the bones and increasing calcium reabsorption in the kidneys, which often results in high PTH. Additionally, because the kidneys are unable to excrete phosphate properly, phosphate levels tend to be high in uremic patients.
What is not a risk factor of urolithiasis in a 34-year-old man?
A. Hypercalciuria
B. Hyperoxaluria
C. Hypomagnesuria
D. Hypercitraturia
E. Hyperuricosuria
D. Hypercitraturia
What is not a risk factor of hypocalcemia in a 69-year-old woman with chronic renal
failure?
A. Vitamin D deficiency
B. Hypoalbuminemia
C. Secondary hypoparathyroidism
D. Hypophosphatemia
E. Renal failure (obviously)
D. Hypophosphatemia (its HYPERphosphatemia that causes Hypocalcemia)
What is the eGFR value characterizing stage 3 of chronic kidney disease (CKD)?
A. 0 - 14 ml/min/1.73m2
B. 90 - 150 ml/min/1.73m2
C. 30 - 59 ml/min/1.73m
D. 15-29 ml/min/1.73m2
E. 60 - 89 ml/min/1.73m2
C. 30 - 59 ml/min/1.73m
Which of the following is not characteristics of pre-renal acute renal failure?
A. Fractional excretion of sodium higher than 2%
B. Normal urinalysis yes
C. Decreased urine output
D. Urine osmolality higher than 500 mOsm yes
E. BUN/creatinine ratio > 20.1
A. Fractional excretion of sodium higher than 2%. Yes should be <1%
5. A 42-year-old man was admitted to the hospital because of severe edema and marked reduction of urine output. Past medical history included respiratory tract infection two weeks ago. Physical examination revealed generalized edema. His arterial blood pressure was 100/60 mmHg. Laboratory test results at admission were as following: HGB 8,8 mmo1/1, HCT (hematocrit test) 45% , RBC 4,9 x1012/L, WBC 13,4 x109/L (high), PLT 560 x109/L (high). Plasma Na+ 139 mmol/l, K+ 4,6 mmo1/1, Creatinine 0,7 mg/d1 Total protein 51,0 g/L, albumin 40%, Total-Cholesterol 430 mg/dL, fibrinogen 530 mg/dL. Urinalysis: sg 1046 g/L, pH 7,0, protein 650 mg/dl, glucose — negative, leukocytes 1-3 per HPF
A. Exacerbated chronic pyelonephritis
B. Acute renal failure
C. Acute glomerulonephritis
D. Nephrotic syndrome
E. Acute urinary tract infection
D. Nephrotic syndrome
Generalized edema → Classic sign of nephrotic syndrome.
Proteinuria (650 mg/dL) → Suggests significant protein loss in urine.
Hypoalbuminemia (Total protein 51 g/L, albumin 40%) → Due to excessive urinary protein loss.
Hyperlipidemia (Total cholesterol 430 mg/dL) → Compensatory mechanism for low oncotic pressure.
High fibrinogen → Nephrotic syndrome is a hypercoagulable state.
Normal creatinine (0.7 mg/dL) → Suggests preserved renal function, ruling out acute renal failure.
A 19-year-old woman was admitted to the hospital because of red-colored urine present for a few days. Physical examination revealed mild edema of eyelids. Her blood pressure was 180/120 mmHg. Laboratory test results at admission were as following: HGB 7,8 mmol/L, Creatinine 0,9 mg/dl; Total protein 71,0 g/L (albumin 55%). Urinalysis: s.g. 1012 g/L, pH 6,7, protein - trace, glucose - negative, leukocytes 3-4 per HPF, erythrocytes - a large number. Contrast phase microscopic examination revealed over 90% dysmorphic erythrocytes, urine was reduced to 500 ml/day.What is the most probable diagnosis?
A. Nephrotic syndrome
B. Acute pyelonephritis
C. Acute glomerulonephritis
D. Acute renal failure due to sepsis no, leukocytes are not elevated
E. Urolithiasis
C. Acute glomerulonephritis
Red-colored urine (hematuria) with dysmorphic erythrocytes (indicating glomerular origin of bleeding).
Edema and high blood pressure (which are commonly seen in glomerulonephritis).
Proteinuria (trace amount).
Decreased urine output (oliguria), with the patient producing only 500 mL/day of urine.
A 56-year old woman had a fever for the past three days. she also had burning dysuria. on physical examination, her temperature is 37,7 C. laboratory studies shows HGB 13,1 g/dL, HCT 40,2%, MCV 86 fL, PLT 226x10^9 and WBC 12,6x10^9/L. A urine dipstick analysis shows s.g. 1.017, pH 6,0; leukocyte esterase-positive, nitrite positive, protein negative, glucose negative, and blood-negative. based on the clinical symptoms and laboratory test results, she is suspected of a urinary tract infection. Which of the following findings of the microscopic examination would also suggest that disease?
A. hyaline casts
B. renal tubular epithelial cells
C. red blood cell casts
D. oval fat bodies
E. white blood cell casts
E. white blood cell casts
A 35-year-old man has had nausea, vomiting, and severe colicky right flank pain radiating into the thigh lasting 3 hours. He is afebrile. Urinalysis shows: RBCs covering the field with no RBC casts, mild proteinuria, pyuria, and bacteriuria. Which of the following is the most likely diagnosis?
A. Acute glomerulonephritis
B. Bladder carcinoma
C. Urolithiasis
D. Urinary tract tuberculosis
E. Renal cell carcinoma
C. Urolithiasis (RIGHT COLICKY PAIN IS THE GIVE AWAY)
A 15-year-old boy is being diagnosed because of jaundice and recurrent acute bone pains. Complete blood count (CBC) reveals HGB 6,5 g/dL, MCV 82,3 fL, PLT 465x109/L, WBC 9,8x109/L, RET 170x109/L, and bilirubin 3,4 mg/dL. What is the most probable type of anemia?
A. Anemia of chronic diseases
B. Anemia of acute blood loss
C. Folate deficiency anemia
D. B12 deficiency anemia
E. Hemolytic anemia
E. Hemolytic anemia (jaundice is the giveaway)
Why Is Hemolytic Anemia the Best Answer?
✔ Jaundice and high bilirubin → Suggest increased RBC breakdown.
✔ High reticulocyte count → Bone marrow is trying to compensate.
✔ Recurrent bone pain → Suggestive of sickle cell disease, a common hemolytic disorder.
,
Option | Why Incorrect? |
|---|
A. Anemia of chronic diseases | Usually presents with low reticulocytes and low iron, which are not seen here. |
B. Anemia of acute blood loss | Would show normal bilirubin and low reticulocyte count early on. This patient has chronic symptoms. |
C. Folate deficiency anemia | Causes macrocytic anemia (high MCV), but this patient has a normal MCV. |
D. B12 deficiency anemia | Also causes macrocytic anemia (high MCV), often with neurological symptoms. |
What are the most useful parameters for the differential diagnosis of microcytic anemia?
A. Plasma iron concentration and CRP
B. Bone marrow biopsy and hemoglobin electrophoresis
C Ferritin concentration and sTfR
D Red blood cell indices and CRP
E. Blood smear and reticulocyte count
C Ferritin concentration and sTfR
A 70-year-old man received the following CBC result: HGB 7,1 g/dl (low), RBC 2,50x1012/L (low), HCT 25% (low), MCV 88 fL (normal), RDW 36,5% (high), MCH 30 pg (normal), WBC 3,2x109/L (low), PLT 105x109/L (low), RET 9,2x109/L (very low). What is the most probable cause of anemia in that case?
A. Iron deficiency
B. Iron and B12 deficiency
C. Bone marrow fibrosis
D. Extracellular hemolysis
E. B12 or folate deficiency
C. Bone marrow fibrosis
What does monocytosis characterize?
A. Recovery stage from agranulocytosis
B. Infectious mononucleosis
C. Temporal arteritis
D. Scarlet's fever
E. Pertussis
A. Recovery stage from agranulocytosis
A 26-year-old obese male patient with no diabetes and negative familial history for cardiovascular disease (CVD) has the following fasting results: T-Cholesterol 172 mg/dl. HDL 28 mg/dL low, LDL 79 mg/dL. TG 325 mg/dL high . What is the appropriate interpretation of his lipid profile?
A. Because of negative familial history for CVD patient should start lipids assessment at his age of 45
B. Lipid profile reflects atherogenic dyslipidemia related to the patient's obesity
C. It is normal lipid metabolism
D. The patient should be diagnosed with primary hyperlipoproteinemia
E. All lipid parameters are within reference values for patients without diabetes
B. Lipid profile reflects atherogenic dyslipidemia related to the patient's obesity
Low HDL and high TG: This combination is characteristic of atherogenic dyslipidemia, which is commonly seen in patients with obesity, metabolic syndrome, and insulin resistance. The patient’s TG of 325 mg/dL is elevated, and his HDL is low, which increases his risk for atherosclerosis and cardiovascular disease.
