Disease Detectives BIG IDEAS + EQUATIONS
5.0(1)
Studied by 18 peopleCard Sorting
1/38
Earn XP
Description and Tags
Last updated 9:12 PM on 2/2/23
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
1
New cards
Classical Epidemiology
studies origins of health problems
2
New cards
Clinical Epidemiology
study patients in health care settings in order to improve the diagnosis and treatment
3
New cards
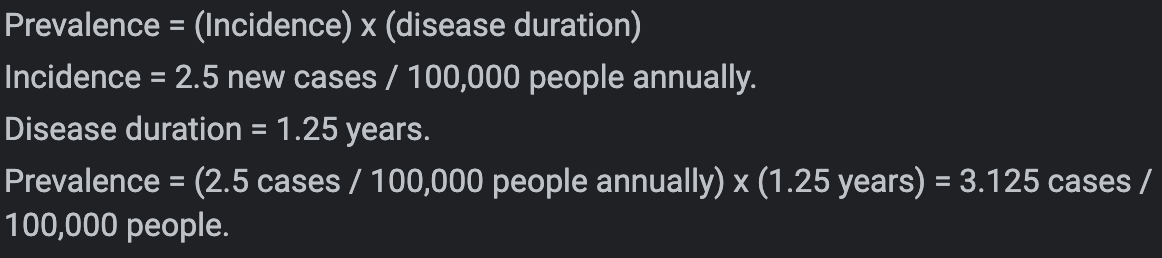
Incidence
\# of new instances of disease in a population over a given time period
\
Measures rapidity of disease occurrence
\
X cases / Y population / Z time
\
Time = the duration of the illness or condition
\
Measures rapidity of disease occurrence
\
X cases / Y population / Z time
\
Time = the duration of the illness or condition
4
New cards
Prevalence
\# of affected persons in the population at any given point in time
\
Measures the proportion of the population with disease \n \n X cases / Y population
\
Measures the proportion of the population with disease \n \n X cases / Y population
5
New cards
Point Prevalence
snapshot of the population + its rate of a certain disease at a point in time
6
New cards
Period Prevalence
tracks the prevalence over a certain duration
7
New cards
13 Steps to Investigate Outbreak
1. Prepare for field work - Research and Supplies, Official Arrangements, Safety Protocols, and Contacts
\
1. Establish the Existence of an Outbreak - Consider Severity, Potential for Spread, Public Concern, and Availability of Resources
\
1. Verify the Diagnosis - Verify Procedures and Eliminate Experimental Error (and Other Errors/Biases, for That Matter)
\
1. Construct a Working Case Definition
\
1. Find Cases Systematically and Record Information - Time: Tables, Epi Curves; Place: Geographical Extent of Disease & Spot Map; Identify By Demographic Information or Exposures to Risk Factor
