PT 712 - Week 1
1/106
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
107 Terms
CN I name
olfactory
CN I - olfactory - primary function
smell
CN II name
optic
CN II - optic - primary function
vision
CN III name
oculomotor
CN III - oculomotor - primary fuction
- upward
- medial
- downward
- up and in
CN IV name
trochlear
CN IV - trochlear - primary function
down and in
CN V name
trigeminal
CN V - trigeminal - primary function
touch - forehead and cheek
- clench teeth
CN VI name
Abducens
CN VI - Abducens - primary function
- abduction
CN VII name
facial
CN VII - facial - primary function
- taste for anterior 2/3 of tongue
- smile
CN VIII name
vestibulococlear (acoustic)
CN VIII - vestibulocochlear - primary function
- hearing
- equilibrium
CN IX name
glossopharyngeal
CN IX - glossopharyngeal - primary function
- posterior 1/3 of the tongue
- speech
CN X name
vagus
CN X - vagus nerve - primary function
- digestion
- defecation
- slowed HR
CN XI name
spinal accessory
CN XI - spinal accessory - primary function
shoulder shrug
CN XII name
hypoglossal
CN XII - hypoglossal - primary function
- tongue movement
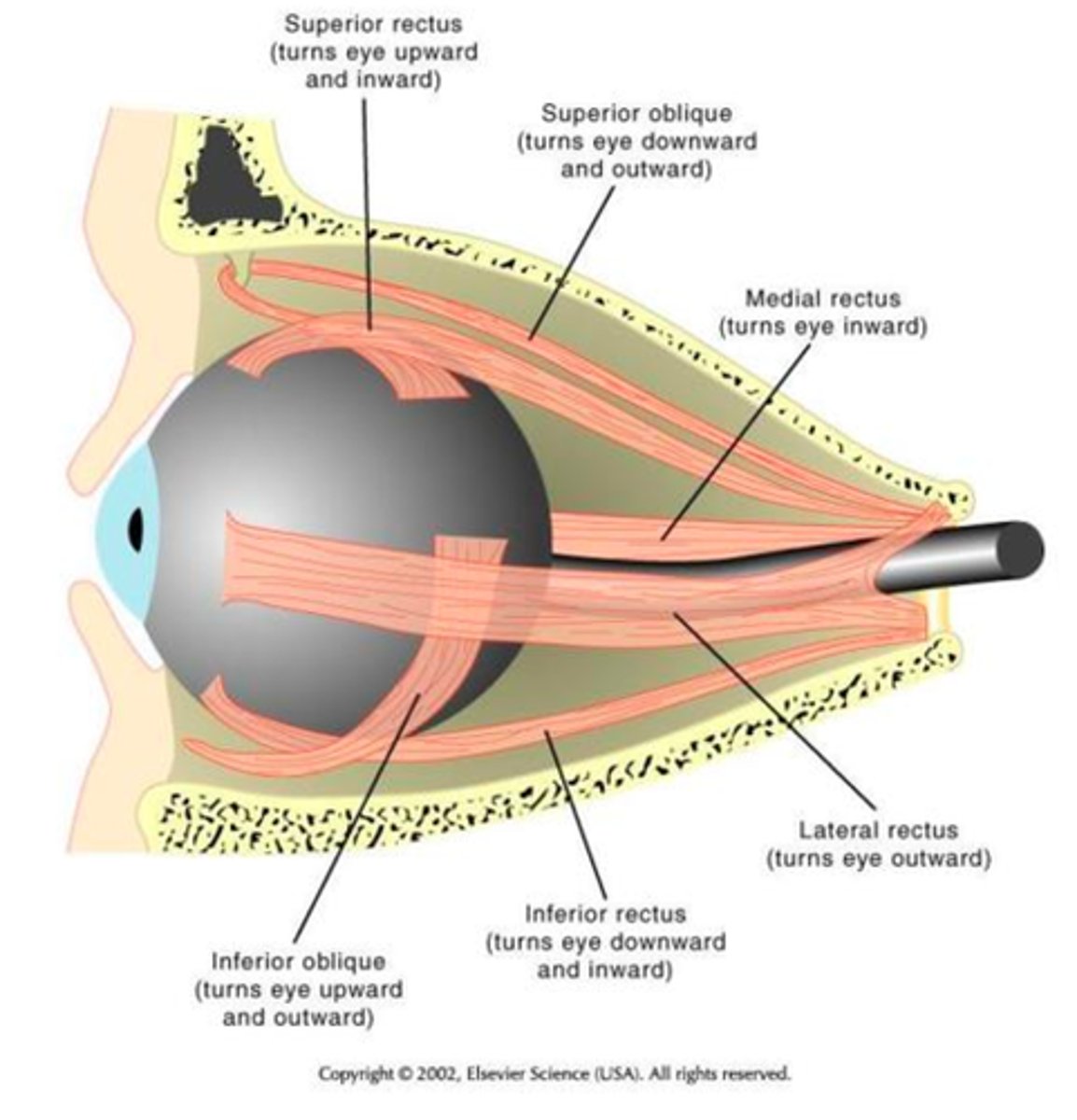
CN III (oculomotor nerve) innervates which eye muscles?
- medial rectus
- superior/inferior recti
- inferior oblique
CN IV (trochlear nerve) innervates which eye muscle?
superior oblique
CN VI (abducens) innervates which eye muscle?