A 26-year-old woman came to her family doctor because of fever up to 39,5oC, sore throat, and lymphadenopathy. Physical examination revealed swollen tonsils covered with white exudate. Laboratory test results were as following: WBC 18,1x109/L (high), Neutrophils 79%, Lymphocytes 15%, Monocytes 4,2%, Eosinophils 0,3%, Basophils
1,5%, CRP 84mg/L, ESR 42mm/h. What is the most probable diagnosis?
A. Streptococcal pharyngitis
B. Diphtheria (grey exudate)
C. Adenoviral pharyngitis
D. Infectious mononucleosis
E. Pertussis
A. Streptococcal pharyngitis (white exudate)
A 25-year-old female patient, office worker, with no complaints, had routine, periodic medical examination with the following results: BP 120/80 mmHg. BMI 25 kg/m2(good), T-Cholesterol 185 mg/dL, LDL 110 mg/dL, HDL 38 mg/dL, TG 169 mg/dL, waist circumference 90 cm, fasting glucose 80 mg/dL. Based on the obtained results, an increase of consumption of which of the following you would advise?
A. Industrial trans fatty acids
B. Palmitic fatty acid (SFA)
C. Polyunsaturated fatty acids n-3
D. Stearic acid
E. Saturated fatty acids
C. Polyunsaturated fatty acids n-3- adding these can lower LDL and raise HDL
40-year-old healthy man, after 16 hours fasting obtained the following lipid results:
T-Cholesterol 185 mg/dL (normal), LDL 124mg/dL (high, > 100), HDL 46 mg/dL (low. normal should be 60 or >), TG 75 mg/dL (normal, they should be less than 150). His BP was 125/85 mmHg (prehypertension up to 140) and BMI 21kg/m2 (normal). Based on the obtained results, what kind of diet modification would you recommend in that case?
A. Decreased trans fatty acids consumption
B. Increased citrus fruits consumption
C. Increased green vegetable consumption
D. Increased sugar consumption
E. Increased alcohol consumption
A. Decreased trans fatty acids consumption
What is a primary target for the therapy in a patient diagnosed with coronary heart disease and hyperlipidemia?
A. Plasma total cholesterol level
B. Plasma lipoprotein (a) level
C. Plasma triglycerides level
D. Plasma LDL cholesterol level
E. Plasma HDL cholesterol level
D. Plasma LDL cholesterol level
An 81-year-old man was admitted to the hospital because of dyspnea, cough, and fever up to 38,5 present for the last two days. Physical examination revealed fine rales over the right lung. Laboratory test results were as following: WBC 21,0x109/L, Neutrophils 89%, Lymphocytes 5%, Monocytes 4,2%, Eosinophils 0,3%, Basophils 1,5%, CRP 153mg/L, ESR 51mm/h. What is the most probable diagnosis?
A. Pertussis
B. Candida albicans infection
C. Myocardial infarction
D. Bacterial pneumonia
E. Pneumothorax
D. Bacterial pneumonia
A 35-year-old healthy man, after 16 hours fasting obtained the following lipid results: T-Cholesterol 150 mg/dL, LDL 105 mg/dL, HDL 30 mg/dL(too low) TG 75 mg/dL. His BP was 123/82 mmHg and BMI 23 kg/m2. Based on the obtained results, what kind of diet modification would you recommend in that case?
A. Reduction of fat intake
B. Reduction of alcohol intake
C. Use of an increased amount of soluble dietary fiber
D. Decrease of dark chocolate and nuts consumption
E. Consumption of an increased amount of fish and n-3 fatty acids
E. Consumption of an increased amount of fish and n-3 fatty acids (this raises HDL)
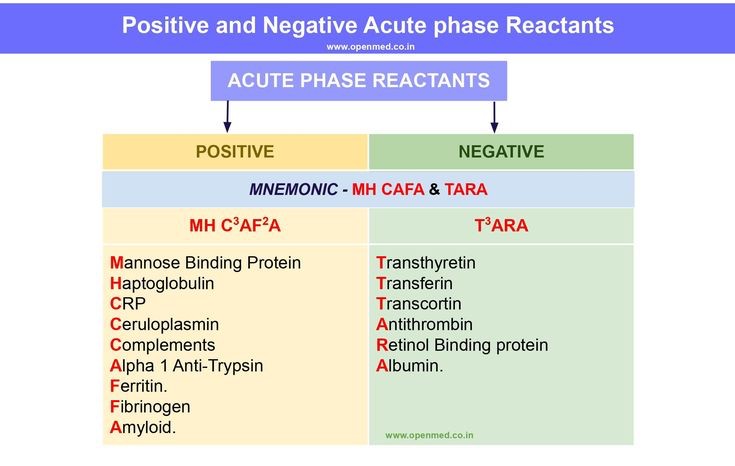
What are the negative acute-phase proteins?
A. Albumin, transferrin
B. Ceruloplasmin, alpha-1-antitrypsin, albumin
C. Fibrinogen, transferrin, albumin
D. Fibrinogen, ferritin, albumin
E. Haptoglobin, alpha-2-macroglobulin, transferrin
A. Albumin, transferrin (in his notes page 153 right column)
A 23-year-old student underwent some screening for cardiovascular disease risk factors. Laboratory test results (fasting) were as following: T-Cholesterol 235 mg/dL, HDL 28 mg/dL, TG 1450 mg/dL. Which of the following conditions may result from lipids abnormalities present in that man?
A. Acute pancreatitis
