Physiology Lecture #4 Neuromuscular System: Strength & Endurance
1/60
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
61 Terms
What is exercise?
Adaptation → stimulus on the body and seeing how body changes/adapts to it
What are the 7 training principles that optimize adaptation?
FITT(E) variables: Frequency Intensity Time Type (Enjoyment)
Overload
Periodization
Reversibility
Individuality
Progressive Overload
Specificity
FITT(E) variables
Frequency Intensity Time Type (Enjoyment)
How often, how much, how long, which specific exercise
Overload
demand must be greater than levels encountered during ADL’s for training effects to occur
Periodization
gradual cycling of specificity, intensity, and volume of training to achieve peak levels of fitness
Start: high volume, low intensity
Progress: low volume, high intensity
Reversibility
Training programs must include a maintenance plan to ensure gains from training are not lost
Individuality
consider specific needs & abilities of the patient
Progressive overload
training stimulus must be progressively increased as the body adapts
Specificity and variables to consider
Training effect is limited to the muscles or muscle groups involved in the activity
Variables to consider:
muscles involved
recruited fiber types
principle energy systems (anaerobic vs. aerobic)
contraction type
contraction velocity & type of activity
order of exercises
progression of exercises
rest intervals
Muscular endurance
ability to perform repeated muscle contractions or to sustain a contraction over time
Cardiorespiratory endurance
the entire body’s ability to sustain prolonged, dynamic exercise using large muscle groups
Strength
maximal force a muscle group can generate
Anaerobic systems
ATP-PCr
Anaerobic glycolytic system
Aerobic system
Oxidative system
What system do you use for short sprints with higher intensity and shorter duration (<15 sec)?
ATP PCr system
What system do you use for longer sprints with middle distance (15 sec to 2 min)?
Glycolytic system
What system do you use for longer distance, lower intensity, longer duration (>3 min)?
Oxidative system
What part of the heart hypertrophies with training?
Left ventricle: more efficient pumps → pumps less often because more blood with each pump
What are some cardiovascular changes/adaptation to aerobic endurance training?
Blood flow to active muscles is increased due to increased:
capillarization
capillary recruitment
blood volume
left ventricular size/strength
stroke volume/contractility
Blood pressure + HR at rest & during submaximal exercise is reduced
Describe the make up of Type I mf
red muscle
high # of mitochondria
Describe the make up of Type IIa mf
mixed muscle
medial # of mitochondria
glycolytic
Describe the make up of type IIx mf
white muscle
low # of mitochondria
Therefore doesn’t really use oxygen
Can you change one muscle type to another?
Yes, you can change fiber type IIx to IIa, but you can’t really go from IIa to IIx
Type I fiber type (chart)
slow-twitch fibers
oxidative
high # of oxidative enzymes + mitochondria
high fatigue resistance
low specific tension
slow shortening velocity
high efficiency
Type IIa fiber type (chart)
intermediate fibers
fast oxidative glycolytic
moderate # of oxidative enzymes
moderate fatigue resistance
high specific tension
intermediate shortening velocity
moderate efficiency
Type IIx fiber type (chart)
fast-twitch fibers
fast- glycolytic
small # of oxidative enzymes
high # of glycolytic enzymes
low fatigue resistance
higher specific tension
fast shortening velocity
low efficiency
How do muscle fibers adapt to aerobic endurance training?
