week 9
osmolarity
the total concentration of all solute particles in a solution
exact composition of ICF (intracellular fluid) vs ECF differs, but at equilibrium the osmolarity of each compartment is the same
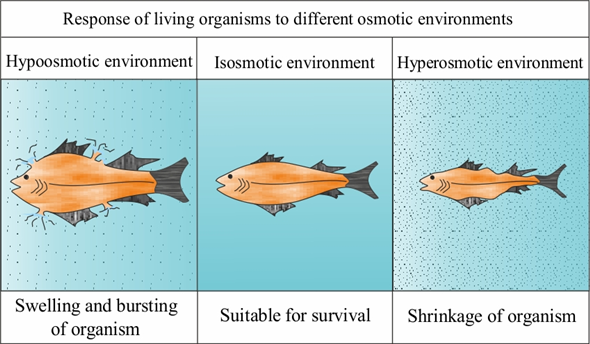
The osmolarity of ICF compared to ECF determines whether water will move from one compartment to the other
a sudden change in osmolarity will result in water moving down its osmotic gradient altering the volume of one compartment compared to the other
can have significantly deleterious effects on normal physiological functioning of organ systems
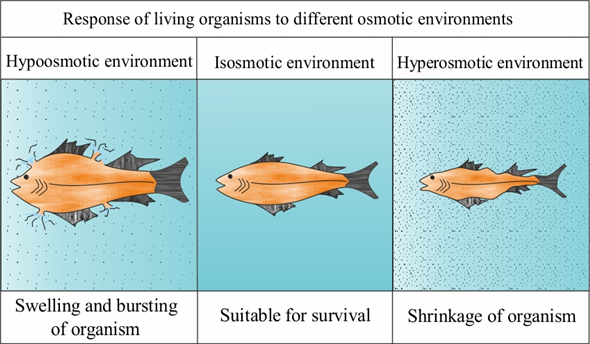
sudden decrease in ECF osmolality
water would move from the ECF into the ICF
causes swelling of cells
In parts of the body where the tissue doesn’t have room to expand (e.g. the skull): sudden increase in pressure within the tissue → compromises blood supply
swelling brain becomes ischaemic and also herniates out through gaps in the skull such as the foramen magnum further compromising blood supply to vital areas such the brainstem eventually leading to death
sudden increase in ECF osmolality
causes water to move from the ICF to the ECF
the cells will shrink
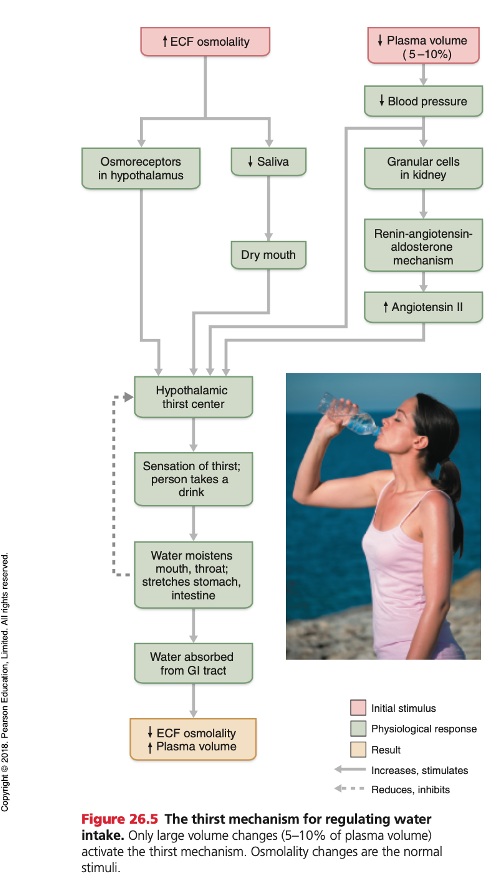
decrease in membrane stretch (in osmoreceptors) activates the hypothalamic effector cells resulting in the sensation of thirst
