Surgical Radiography
1/116
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
117 Terms
Zone 1
Un-restricted- may enter in street clothes
Zone 2
Semi-restricted- only person in scrubs, hair and shoe covers
Zone 3
Restricted- must also have mask on
Benefits of Radiography in the OR
Precision placement of surgical implants/ shorter surgery time
less invasive surgery, smaller incisions/decreased risk of infection
Identification of retained surgical objects like sponges and needles
Visualization of soft tissue anatomy with contrast (vascular)
sterile gown
waist up
Clean C-arm how much
Once a week
We are a member of the non-sterile team
surgery
Challenges
Technologists work under the direction of surgeons
Necessary skills include aseptic technique, radiation protection, communication, anatomic landmarks, and pathologic findings
Must be able to perform accurately, quickly, and competently
Radiation Protection in the OR
Placing the image intensifier (III) on top decreases radiation exposure for all staff
Radiation protection
Image intensifier on the Top (More scatter)
Radiation protection
Image intensifier the Bottom
The closer the image intensifier is to the x-ray tech is it better or worse for the tech?
Better for the tech
Advantages of II Closet to Patient
The closer the image intensifier is to the patient= the further the tube is from the patient
Results in:
-Less magnified image
- Less radiation (entrance skin dose) to the patient
Mini C-Arm
Very compact, mobile fluoroscopic imaging system designed for real-time imaging of the extremities
Provides imaging versatility right in the surgical suite, regardless of how challenging the extremity procedure may be
O- Arm
Intraoperative surgical imaging system, with the ability to obtain 2D and 3D images that can help confirm alignment and accuracy during spinal procedures
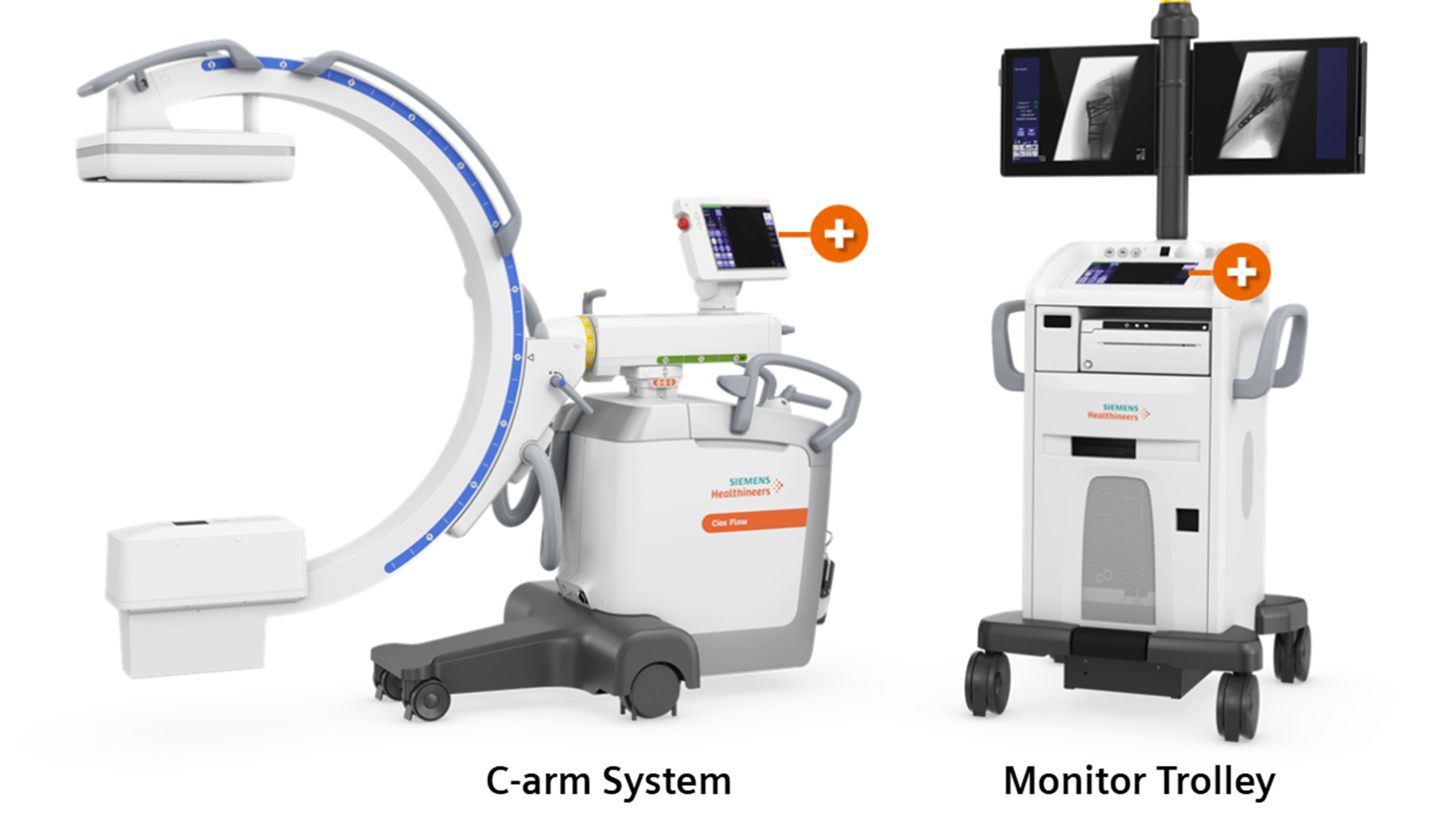
C-arm system
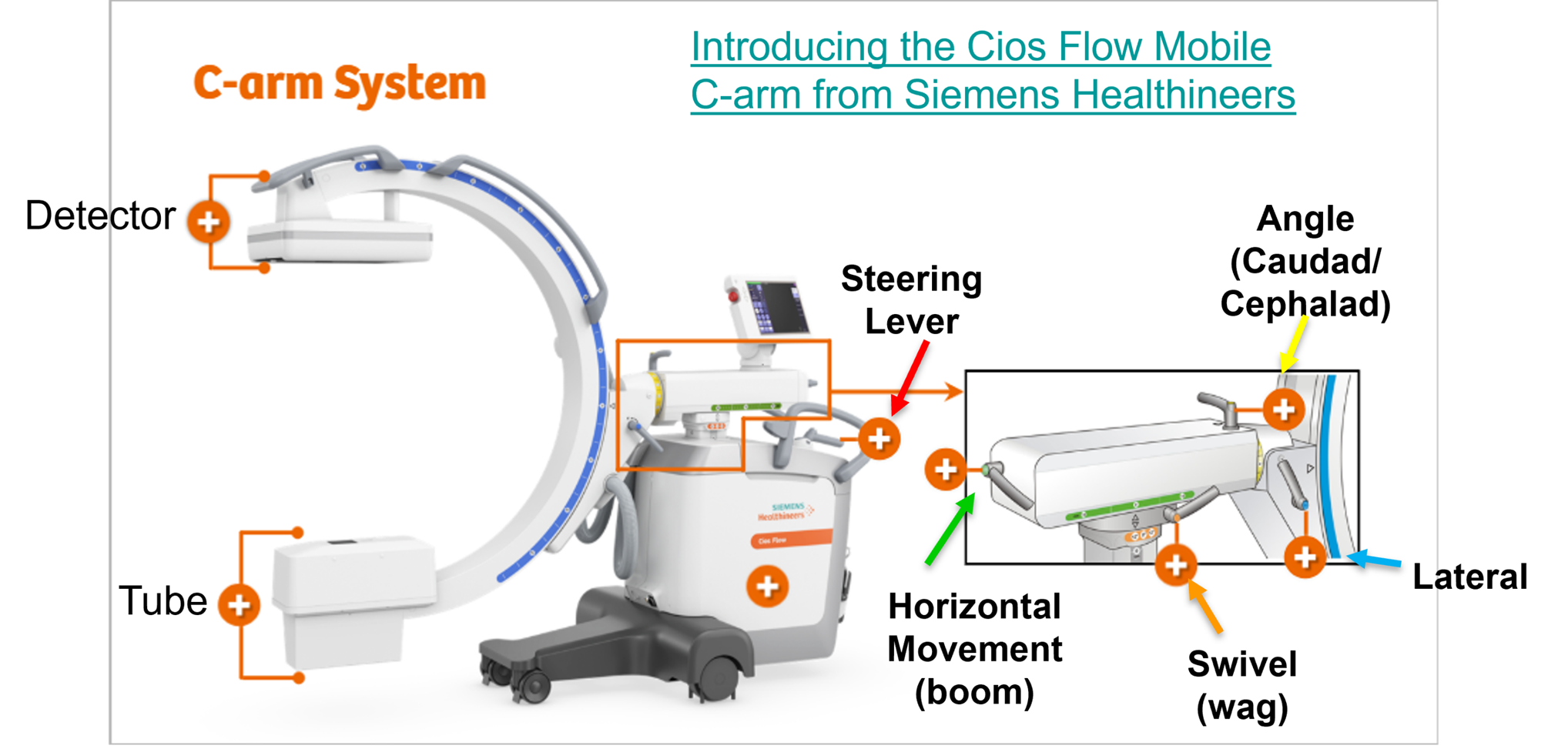
C- arm system + Monitor
Horizontal Movement (Boom)
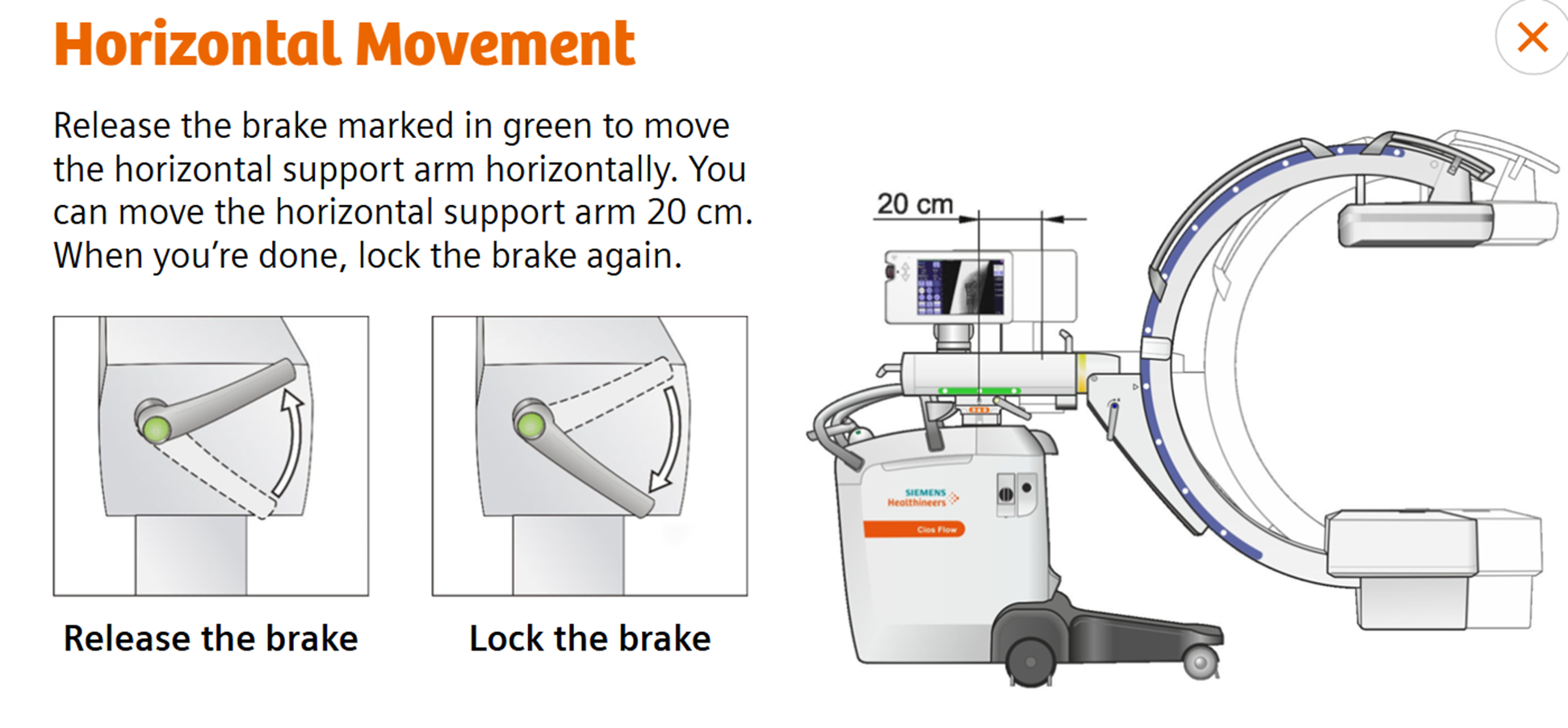
Release the brake marked in green to move the horizontal support arm horizontally. You can move the horizontal support arm 20 cm. When your done, lock the brake again
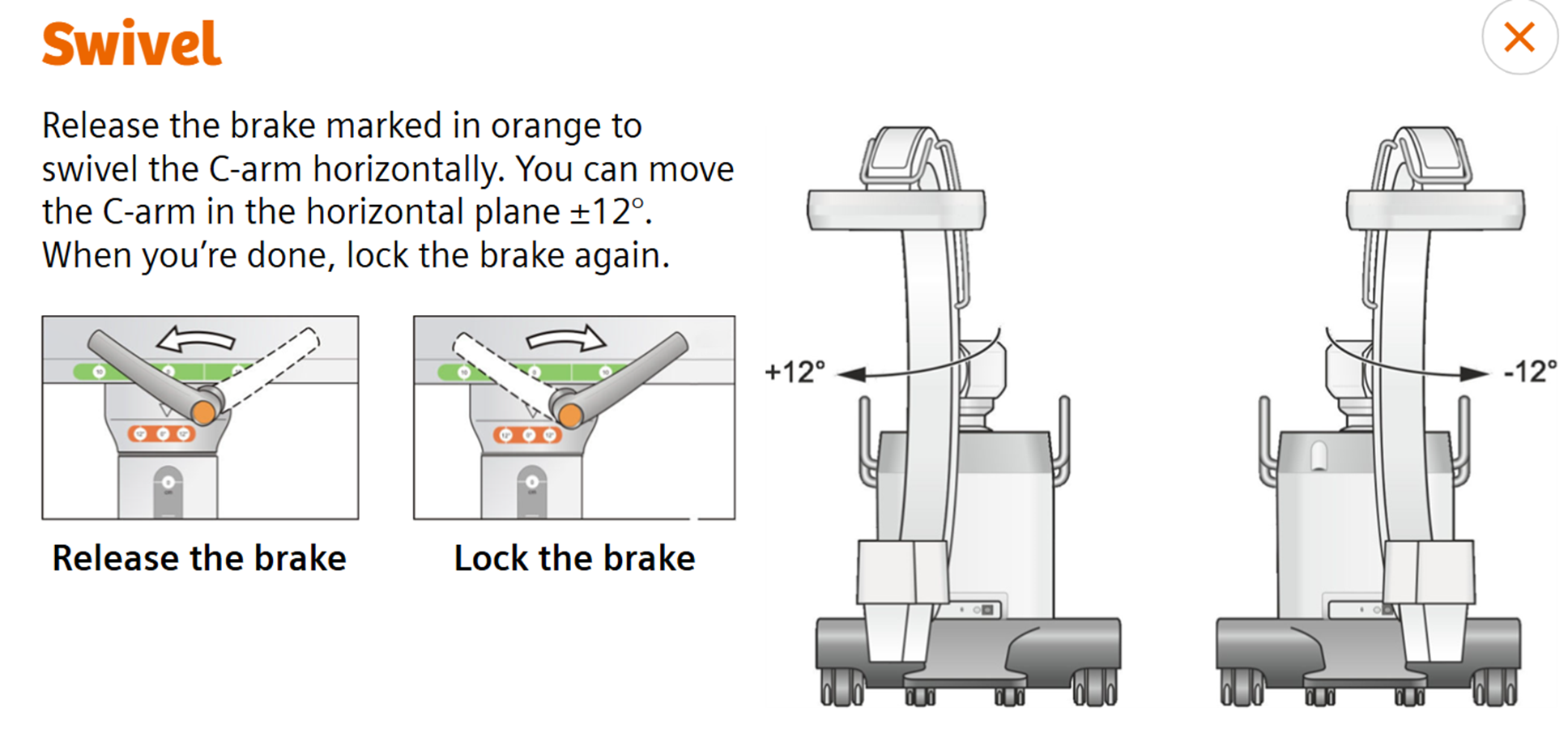
Swivel (Wag)
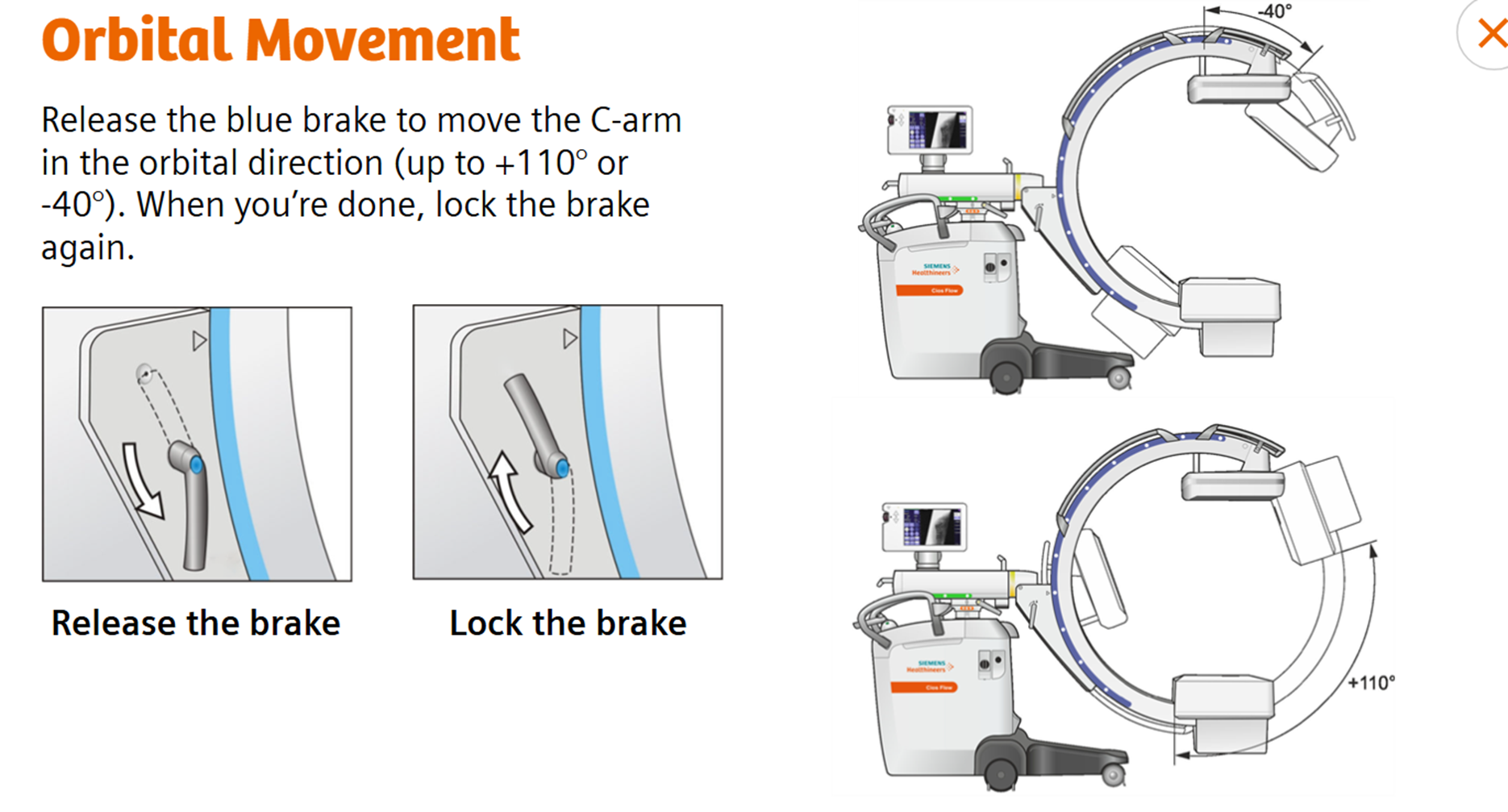
Orbital Movement ( Lateral)
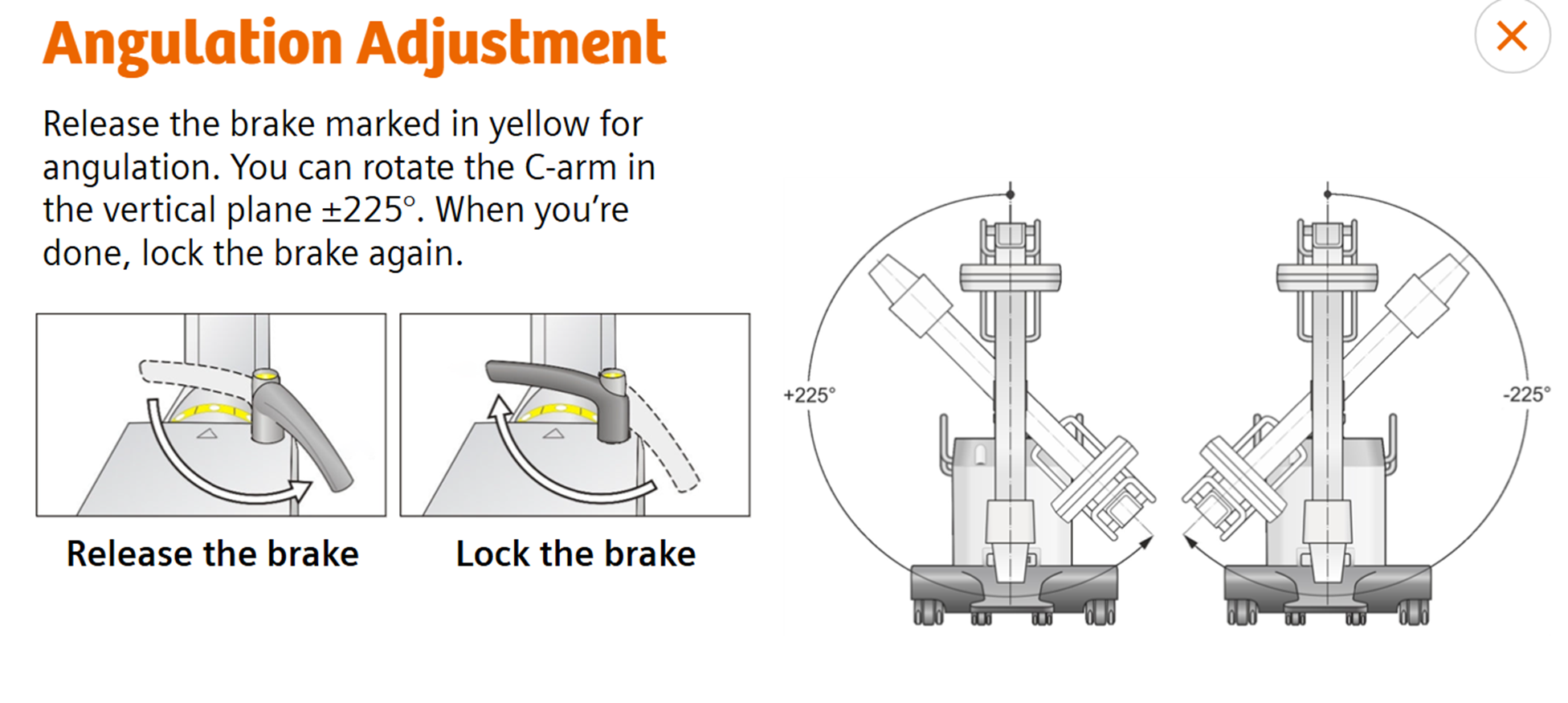
Angular adjustment
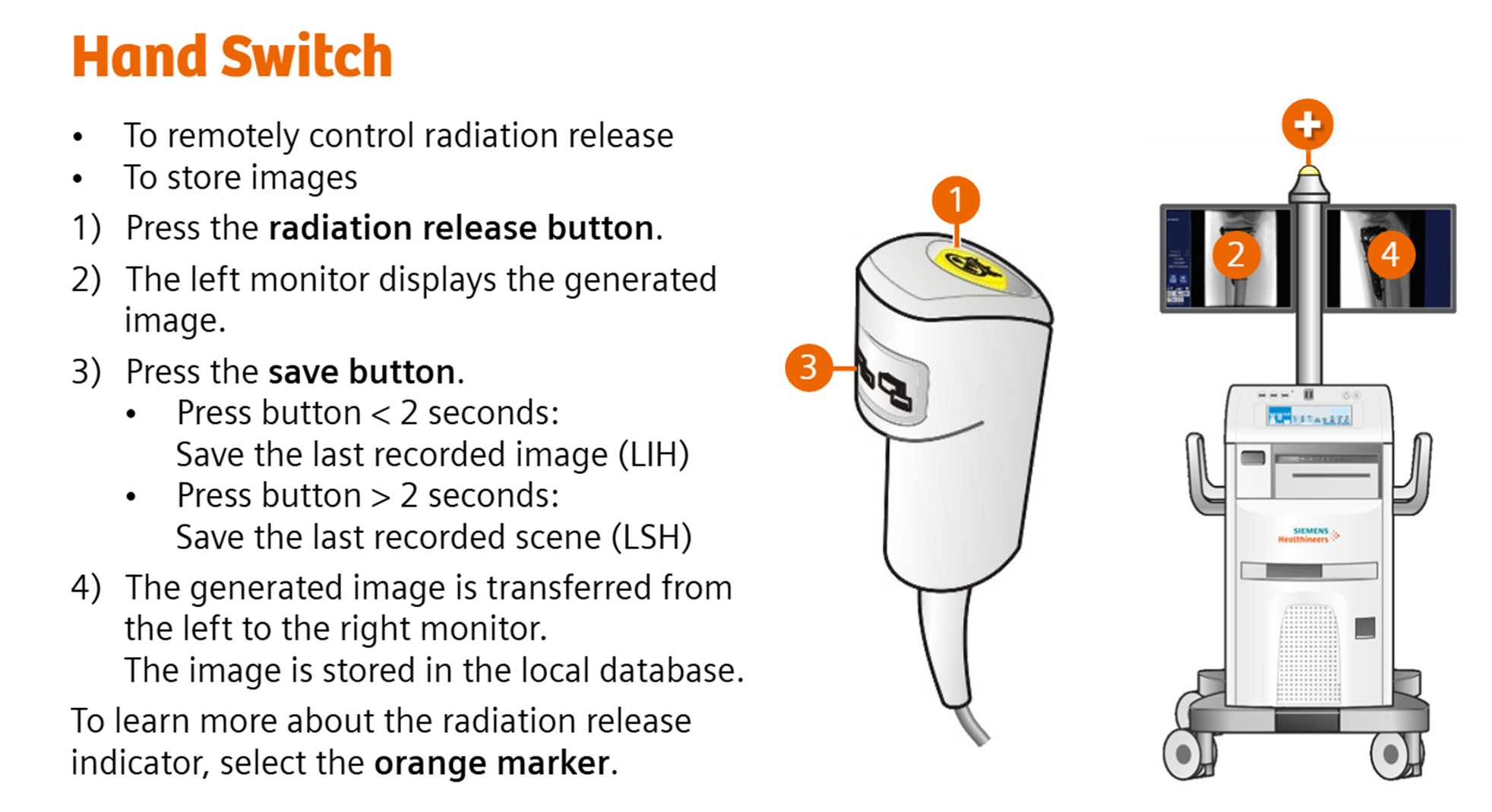
Hand switch
Remotely control radiation release
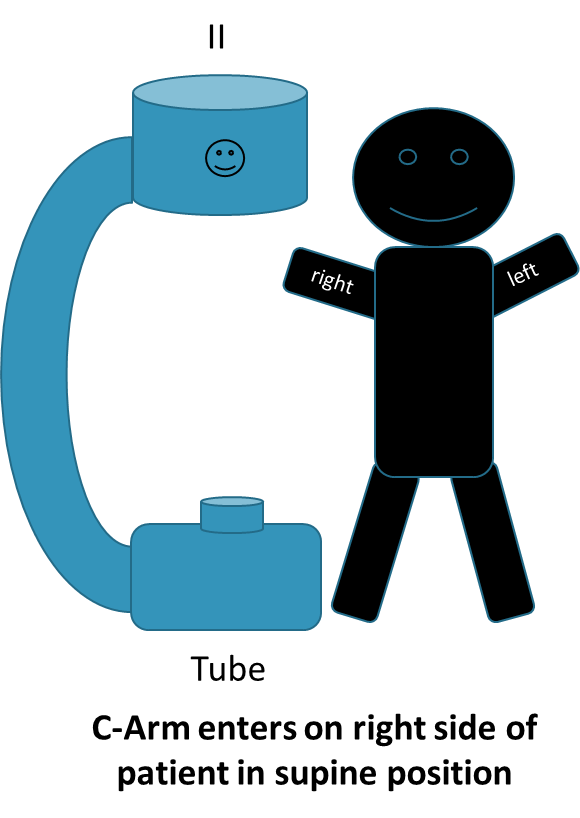
Smiley face
Located on the image intensifier
if standing at base of the c-arm, it would appear on right hand side Depicts position of patient