increased size of type I fibers
transition of type IIx → type IIa
transition of type II → type I
increased # of capillaries per mf & in a given cross-sectional area of muscle to help with oxygen delivery for aerobic metabolism
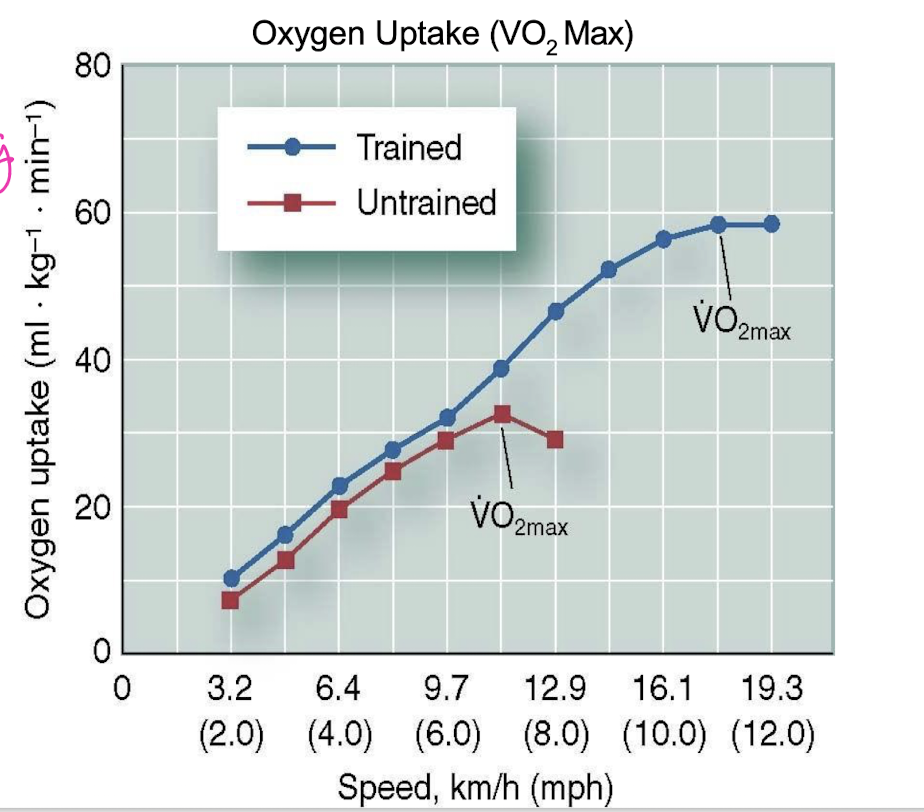
Effects of aerobic exercise on metabolism (graph)
O2 uptake improves with training → you plateau instead of dropping off
Metabolic adaptations to aerobic endurance training
Increased:
oxidative enzymes
# of mitochondria
VO2 max/ oxygen uptake
ATP generating capacity
Lactate threshold increases due to:
increased clearance of lactate & hydrogen ion
decreased production of lactate
increased efficiency of aerobic metabolism
Maximal oxygen uptake (VO2 max)
indicator of cardiorespiratory endurance & aerobic fitness
normal active untrained college students = 38-42 ml/kg/min
What are the contributing factors of oxidative capacity?
# of mitochondria
fiber type composition
oxidative enzyme activity w/in muscle
endurance training
age: after age 25-30, decrease ~1% per year
What systems benefit from aerobic training?
ATP-PCr
Glycolytic
Energy system adaptations to anaerobic training
increased ATP-PCr system enzyme activity
increased activity of key glycolytic enzymes
no effect on oxidative enzyme activity
no increase in capillary density (O2)
no effect on VO2 max
Metabolic system adaptations to anaerobic training
Increased:
anaerobic metabolic function
short term, high intensity capacity
acid base imbalance tolerance (can handle lactic acid better)
ATP-PCr and glycolytic enzymes
Neuromuscular adaptations to anaerobic training
Increased:
# of motor units recruited w/ improved synchronicity → improved force
efficiency with reduced coactivation of agonist & antagonist muscles
mf recruitment
cross-education
Decreased:
inhibitory mechanisms (golgi tendon organs, antagonists)
Adaptations to resistance training
increased strength & power
neural mechanisms leading to strength gains:
increased frequency of stimulation, # of mu’s, synchronicity of recruitment
Rate coding
Explains how the intensity of a stimulus impacts the rate in which it stimulates the muscle
More intense stimulus = more frequent contraction = more force + power
Force production increases with:
Increased:
recruitment of mu’s
frequency of stimulus
type II recruitment (more force + mf’s)
Larger vs. smaller muscle groups (glute max vs. med)
What are the 3 rules of adaptions with resistance training?
neural adaptations are always first and accompany strength gains
transient (acute) muscle hypertrophy results from edema
chronic muscle hypertrophy reflect actual structural changes in the muscle (increased size of individual mf’s)
When do you see neural activation and fiber hypertrophy?
