Looks like no one added any tags here yet for you.
What is the normal Serum Osmolality in the body?
275-290 mOsm/kg
Def of hypovolemia
loss of Na and water exceeding intake
Signs/Symptoms of Hypovolemia
lower plasma vol
hypotension, tachycardia
thirsty, fatigue, weak, cramps, dizzy
diminished skin turgor
altered mental status
Causes of hypovolemia (low volume):
Think: anything that would cause us to lose fluid
Outside the renal system:
GI Issues
vomiting, diarrhea, ng suctioning
Skin/respiratory
sweat, burns
Hemorrhage (blood loss)
Renal System:
diuretics
hypoaldosteronism
osmotic diuresis, salt wasting nephropathies
Would you expect a person with hypovolemia to have high or low BUN/SCr ratio?
HIGH (normal is 10:1, in hypovol it’s 20:1 or higher)
How is mild and severe hypovolemia treated?
mild- fluids like gatorade/pedialyte
severe- IV NS!!!!!!!!!!!!!!!!!!!!!!!!!!!
How does edema develop?
can’t excrete sodium
decrease in BV even though normal ECF
Increased cap/venous pressure
altering starling forces
What medication can be used to treat edema?
diuretics
What is the treatment for life-threatening pulmonary edema?
IV Diuretics
In order to treat edema, we also need to treat the _____________ _______________ and restrict ________ in the diet.
In order to treat edema, we also need to treat the underlying cause and restrict Na in the diet.
Generic names of the 4 loop diuretics:
Furosemide
Bumetanide
Torsemide
Ethacrynic Acid
What is the most potent diuretic?
Loop
MOA of Loop diuretics:
inhibit NKCC transporter in loop of henle
Contraindications of loop diuretics:
sulfonamide allergy (except ethacrynic)
anuria (can’t pee)
liver coma
low electrolytes
ADRs of Loop Diuretics:
low Na, K, Cl, Ca
Hyperuricemia, Hyperglycemia
Ototoxicity
How do we overcome diuretic resistance?
combine diuretics (loop+thiazide)
increase dose
Name 3 thiazide and 3 thiazide-like diuretics:
Thiazide:
Chlorothiazide
Hydrochlorothiazide
Methyclothiazide
Thiazide-Like:
Chlorthalidone
Indapamide
Metolazone
MOA of Thiazide Diuretics:
inhibit Na/Cl symporter in distal tubule
Contraindications of Thiazide Diuretics:
sulfonamide allergy
anuria
pregnant
ADRs of Thiazide Diuretics:
low Na, K, Cl
increased Ca
(different than loop)
Hyperuricemia, hyperglycemia
Hyponatremia Risk Factors:
age
nursing home pts
exercise induced
marathon runners
Below _____ mEq/L is considered hyponatremia.
135
Acute Symptomatic Hyponatremia results from an _____________ in neuron volume and cerebral ___________.
results from an increase in neuron volume and cerebral edema.
Symptoms of mild, moderate, and severe acute symptomatic hyponatremia:
(idk how important this is to know)
mild- HA, nausea
moderate- HA, lethargy, disoriented
severe- coma, seizure, respiratory arrest
treatment of acute symptomatic hyponatremia:
NS or 3% saline (be careful)
Improper therapy/ Rapid correction of the hypotonic state of the brain can cause:
osmotic demyelination
Can I use NS to correct low osmolarity/hypotonic state in the brain?
YES
Can I use 3% saline to correct low osmolarity/hypotonic state in the brain?
NO- OSMOTIC DEMYLENIATION
DO NOT raise serum Na more than ____ mEq/L wihtin 24 hours.
12
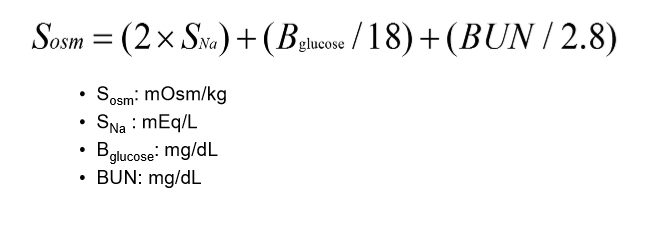
To determine whether or not you have isotonic, hypotonic, or hypertonic hyponatremia, you must calculate what?
DON’T HAVE TO MEMORIZE THE EQUATION JUST BE ABLE TO RECOGNIZE!!!!!!!!!!!!
serum osmolarity
Isotonic Hyponatremia is called _______________. It’s uncommon, but usually caused by what?