B. Acute hepatitis
C. Chronic kidney disease
D. Acute appendicitis
E. Acute kidney disease
A. Acute pancreatitis (TG over 1000)
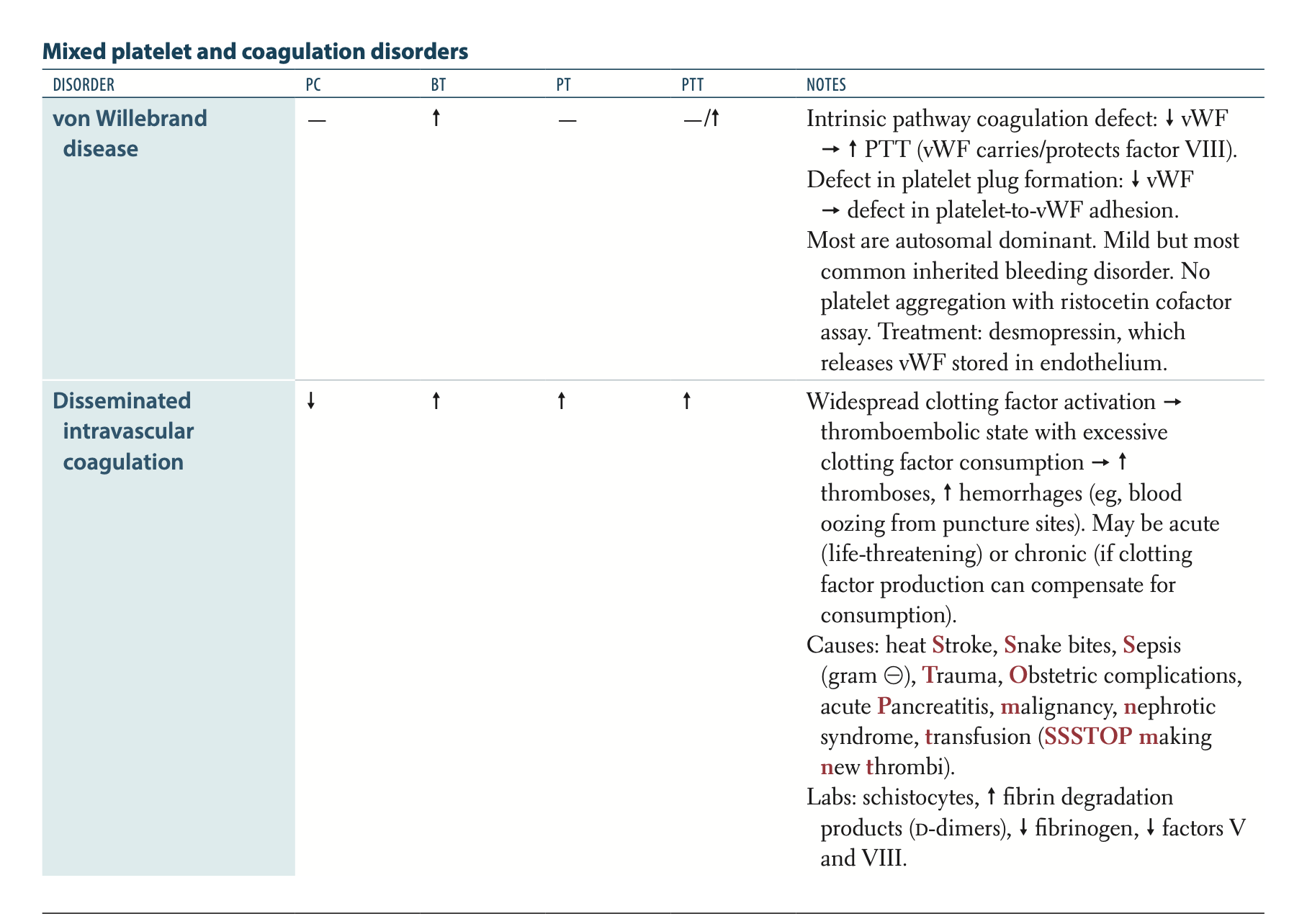
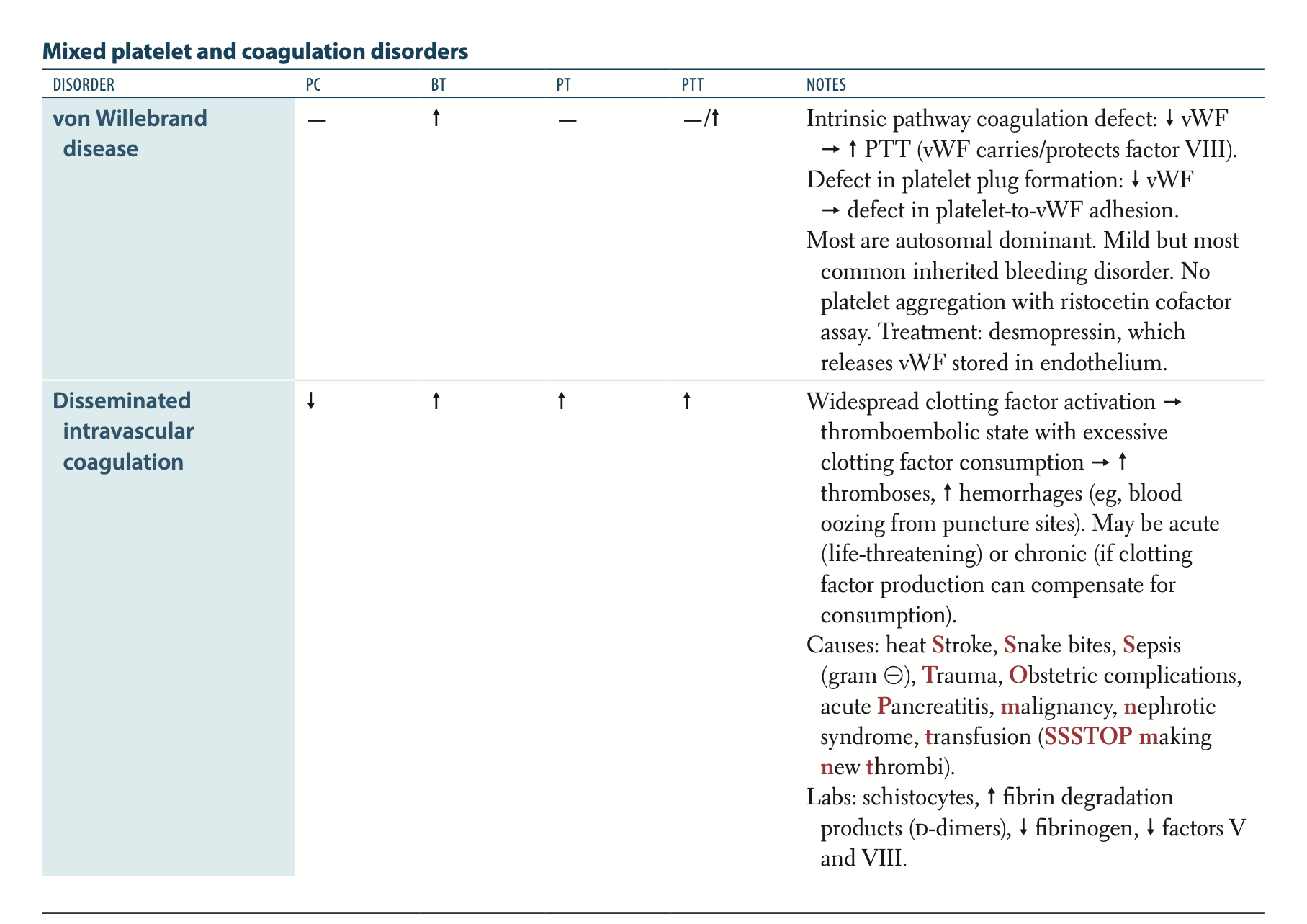
Which of the following abnormalities are characteristic of disseminated intravascular coagulation (DIC)?
A. Low platelets count, increased INR and aPTT, low D-dimers, high fibrinogen
B. Increased platelets count, decreased INR and aPTT, low D-dimers, elevated
fibrinogen
C. Low platelets count, increased INR and aPTT, high D-dimers, low fibrinogen
D. Low platelets count, decreased INR and aPTT, low D-dimers, low fibrinogen
E. Low platelets count, decreased INR and aPTT, high D-dimers, low fibrinogen
Low platelets count, increased INR and aPTT, high D-dimers, low fibrinogen (notes
page 66 of VIGGS doc) DIC is always associated with high-D-dimers
A 22-year-old man came to his family doctor because of the yellow sclera that he experienced for the second time (first time during the flu and now after an overnight work and stress). Physical examination revealed no abnormalities except for slight jaundice. Laboratory tests results were as following: WBC 6,9x109/L; RBC 5,2x1012/L; HGB 15,3 g/dL; HCT 47 %; MCV 87 fL; MCH 29 pg; RDW 13%; PLT 276 x109/L; RET 80x109/L. CRP 1 mg/L, ALT 30 IU/L, AST 32 IU/L, GGT 28 IU/L, ALP 62 IU/L, Bilirubin 3,6 mg/dL, PT 10 sec, Albumin 50 g/L. Serum protein electrophoresis: normal.
Urinalysis: normal. What is the most probable diagnosis?A. Hemolysis
B. Liver cirrhosis
C. Chronic viral hepatitis
D. Alcohol abuse
E. Gilbert's syndrome
E. Gilbert's syndrome (stress and prior infection)
A 31-year-old woman was complaining of polyuria and polydipsia. Her body weight decreased by 3 kilograms during the past three weeks. Her fasting plasma glucose concentration was 250 mg/dl? What is the most probable cause of her symptoms?
A. Urinary tract infection
B. Diabetes mellitus
C. Impaired fasting glycemia
D. Impaired glucose tolerance
E. Pregnancy
B. Diabetes mellitus
Which of the following statements concerning procalcitonin is false?
A. In the course of severe bacterial infection, it is produced by the cells of the lung, the intestine, the kidney, and the liver response to bacterial infections but also in response to tissue injury.
B. Procalcitonin is used for differentiation of patients with SIRS from sepsis
C. Its level correlates with the patients condition
D. In the course of sepsis CRP is a better marker than procalcitonin
E. The level of procalcitonin doesn't rise significantly in the course of viral
infections
D. In the course of sepsis CRP is a better marker than procalcitonin
A 76-year-old male patient was admitted to the hospital because of fatigue, low grade fever, weight loss of 7kg during the past 6 months, severe pain and stiffness of shoulders and hips. Laboratory tests results were as following: HGB 10,8g/d1, MCV 83fL, RBC 3,36x1012/L, HCT 34,1%, WBC 8,75x109/L, Neutrophils 65%, Lymphocytes 25%, Monocytes 5,2%, Eosinophils 3,3%, Basophils 1,5%, ESR 105mm/h, CRP 87mg/L, RF 5 IU/mL (N<14 IU/mL), uric acid 3,5mg/d1. What is the most probable diagnosis?
What is the most probable diagnosis?
A. Gouty arthritis
B. Rheumatoid arthritis
C. Loffler's syndrome
D. Reactive arthritis
E. Polymyalgia rheumatica
Polymyalgia rheumatica (ESR is very high and along with temporal arteritis is the only one that could have an ESR over 90....so it has to be this
Reasoning:
Polymyalgia rheumatica (PMR) typically presents with severe pain and stiffness in the shoulders and hips, often in elderly individuals. This patient has a history of musculoskeletal pain that is characteristic of PMR.
Elevated ESR (105 mm/h) and CRP (87 mg/L) are highly suggestive of inflammation and are frequently seen in PMR, a condition known for causing systemic inflammation.
The patient’s weight loss, fatigue, and low-grade fever are common systemic manifestations of PMR.
