Looks like no one added any tags here yet for you.
thyroid hormones
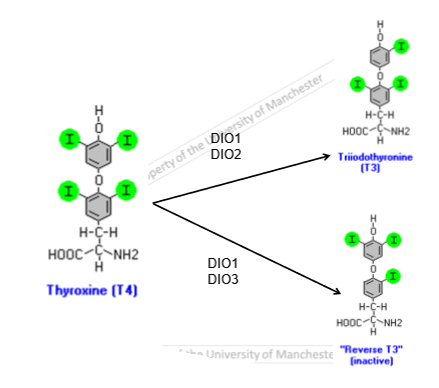
derived from tyrosine
reverse t3 is inactive form of thyroxine
less than 1% of rt3 is secreted
thyroxine(t4)
insoluble in serum
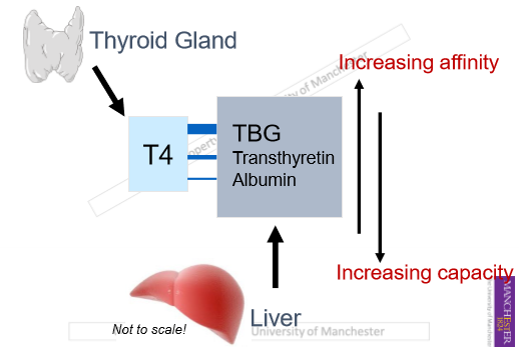
transported in serum with specific binding proteins
binding proteins synthesised in liver
liver disease can lead to loss of effective t4 transport to peripheral tissues
liver disease may be a reason for thyroid disease
thyroid hormone binding proteins
reservoir of thyroid hormones in blood
albumin is ubiquitous(very common)
albumin binds 5-10% of plasma t4
transthyretin(TTR) binds 20% of plasma t4, important for delivery to CNS
thyroxine-binding globulin(TBG) binds 70-75% of plasma t4, large circulating reservoir of t4, prevents loss in urine
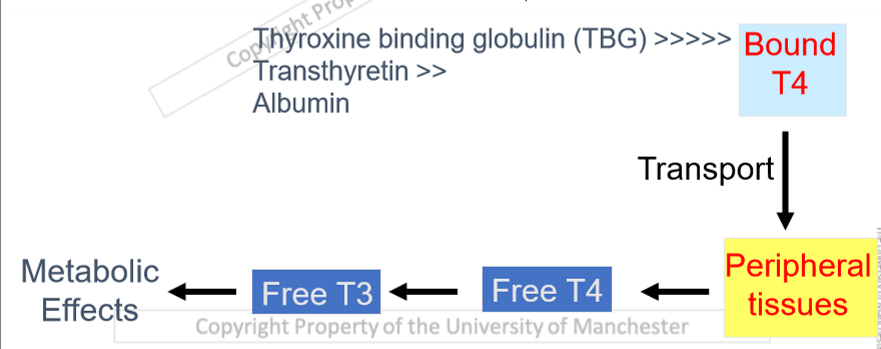
thyroid hormone transport
bound t4 circulated around the body
needs to be free to interact with receptors
different degree of looseness to binding proteins
t4 needs to be converted to t3(active form)
thyroid hormone produced daily from thyroid gland
affinity and capacity of t4 binding proteins
albumin has loose bond with thyroid so it is released easily
when there is a lot of albumin, large capacity for binding protein to bind to hormone
TBG has high affinity and low capacity for t4
transthyretin has low affinity has a low affinity and high capacity for t4
albumin has a very low affinity and high capacity for t4
specificity of thyroid hormone binding proteins- t3
TBG binds to t4 and t3, half life 5 days
transthyretin binds t4 only, half life 2-3 days
albumin binds to t3 and t4, half life of 15 days
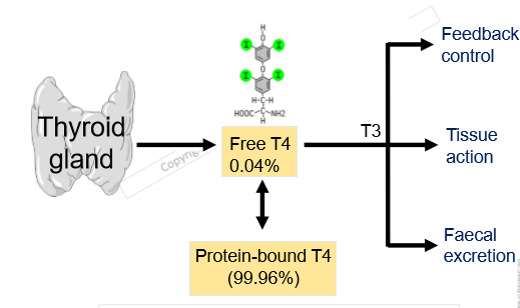
protein bound t4: protein bound t3 is 20:1
thyroxine binding globulin(TBG)
single polypeptide chain
20 CHO by weight
increased by t4 and oestrogens/androgens
stability and half-life extended after t4 binding
doubles in concentration during pregnancy