\
1. Describe and Orient the Data in Terms of **Person, Place, and Time** - Descriptive Epidemiology
\
1. Develop Hypotheses (Agent/Host/Environment Triad) = Chain of Transmission
\
1. Evaluate Hypotheses - Analytical Studies (MUST Have a Control Group)
\
1. Refine Hypotheses if Necessary
\
1. Compare and Reconcile with Laboratory and/or Environmental Studies
\
1. Implement Control and Prevention Measures (ASAP!)
\
1. Initiate or Maintain Surveillance - Monitor Implementation: Track New Cases, Check the Outbreak’s Spread Outside Targeted Area, Control and Change if Needed
\
1. Communicate Findings - Reports, To Important People and Public
8
New cards
5 Steps for Surveillance
1. Identify, define, and measure the health problem of interest
\
1. Collect and compile data about the problem (and if possible, factors that influence it)
\
1. Analyze and interpret these data
\
1. Provide these data and their interpretation to those responsible for controlling the health problem
\
1. Monitor and periodically evaluate the usefulness and quality of surveillance to improve it for future use. (Surveillance of a problem often does not include actions to control the problem
9
New cards
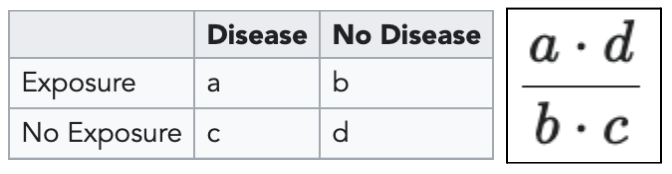
Odds Ratio
the odds of an event in an experimental group relative to that in a control group
10
New cards
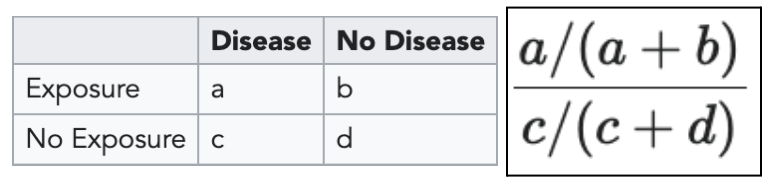
Relative Risk
ratio of risk of an event in one group (e.g., exposed group) versus the risk of the event in the other group (e.g., nonexposed group)
11
New cards
Attack Rate
rate that a group experienced an outcome or illness equal to the number sick divided by the total in that group
\
For exposed: a/(a+b) → should be HIGH
For unexposed: c/(c+d) → should be LOW
\
For exposed: a/(a+b) → should be HIGH
For unexposed: c/(c+d) → should be LOW

12
New cards
Chi-Square
used to determine the statistical significance of the *difference* indicated by the relative risk or odds ratio; compares your observed values (a, b, c, and d) with the *expected* values for those same groups
\
Expected Value: \[ (a+b)(b+c) \] / (a+b+c+d)
\
Expected Value: \[ (a+b)(b+c) \] / (a+b+c+d)
![used to determine the statistical significance of the *difference* indicated by the relative risk or odds ratio; compares your observed values (a, b, c, and d) with the *expected* values for those same groups
\
Expected Value: \[ (a+b)(b+c) \] / (a+b+c+d)](https://knowt-user-attachments.s3.amazonaws.com/0fbde2c2d102499394777907f1387382.jpeg)
13
New cards
P-value
the measure of how confident you are that your findings are NOT due to chance
\
If P-value is LESS than alpha (0.05 or 5%), the data is significant
\
ex) P-value of 0.01 → 10% chance your results were a result of random fluctuations
\
If P-value is LESS than alpha (0.05 or 5%), the data is significant
\
ex) P-value of 0.01 → 10% chance your results were a result of random fluctuations
14
New cards
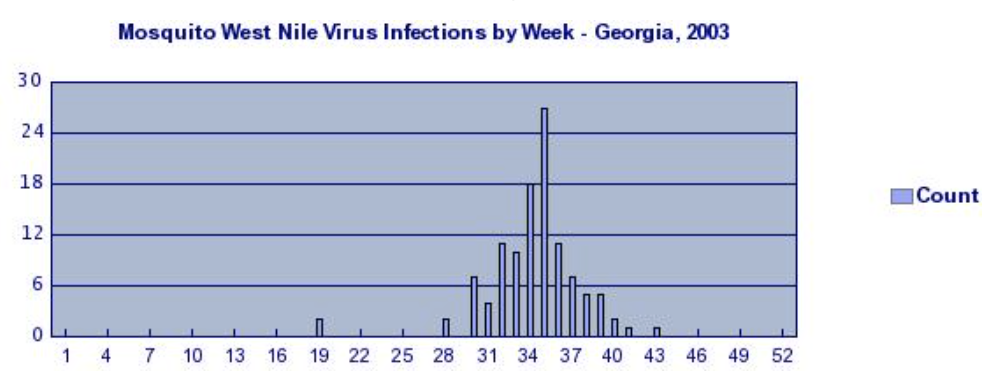
Epi-Curves
a histogram (graph consisting rectangles) that shows the course of an outbreak by plotting the number of cases of a condition according to the time of onset