Normal RF (5 IU/mL) and normal uric acid (3.5 mg/dL) make conditions like rheumatoid arthritis and goutless likely, as these conditions would typically show elevated RF or increased uric acid levels.
A 25-year-old healthy female undergone assessment of her lipid profile with the following results: T-Cholesterol 167 mg/dL, TG 290 mg/dL. HDL 70 mg/dL, LDL 90 mg/dL. What is the most likely cause of triglyceride levels in this case?
A. Malnutrition
B. Non-fasting condition
C. Undiagnosed hyperthyroidism
D. Developed neoplastic disease
E. Undiagnosed hypothyroidism
B. Non-fasting (postprandial) condition (TGs being that high with low cholesterol is very
rare)
Which of the following statements concerning oral glucose tolerance test (OGTT) is not true?
A. OGTT is not used in the routine diagnostics of diabetes mellitus
B. The patient can go for a walk during the test
C. 2 hours' plasma glucose between 140-200 mg/dL is referred to as impaired glucose
tolerance
D. The patient should fast overnight before the test
E. An unrestricted carbohydrate diet is advised for three days before the test
B. The patient can go for a walk during the test
A 72-year-old diabetic male was found unconscious. On admission, his laboratory test results were as following: WBC 6,4x109/L, RBC 5,0x1012/L, HGB 14,8 g/dL, HCT 48%, MCV 88 fL, MCH 30 pg, MCHC 35 g/dL, RDW 13,7 %, PLT 310x109/L. Glucose 850 mg/dL, Na' 144 mmol/L, K+ 5.1 mmol/L, creatinine 2,1 mg/dL. Urinalysis: pH 6.0, s.g. 1026, PRO 150 mg/L, GLU 7,5 g/dL, KET negative, BIL negative, URO 0,2 U/dL, BLO negative, NIT negative, Leu 0-2/HPF, hyaline casts, single bacteria. Arterial blood gasometry: pH 7,34; p02 84 mmHg; pCO2 40 mmHg; HCO3- 19 mmol/L; BE (-) 2,5 mmol/L. What is the kind of patients' glucose metabolism disorder?
A. Well-controlled diabetes
B. Hyperglycemic hyperosmolar state
C. Hypoglycemic coma
D. Diabetic ketoacidosis
E. Unclassified hyperglycemia
B. Hyperglycemic hyperosmolar state
What are the conditions resulting in the elevated ESR?
A. Dehydration, old age, tuberculosis
B. Dehydration, neoplastic disease, temporal arteritis
C. Anemia, dehydration, rheumatoid arthritis
D. Polymyalgia rheumatica, pregnancy, Hodgkin's disease
E. Tuberculosis. dehydration, bacterial pneumonia
D. Polymyalgia rheumatica, pregnancy, Hodgkin's disease
Erythocyte sedimentation rate (ESR)
Used to Monitor disease activity ⇒ Polymyalgia rheymatica, temporal arteritis ⇒ *>90mm/h* Rare of RBC sedimentation in 1 hour (Via Antocoagulate blood is left to set and analysis of fall of RBC).
• Normal ESR increase: Menstruation, pregnancy, age (>50)
Factors accelerating ESR rate:
• Increased fibinogen, Increased globulin, Anemia, Increases cholesterol, decreased albumin, inflammatory diseases, cancer, hyperfibrynogenemia.
• Bacterial infections
• >100mm/h ⇒ Metastases of cancer
A 78-year-old female patient presented with numbness of fingers and "weird" pains moving down the spine. She was pale, complaining of troubles with memory. Her CBC revealed: HGB 7,8g/dL, MCV 112fL, WBC 4,0x109/L, PLT 350x109/L. What is the most probable cause of anemia?
A. Autoimmune hemolytic anemia
B. B12 deficiency
C. Acute blood loss
D. Congenital spherocytosis
E. Folate deficiency
B. B12 deficiency (known to affect CNS)
A 25-year-old woman with no previous medical history and no current medical problems had the routine, periodic medical examination with the following results (laboratory test fasting): waist circumference 80 cm; BP 120/80 mmHg, BMI 23,5kg/m2, T-Cholesterol 155 mg/dL, LDL 87 mg/dL, HDL 44 mg/dL, TG 119 mg/dL; glucose 80 mg/dl. What is the appropriate interpretation of the above results?
A. She should be ordered OGTT
B. She presents with abnormal lipids profile
C. She should be diagnosed with diabetes mellitus
D. She is healthy, and her results are characteristic of gender and age
E. She should be diagnosed with metabolic syndrome
D. She is healthy, and her results are characteristic of gender and age
Which of the following abnormalities is present in the cause of hemolytic anemia?
A. Increase of conjugated bilirubin concentration
B. Reduction of lactate dehydrogenase activity
C. Increase of unconjugated bilirubin concentration
D. Increase of haptoglobin concentration
E. Decrease of unconjugated bilirubin concentration
C. Increase of unconjugated bilirubin concentration
A 41-year-old woman was admitted to the hospital because of general weakness, weight loss of 5 kg during the past six months, and early morning, the long-lasting stiffness of the joints of hands and feet. Physical examination revealed generalized pallor and swollen, warm and painful joints. Blood test results were as following: HGB 9,8g /dl, MCV 81fL, RBC 3,36x1012/L, HCT 32,1%, WBC 9,1x109/L, ESR 85mm/h, CRP 67mg/Lhigh, RF 54 IU/mL high (N<14 IU/mL), uric acid 4mg/dL. What is the most probable diagnosis?
A. Reactive arthritis
B. Gouty arthritis
C. Fibromyalgia
D. Rheumatoid arthritis
E. Polymyalgia rheumatica
D. Rheumatoid arthritis
Which of the following statements concerning haptoglobin is true?
A. Haptoglobin is one of the negative acute-phase proteins
B. Haptoglobin concentration increases in the course of hemolytic anemia
C. Haptoglobin combines with myoglobin
D. Haptoglobin is produced in the small intestine
E. Haptoglobin concentration decreases in the course of hemolytic anemia
Haptoglobin concentration decreases in the course of hemolytic anemia
in hemolytic anemia, haptoglobin is consumed as it binds to free hemoglobin released from lysed red blood cells, leading to a decrease in its concentration.
A 64-year-old man, non-smoker with a BMI of 27.5 kg/m2, was diagnosed with a moderate stage of peripheral artery disease and hypercholesterolemia. His lipid profile was then as following: T-Cholesterol 362 mg/dL, TG 160 mg/dL, HDL 37 mg/dL, LDL 293 mg/dL. He underwent hypolipemic monotherapy followed by combined hypolipemic therapy in addition to lifestyle intervention for 12 weeks, resulting in the following laboratory tests values: T-Cholesterol 324 mg/dL, TG 90 mg/dL, HDL 41 mg/dL, LDL 265 mg/dL, and glucose 90 mg/dL. What is the most probable cause of his lipid profile
abnormalities?
A. Alcohol abuse
B. Acute hepatitis
C. Systemic vasculitis
D. Addison's disease
E. Hypothyroidism
E. Hypothyroidism
A 34-year-old man came to his family doctor because of fever up to 39oC, sore throat, lymphadenopathy, and splenomegaly. Physical examination revealed swollen tonsils with a thick coating. Laboratory tests results were as following: WBC16,18x109/L Neutrophils 39%, Lymphocytes 55%, Monocytes 4,2%, Eosinophils 0,3%, Basophils 1,5%, CRP 4mg/L, ESR 10mm/h. What is the most probable diagnosis?
A. Pertussis
B. Diphtheria
C. Adenoviral pharyngitis
D. Streptococcal pharyngitis
E. Infectious mononucleosis
E. Infectious mononucleosis (lymphocytosis and splenomegaly)
A 37-year-old female with BMI 30 kg/m2 was ordered OGTT with the following result: 0 min: 99 mg/dL and 120 min: 190 mg/dL. What type of glucose metabolism disorder in present in that case?
A. Impaired glucose tolerance
B. Normal glucose tolerance
C. Impaired fasting glycemia
D. Type 1 diabetes mellitus
E. Type 2 diabetes mellitus
A. Impaired glucose tolerance
Diagnostic Criteria for Glucose Metabolism Disorders
Condition | Fasting Glucose (mg/dL) | 2-Hour OGTT (mg/dL) |
|---|---|---|
Normal Glucose Tolerance | <100 | <140 |
Impaired Fasting Glucose (IFG) | 100–125 | <140 |
Impaired Glucose Tolerance (IGT) | <126 | 140–199 |
Diabetes Mellitus | ≥126 | ≥200 |
mpaired Glucose Tolerance (IGT) is a prediabetic condition, meaning that blood glucose levels are higher than normal but not high enough to be classified as diabetes. It is a strong risk factor for developing Type 2 Diabetes Mellitus (T2DM), cardiovascular disease (CVD), and metabolic syndrome.