levels lowered by corticosteroids, illness, stress, cirrhosis, nephrotic disorders
leaky nephrons- excrete it, lose from circulation
t4 location
small percentage will never be bound
t4 needs to be converted to t3 first
TBG and TTR functions
prolong t4 availabilityy to target tissues
buffer effects of altered t4 secretion rate from thyroid gland
reservoir for t4 storage
determine and control rate and direction of delivery of t4 to specific tissues
transport of t3 and t4 into cells
bound t3 and t4 can’t enter cells
free t3 and t4 enter cells via specific transporters(MCT8, MCT10, OATP1c1)
t4 is inactive and must be converted to t3 by intracellular iodothyronine deiodinases
iodothyronine deiodinases
seleno-cysteine containing enzymes
selenium accepts iodide
inactive t3 is there to make sure correct amount of thyroid hormone is present to allow correct brain development in the foetus
DIO3 fine tunes concentration of thyroid during development
iodothyronine deiodinaase 1 -DIO1
predominates in liver, kidney and muscle
also found in thyroid
produces most of circulating t3
iodothyronine deiodinase 2- DIO2
predominates in areas of CNS, pituitary thyrotropes
controls intracellular t3 concentration
important for feedback regulation
found in skeletal muscle in some species
iodothyronine deiodinase 3-DIO3
produces inactive rt3
prevents thyroid hormone access to specific tissues
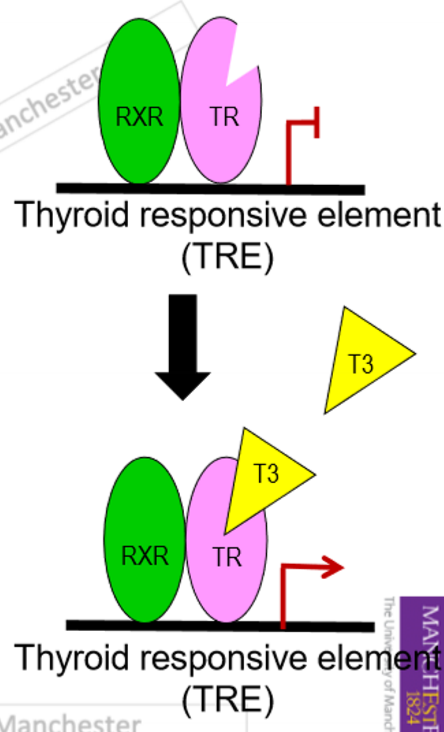
thyroid hormone action
thyroid hormone receptor(TR)
TR alpha and beta
found in nucleus
heterodimer with retinoid X receptor
works as a transcription factor
binds to thyroid responsive elemen(TRE)
increased 15 fold affinity for t3 than t4, so t3 more active
increased gene transcription
can also inhibit gene transcription
in the anterior pituitary gland
t3 responsive genes include those encoding increased growth hormone, decreased prolactin, decreased alpha and beta subunits of TSH
when t3 bound it triggers transcription
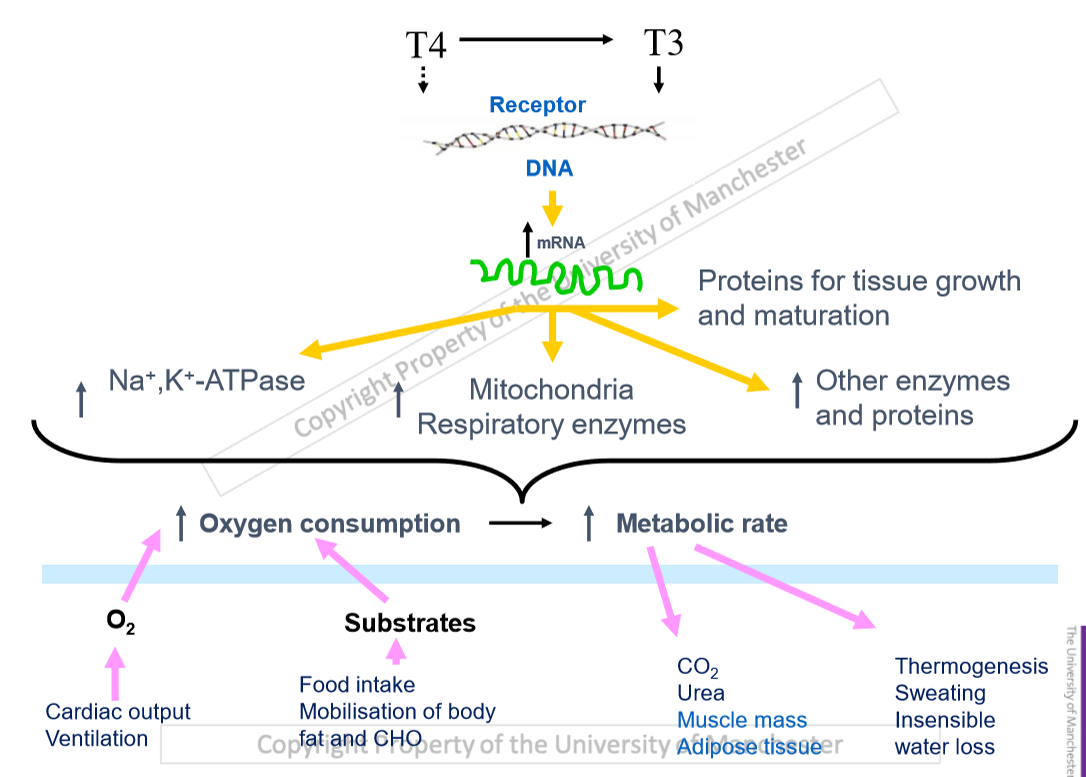