mechanism in charge of maintenance of osmolality
thirst ADH mechanism
osmoreceptors
(membrane) stretch receptors
located in the hypothalamus
cells either swell or shrink depending on changes in the local ECF osmolarity
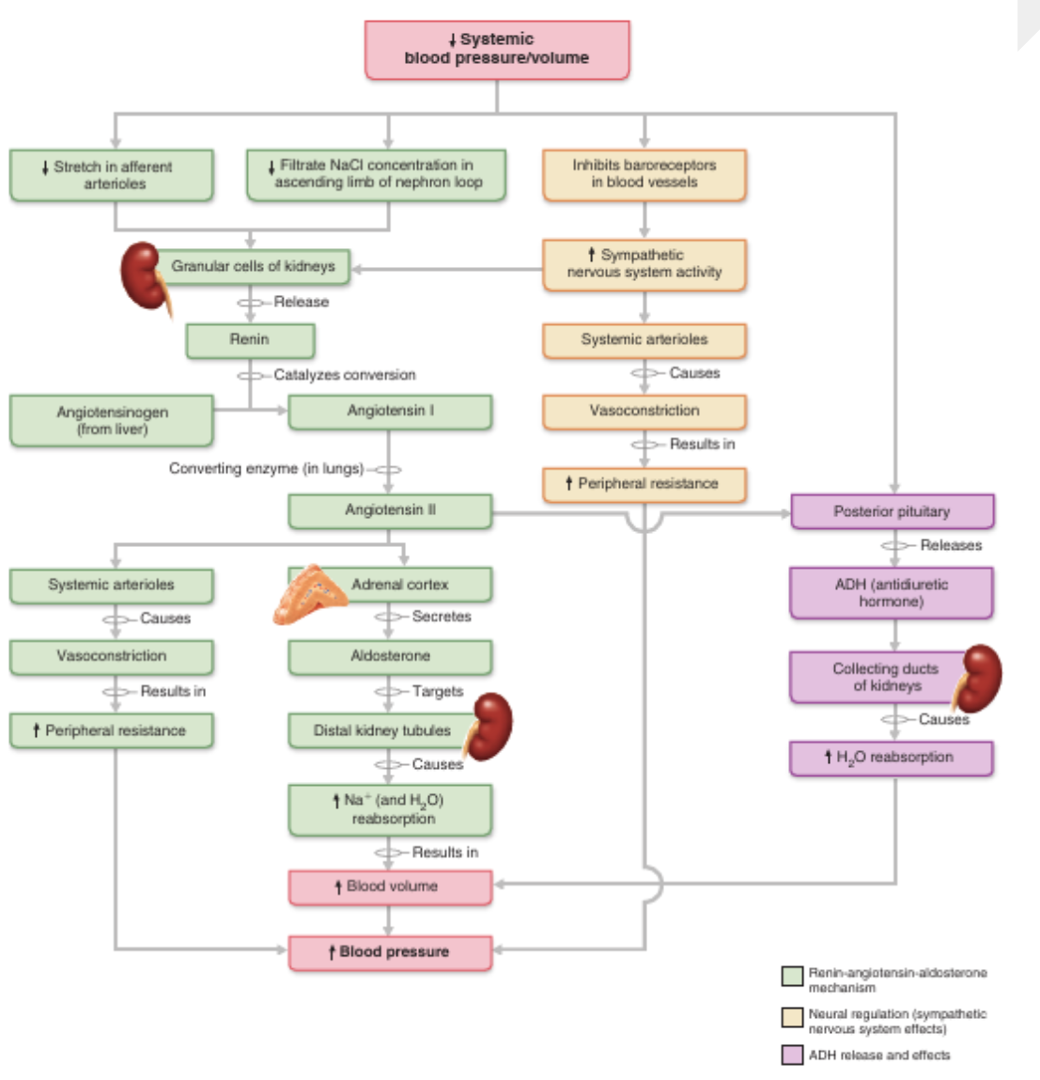
Hypovolaemia
loss of intravascular volume causes a decrease in stretch – the baroreceptors feed this back to the vasomotor centre in the brainstem
e.g. sweating
detected by stretch receptors/baroreceptors
(located in the kidney (granular cells) & great vessels: aorta, carotid arteries, vena cava, atria)
The response of the vasomotor centre to hypovolaemia includes:
increase in sympathetic nervous system activity (maintains blood pressure and flow to vital organs)
Activation of the hypothalamic thirst centre
Activation of the renin angiotensin aldosterone system (RAAS)
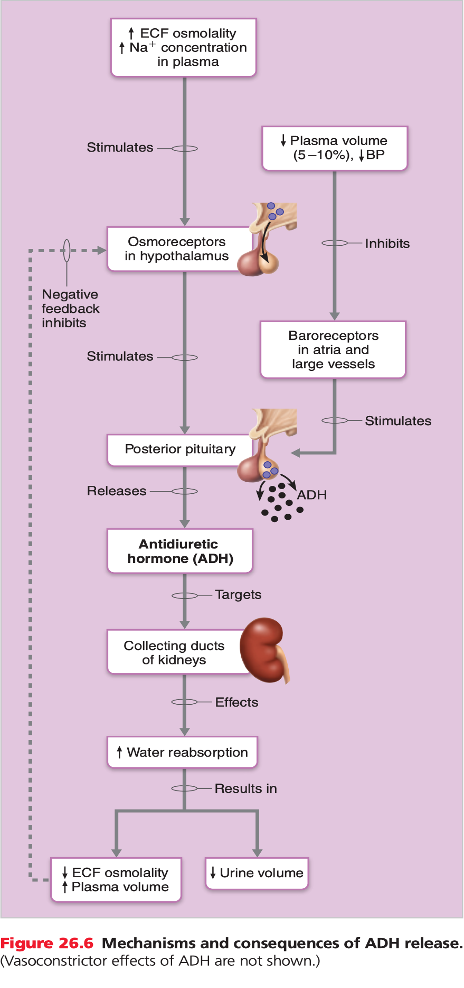
ADH secretion from the posterior pituitary
ADH purpose
regulates water output
triggered by increase in ECF osmolality or decrease in water volume
produced in hypothalamus → secreted by posterior pituitary gland
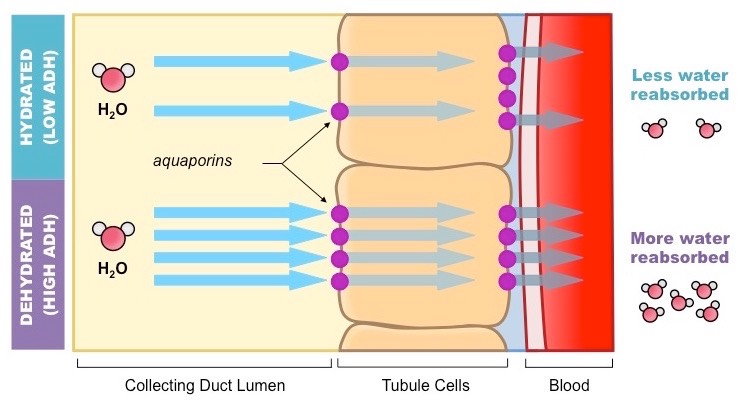
ADH process of action
insertion of pre-formed water channels (aquaporins) into the luminal membrane of principal cells in the renal collecting ducts