A 58-year-old male patient with eight years' history of chronic type C viral hepatitis was systematically monitored with laboratory tests. His recent laboratory test results were as follows: AST 65 IU/L, ALT 54 IU/L, ALP 185 U/L, AFP 835 pg/L (N<15 pg/L).
What is the most probable diagnosis?
A. Alcohol abuse
B. Hepatocellular carcinoma
C. Autoimmune hepatitis
D. Chronic hepatitis
E. Drug-induced liver injury
B. Hepatocellular carcinoma (fairly confident due to the presence of chronic Hep C and
elevated AFP)
Which of the following is the marker of heart failure? (please help confirm)
A. NT-proBNP
B. h-FABP
C. Myoglobin
D. CKMB mass
E. cTnl
A. NT-proBNP
A 51-year-old man admitted to the hospital because of sudden onset of crushing chest pain. Troponin T concentration was measured at admission. 3 hours and 6 hours after admission with the following results : 0.007 - 0.012 - 0.210 ng/mL. (N<0.019ng/mL) What is an adequate interpretation of troponin results?
A. The patient needs another troponin measurement 12 hours after admission
B. Diagnosis of aborted MI
C. Diagnosis of with acute myocardial infarction (MI)
D. The patient needs the determination of CKMB mass concentration to make the
diagnosis
E. Diagnosis of unstable angina
C. Diagnosis of with acute myocardial infarction (MI)
What is the acid-base disorder in the patient with the following result of arterial blood gasometry? pH 7,17; pCO2 12,0 mmHg; p02 101,9 mmHg, s02 95,8%, HCO3- 7,2 mmol/L; BE (-)20,2 mmol/L? •
A. Partially compensated respiratory acidosis
B. Respiratory alkalosis and metabolic acidosis
C. Partially compensated respiratory alkalosis
D. Partially compensated metabolic acidosis
E. Uncompensated metabolic acidosis
D. Partially compensated metabolic acidosis (the pH being in the "close" range makes it partially compensated.
-Interpretation:
Low pH suggests acidosis.
Low HCO3- and negative BE point to metabolic acidosis.
Low pCO2 indicates the respiratory system's attempt to compensate by blowing off CO2 (which lowers acid levels).
Since metabolic acidosis is present and the respiratory system is compensating by lowering pCO2, the condition is partially compensated metabolic acidosis.
A 56-year-old man was admitted to the hospital because of jaundice and abdominal pain increasing for 3 weeks. There was no past medical history. Laboratory tests results obtained on admission were as following: WBC 8,9x109/L; RBC 4,2x1012/L; HGB 12,3g/dL; HCT 38 %; MCV 85 fL; MCH 28 pg; RDW 13.5%; PLT 476x109/L; RET 28x109/L. CRP 11 mg/L, ALT 80 IU/L, AST 65IU/L, GGT 758 IU/L, ALP 725 IU/L, Bilirubin 6,6mg/dL, PT 14 s, Albumin 35 g/L. Urine: bilirubin positive, urobilinogen normal.
What is the most probable diagnosis?
A. Chronic hepatocellular damage
B. Acute hepatocellular damage
C. Bile ducts obstruction
D. Gilbert's syndrome
E. Autoimmune hepatitis
C. Bile ducts obstruction
Reasoning:
Jaundice and abdominal pain over a 3-week period suggest a liver or biliary tract issue.
Markedly elevated levels of GGT (758 IU/L) and ALP (725 IU/L) are strongly indicative of cholestasis(obstruction of bile flow), which points toward a bile duct obstruction.
The elevation of bilirubin (6.6 mg/dL) and the presence of bilirubin in the urine further support obstructive jaundice.
ALT (80 IU/L) and AST (65 IU/L) are elevated but not to the extent seen in acute hepatocellular injury, which makes a hepatocellular process less likely.
The patient has a high platelet count (476x10^9/L), which can occur in conditions like cholestasis.
A 68-year-old man with no bad habits diagnosed with the new onset of type 2 diabetes mellitus. There was no past medical history. What is the patient's
recommended LDL concentration?
A. <130 mg/dl (3,36 mmo1/l)
B. <115 mg/dl (2,97 mmo1/l)
C. <100 mg/dl (2,59 mmol/I)
D. <70 mg/dl (1,81 mmol/I) LDL should always be as low as possible
E. <160 mg/dl (4,14 mmol/I)
C. <100 mg/dl (2,59 mmol/I) (Only needs to be <70 if there is concomitant CHD)
55. Which tests doesn't confirm elevated cortisol concentration?
A. 24-hour urinary free cortisol level
B. Low-dose dexamethasone suppression test (LDDST)
C. High-dose dexamethasone suppression test (HDDST)
choice
D. Late-night salivary cortisol measurements
E. Plasma cortisol measurements
C. High-dose dexamethasone suppression test (HDDST) (If the question is asking
which test doesn't measure elevated cortisol concentration then this might be the right
choice [used to assess ACTH response])
65. What is the best test to diagnose Cushing's Disease?
a. Serum cortisol
b. 24-hour urine cortisol
c. Serum ACTH
d. High doses dexamethasone suppression
e. Cortisol response to glucose
d. High doses dexamethasone suppression (8mg)
A 5-year-old boy was admitted to the hospital because of acute pain and edema of the left knee. His parents reported similar episodes since he started crawling/walking. His laboratory test results were as following: PLT 379 x109/L(normal), ST 7 min (N: 2-8 min.), APTT 59 s(elevated), PT 12 s (normal). What test would you order next to establish the most probable cause of bleeding disorders in that case?
A. The activity of factor VIII
B. Fibrinogen concentration
C. The activity of von Willebrand factor
D. The activity of factor XI
E. The activity of factor VII
A. The activity of factor VIII
The most likely diagnosis for this 5-year-old boy is hemophilia A, which is a clotting factor deficiency (specifically factor VIII). This condition would explain the recurrent episodes of joint pain and swelling, as well as the elevated APTT (activated partial thromboplastin time), which suggests a deficiency in one of the intrinsic pathway clotting factors.
What is the influence of a low-caloric and high-carbohydrate diet on lipid profile?
A. Increases TG
B. Decreases HDL and increases LDL
C. Increases LDL
D. Increases T-Cholesterol
E. Increases T-Cholesterol, LDL, and HDL
A. Increases TG
A 52-year-old male alcoholic presented with severe weakness. The neurologic examination and mental status were normal. A CBC exhibited HGB 7,0 g/dL(low). MCV 82 fL, WBC 22.5x109/L and PLT 775x109/L(high) What is the most probable cause of anemia in that case?
A. Autoimmune hemolytic anemia
B. Acute blood loss
C. Congenital spherocytosis
D. Folate deficiency
E. B12 deficiency
B. Acute blood loss
Reasoning:
The patient is an alcoholic, and chronic alcoholism can lead to gastritis or peptic ulcers, both of which can result in acute or chronic gastrointestinal bleeding. This bleeding could lead to acute blood loss anemia.
The WBC count of 22.5 x 10^9/L and thrombocytosis (PLT 775 x 10^9/L) could indicate inflammatory or reactive changes due to the blood loss.
The MCV of 82 fL is normocytic, which is typical of acute blood loss anemia, as the body attempts to compensate with normal-sized red blood cells during initial blood loss.
The hemoglobin level (HGB 7.0 g/dL) is low, which aligns with acute blood loss anemia.
Which of the following does not cause an increase of BNP/NT-proBNP
concentration?
A. Pulmonary embolism
B. Atrial fibrillation
C. Chronic pancreatitis
D. Thyroid disorders
E. Mitral regurgitation
C. Chronic pancreatitis
What is the general goal of well-control diabetes mellitus in adults?
A. HbA1c <=7,0%
B. Fasting glucose <70 mg/dl
C. HbA1c >=7,0%
D. Fasting glucose < 140 mg/dl
E. Random blood glucose > 70 mg/dl
A. HbA1c <=7,0%(less than 7 is the rule)
What does the Bence-Jones protein test indicate?
A. Proliferation of leukemia cells
B. Urine output of light chains of immunoglobulin
C. Involvement of lymph nodes
D. Increased plasmocytes number in blood smear
E. Presence of immunoglobulin in plasma
B. Urine output of light chains of immunoglobulin
What does 90% NPP (negative predictive value) of normal NT-proBNP
concentration obtained in patients suspected of heart failure (HF) mean?
A. The probability of having HF equals to 90%
B. 90% of normal NT-proBNP results require confirmation in another blood sample
C. 10% of normal NT-proBNP results are false negative
D. HF is ruled out with 90% probability
E. 90% of normal NT-proBNP results are false negative
D. HF is ruled out with 90% probability (NPV means that the number in percentage form
indicates that a negative result means that number of subejcts don't have the disease)
A 54-year-old man admitted to the hospital because of leg edema, ascites, and
abdominal discomfort. There was no past medical history. He used to abuse alcohol.