lateral rectus
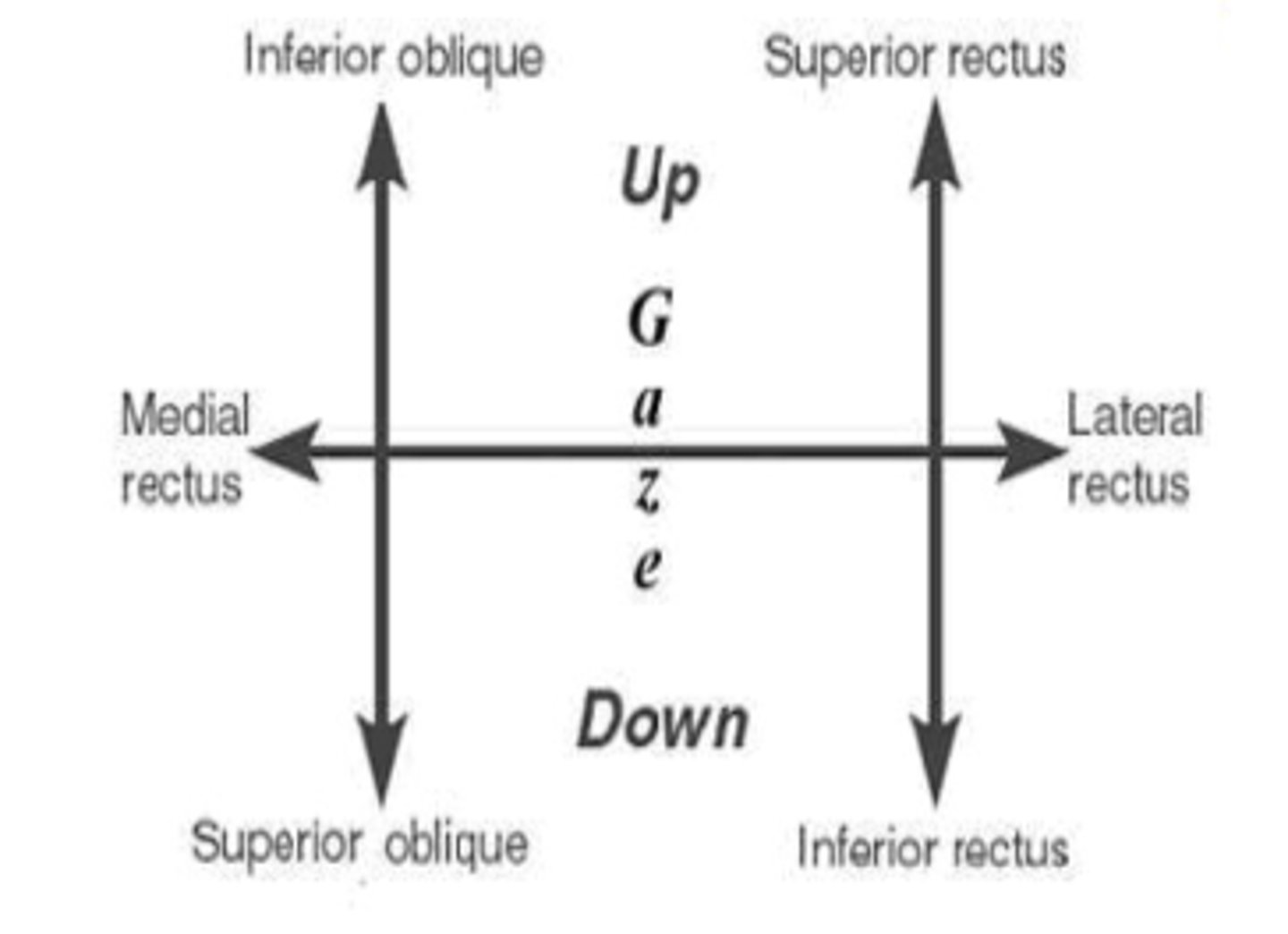
action of the superior rectus
turns eye upward and inward
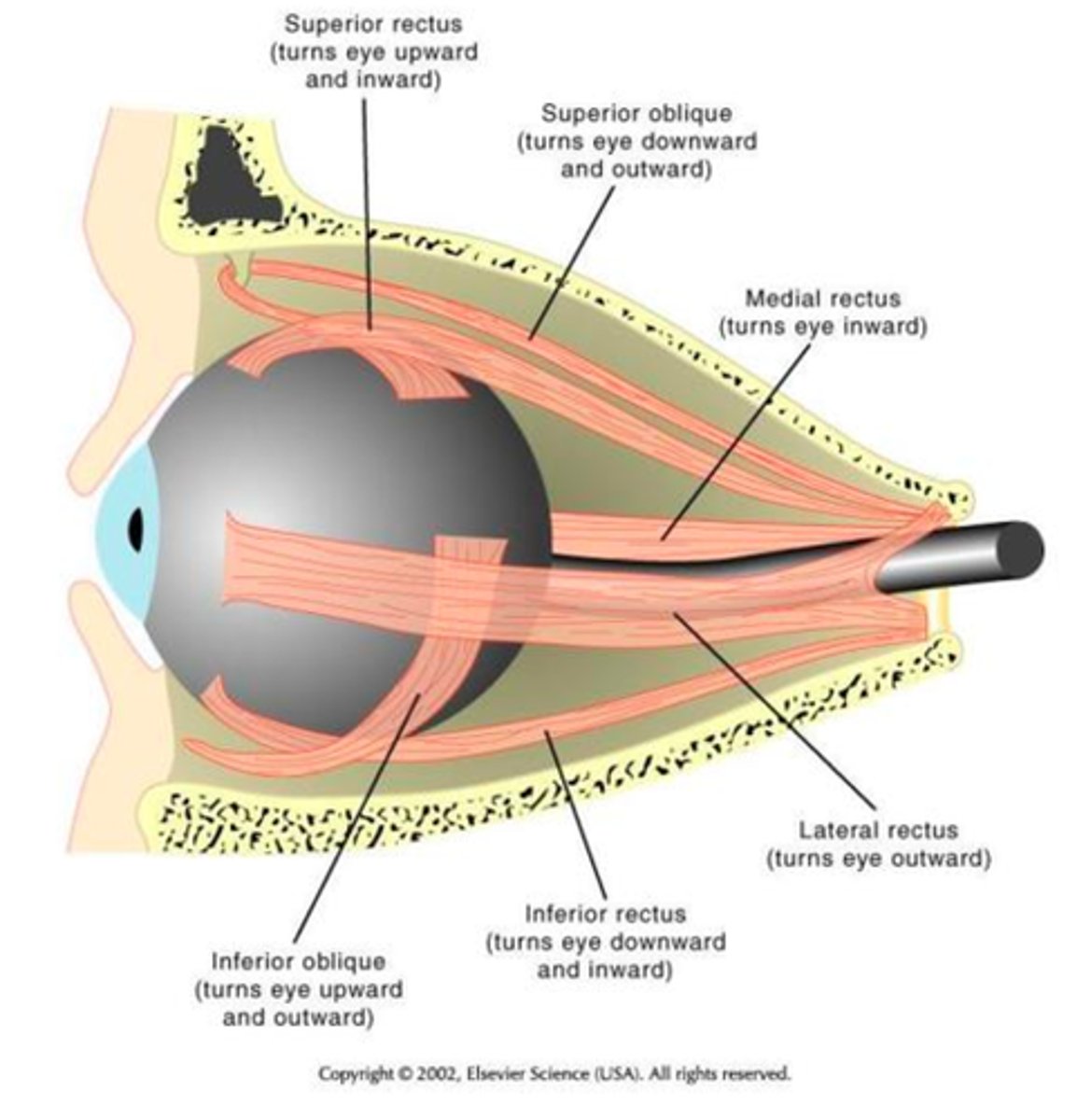
action of the superior oblique
turns eye downward and outward
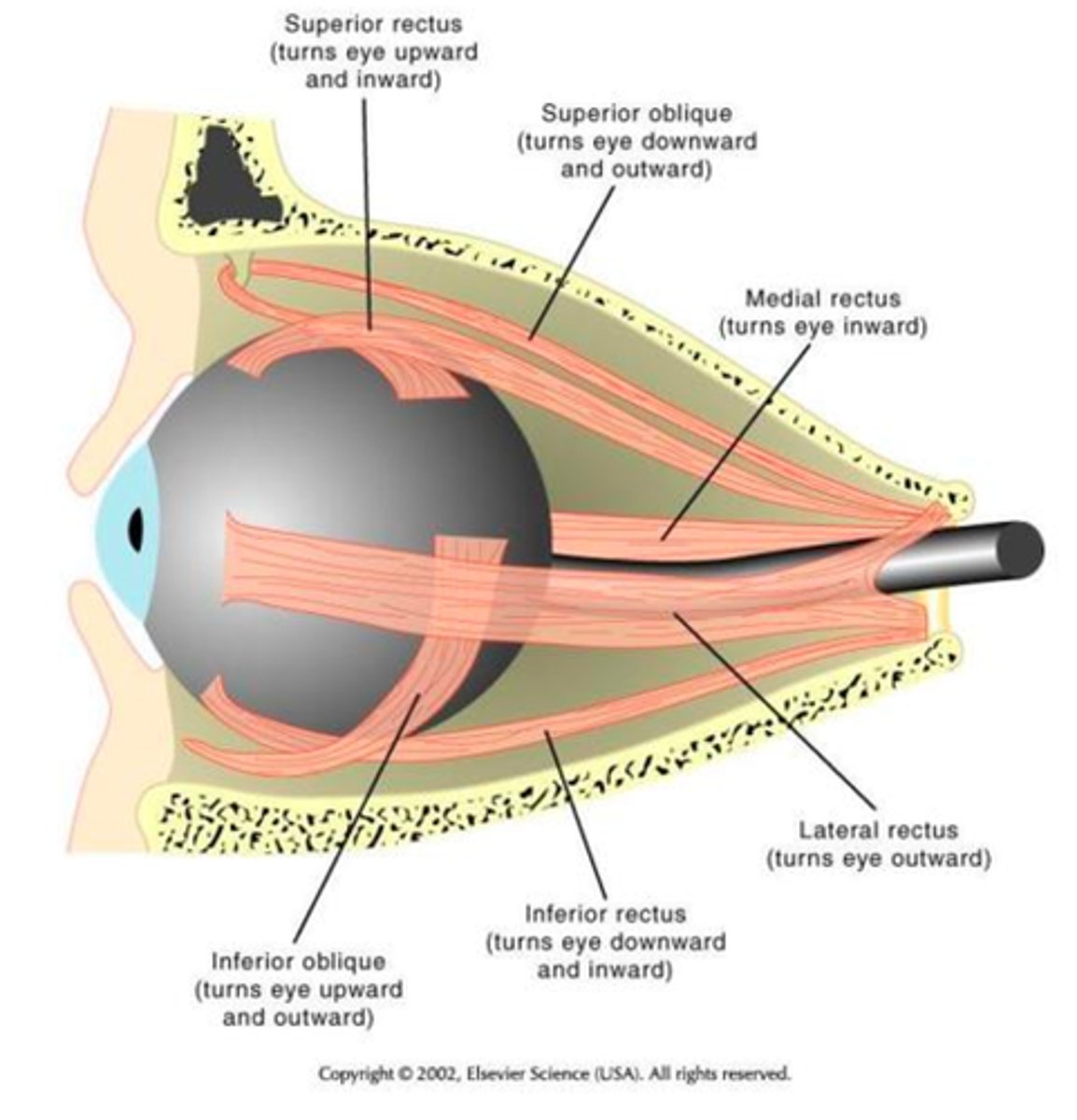
action of the medial rectus
turns eye inward
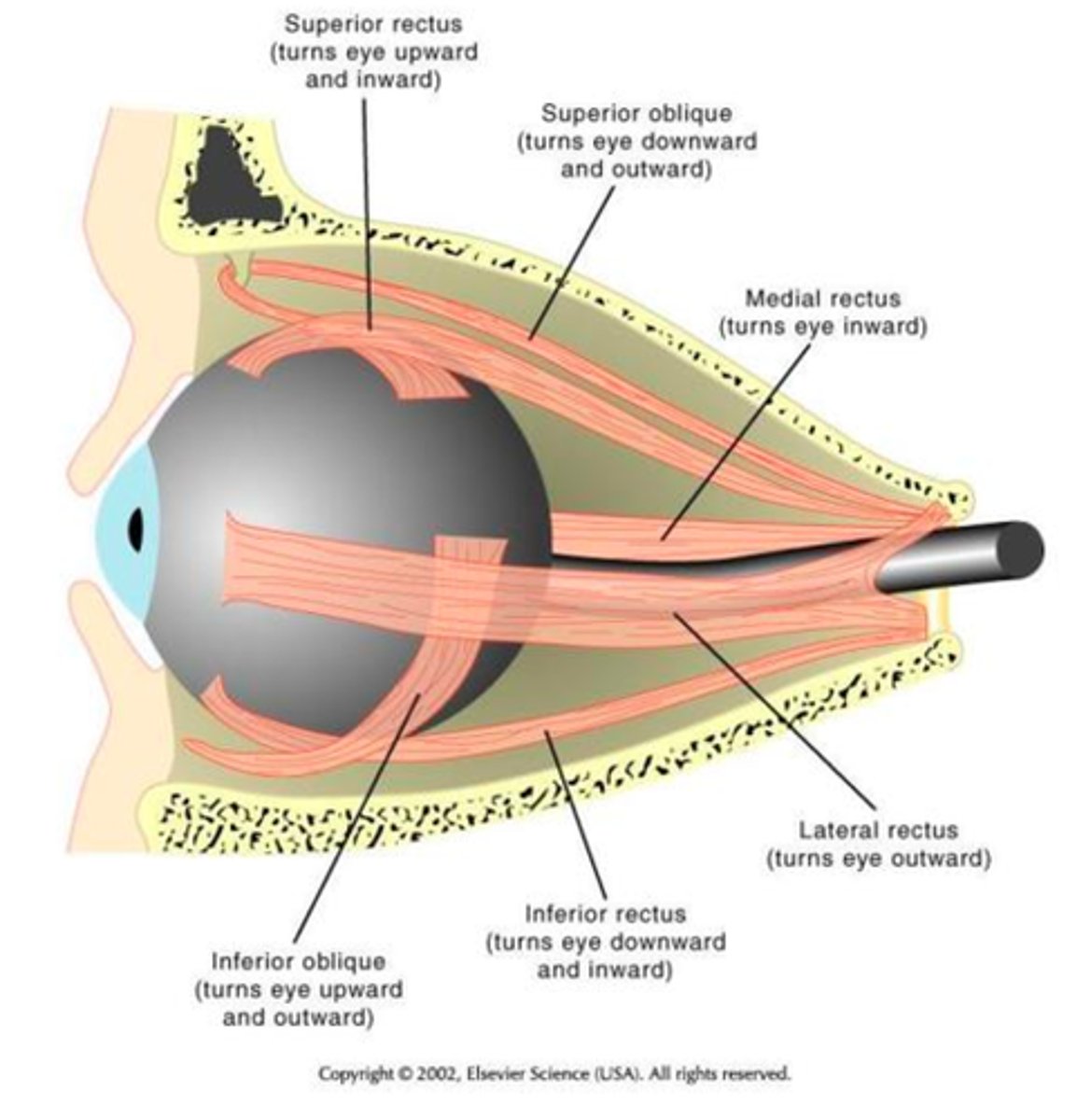