if smile is at head of patient, no orientation needs to occur to your image (coming in from left)
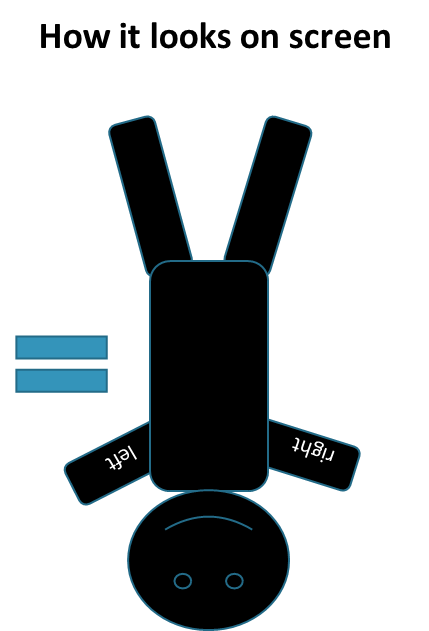
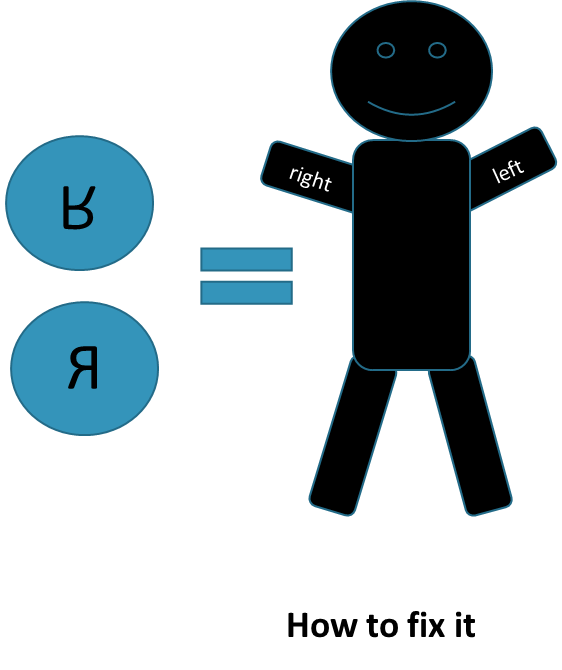
If smile is at foot of patient and the patient is supine, you need to orient by selecting both rs
If smile is at foot of patient and the patient is prone, you need to orient by selecting the head to toe R
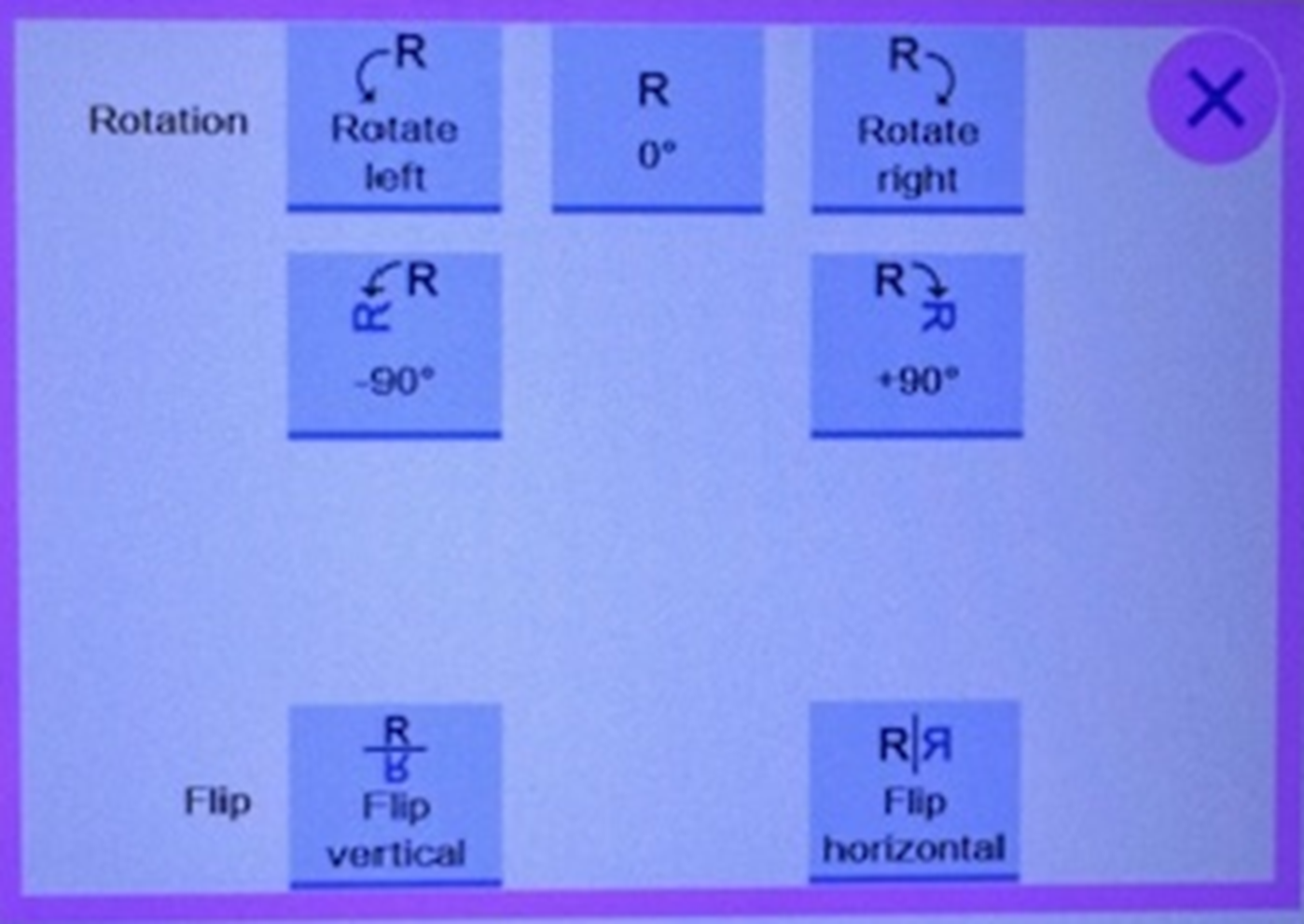
C-arm R’s
C-arm
Common procedures:
Cystoscopy-
ELC
ERCP
HIP NAILING/ FEMUR RODDING
ANTERIER HIP REPLACEMNTS
ORTHOPEDIC EXTREMIDIES
PAIN MANAGMENT
PORTABLE ABDOMEN
POERT OF CATH AND MORE
When OR is ready for us
OR cell phone- tech gets called and hands off to next tech or facilitator, signs out at facilitator desk
OR protocol book for review- by lead tech office and by OR computers
Identify patient via:
-Time out,
-check ID bracelet if not sterile
-check with anesthesia
ND-NC
No dictation, no charge transcribed, ex, cysto, portacath, spinal stim, bladder stim, or at surgeon request
Order Procedure
Ideally order before beginning procedure on computer in an OR but can order after if necessary
Index card, patient sticker from chart, begin time, fluoro time, c-arm number
OR protocol book for review- by lead tech office and by OR computers
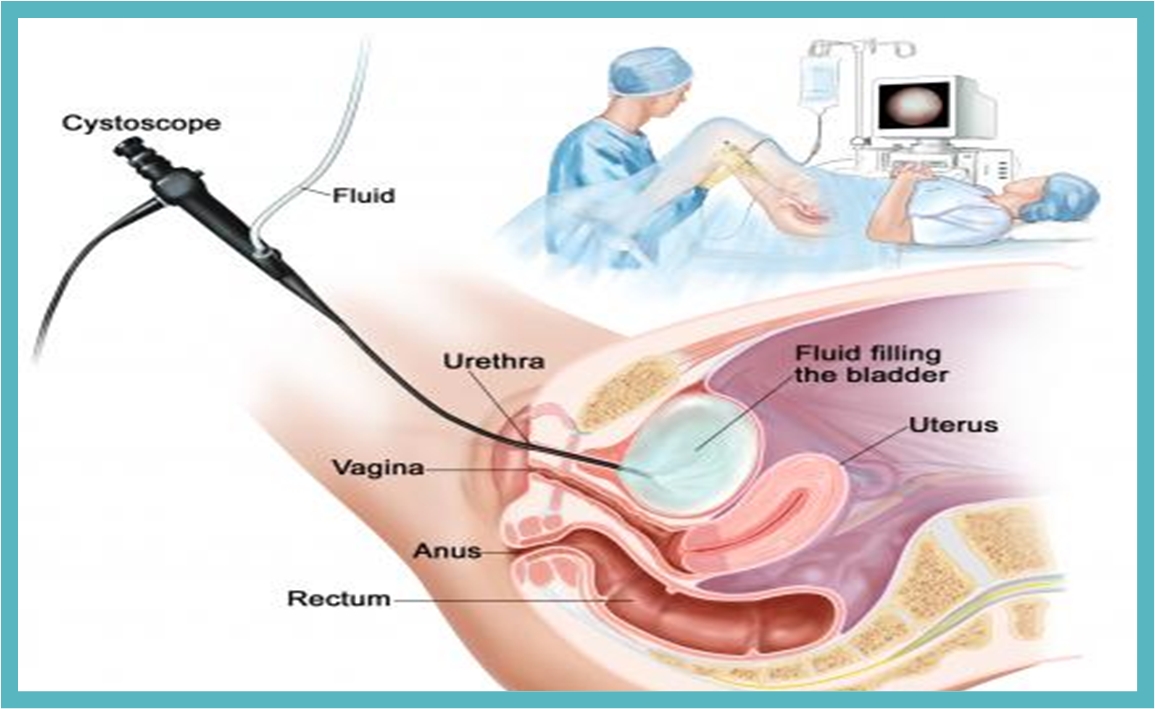
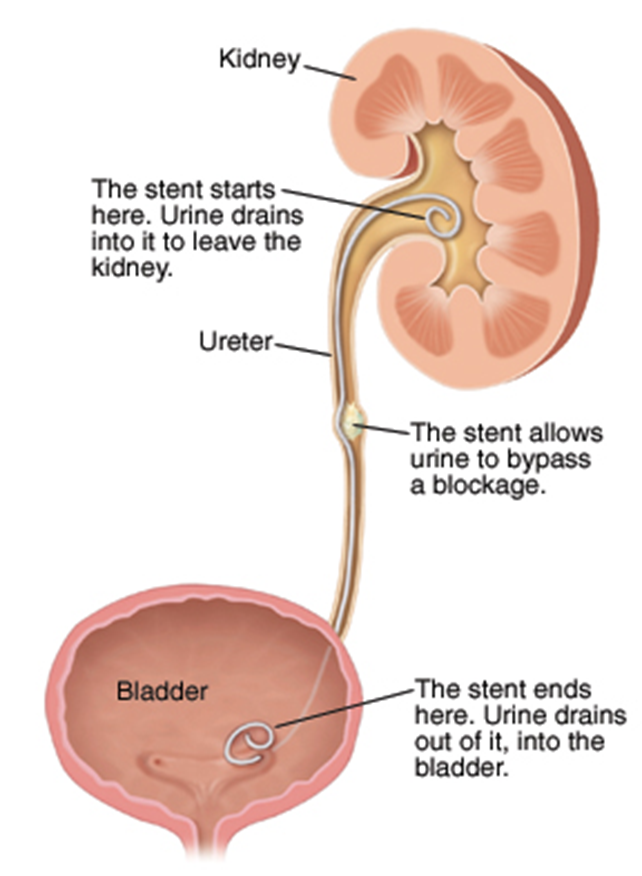
Cystoscopy- Cysto
A diagnostic procedure that allows the physicians to directly examine the urinary tract, particularly the bladder, the urethra, and the opening to the ureters. Cystoscopy can assist in identifying problems with the urinary tract, such as early signs of cancer, infection, strictures (narrowing), obstruction (stones), and bleeding
Charge- XR CYST ROOM ND-NC
Cystoscopy
Cystoscopy- put STENT in
Adenocarcinoma of Prostate
Type of cancer that develops in gland cells
radiographic apperance
elevates and impresses the floor of the constriction-filled bladder in an irregular pattern
Adenocarcinoma of Prostate causes
idopathic
risk factor- inherited gene mutation, inflammation of the prostate
complications- erectile dysfunction, urinary incontinence, and severe pain if the cancer spreads to the bones.
•Local stage
– No sign that the cancer has spread outside of the prostate. The relative 5-year survival rate for local stage prostate cancer is nearly 100%.
•Regional stage –
Cancer has spread from the prostate to nearby areas. The relative 5-year survival rate for regional stage prostate cancer is nearly 100%.
•Distant stage –
Includes the rest of the stage IV cancers – cancers that have spread to distant lymph nodes, bones, or other organs (M1). The relative 5-year survival rate for distant stage prostate cancer is about 29%.