first 6 weeks = MU recruitment & Co-activation
early gains in strength are more influenced by neural factors
10-16 weeks:
long-term strength increases due to mf hypertrophy
Transient (acute) hypertrophy
Increase in muscle size that immediately follows a single exercise bout
fluid accumulation in interstitial & intracellular space from blood plasma
Chronic hypertrophy
Increase in muscle size after long-term resistance training
facilitated by post exercise nutrition
net increase in actin & myosin synthesis
changes in mf size
Types of resistance training
static contraction (isometric)
free weights
eccentric training
isokinetic training
variable resistance (theraband)
plyometrics (explosive movements)
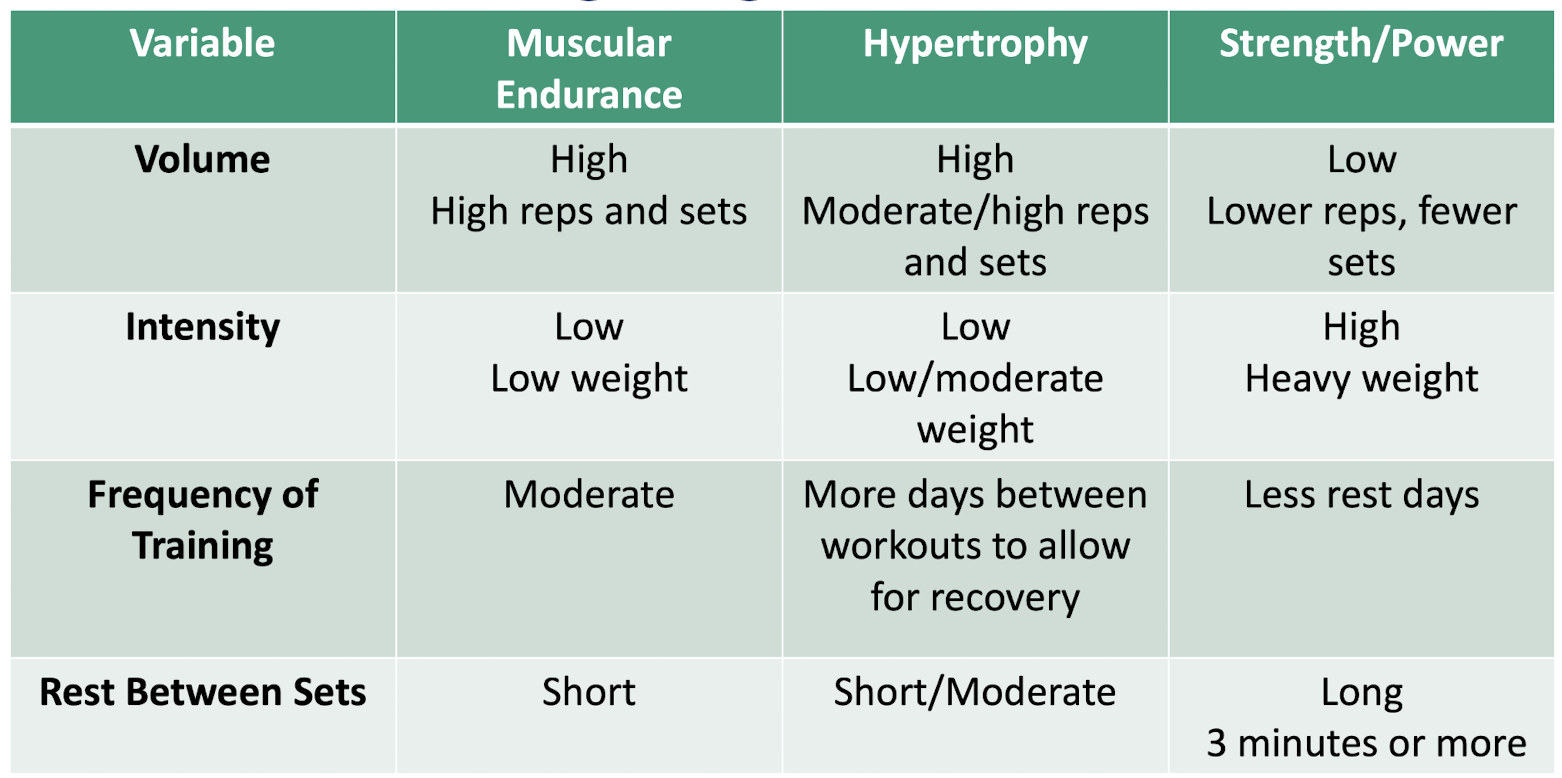
What do you do when you want to enhance strength development?