action of the lateral rectus
turns eye outward
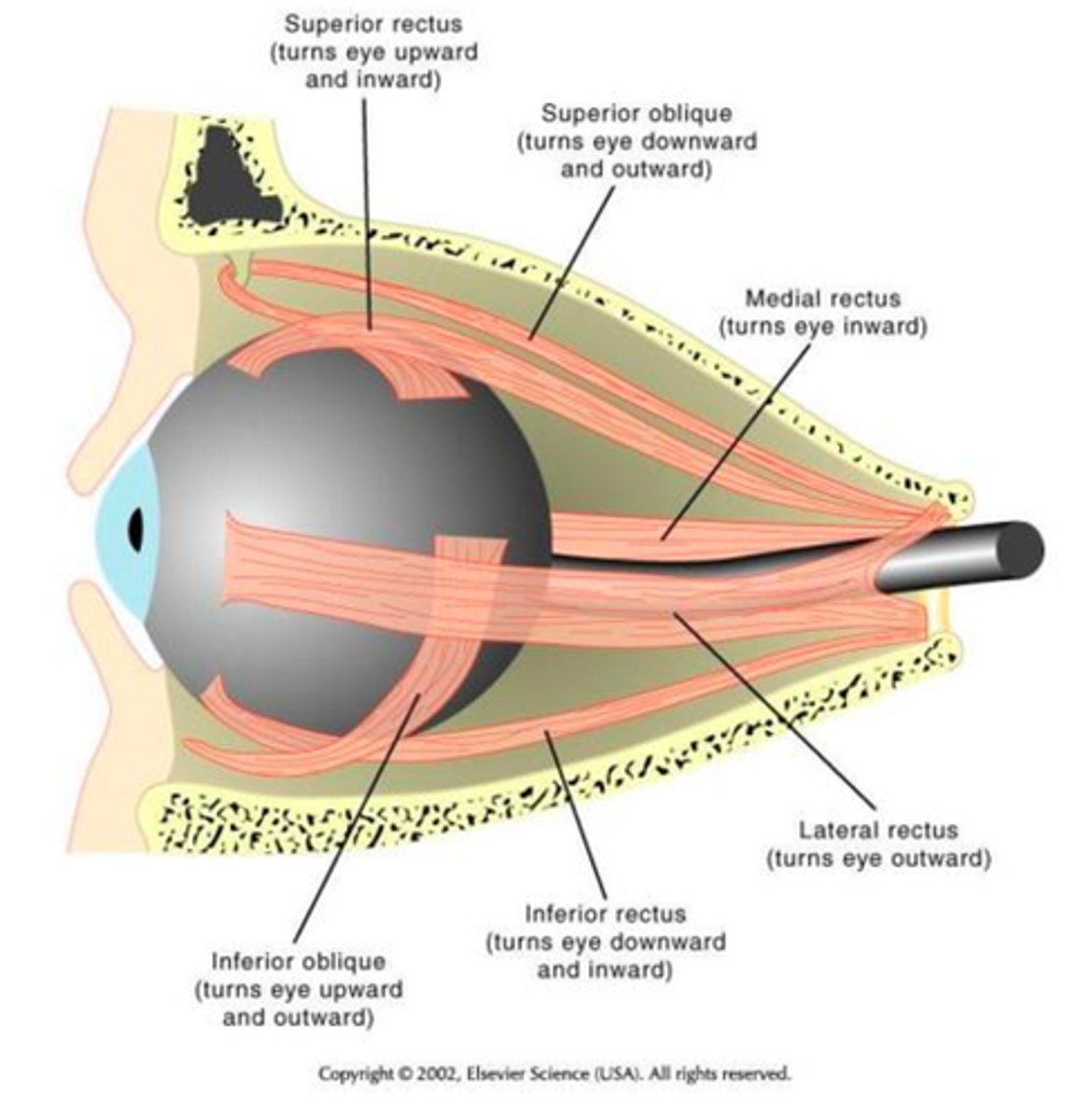
action of the inferior rectus
turns eye downward and inward
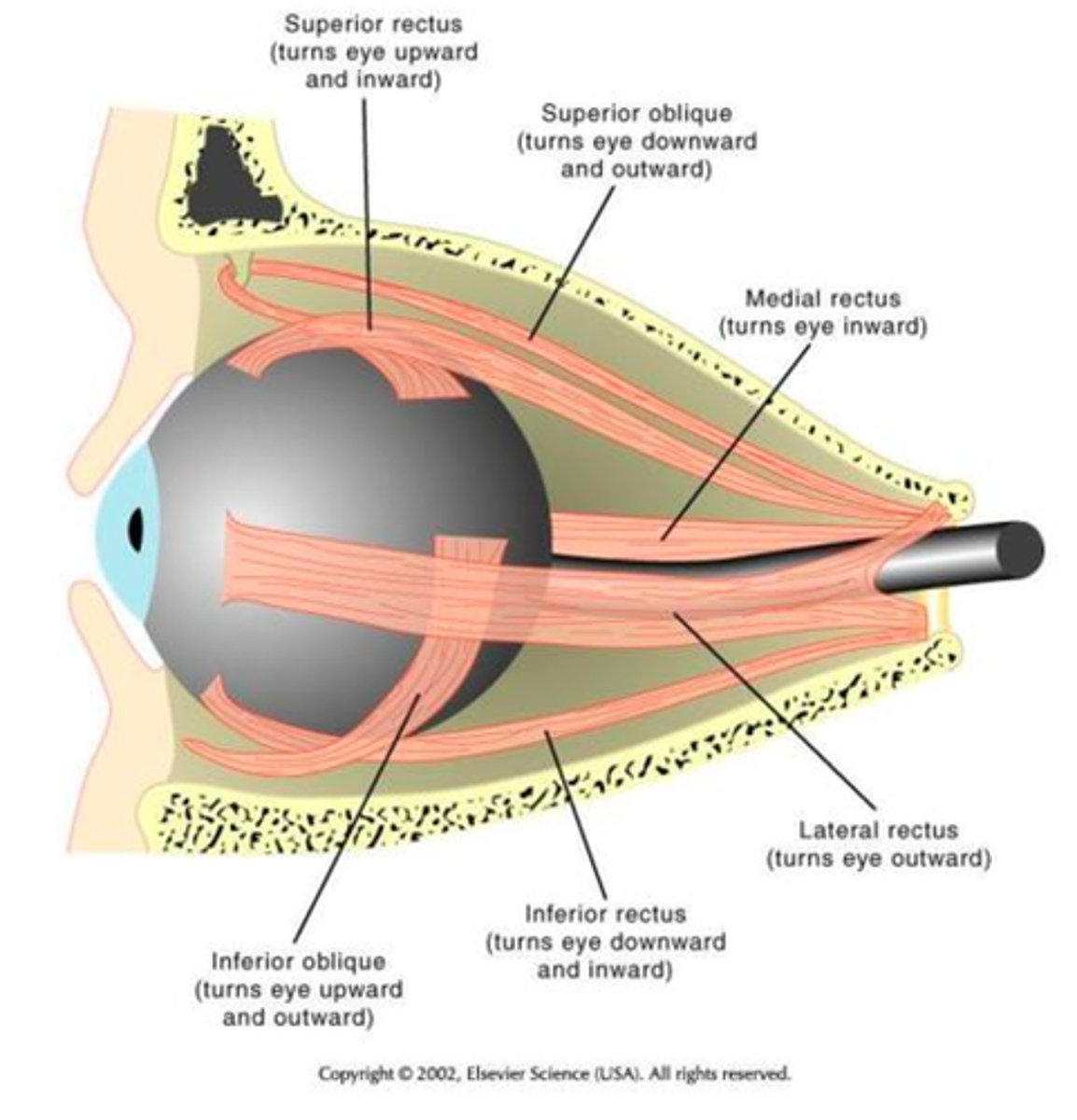
action of the inferior oblique
tuns eye upward and outward
define visual acuity
clarity of vision and is dependent on optical and neural factors
what optical and neural factors does visual acuity depend on?
- sharpness of the retinal focus within the eye
- health and functioning of the retina
- sensitivity and interpretative faculty of the brain
Which cranial nerve function is visual perception?
CN II (optic nerve)
Which cranial nerves are for oculomotor control?