called pseudohyponatremia
caused by:
hyperlipidemia, hyperproteinemia
(treat what’s causing this)
Hypertonic Hyponatremia causes:
Think: something is causing water to be pulled out of the cells= causes low Na conc
Causes:
hyperglycemia
osmotic diuretics
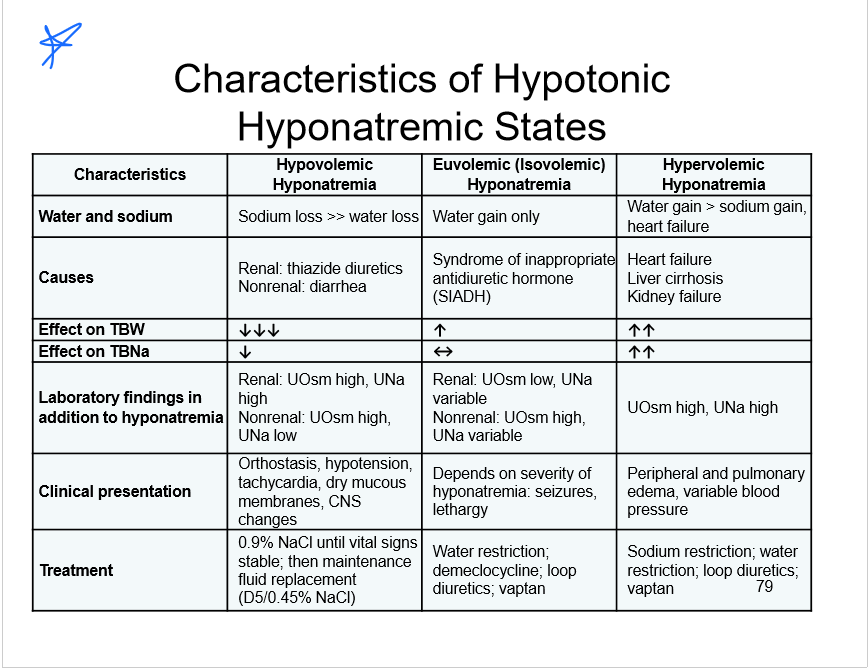
For hypotonic hyponatremia what is the 1st thing to determine?
fluid status (hypovolemic, hypervolemic, euvolemic)
Causes of hypovolemic hypotonic hyponatremia:
transient hypernatremia
marathon runners
think: we running lots and losing fluids, so we release lots of ADH, but then we done running and drink tons of water= causes hyponatremia
causes outside renal system:
diarrhea, sweating
renal system causes
diuretics
adrenal insufficiency
hypovolemic hypotonic hyponatremia treatments:
NS
when volume restored= switch to 0.45% NS
MOST COMMON CAUSE OF euvolemic hypotonic hyponatremia:
SIADH
Causes of SIADH:
tumors
CNS disorders
pulmonary disorders
drugs
Other causes of Euvolemic Hypotonic Hyponatremia:
renal/adrenal insufficiency
hypothyroidism
polydipsia
low sodium diet
What happens to water and Na in the following conditions:
euvolemic hypotonic hyponatremia
hypovolemic hypotonic hyponatremia
hypervolemic hypotonic hyponatremia
euvolemic hypotonic hyponatremia
normal Na
high water
hypovolemic hypotonic hyponatremia
low Na
low water
hypervolemic hypotonic hyponatremia
high Na
high water
SIADH treatment
restrict water
treat underlying cause
increase solute uptake
Meds: Demeclocycline, Vaptans
What % NaCl is usually used in patients with Euvolemic Hypotonic Hyponatremia?
3% NaCl
Demeclocycline inhibits the action of
ADH
Causes of Hypervolemic Hypotonic Hyponatremia:
CHF
cirrhosis
nephrotic syndrome
What should be restricted for a patient with Hypervolemic Hypotonic Hyponatremia?
salt and water
Treatment for Hypervolemic Hypotonic Hyponatremia caused by CHF:
digoxin
ACE Inhibitors
ARBs
Treatment of symptomatic patients for Hypervolemic Hypotonic Hyponatremia:
3% NaCl
fluid restriction
loop diuretics
What are the names of the 2 ADH antagonists approved for treatment of euvolemic or hypervolemic hyponatremia pts?
Conivaptan
Tolvaptan
Conivaptan:
MOA
ROA
MOA- antagonizes ADH receptors
ROA- IV
Conivaptan:
CIs
Cautions
ADRs
CI:
hypovolemic hyponatremia (pretty obvious)
hypersensitivity
using a CYP 34A inhibitors
Cautions:
anything that’s gonna deal w/ low volumes (hypotension, hypovolemia, etc.)
heart failure, renal/liver impairment
ADRs:
hypotension, fever, low K
Tolvaptan:
MOA
ROA
MOA- antagonizes ADH receptors
ROA- oral
Tolvaptan:
CIs
Cautions
ADRs
CI
NOT for pts. that need IMMEDIATE TREATMENT
hypovolemic hyponatremia
hypersensitivity
anuria
Cautions
don’t use w/ 3% NaCl
monitor Na, K, and vol status
use of CYP 3A inhibitors/inducers
cirrhosis patients
ADRs
common: thirsty, constipated, hyperglycemia, anorexia, polyuria
serious: DVT, V-fib, DIC, CVA, PE, rhabdomyolysis
FDA warning and boxed warning for Tolvaptan
FDA Warning:
can cause liver damage
not used longer than 30 days
Boxed:
only start/resume therapy in hospital where Na levels can be closely monitored
Drug Interactions of Tolvaptan:
CYP 3A inhibitors/inducers
P-gp inducers
digoxin
Great Summary Slide:
Rapid correction of a hypertonic state/high osmolarity of the brain can cause:
cerebral edema
Hypernatremia is caused by a ____________ in neuronal cell volume.
decrease
Treatment of hypovolemic hypernatremia:
0.9% NS
once volume restored—>0.45%NS, or D5W
Treatment of Hypervolemic/Euvolemic Hypernatremia:
hyperglycemia induced diuresis
postobstructive diuresis
hyperglycemia induced diuresis
insulin
0.9% NS
postobstructive diuresis
infuse hypotonic fluids
0.45% NaCl
What happens to ADH in a patient with Diabetes Insipidus?
low ADH output or
decreased response to ADH
Central Diabetes Insipidus treatment:
Desmopressin
PO or Nasal
NASAL recommended
Nephrogenic Diabetes Insipidus treatment:
stop drugs that contribute to the condition
correct high calcium and low potassium
restrict sodium
thiazide diuretic
indomethacin
Treatment of sodium overload:
loop diuretics
increase sodium excretion
IV D5W