low-repetition, high resistance
What do you do when you want to optimize muscular endurance?
high reps, low resistance
Resistance training programs chart: volume, intensity, frequency, rest
Acute muscle soreness
accumulation of end products (H+) of exercise in the muscles or edema
usually disappears minutes or house after exercise
Delayed onset muscle soreness (DOMS)
Soreness is felt 12-48 hours after strenuous bout of exercise
primarily from eccentric muscle activity
more muscle breakdown than protein synthesis
Prevention:
initial training at lower intensity w/ gradual increases
reduce eccentric component during early training
Isometric measurement of strength
Hold contractions 3-5 seconds
advantage: simple, only 1 point tested
disadvantage: most activities are dynamic (full ROM
Free weight measurement of strength
1 Rep Max:
isotonic measurement
max weight an individual can lift at once
Methods: free weight & adjustable resistance machine
Advantage: low cost, dynamic
Disadvantage: risk of injury as weight increases
Isokinetic measurement of strength
maintains constant speed w/ varying resistance through ROM
Advantage: provides feedback on differences in force through ROM
disadvantage: lots of money + time
Variable resistance measurement of strength
resistance changes through ROM in conjunction w/ change in joint angles
eliminates joint mechanical advantages & inertial effect
Advantage: maximizes muscle force through full ROM
Disadvantage: uniformity b/t trials, time
Clinical measure of exercise intensity: VO2 max
highest rate of O2 consumption attainable during max exercise
can be improved with endurance training
Clinical measure of exercise intensity: talk test
Light intensity: should be able to sing during activity
Moderate: can carry conversation
Vigorous: winded or too out of breath to hold conversation
Clinical measure of exercise intensity: Target heart rate
Based on max heart rate
220 - age = HR max
HR max x 0.6 = target HR
verify by taking pulse
Clinical measure of exercise intensity: Rating of perceived exertion
subjective measurement that can be used to determine intensity of aerobic workout
Determined by:
cue of increased rate of breathing
ask if patient senses their HR is faster
ask how hard does it feel like you’re working?
Want to workout b/t 12-16 (50-85% HR max)

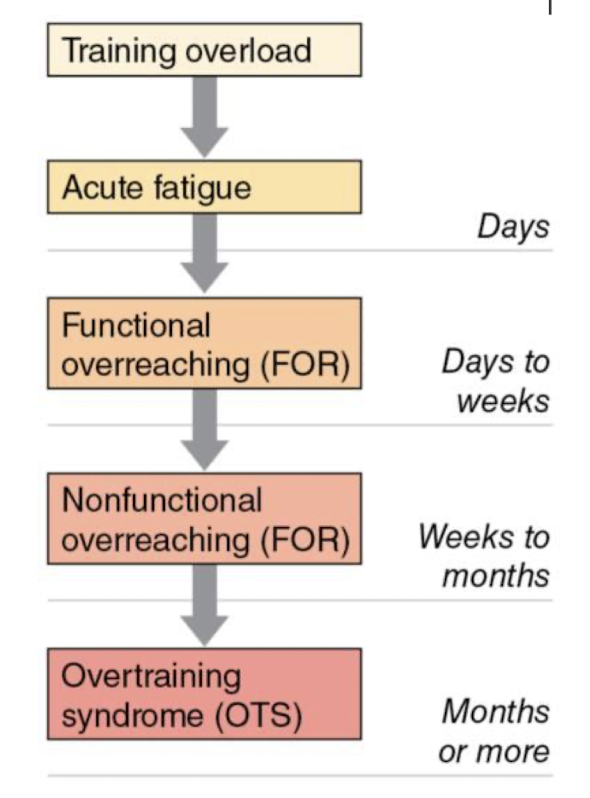
Overtraining
Excessive overload w/ inadequate recover → accumulated training stress
signs & symptoms:
extreme fatigue, illness, injury, hormone disturbance
Long-term performance losses
Detraining
loss of accumulated physiological adaptations with reduction in frequency, volume, and intensity of training
if you don’t use it, you lose it
Magnitude depends on length of detraining period & initial status
quicker gains with return to training → muscle memory
Muscle atrophy
inactive muscle with injury, immobilization or cessation of training
transition of type IIx → type IIa
decreased strength, protein synthesis, cross-sectional area
muscles can recover when activity is resumed