His laboratory test results are as following:
ALT 57 IU/L; AST 73 IU/L; GGT 139 IU/L; Bilirubin '1.6 mg/dL; PT 14 s.; Total Protein:
6,7 g/dL, Albumin 2,0 g/dL; Serum protein electrophoresis: albumin 43 %, gamma-
globulins 36 %.
What is the most probable diagnosis?
A. Alcoholic hepatitis
B. Extrahepatic bile ducts obstruction
C. Autoimmune hepatitis
D. Gilbert's syndrome
E. Liver cirrhosis
E. Liver cirrhosis (key indicator is the slightly elevated levels of BOTH ALT and AST)
While the patient has a history of alcohol abuse and mild elevation in liver enzymes, the combination of symptoms (ascites, edema, low albumin) is more typical of cirrhosis, which is a more advanced stage of liver damage.
A 27-year-old woman with no past medical history was brought to the hospital
because of drowsiness and lethargy. BP on admission was 90/50 mmHg. The physical
examination revealed no other abnormalities. Baseline tests performed in the
Emergency Department revealed the following results:
Plasma Na+120 mmol/L(low); K+ 6.2 mmol/L(high); Glucose 55 mg/dL; 1T4 12,85
pmol/L; TSH 2.3 mU/L What is the most probable diagnosis?
A. Hashimoto's disease and Addison's disease (APS-2)
B. Cushing's syndrome and hyperthyroidism
C. Insulinoma and Cushing's syndrome
D. Cushing's syndrome and hypothyroidism
E. Addison's disease
E. Addison's disease
Which of the following is not the characteristic of an ideal biomarker?
A. Standardized
B. Cost-effective
C. Accurate
D. Reproducible
E. Low negative predictive value
E. Low negative predictive value
What is the acid-base disorder in the patient with the following result of arterial blood
gasometry?
pH 7,56; pCO2 39,0 mmHg; p02 97,8 mmHg, s02 96,4%, HCO3- 41,0 mmol/L; BE 14,6
mmol/L?
A. Uncompensated respiratory alkalosis
B. Uncompensated metabolic alkalosis
C. Metabolic alkalosis with respiratory acidosis
D. Partially compensated respiratory alkalosis
E. Partially compensated metabolic alkalosis
B. Uncompensated metabolic alkalosis
A 39-year-old woman was ordered a routine medical examination. She was
asymptomatic, otherwise healthy. She was not taking medications. Her laboratory testresults were as follows: ALT 250 IU/L; AST 218 IU/L; GGT 300 IU/L; Bilirubin 1,3 mg/dL(high); PT 13 s.; Serum protein electrophoresis: normal result. What is the most probable cause of laboratory tests abnormalities found in that patient?
A. Extrahepatic bile ducts obstruction
B. Gilbert's syndrome
C. Liver cirrhosis
D. Chronic viral hepatitis
E. Acute viral hepatitis
D. acute viral hepatitis
.
Chronic vs. Acute Viral Hepatitis: Key Differences
Feature | Acute Viral Hepatitis | Chronic Viral Hepatitis |
|---|---|---|
Definition | Liver inflammation lasting <6 months | Liver inflammation lasting >6 months |
Causes | HAV, HBV, HCV, HEV (most common) | HBV, HCV, HDV (HAV & HEV do NOT cause chronic infection) |
Symptoms | Flu-like symptoms, jaundice, abdominal pain, nausea, dark urine | Often asymptomatic; fatigue, mild RUQ discomfort |
ALT/AST Levels | Markedly elevated (>200-1000 IU/L) | Mildly elevated (<100-200 IU/L) |
Bilirubin | Increased, especially in icteric phase | Mild or normal |
Prothrombin Time (PT/INR) | Usually normal unless severe | May be prolonged in advanced disease |
Serum Protein Electrophoresis | Usually normal | May show polyclonal hypergammaglobulinemia(chronic inflammation) |
Liver Biopsy Findings | Ballooning degeneration, lobular inflammation | Fibrosis, ground-glass hepatocytes (HBV), portal inflammation |
Risk of Progression to Cirrhosis | Low, usually resolves | High (especially in HCV, HBV + HDV coinfection) |
Treatment | Supportive care (hydration, rest) | Antiviral therapy for HBV, HCV |
,
Option | Why Incorrect? |
|---|
A. Extrahepatic bile ducts obstruction | Would cause markedly high bilirubin & ALP, with less ALT/AST elevation. No mention of jaundice or pain. |
B. Gilbert's syndrome | Causes isolated bilirubin elevation, without ALT, AST, or GGT abnormalities. |
C. Liver cirrhosis | Would show low albumin, abnormal protein electrophoresis, prolonged PT, and lower AST/ALT ratio (~<100 IU/L). |
A 53-year-old woman with active rheumatoid arthritis treated long time with NSAID and steroids was ordered some laboratory tests with the following results: WBC 7,9x109/L; RBC 4,0 x1012/L; HGB 7,8 g/dL; HCT 25,9 %; MCV 71,5 fL; MCH 15,5 pg; RDW 14%; PLT 376x109/L; RET 19,0x109/L. Ferritin 680 ng/mL; TIBC 55 pg/dL; Iron 5 pg/dL. What test would you order to prove the presence of a pure iron deficiency in this case?
A. Bone marrow flow cytometry
B. Transferrin
C. sTfR
D. Haptoglobin
E. Transferrin saturation
C. sTfR
30-year-old female patient complained about general discomfort, muscle pain, arthralgia, nausea, loss of appetite, increased body temperature for last week, and delicately yellow sclera. There is no past medical history. Nine weeks ago, she visited her dentist. Laboratory test results are as
following: ALT 1380 IU/L, AST 1092 IU/L, ALP 162 IU/1_, GGT 290 IU/L, Bilirubin 3 mg/dL. Urine findings: Bilirubin positive, Urobilinogen increased.
What tests would you order next to continue the diagnostic procedure?
A. HBsAg, IgM anti-HBc, and anti-HCV
B. Serum protein electrophoresis and liver biopsy
must to know other methods of egzaminition. Yes you must to.
C. Serum protein electrophoresis and ANA
D. Anti-HCV and anti-HDV
E. Concentration of conjugated bilirubin
A. HBsAg, IgM anti-HBc, and anti-HCV
A 59-year-old woman was admitted to the hospital because of resting dyspnea and marked worsening of general condition exacerbating rapidly for the past three hours. For the last few months, she was being given chemotherapy because of colorectal cancer. Laboratory test results obtained at admission were as following:WBC 5,3x109/L, HGB 10,6g/dL, RBC 3,54x1012/L, HTC 34,3 %, MCV 96,9 fL, MCH 29,9 pg.; PLT 176x109/L; RDW 20,8%, CRP 20 mg/L, bilirubin 1,0 mg/dL, D-dimer >10000 ng/mL (N<500ng/mL).
What is the most probable diagnosis?
A. Acute blood loss
B. Acute pulmonary embolism
C.Acute pneumonia
D. Acute hemolysis
E. Acute disseminated intravascular coagulation (DIC)
B. Acute pulmonary embolism
The D-dimer level is very elevated (>10,000 ng/mL), which is a strong indicator of thrombotic events, including pulmonary embolism.
Which of the following does not cause the increase of cardiac troponin (I or T) concentration?
A. lschemic stroke
B. Common cold
C. Chronic kidney insufficiency
D. Cardiac arrhythmia
E. Chronic heart failure
B. Common cold
A 54-year-old man had a 2-day episode of increasing shortness of breath and
sputum production. The chest radiograph revealed left lower lobe pneumonia. The following arterial blood gasometry was obtained at admission with the patient breathing room air: pH 7,25(low); pCO2 70,0 (High)mmHg; p02 65,0 mmHg, s02 8E0%, HCO3 24,0 mmol/L(normal); BE 1,2 mmol/L. What is the acid-base disorder present in that patient?
A. Metabolic alkalosis
B. Respiratory acidosis and metabolic alkalosis
C. Chronic respiratory acidosis
D. Acute respiratory acidosis
E. Metabolic acidosis
D. Acute respiratory acidosis
Which of the following is not the source of AST?
A. Erythrocytes
B. Heart
C. Kidney
D. Liver
E. Pancreatic gland
E. Pancreatic gland
What is the best tumor marker for the monitoring of patients with breast cancer (1)
and patients with gastric cancer (2)?
A. (1) CA 15.3 and (2) CEA with CA19.9
B. (1) CA 125 and (2) CEA
C. (1 ) CEA and (2) CA 125
D. (1) CA 15.3 and (2) AFP with CA 19.9
E. (1) CA 125 and (2) AFP with CA 19.9
A. (1) CA 15.3 and (2) CEA with CA19.9
What is the most sensitive marker of intravascular hemolysis?