→ makes the luminal membrane permeable to water
→ water moves out of the renal tubular fluid (hypo-osmotic) down its osmotic gradient into the hyperosmotic renal interstitium
hyperosmotic
ICF higher osmolality (solute concentration)
hypoosmotic
ECF higher osmolality (solute concentration)
RAAS
Renin angiotensin aldosterone system
controls volume status via effects on sodium reabsorption in the kidney
Hypovolaemia → production of renin by the renal granular cells
rate limiting step in the production of the hormone angiotensin II (AII)
angiotensin II actions
target of antihypertensive drugs - inhibited by ace inhibitors
increases Na reabsorption in the kidney
stimulates production of aldosterone
(also Na reabsorption)
systemic vasoconstriction via AT1 receptors (increase BP)
preserves renal function by selective vasoconstriction of some renal arterioles (only at low levels, maintains glomerular function)
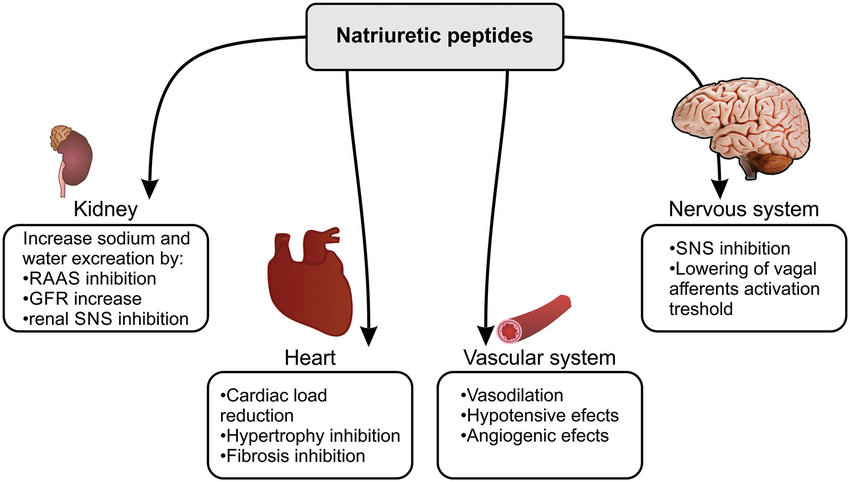
natriuretic peptides
released when hypervolemic
Atrial and brain natriuretic peptides (ANP, BNP) inhibit secretion of renin and aldosterone
burns fluid loss
systemic inflammatory response - vasodilation and capillary leakiness
damage to skin barrier
damage to cells - loss of intracellular volume into ECF
loss of intravascular volume (blood volume) into ECF