Benign Prostatic Hyperplasia
Enlargement of the prostate gland
•Cause: Disturbance of hormone secretions from the sex glands
•Risk Factors – Age, family history, diabetes and heart disease, lifestyle
•Complications: Bacterial infection, pyelonephritis
•Radiographic appearance: Elevates and impresses the floor of the contrast-filled bladder in a smooth pattern
•J –shaped or fish-hook appearance of distal ureters
•Technical: No changes, Ultrasound used to visualize
•Prognosis: Good
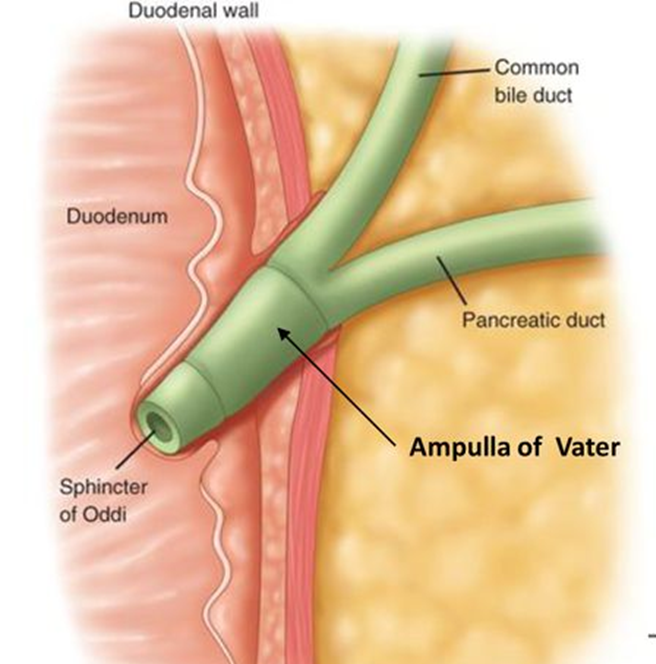
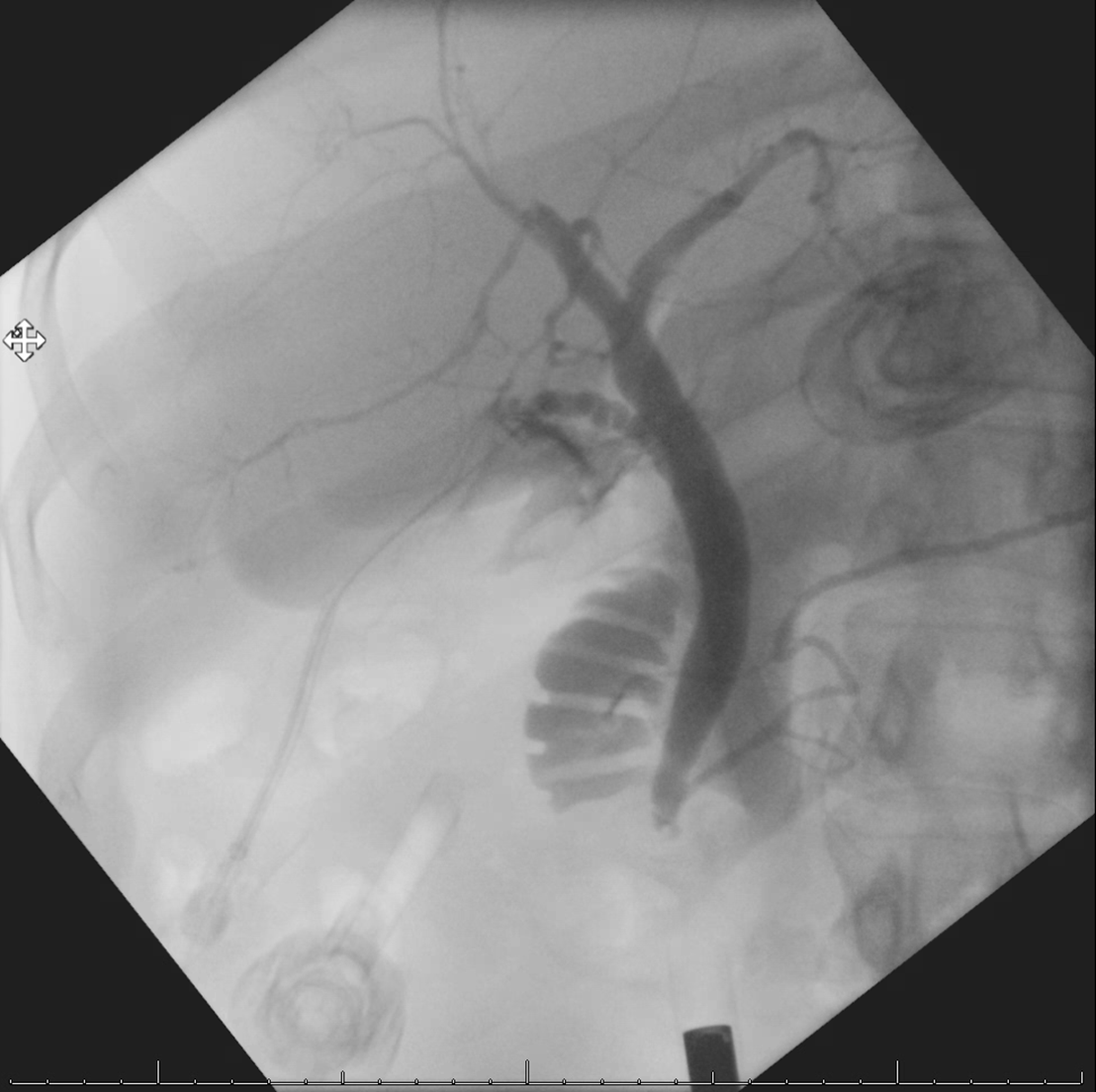
Surgical Cholangiography
AKA interoperative Cholangiogram (IOC)
Investigates the patency of the bile ducts and the functional status of the sphincter of the hepatopancreatic ampulla to reveal the presence of calculi that cannot be detected with palpation
•After exposing, draining, and exploring the biliary tract, and frequently after excising the gallbladder, the surgeon inject contrast (cholangiogram)
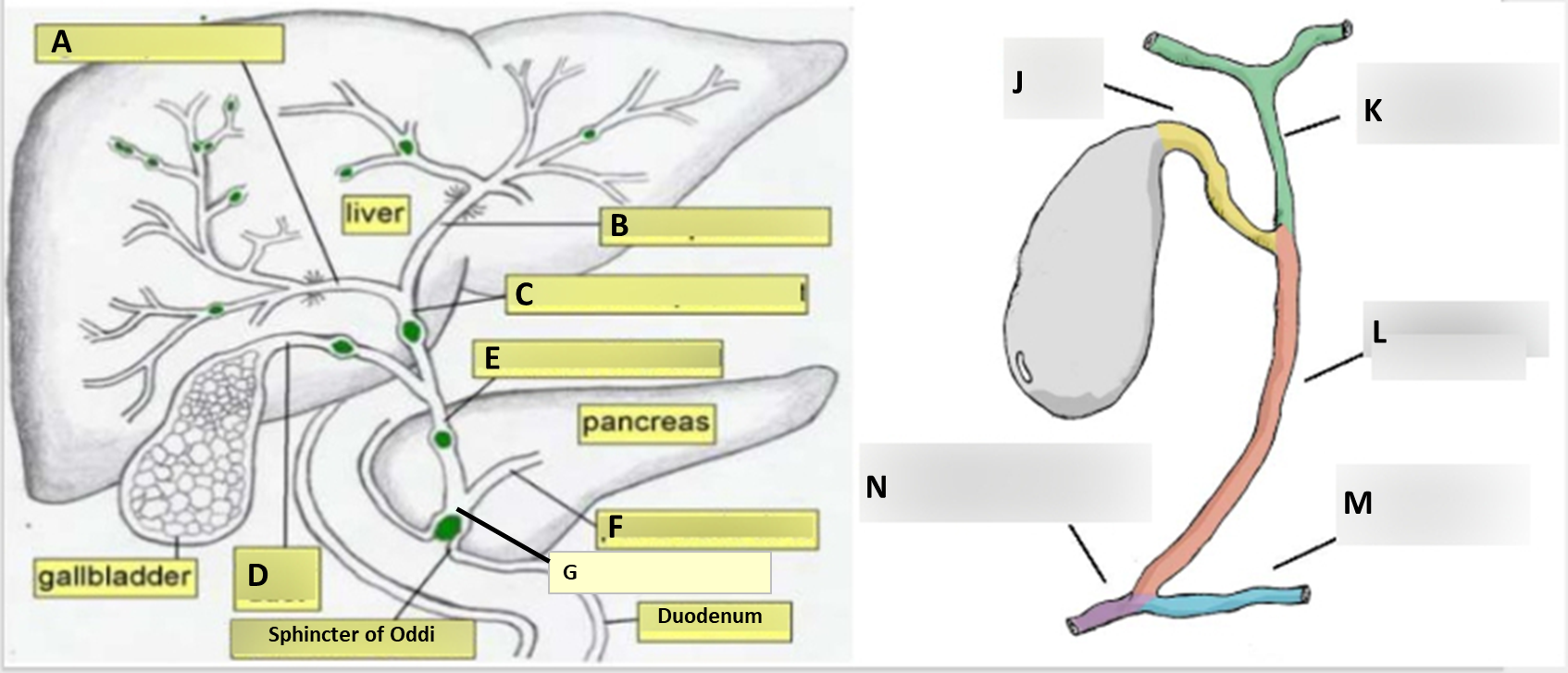
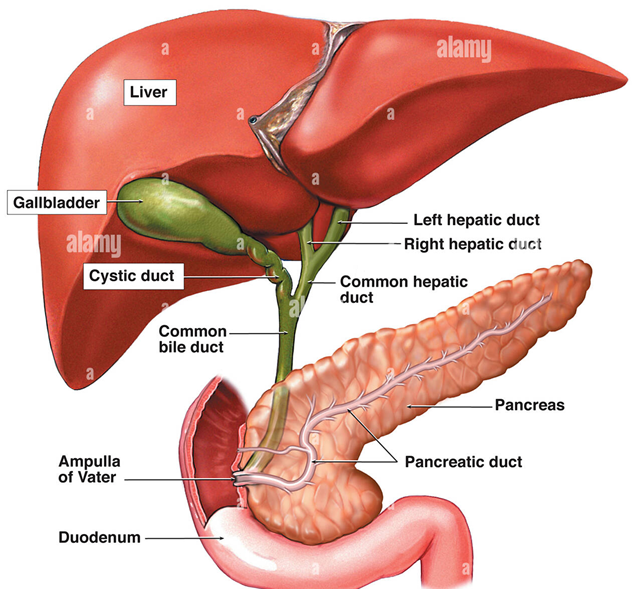
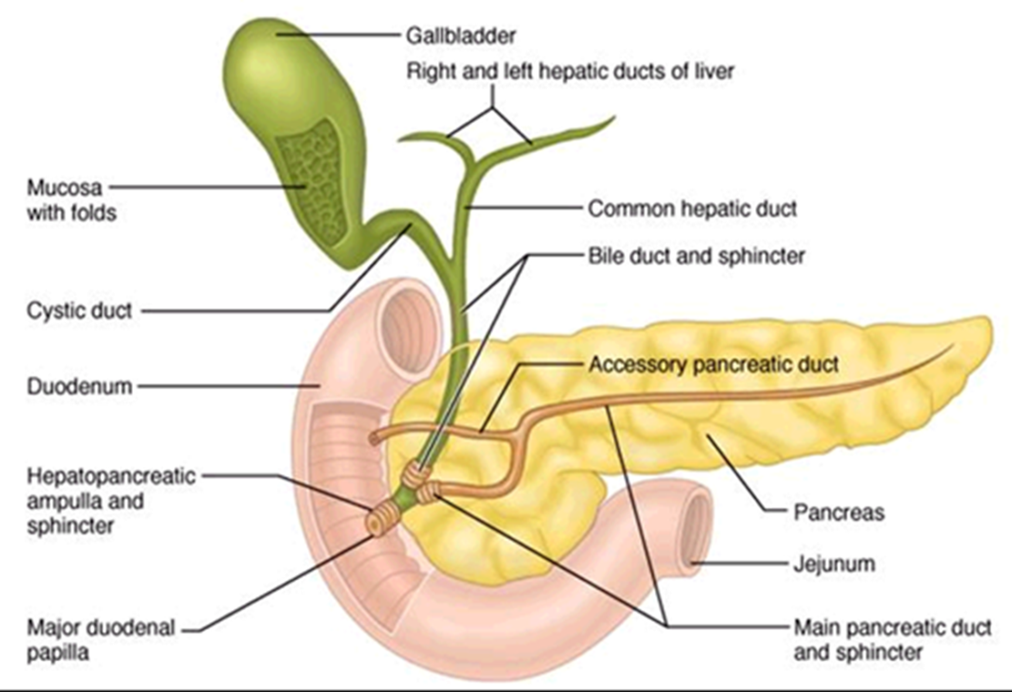
Anatomy
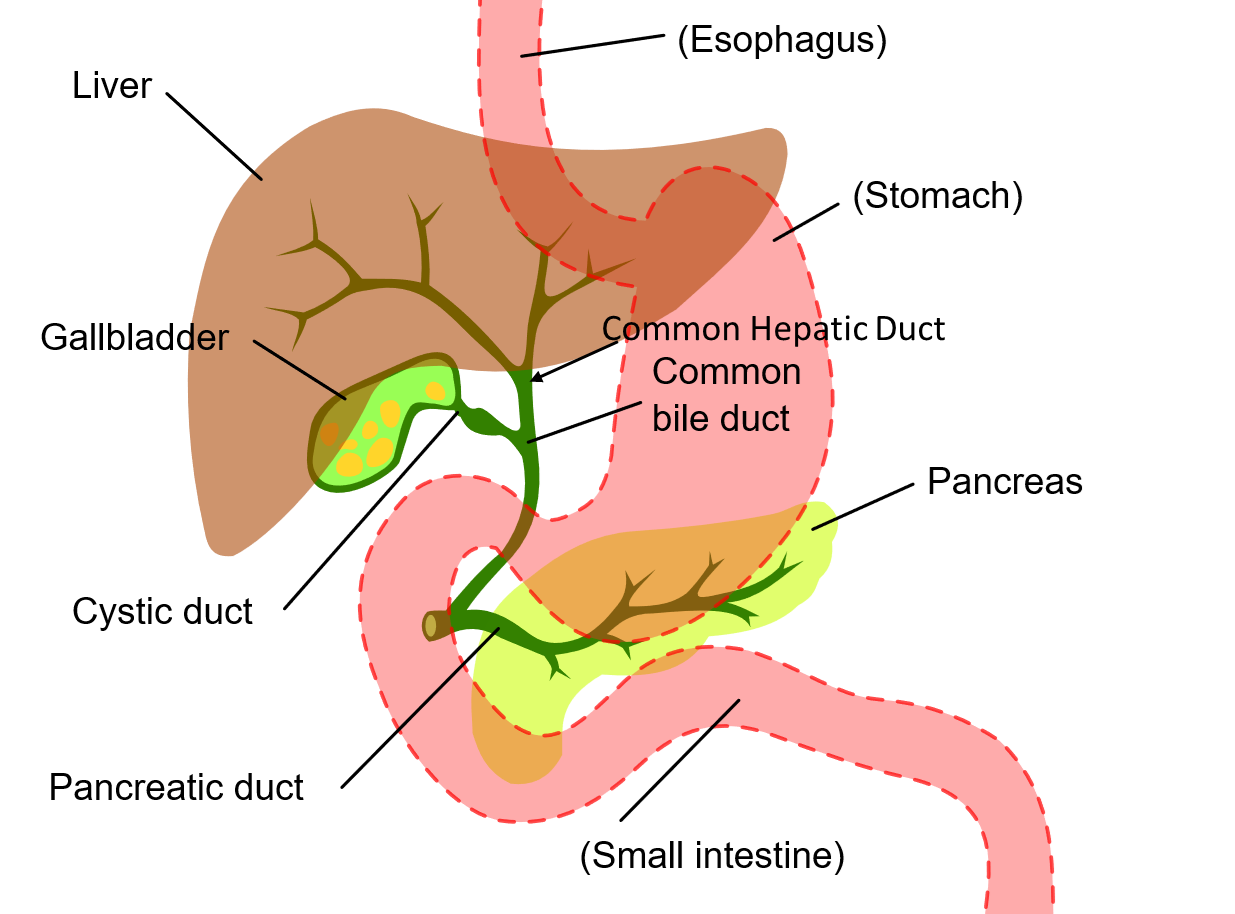
Anatomy
Anatomy
X-ray of anatomy
Early Laparoscopic Cholecystectomy (ELC)
•Surgical removal of the gallbladder using a tiny camera inserted through the navel for guidance (laparoscopic)
•When imaging is used during an ELC it is referred to as an Operative Cholangiogram (can also be done using the portable and a detector)
•Approximately 20 million people in the United States have gallstones. Of these people, there are approximately 300,000 cholecystectomies performed annually.
ELC
•The surgeon locates the common bile duct and inserts a catheter to introduce x-ray contrast
•
•Technologist responsibilities:
•Move the C-Arm to directly over the patient’s gallbladder (right upper quadrant)
