Mayo - HFpEF and LA strain
1/7
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
8 Terms
In patient with normal LVEF, what criteria do you evaluate for diastolic dysfunction?
Average E/e’ > 14
Septal e’ velocity < 7 or lateral e’ velocity < 10 cm/s
TR velocity > 2.8 m/s
LA volume index > 34 mL/m2

If you have a reasonable pre-test probability of HFpEF (dyspneic patient in sinus rhythm) and E/e’ ratio < 15, what do you do next?
Exercise them and see what happens to E/e’ ratio.
FYI Exercising them could also reveal it was coronary ischemia instead all along.
E/e’ correlates with PCWP but…
DOES NOT EQUAL IT
FYI E/e’ > 15 likely has an elevated PCWP; E/e’ < 8 likely to have normal PCWP
When ultra sounding lung, you’re essentially looking at artifacts.
If only horizontal artifact, then you have normal dry lungs (A-line pattern)
If you have an interstitial process/wet lungs, you will see…
Vertical B-line pattern
FYI the more B lines, the worse the lung congestion
FYI so when diagnosing HFpEF and you do stress echo, can also do focused lung ultrasound before and after and if you notice edema + E/e’ suggestive of diastolic dysfunction think HFpEF

Trial studying role of Spiro with patients with HFpEF
TOPCAT
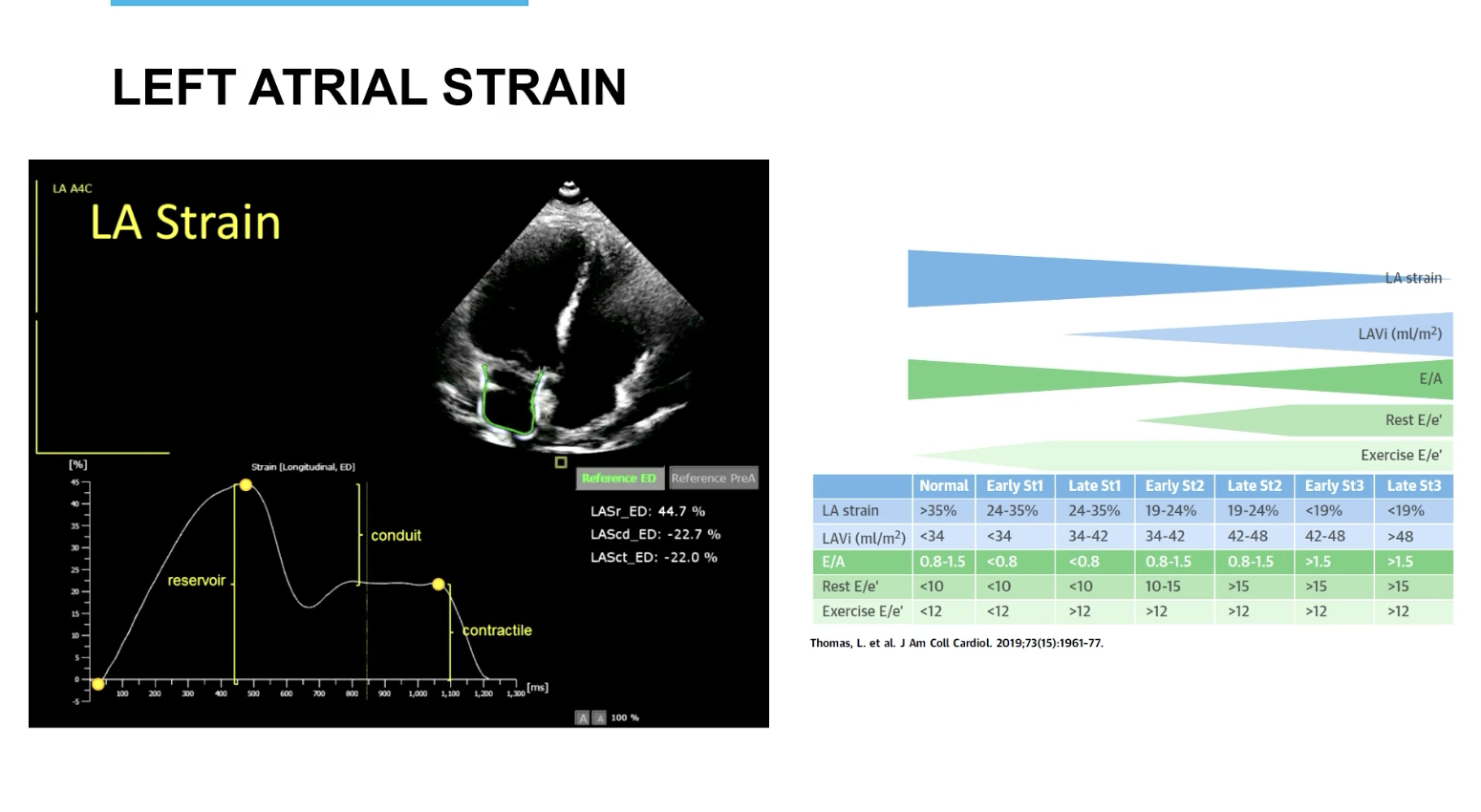
Left atrial strain, typically the LA does not..
improve.
FYI usually superior from LA volume
FYI you don’t need the chart in the image, just FYI. Also just know the LA reservoir will change with HFpEF
FYI patients with HFpEF have normal LVEF but not necessarily totally normal…
GLS. They usually have some degree of systolic dysfunction seen on strain imaging.