A. Haptoglobin
B. C-reactive protein
C. Transferrin
D. Ceruloplasmin
E. Albumin
A. Haptoglobin
Which of the following reflects adequate control of glycemia during 2-3 weeks before
testing?
A. Normal fasting glucose
B. Decreased value of HbA1c
C. Normal postprandial glucose
D. Normal urinalysis
E. The normal concentration of plasma fructosamine
E. The normal concentration of plasma fructosamine
An 18-year-old woman complaining of frequent nose bleeding, easy bruising, and excessive menstruations for the last three years. Her laboratory tests results were as following: PLT 200 x109/L, BT 12 min (N: 2-8 min.), APTT 45 s, PT 11 s. What test would you order next to establish the most probable cause of bleeding disorders in that case?
A. The activity of factor VIII
B. Concentration of fibrinogen
C. The activity of von Willebrand factor
D. The activity of factor IXE. The activity of factor VII
C. The activity of von Willebrand factor
What may a urine sample in so-far undiagnosed diabetic consists of?
A. Ketones and adrenaline
B. Ketones and adrenaline
C. Glucose
D. Glucosose and bilirubin
E. Glucose and adrenaline
C. Glucose
What is the typical kinetics (beginning of increase - maximal concentration -
normalization) of cardiac troponin I concentration in the course of myocardial infarction?
A. 3-4 hours; 24 hours; 1-5 days
B. 1-2 hours; 48 hours; 5-14 days
C. 2-3 hours; 36 hours; 5-10 days
D. 3-4 hours; 24 hours; 5-10 days
E. 3-5 hours; 24-36 hours; 1-2 days
D. 3-4 hours; 24 hours; 5-10 days
Which of the following conditions is not characterized by a macrocytic peripheral
blood smear picture?
A. Folic acid deficiency
B. Myelodysplastic syndrome (MDS)
C. Hemolytic anemia
D. Vitamin B12 deficiency
E. Anemia of chronic diseases (ACD)
E. Anemia of chronic diseases (ACD)
A 32-year-old woman with no past medical history admitted to the hospital because of drowsiness and lethargy. On admission, her BP was 90/50 mmHg. Baseline tests performed in the Emergency Department revealed the following: Plasma Na+ 120 mmol/L(low): K+ 6.2 mmol/L(high): Glucose 55 mg/dL: fT4 1,28 ng/dL: TSH 2,3 mU/L. What is the most probable diagnosis?
A. Cushing's disease
B. Addison's disease
C. Insulinoma
D. Hashimoto's disease
E. Cushing's syndrome
B. Addison's disease
Why Addison’s Disease?
Primary adrenal insufficiency (Addison’s) = Low cortisol and aldosterone.
Aldosterone deficiency → Hyponatremia & hyperkalemia (due to Na+ loss & K+ retention).
Cortisol deficiency → Hypoglycemia & hypotension (due to reduced gluconeogenesis & vascular tone).
Symptoms include fatigue, weight loss, skin hyperpigmentation (if chronic), dizziness, and craving for salty foods.
An 89-year-old man is complaining about numbness of fingers, weakness and
recently increasing memory loss. His CBC reveals WBC 2,0x109/L, RBC 1,3x1012/L, HGB 5,0 g/dl, HCT 15%, MCV 118 fL, MCH 36,5 pg, MCHC 35,7 g/dl, PLT 60x109/L. What is the most likely diagnosis?
A. Hemolytic anemia
B. Macrocytic anemia due to reticulocytosis
C. Aplastic anemia
D. Anemia of chronic disease
E. Megaloblastic anemia due to B12 deficiency
E. Megaloblastic anemia due to B12 deficiency
(the MCV being 118 and the CNS
symptoms give us the answer)
A 25-year-old man has mild pharyngitis followed by a high fever over the past 24 hours. His skin shows extensive areas of hyperplgmentation. Vital signs Include a body temperature of 39,0oC, HR 102 BPM, respiration rate 21 BPM, and BP 80/55 mmHg. Laboratory studies show a plasma Na+ 113,0 mmol/L, K+ 6,3 mmol/L, CI- 92,0 mmol/L, glucose 42 mg/dL, and plasma creatinine 1,1 mg/dL. Which of the following laboratory findings is most likely to be present in this man?
A. Elevated cortisol
B. Increased ACTH and Increased cortisol
C. Increased ACTH and decreased cortisol
D. Decreased TSH and decreased fT4
E. Decreased TSH and increased fT4
C. Increased ACTH and decreased cortisol
Which of the following is a currently recommended biochemical marker of
myocardial necrosis?
A. CKMB mass
B. Troponin I or T
C. Myoglobin
D. Pregnancy-associated plasma protein type A (PAPP-A)
E. hFABP
B. Troponin I or T
C. BNP or NT-proBNP (heart failure)
D. h-FABP (biomarker of MI)
E. D-dimer (biomarker of thrombosis, pulm embolism)
F. CK-MB mass (cardiac marker of acute MI, sometimes use troponin test instead)
G. hs-cTnT (high-sensitivity assay for cardiac troponin T)
• Heart morbidity & mortality factor: BNP, NTBNP
• Cardiac markers:
• First to last to show up:
• H-FABP (heart fatty acid binding protein)
• Detectable in blood w/in 1-3 hrs of pain
• Myoglobin• Detectable in blood w/in 2 hrs of pain
• CK-MB
• Detectable in blood w/in 10-24 hrs of pain
• Troponin
• Detectable in blood w/in 12-48 hrs of pain
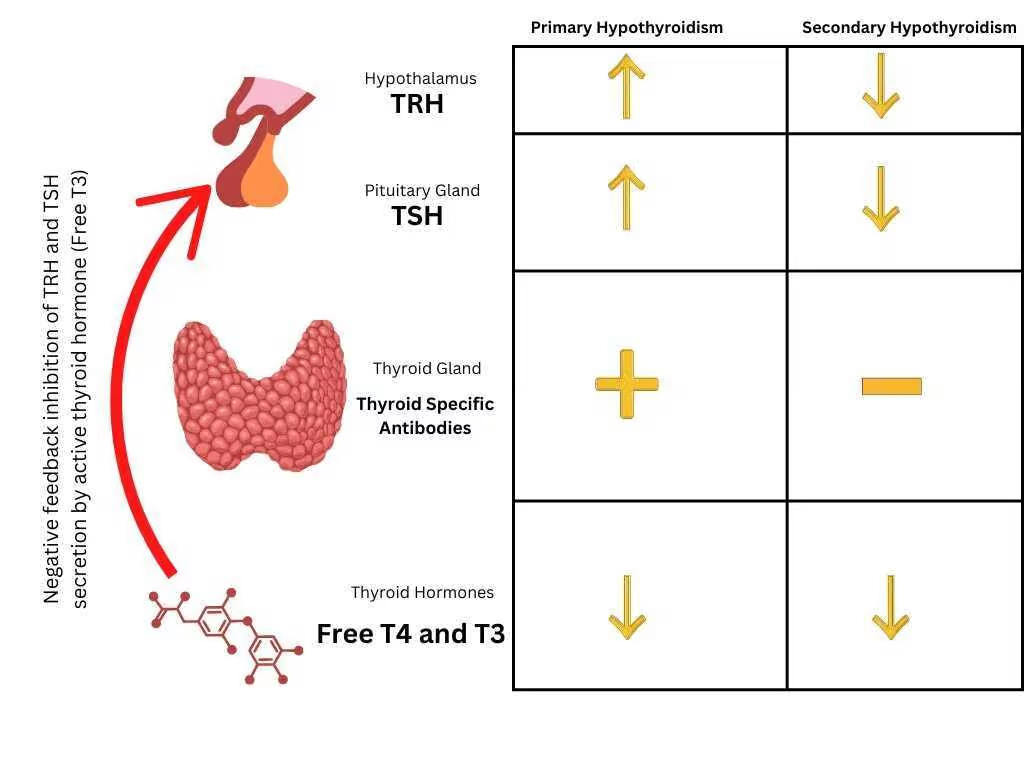
A 60-year-old overweight female, psychiatry outpatient, complained of constipations, progressive weakness and decreased effort tolerance. Laboratory test results were as following: Plasma Na+ 137 mmol/L. K+ 4.69 mmol/L, ALT 20 IU/L, AST 27 IU/L. GGT 12 lU/L. Bilirubin 0,34 mg/dL; T-Cholesterol 332 mg/dL, TG 160 mg/dL. HDL 74 mg/dL, LDL 226 mg/dL. TSH 0,15 mU/L, fT3 1.31 pg/mL, fT4 0.48 ng/dL.