•The patient is supine on the table
•You will be obtaining a PA projection (tube under patient)
•Fluoro while the surgeon pushes contrast through the bile duct and biliary tree
•Send images to PACS
BOTH R’S
ELC- Anatomy
RH ELC
•The C-Arm remains parked against the OR wall until the surgeon places the catheter into the bile duct.
•After fluoroing the C-Arm is parked back against the wall and cleaned.
ELCs have 3 different charges
•“OP Cholangiogram”
•Any initial laparoscopic injection of contrast
“OP Cholangiogram ADL SET”
Charge for additional images, usually after the placement of a “T” tube done in an open cholecystectomy
“OP Cholangiogram ND – NC”
•– If no images saved since contrast was not successfully injected.
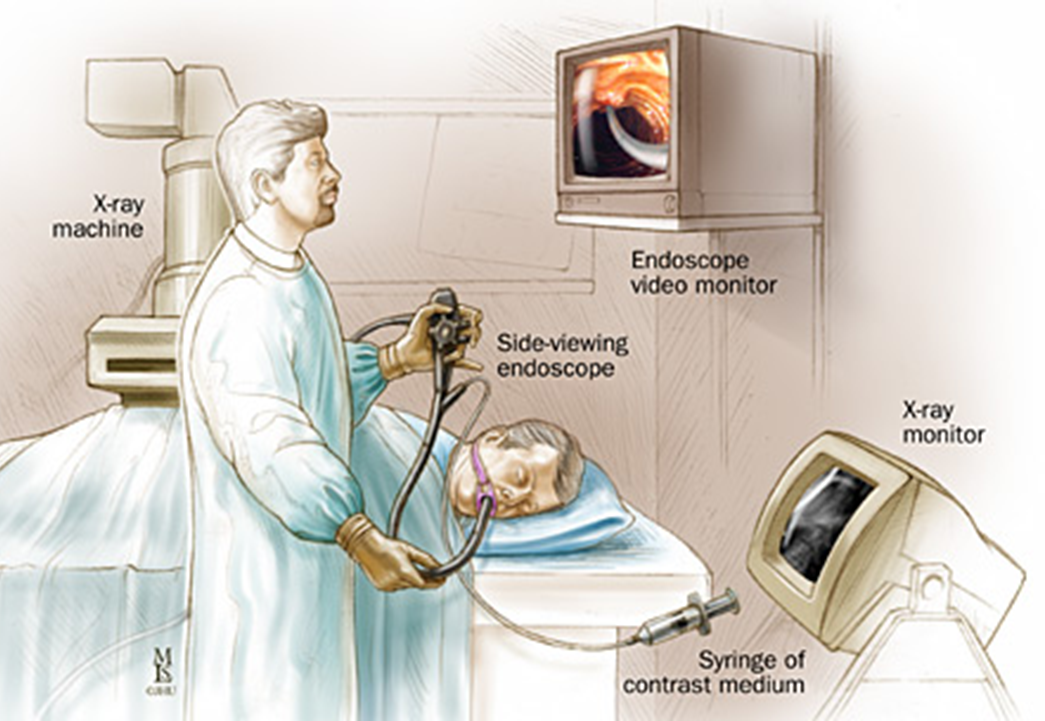
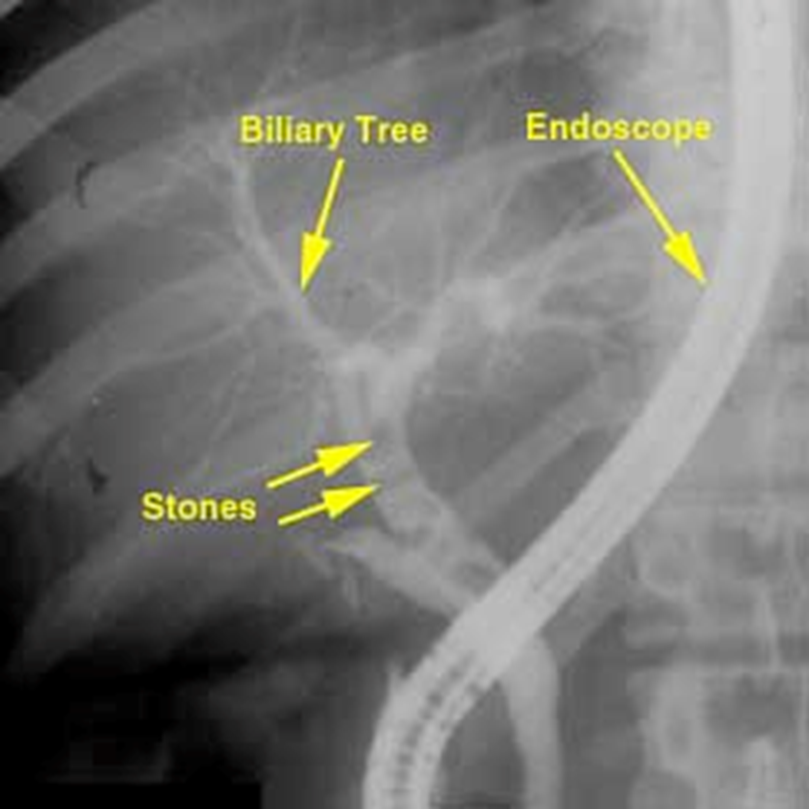
Endoscopic Retrograde Cholangiopancreatography (ERCP)
•Used primarily to diagnose and treat conditions of the liver, gallbladder, bile ducts, and pancreas including gallstones, inflammatory strictures (scars), leaks (from trauma and surgery), and cancer
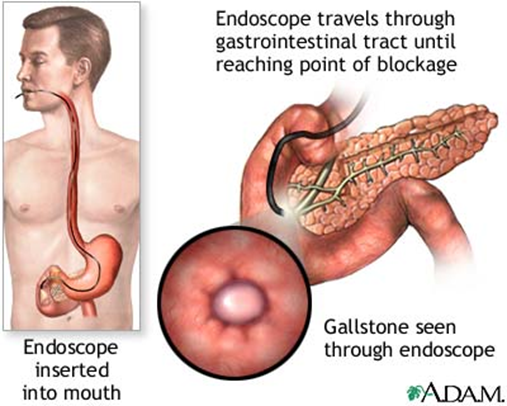
•Combines the use of x-rays and an endoscope
•Through the endoscope, the physician can see the inside of the stomach and duodenum, and inject contrast into the ducts in the biliary tree and pancreas so they can be seen on x rays
ERCP
•Performed by a Gastroenterologist (RH – Procedural Suites RM 8 T Ground)
•Technologist Responsibilities:
•Fluoro over the patient’s biliary system
•Save and send images to PACS
•RH Charging:
•ERCP – If biliary ducts and pancreatic duct visualized
•ERC – If only biliary ducts
•ERP – If only pancreatic duct
ERCP
– If biliary ducts and pancreatic duct visualized
•ERC
If only biliary ducts
•ERP
– If only pancreatic duct
RH ERCP (C-arm)
•The patient is in LAO position on the GI table.