CN III, IV, and VI (oculomotor, trochlear and abducens)
the image must be held steady on the _______ of the retina for a clear picture
fovea
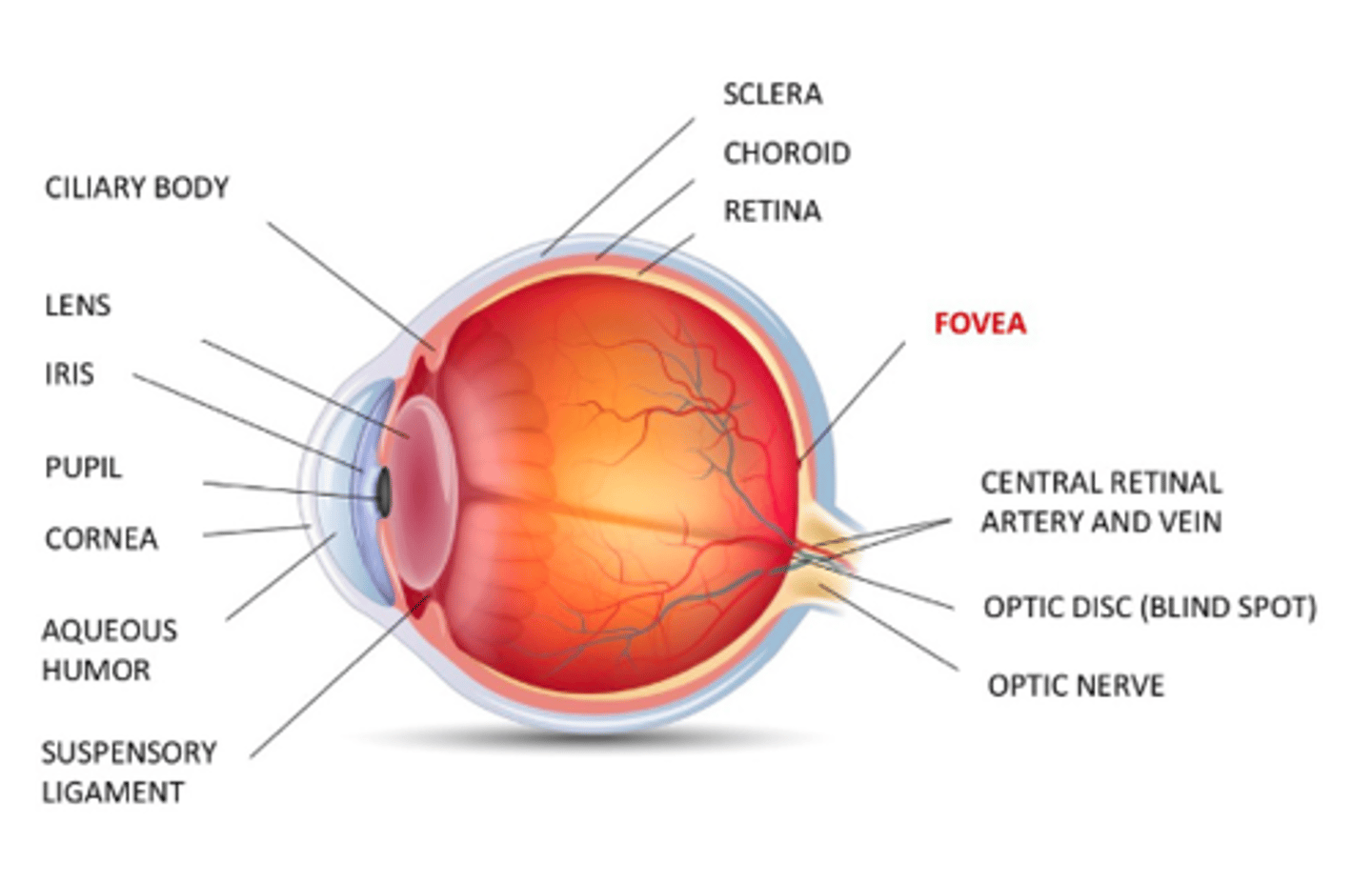
if the image is not held steadily on the fovea of the retina, what can occur?
- blurry vision
- diplopia (double vision)
- eye strain
- dizziness
- oscillopsia (world moves with head movements)
- disequilibrium (balance and vision linked)
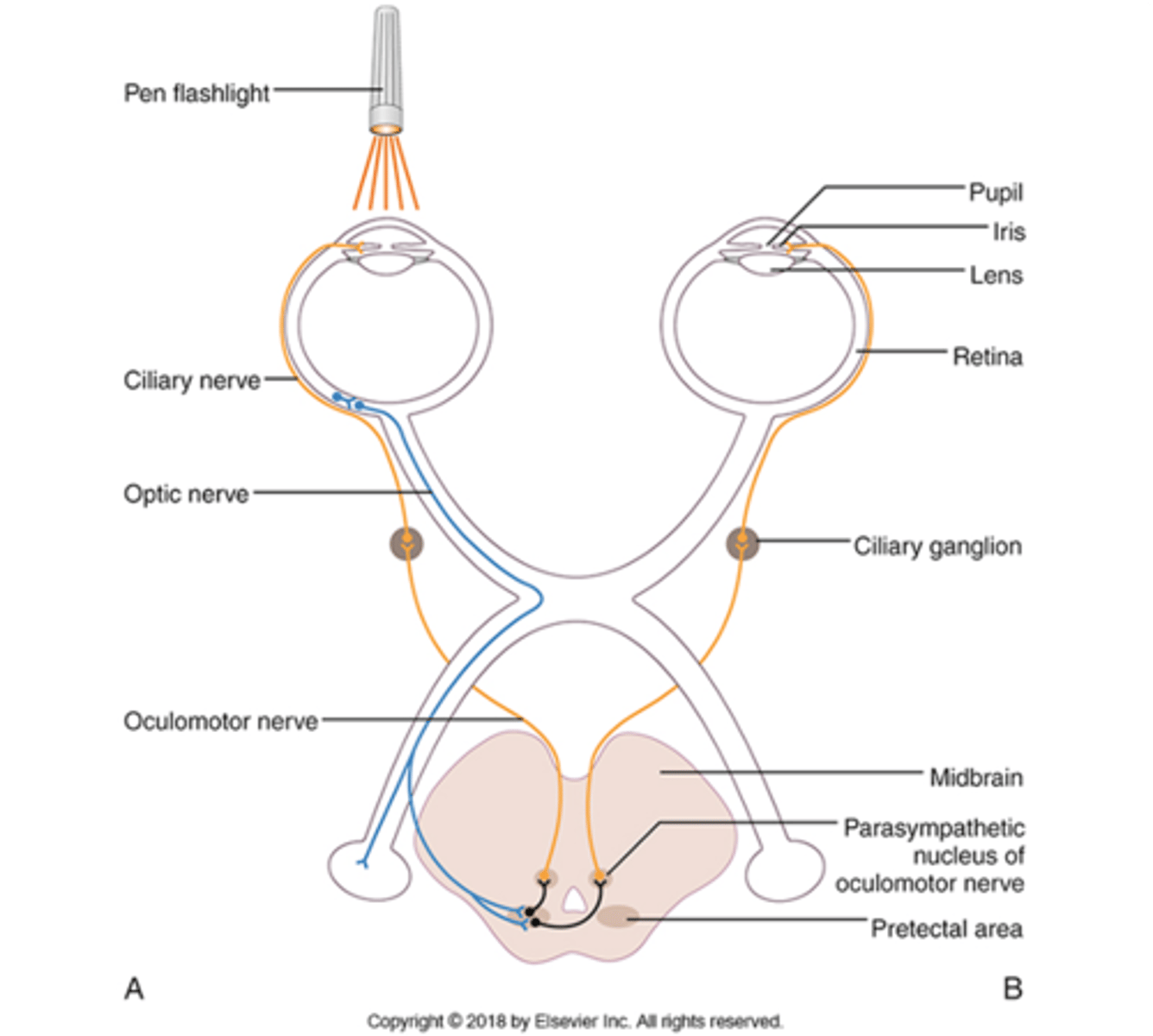
describe the pupillary light reflex
light shined into 1 eye constricts both pupils