biological actions of thyroid hormones
control of basal metabolic rate
growth regulating roles of thyroid hormones
role of thyroid hormones in foetal development
cardiovascular effects
musculoskeletal effects
control of basal metabolic rate
influence expression of particular proteins
increase oxygen demand
increased cardiac output and ventilation rate
increased waste products
insensible water loss- breathe out more deeper, lose water from lungs
hyperthyroidism leads to high metabolic rate, tremor, muscle wastage
most common endocrine disorder in cats, weight loss despite normal or increased appetite
growth regulating roles of thyroid hormone
most bodily functions affected
often synergise with other hormones
deficiencies lead to abnormal growth, development, reproduction, behaviour, metabolism
exert effects on all organs and tissues throughout life
absence of thyroid hormone in children leads to growth problems
leads to arrest of bone elongation, delayed bone maturation, reduction in growth hormone secretion
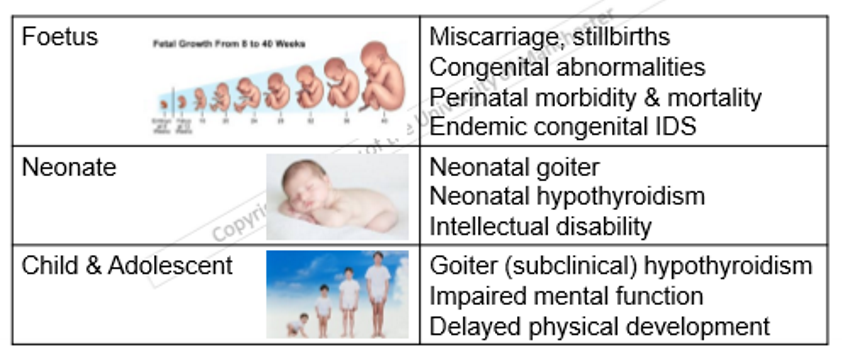
thyroid hormone in foetal development
key role in developing neural and skeletal systems
loss of t4 supply to foetus leads to irreversible intellectual disability and dwarfism
cretinism- iodine deficiency syndrome
metamorphosis requires thyroid hormones
cardiovascular effects
t3 increases cardiac contraction and output, heart rate, oxygen supply to tissues, CO2 removal from tissues
direct effects- increased myocardial Ca uptake, increased expression of alpha myosin heavy chain decreased beta, increased expression of ryanodine receptor(RYR) in SR
indirect effects- increased metabolism, thermogenesis, vasodilation, increased sensitivity to catecholamines
musculoskeletal effects
t3 has potent stimulatory effect on bone turnover, increasing formation and resorption
t3 increases linear bone growth after birth
t3 increases rate of muscle relaxation
normal skeletal muscle function needs t3
smaller skull for hypothyroid individuals