•The C-Arm approaches from the patients left and centers over the right upper quadrant.
•Technologist will fluoro or provide doctor with fluoro pedal
ERCP

How gallbladder moves right upper quadrant
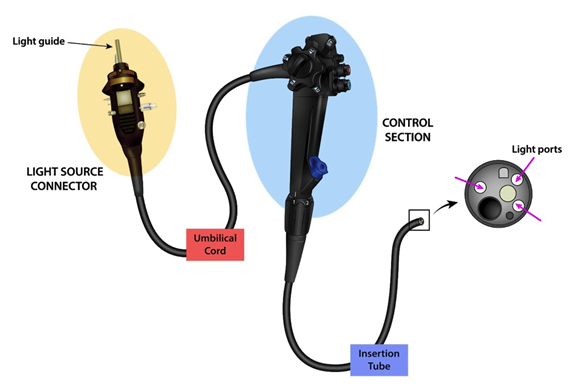
Endoscope
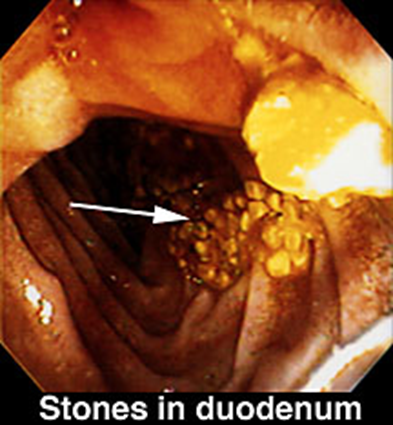
STONES

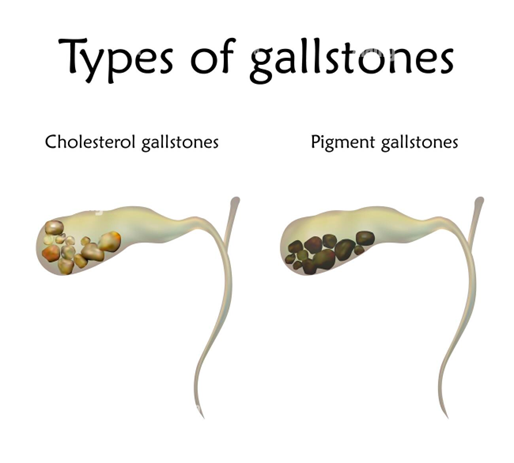
Cholelithiasis
Gallstones
•Hardened deposits in the gallbladder primarily made of cholesterol or bilirubin (pigment)
•Cause: idiopathic
•Genetic predisposition, excess weight, female
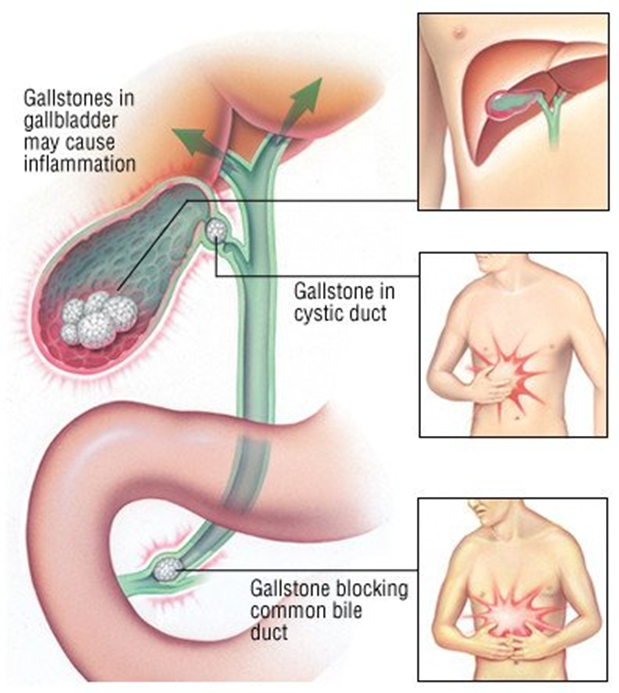
•Complications: Obstruction of the common bile duct. Inflammation or infection of the gallbladder or common bile duct
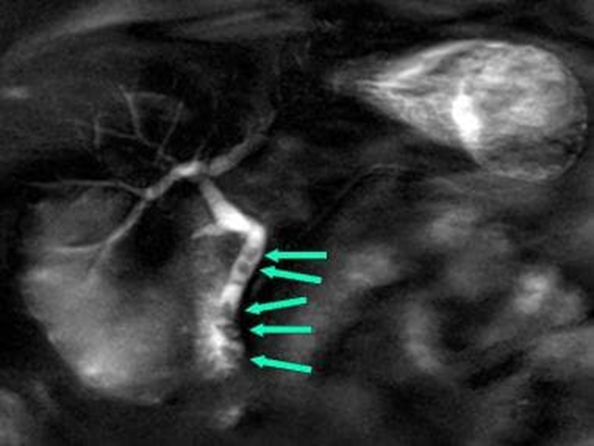
•Radiographic appearance:
•Most gallstones are radiolucent and visible only on contrast exams or US
•Alternating opaque and lucent rings
•Can have a Mercedes-Benz sign – if gas fissure is present inside it
•Prognosis: Good
Cholelithiasis

Cholecystitis
Inflammation of the gallbladder
•Cause: 95% of cases occurs after obstruction of the cystic duct
•Complications: Gangrene and rupture
•Radiographic appearance:
•US – distended gallbladder with gallstones with edema
•Radionuclide cholescintigraphy – failure to accumulate radioactivity in gallbladder
•Prognosis: Complete remission within 1-4 days
Cholecystitis
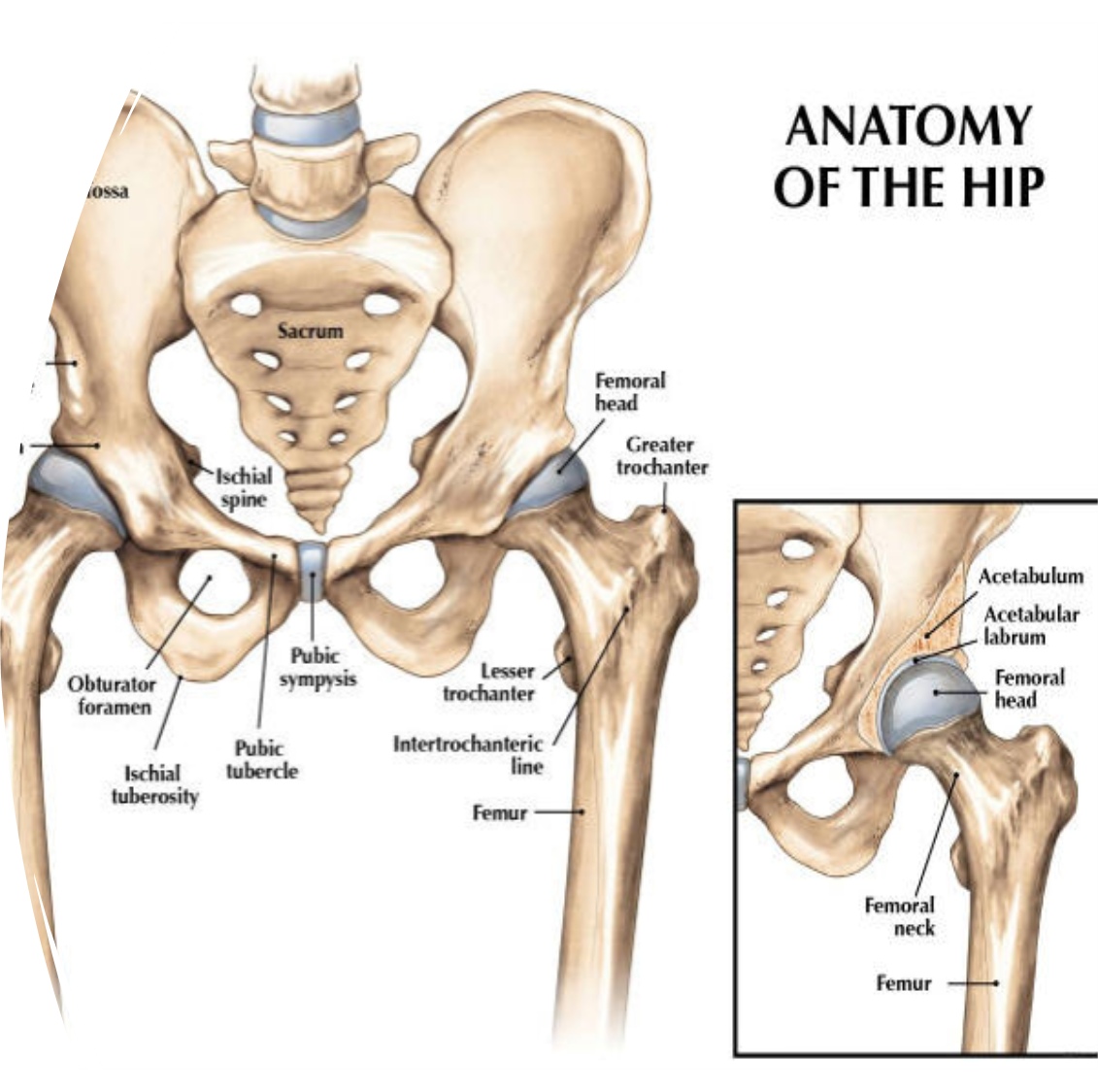
Anterior Hip Replacement
Surgeon makes a four-inch incision through the front of the leg
Benefits of the Anterior Approach
Frontal entry makes it possible to reach the joint by separating rather than cutting and then reattaching muscles
Less risk for hip dislocation after surgery
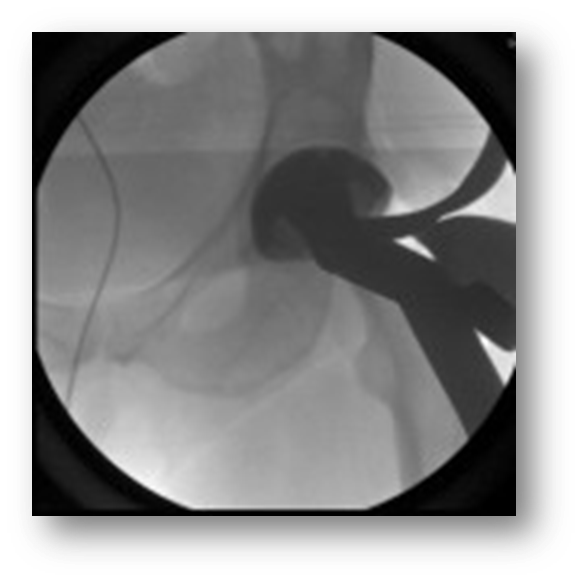
Anterior Hip Replacement
•C-Arm enters on opposite side of hip of interest
•At RH: images of the affected hip and pelvis are taken to see the trochanters and obturators
•PA views only
•Radlink may be used depending on physician
•There is a cable that connects the C-Arm to the Radlink tower so that the rep can pull images from the c-arm
Hip anatomy
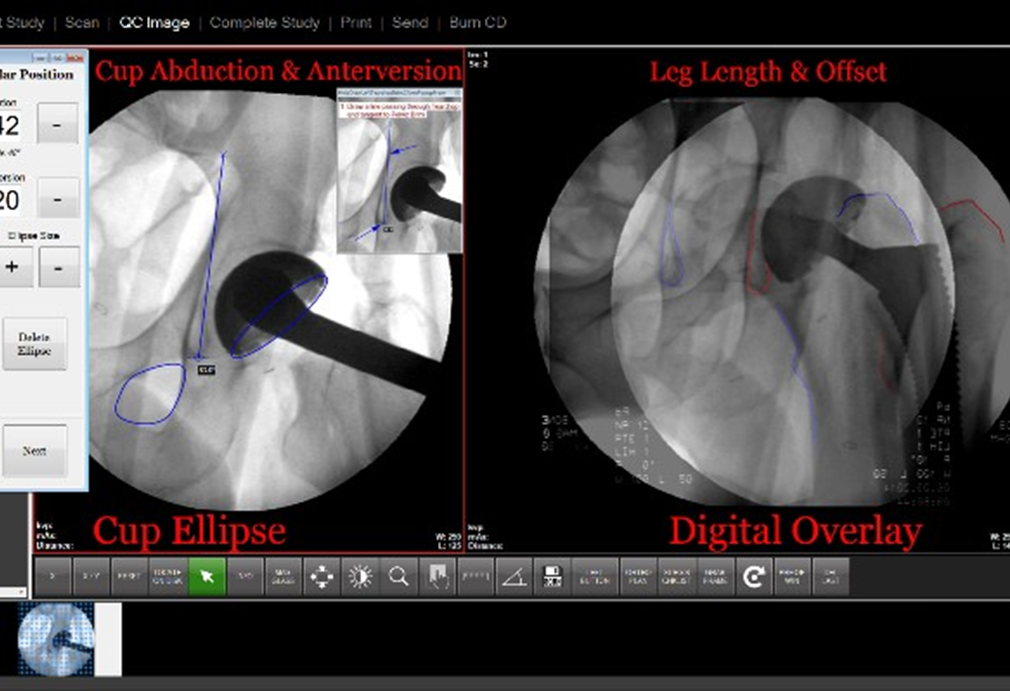
Radlink at RH
•Radlink software allows a live image to be grabbed from the C-Arm or portable monitor and shown on the Radlink monitor.
• The doctor or equipment rep can perform different manipulations to the image on the Radlink monitor.
•Examples: road mapping, sizing
•Always ordered as No Dictation with Radlink order
•Dr. Slotkin, Dr. Longenecker, and Dr. McAlpine are the doctors who may use this equipment
Radlink looks like:
Hana Table

Acetabular reaming

Acetabular implantation
Final Fit

Hip nailing
Open reduction internal Fixation (ORIF) of a fractured proximal femur
An Orthopedic surgeon uses x-ray to guide the wire into the femur
The hardware might end up in the proximal femur (nailing) or extend down to the knee, rodding
Patient may be placed supine with legs crossed, supine with the unaffected leg frogged, or in a lateral position lying on the unaffected side
Hip nailing
A bag is usually placed over the C-arm tube (bottom) due to the high level of vascularity of these cases
Hip nailing
The C-Arm approaches from the unaffected side
sterile team on the affected side
Ensure Black Diamond video cord is plugged in and C-athe rm images are on the room monitor for the surgeon
C-arm responsibilities
Center and position the C-arm appropriately over patients affected hip
save images
Femur rodding
very vascular just like hip nailing,
femur rodding is set up similar to?