When describing the pupillary light reflex, the optic nerve projects onto the lateral geniculate nucleus and also travels down a parallel path to the _______________
oculomotor nuclei
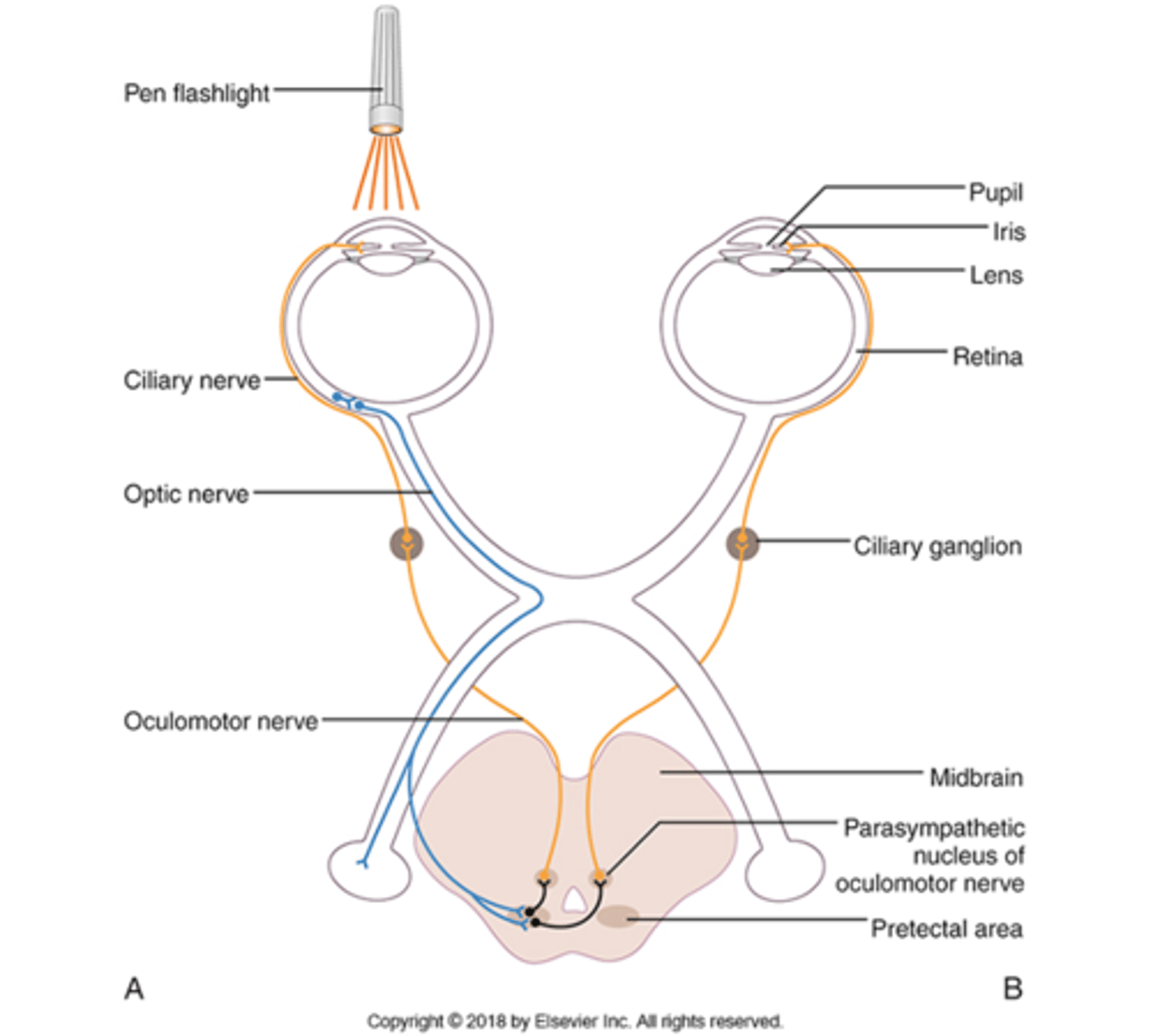
When stimulated by the optic nerve, the oculomotor nuclei sends (bilateral/unilateral) projections down the oculomotor nerve and causes (ones or both) eyes to constrict
bilateral
both eyes
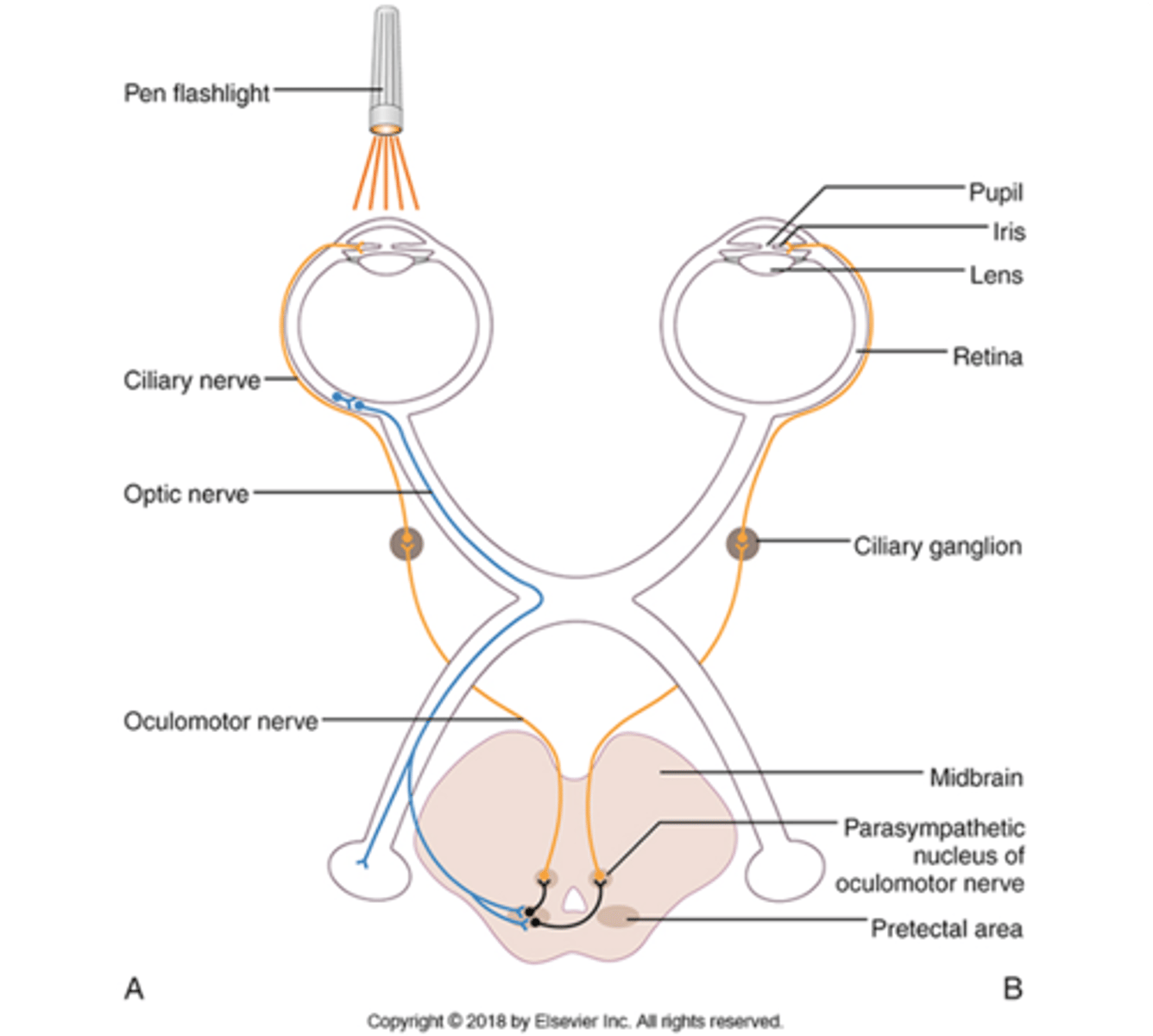
in the pupillary light reflex, which cranial nerve is afferent and which is efferent?