Fluid from leaky capillaries internally results in oedema of tissues and organs
Without intervention, hypovolaemic shock occurs
hypovolaemic shock
Shock: condition in which blood vessels are inadequately filled, blood cannot circulate normally
signs: tachycardia, increased capillary refill time
Hypovolaemic shock: shock due to loss of intravascular volume (either plasma and red cells or just the plasma)
common causes: blood loss, vomiting, severe diarrhoea, extensive burns
intravenous fluids
most common type: crystalloid: consists of water and electrolytes, same osmolality as ECF
most common IVs:
sodium compound lactate (CSL)
normal saline (0.9% NaCl)
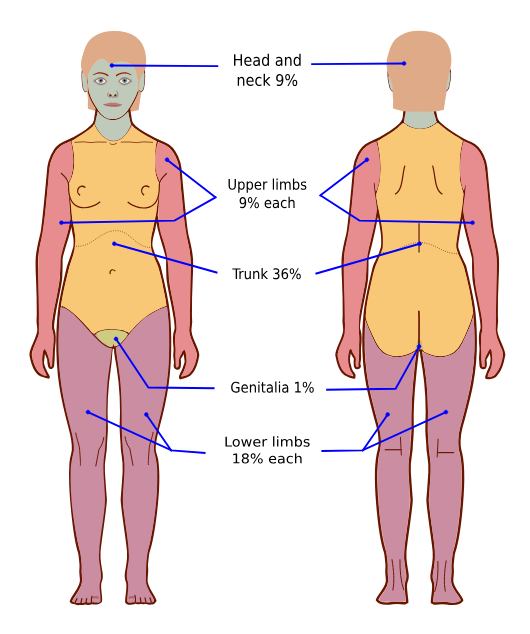
Parkland formula
used to guide fluid management in patients with major burns
3-4mls / kg / %burn
over the first 24 hrs
half should be given in the first 8hrs, the other half over the following 16hrs
paediatric fluid replacement (e.g. dehydration)
volume resuscitation
normal saline of CSL until signs of shock resolve
maintenance
ideally orally-administered isotonic, 5% glucose (prevent hypoglycemia) fluids
4:2:1 formula (Useful guide, but over-estimates requirements)
replacement of ongoing losses
measure or estimate ongoing losses
baroreceptor stimulation
indicates increase in MAP