Hip nialing
Femur rodding the screws are
screws to insert into rod must be imaged laterally to form perfect circles
Femur rodding responsibilities
tech responsibility to make sure the circle is perfect and adjust the C-arn uf not
Save and send Ap and lateral images
Orthopedics extremities
•Surgical repair of any extremity with fluoro guidance
•Open or closed repair
Orthopedic extremities C arm
•C-Arm and monitor position vary with each body part and surgeon preference
•Technologist and OR staff must communicate to allow C-Arm placement without interrupting sterile fields.
•Technologist Responsibilities:
•Arrange equipment based upon body part and physician preference
•
•Maintain AP and lateral images on the C-Arm monitor
•Communicate with OR staff to maintain the sterile field
•
•Save images and send to PACS
External fixation
Screws are placed into the bone above and below the fracture, and a device is attached to the screws from outside the skin, where it may be adjusted to realign the bone
on the patient for 4-10 months
Spinal surgeries
Fusion
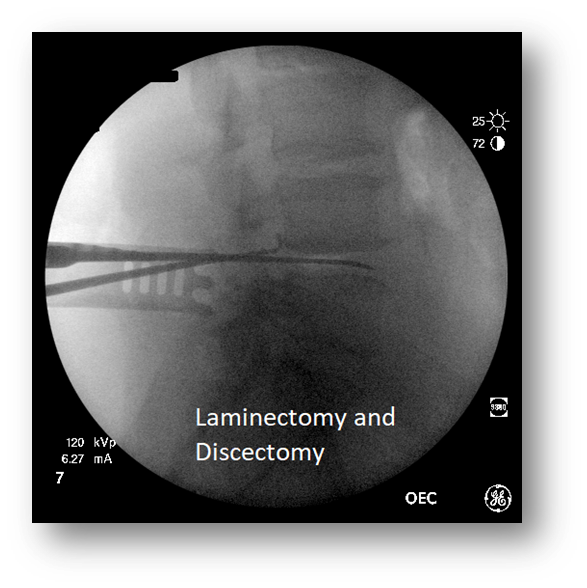
Discectomy
Laminectomy
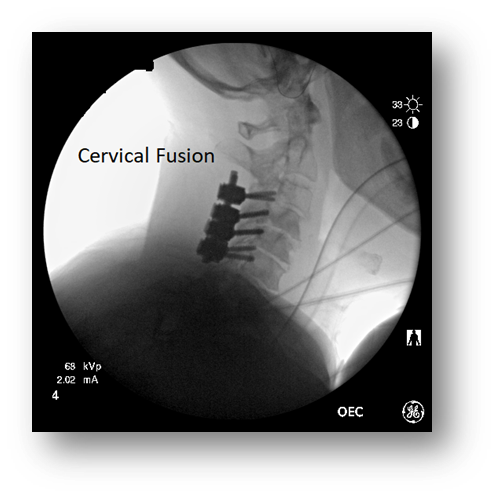
Fusion sp[inal surgery
•Permanent fixation of 2 or more vertebrae using metal screws and rods
•Takes away some flexibility but may stop the progress of deterioration, such as scoliosis
Discectomy spinal surgery
•: Removal of a portion of a herniated disc or complete disc removal during a spinal fusion
•Herniated discs can irritate surrounding nerve branches and cause severe lower extremity pain
•The disc is replaced by a “cage” during fusions
Laminectomy spinal surgery
•Surgical operation to remove the back of one or more vertebrae, usually to give access to the spinal cord or to relieve pressure on nerves
Spinal surgery
•Cervical surgery is usually done with the patient laying supine
•Thoracic and lumbar surgery is done with the patient laying prone
•Either a C-Arm or portable machine can be used
•Based on surgeon preference
mostly in lateral images
C- Arm for Spinal Surgery
•Most surgeons will take preliminary images prior to draping the patient to help position equipment
•AP/ PA images should be marked with L or R
•The tube should be perpendicular to the patient’s spine to ensure true lateral image
•Tech may need to angle C-Arm to open spaces
Vascular studies (Arteriograms)
•Use injections of contrast under fluoro to evaluate blood vessels for strictures or ruptures
•Intra-operative Arteriograms
•Venous bypasses in extremities
•Aortic stent placement for abdominal aneurysms
Vascular studies (Subtraction)
•Removal all bone or other artifacts from an image for better visualization of contrast-filled vessels
For spinal surgery patient is positioned how?
curved to aid in straightening out disc spaces
Spinal surgery
Cervical Fusion
Vascular studies Road mapping
•A type of imaging in which contrast is injected ONCE, but the image of that contrast is superimposed over subsequent images that are not contrast injected resulting in less radiation exposure and contrast use
Vascular Studies (Arteriograms)
•Technologist Responsibilities:
•Must be proficient in the vascular capabilities of a C-Arm
•Subtraction; roadmapping; cine runs
•Ensure the C-Arm does not move once it is centered over the area of interest – use your brake!
•Provide proper lead protection for all present OR staff
•Vascular studies are among the highest in fluoro times
•Be prepared to mark anatomy and make annotations on images