Afferent: CN II (optic nerve)
Efferent: CN III (oculomotor nerve)
What other parasympathetic function does CN III (ocolomotor) have?
provides accommodation for near vision
decreases tension on ligaments that hold the lens to flatten it to allow focus
name some functional implications of oculomotor control
- visual proprioception
- fix eyes on and maintain stable visual targets
- potential collision anticipation
- anticipating motor control/postural control requirements
define nystagmus
- involuntary rhythmic conjugate eye movement
- may be spontaneous, gaze evoked or positional
how is nystagmus named?
named by the direction of the fast phase
What is the peripheral nervous system source of nystagmus
- damage to vestibular receptor or nerve
- engaged when head rotation exceeds limits of eye rotation, to produce a slow phase eye movement (VOR) in one direction and a fast saccadic "reset" back towards primary position
what is the central nervous system source of nystagmus?
occurs as a result of number of different brain conditions or damage to certain brain (stem) structures
What are 3 examples of physiological (normal) nystagmus?
- end point
- rotary
- optokinetic nystagmus
describe end point nystagmus
nystagmus is observed at end-point in 30% of healthy individuals
describe rotary nystagmus
occurs when head spinning is induced
describe optokinetic nystagmus
keeping moving targets on fovea
What are 3 types of pathological nystagmus?
- spontaneous
- gaze-evoked
- positional
describe gaze evoked nystagmus
- damage to neural integrator
- must be differentiated from end-range nystagmus
What are the 6 neuronal control systems for vision?
- visual fixation
- VOR (vestibular ocular reflex)
- OKR (optokinetic reflex)
- pursuit
- saccades
- vergence
define visual fixation
maintains visual gaze on a singular location