15
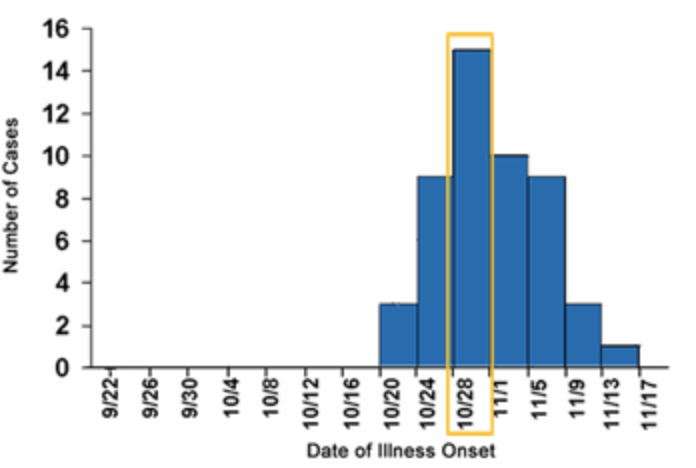
New cards
Point Source
persons are exposed over a brief time to the same source, such as a single meal or an event
\
Shape of curve (commonly) RISES RAPIDLY + contains a definite peak, followed by a gradual decline
\
Shape of curve (commonly) RISES RAPIDLY + contains a definite peak, followed by a gradual decline
16
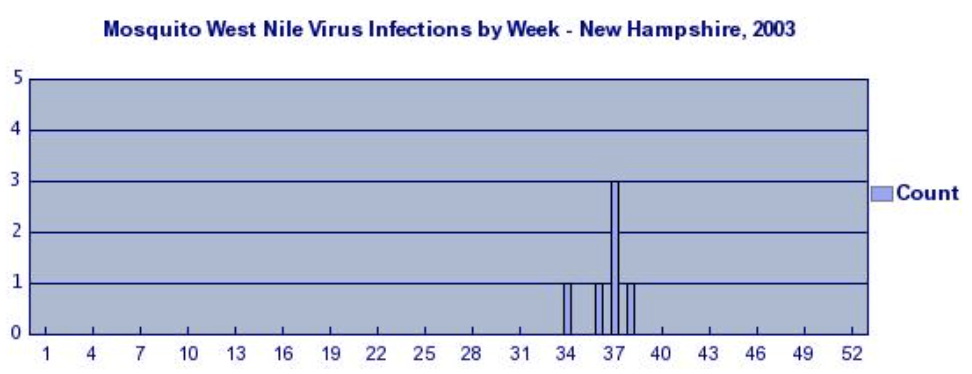
New cards
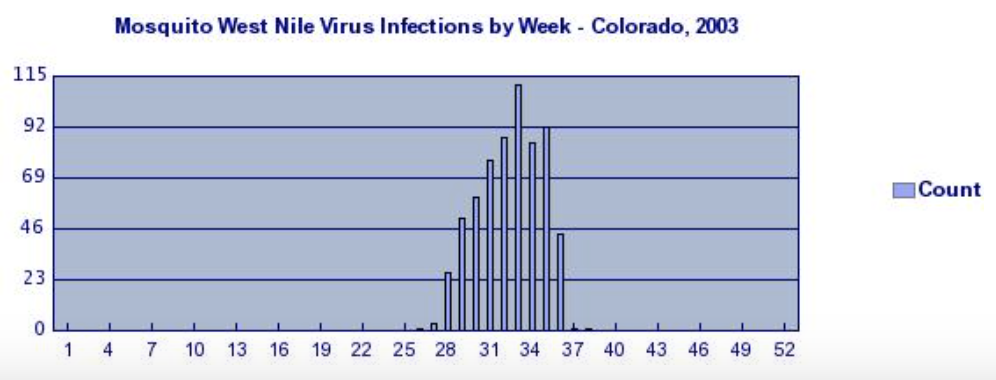
Continuous Common Source
when persons are exposed to the same source but exposure is prolonged over a period of days, weeks, or longer
\
\*the down slops of the curve may be very SHARPif common source is removed or gradual if the outbreak is allowed to exhaust itself
\
\*the down slops of the curve may be very SHARPif common source is removed or gradual if the outbreak is allowed to exhaust itself
17
New cards
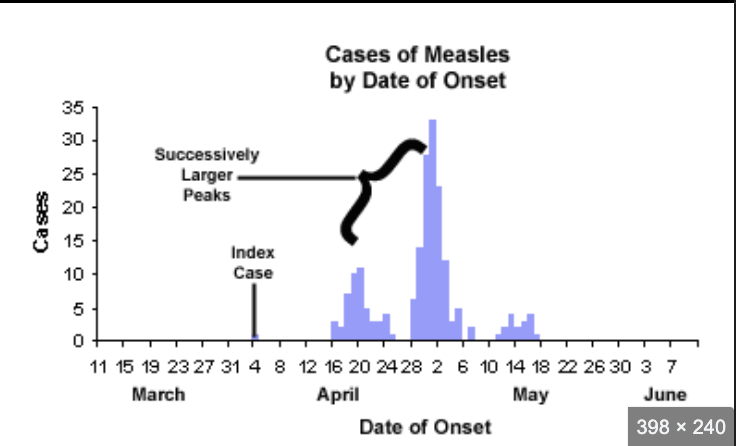
Propagated (Progressive Source)
when one or more of the first wave of cases serves as a source of infection for subsequent cases and those subsequent cases, in turn, serve as sources for later cases
\
SHAPE: curve usually contains a series of successively larger peaks (reflects increasing # of cases caused by person-to-person contact)
\
distance between peaks may be rough indication of the incubation period of the disease
\
As outbreak progresses, peak flattens out
\
SHAPE: curve usually contains a series of successively larger peaks (reflects increasing # of cases caused by person-to-person contact)
\
distance between peaks may be rough indication of the incubation period of the disease
\
As outbreak progresses, peak flattens out
18
New cards
Random Error
the result of fluctuations around a true value because of sample population; use of invalid outcome. measure that equally misclassifies cases. and. controls
\
can be reduced by: INCREASING sample size + making measurements more precise
\
can be reduced by: INCREASING sample size + making measurements more precise
19
New cards
Precision
measure of random error that is inversely related (INCREASING random error DECREASES precision)
20
New cards
Systematic Error
usually consistent and repeatable and often occurs from flawed equipment or experimental design
21
New cards
Selection Bias
when selection of participants for a study is affected by an unknown variable that is associated with the exposure and outcome being measured
22
New cards
Information Bias
when bias (any systematic error) is introduced though an error in measurement or observation
23
New cards
Confounding bias
results from mixing effects of several factors (deals with causation and NOT variations in study results)
24
New cards
Hill’s Criteria for Causation
nine viewpoints by which to evaluate human epidemiologic evidence to determine if causation can be deduced
\
1. Strength of Association - relationship is clear and risk estimate is high
2. Consistency - observation of association must be repeatable in different populations at different times
3. Specificity - a single cause produces a specific effect