What is the most probable diagnosis concerning the patient's metabolic abnormalities?
A. Secondary hypothyroidism with secondary hypercholesterolemia
B. Chronic liver disease with primary hypertriglyceridemia
C. Chronic liver disease with secondary hypertriglyceridemia
D. Primary hypothyroidism with secondary hypercholesterolemia
E. Secondary hyperthyroidism with primary hypercholesterolemia
A. Secondary hypothyroidism with secondary hypercholesterolemia
A 22-year-old man was complaining of arthralgia, bone and muscle pain, general discomfort, increased body temperature, nausea, and loss of appetite for several days. One week ago he visited his family doctor because of tiredness. Past medical history included a short experience of i.v. drugs intaken several weeks ago. Physical examination revealed an enlarged liver with a tender edge. Laboratory test results were as follows: ALT 1135 IU/L, AST 1045 IU/L, GGT 258 IU/L, ALP 185 IU/L, Bilirubin 1,7 mg/dL, PT 13 sec, Albumin 45 g/l. What is the most probable diagnosis?
A. Drug-induced liver injury
B. Gilbert's syndrome
C. Chronic viral hepatitis
D. Autoimmune hepatitis
E. Acute Viral hepatitis
E. Acute Viral hepatitis
What are the changes in kidney function parameters which might result just from aging?
A. Increased GFR and decreased plasma creatinine
B. Decreased GFR and elevated plasma creatinine
C. Decreased GFR and normal plasma creatinine
D. Aging doesn't affect kidney function
E. Decreased GFR and decreased plasma creatinine
Decreased GFR and normal plasma creatinine
What does 95% diagnostic specificity of the diagnostic test mean?
A. 95 over 100 sick patients will not be diagnosed with the disease
B. 5 over 100 healthy patients will be diagnosed with the disease
C. 95% of examined patient will require the additional tests to diagnose the disease
D. The probability of false-positive result equals to 95%
E. 95% of examined patients are ill
5 over 100 healthy patients will be diagnosed with the disease
A 25-year-old male patient arrives at the Emergency Department with blood glucose 450 mg/dL, plasma osmolarity of 290 mOsmol/kgH20, pH 7,22; pCO2 25 mmHg, HCO3- 16 mmol/L. He complains of thirst, polyuria. The patient is breathing rapidly and has a fruity breath smell. What is the most probable diagnosis?
A. Hypoglycemia
B. Lactic acidosis
C. Diabetic ketoacidosis
D. Kidney acidosis
E. Hyperglycemic hyperosmolar state
C. Diabetic ketoacidosis
A 23-year-old woman complains of difficulty with concentrating on her job at work lasting for the past month. She is continually getting up and walking around to visit co- workers. She complains that the work area is too hot. She seems nervous and spills her coffee a lot. She eats more than usual but lost 7 kg during the past month. On physical examination, her temperature is 37.5°C, pulse 101 BM, respiratory rate 18 breaths per minute, and blood pressure 145/85 mm Hg. Which of the following laboratory findings Is most likely to be present in this women?
A. Decreased iodine uptake
B. Decreased plasma Insulin
C. Decreased ACTH
D. Decreased TSH
E. Increased ACTH
D. Decreased TSH
Which of the following sets of laboratory tests is the most useful in the differential diagnosis of coma present in a 58-year-old female suffering from type 2 diabetes mellitus for 20 years?
A. Plasma glucose and arterial blood gas analysis
B. Plasma glucose and urine glucose
C. Urine glucose and urine albumin
D. HbA1c level and plasma glucose
E. Arterial blood gas analysis and HbAl c level
B. Plasma glucose and urine glucose
Julia
I think its A
Which one of the following sets of results is the most consistent with the liver
cirrhosis?
A. AST 800 IU/L, ALT 1100 IU/L; PTL 220x10^9/L; PT 14 sec
B. AST 85 IU/L, ALT 145 IU/L; PTL 160x10^9/L; PT 13sec
C. AST 4000 IU/L, ALT 3680 IU/L; PTL 400x10^9/L; PT 17 sec
D. AST 28 IU/L, ALT 35 IU/L; PTL 280x10^9/L; PT 11 sec
E. AST 410 IU/L, ALT 179 IU/L, PTL 95x10^9/L; PT 18 sec
E. AST 410 IU/L, ALT 179 IU/L, PTL 95x10^9/L; PT 18 sec
look into this
Which of the following reflects adequate control of glycemia during 2-3 hours before testing?
A. Decreased value of HbA1c
B. Normal urinalysis
C. Normal postprandial glucose
D. The normal value of plasma fructosamine
E. Normal fasting glucose
B. Normal urinalysis
might be Cc
What is the daily urine albumin excretion characterizing albuminuria?
A. 300 -500 mg/24 hrs
B. < = 30 mg/24 hrs
C. 30-300 mg/24 hrs
D. < 20 mg/24 hrs
E. > 500 mg/24 hrs
C. 30-300 mg/24 hrs
microalbuminuria - urinary albumin excretion rate from or 30-300 mg/24h (urine albumin
concentration ranges from 20 to 200 mg/l) - predicts the later development of clinical diabetic
nephropathy
A 68-year-old woman was taking 75mg of ASA (acetylsalicylic acid) for the last four years as secondary prevention of a cardiovascular event. Recently she was additionally prescribed LMWH (enoxaparin) because of a leg fracture. What kind of abnormalities in basic laboratory tests is the most probable in that patient?
A. APTT: unaffected; INR: unaffected; BT: unaffected; PLT: decreased
B. APTT: prolonged; INR: unaffected; BT: unaffected; PLT: unaffected
C. APTT: unaffected; INR: unaffected; BT: prolonged; PLT: unaffected
D. APTT: unaffected; INR: prolonged; BT: unaffected; PLT: unaffected
E. APTT: unaffected; INR: unaffected; BT: prolonged; PLT: decreased
C. APTT: unaffected; INR: unaffected; BT: prolonged; PLT: unaffected
Effects of ASA (Aspirin):
Irreversibly inhibits COX-1 and COX-2, leading to decreased thromboxane A2 (TXA2) production.
This impairs platelet aggregation and prolongs bleeding time (BT).
A 23-year-old female was complaining of frequent urination with burning. She was instructed to collect a clean catch, midstream sample of the urine which was tested with the following results: blood (1+), protein (1+), nitrite (positive), leukocyte esterase (3+), 40-60 WBC/HPF, 18-20 RBC/HPF, many bacteria, many squamous epithelial cells. Based on her symptoms and urinalysis result, what might be the most probable diagnosis?
A. These are typical findings of poorly collected urine specimen In menstruating women
B. Atypical urinary tract infection
C. Typical urinary tract infection
D. Nephritic syndrome
E. Glomerulonephritis
C. Typical urinary tract infection
Blood (1+): Presence of blood in the urine is common in UTIs.
Protein (1+): Mild proteinuria can occur in UTIs.
Nitrite (positive): Nitrites are typically produced by Gram-negative bacteria (like E. coli), which are common culprits in UTIs.
Leukocyte esterase (3+): This is an enzyme found in white blood cells, and its presence indicates significant leukocyte activity, suggesting infection.
What is the laboratory test recommended for the monitoring of unfractionated heparin treatment?
A. INR
B. PLT and INR
C. PT and PLT
D. Unfractionated heparin treatment doesn't require laboratory monitoring
E. APTT
E. APTT
Which of the following statements concerning highly sensitive (hs) troponin assays
is false?
A. Have higher negative predictive value for acute myocardial infarction (MI) than standard assays
B. It is common to detect circulation levels of cardiac troponin in healthy individuals
C. Are associated with a 2-fold increase in the detection of type 2 MI
D. Have lower analytical sensitivity than standard assays
Elevations beyond 5-fold the upper reference limit have high (>90%) positive
predictive value for acute type 1 MI
D. Have lower analytical sensitivity than standard assays — False. The primary advantage of hs-troponin assays is their higher analytical sensitivity compared to standard assays, allowing them to detect lower levels of troponin and improve diagnostic accuracy.
A 48-year-old female presented to the general practitioner because of decreased effort tolerance and loss of 5 kilos of her body weight over the last two months. Her BMI was 22,7 kg/m2, BP 140/90 mmHg. and HR 90/min. Fasting lab test results were as following: Glucose 115 mg/dL, Na+ 140 mmol/L, K+ 4,5 mmoI/L, T-Cholesterol 120 mg/dL, HDL 42 mg/dL, TG 110 mg/dL, LDL 56 mg/dL, TSH 0,01 mU/L. What is the most likely diagnosis?
A. Addison's disease
B. Hypothyroidism
C. Cushing's syndrome
D. Hyperthyroidism
E. Type 1 diabetes mellitus
D. Hyperthyroidism