4. Alternative Explanations - consideration of multiple hypotheses before making conclusions about whether an association is causal or not
5. Temporality - cause/exposure must precede the effect/outcome
6. Dose-Response Relationship - an increasing amount of exposure increases the risk
7. Biological Plausibility - the association agrees with currently accepted understanding of biological and pathological processes more exposure = more risk
8. Experimental Evidence - the condition can be altered, either prevented or accelerated, by an appropriate experimental process
9. Coherence - the association should be compatible with existing theory and knowledge, including knowledge of past cases and epidemiological studies
\
1. Strength of Association - relationship is clear and risk estimate is high
2. Consistency - observation of association must be repeatable in different populations at different times
3. Specificity - a single cause produces a specific effect
4. Alternative Explanations - consideration of multiple hypotheses before making conclusions about whether an association is causal or not
5. Temporality - cause/exposure must precede the effect/outcome
6. Dose-Response Relationship - an increasing amount of exposure increases the risk
7. Biological Plausibility - the association agrees with currently accepted understanding of biological and pathological processes more exposure = more risk
8. Experimental Evidence - the condition can be altered, either prevented or accelerated, by an appropriate experimental process
9. Coherence - the association should be compatible with existing theory and knowledge, including knowledge of past cases and epidemiological studies
25
New cards
Infant Mortality Rates
ratio of deaths to births
26
New cards
Sensitivity
the chance of testing positive if you do have the disease

27
New cards
Specificity
the chance of testing negative if you do not have the disease

28
New cards
Attack Rate
total number of new cases / total population
29
New cards
Case Definitions
a set of standard criteria for classifying whether a person has a particular disease, syndrome, or other health condition
\
includes criteria for person, place, time, and clinical features
\
includes criteria for person, place, time, and clinical features
30
New cards
Length Time Bias
overestimation of survival duration due to the relative excess of cases detected that are asymptomatically progressing, while fast progressing cases are detected after giving symptoms
31
New cards
Simpson’s Paradox
Women appeared to be more susceptible (influenced) to an illness than men, but when studies were carried out, men were found to have higher probability of contracting illness
32
New cards
Pigmalion Effect
researchers convey high expectations to subjects; the subjects produce those results
33
New cards
Cross Sectional
a survey, health questionnaire, “snapshot in time”
\
Fastest
Least Expensive
Good for more than 1 Outcome
\
Fastest
Least Expensive
Good for more than 1 Outcome
34
New cards
35
New cards
36
New cards
37
New cards
38
New cards
39
New cards