define pursuit
hold images of a moving target stable on the retina
define extraocular movement
muscle testing of the eyes
define ocular alignment
maintains eyes centered in the socket
define saccades
rapid movements of the eyes to place the object of interest on the fovea
define vergence
adjusts the eyes for different viewing distances
define vestibular ocular reflex
stabilizes images on fovea of retina during head movement
define optokinetic reflex
hold images of moving targets on the retina
What are the 6 tasks included in the oculomotor exam?
- alignment
- spontaneous and/or gaze evoked nystagmus
- extra ocular movements
- smooth pursuit
- saccades
- convergence
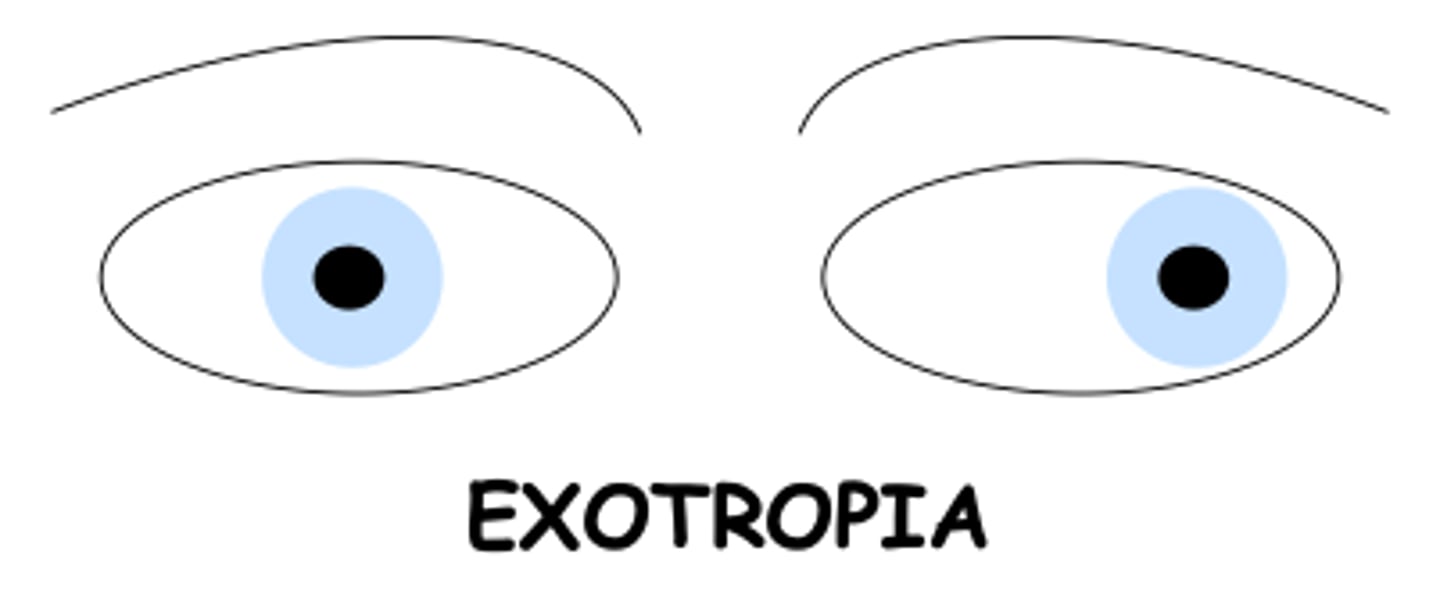
describe the ocular misalignment: exotropia
one or both eyes turn outward
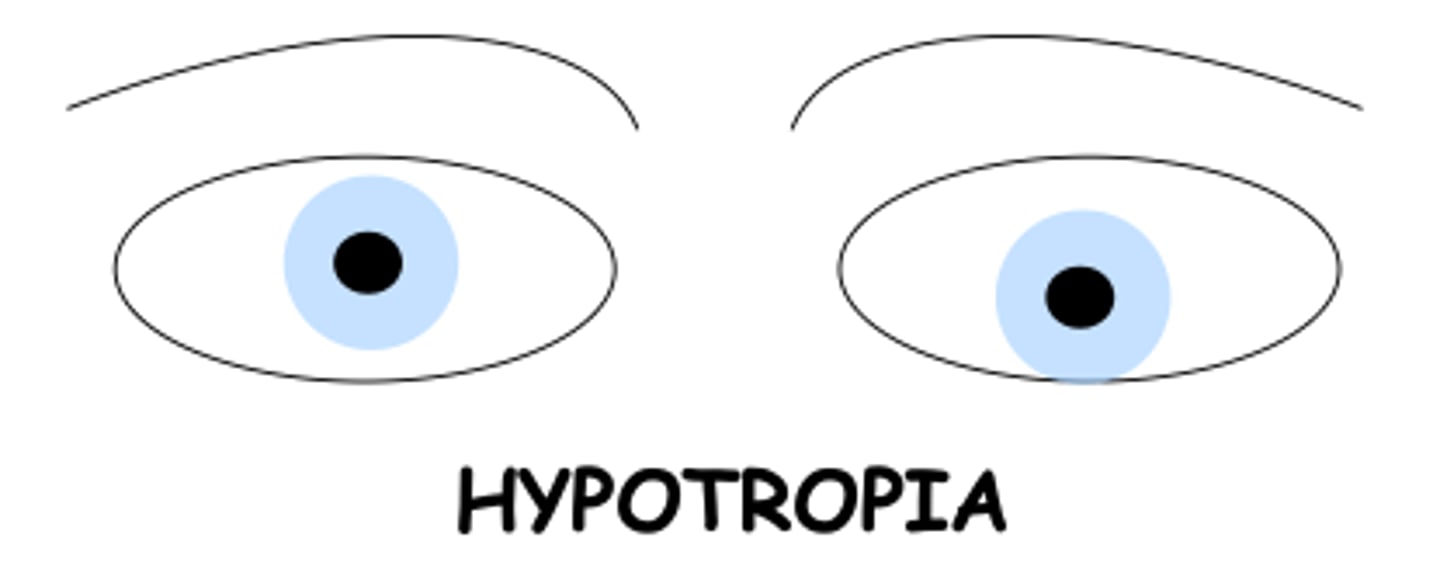
describe the ocular misalignment: hypotropia
one eye deviates downward relative to the other
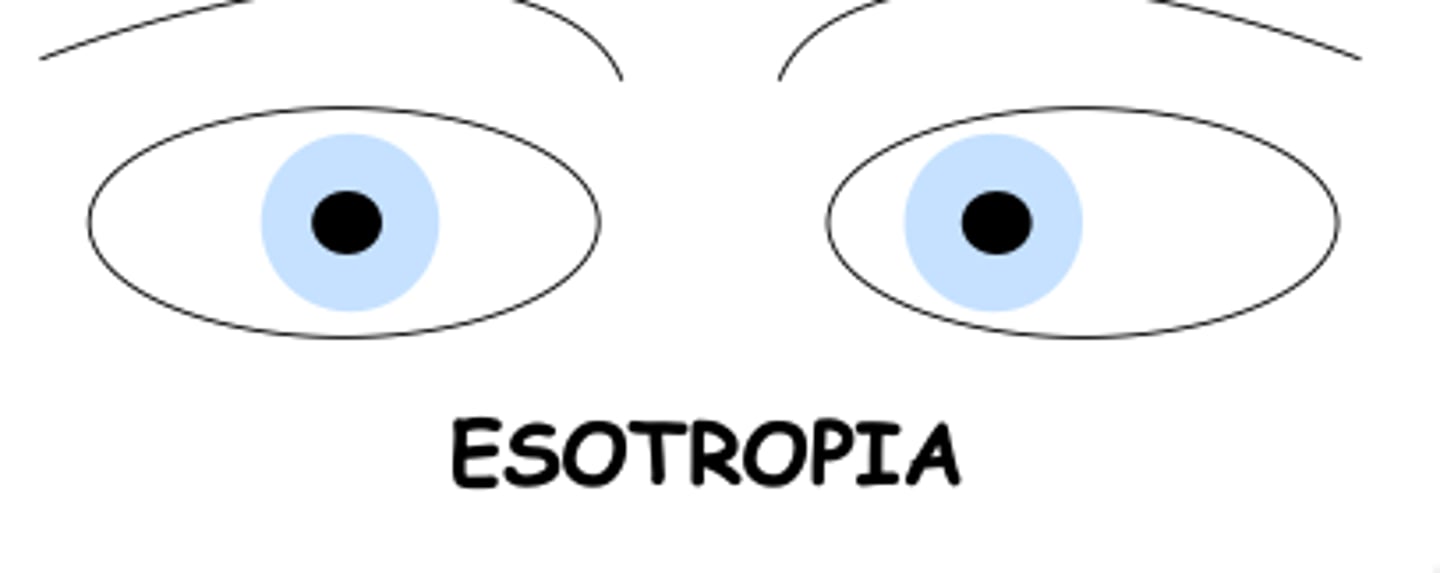
describe the ocular misalignment: esotropia
one or both eyes turn inward
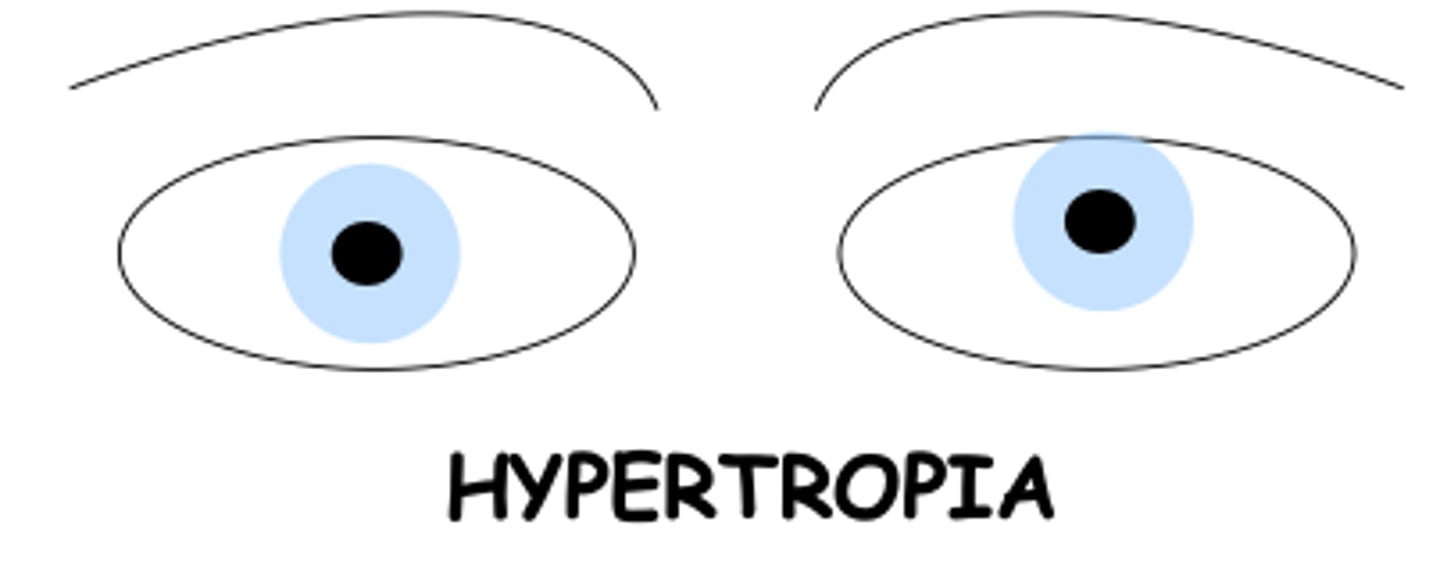
describe the ocular misalignment: hypertropia
one eye deviates upward compared to the other
how to test Gaze-evoked nystagmus (GEN) in the clinic?
- move object 30 degrees to side of midline and have patient maintain position
- test both horizontally and vertically
- test with and without fixation
- note presence and direction of nystagmus
How to assess extra-ocular movements in the clinic
- determine if ROM is full and gaze is conjugate (eyes move together)
what does abnormality of extra ocular movements indicate?
potential cranial nerve abnormality
How to test smooth pursuit in clinic?
- smoothly move discrete target 30 degrees from center horizontally and vertically
what is abnormal finding in smooth pursuit?
- abnormal if catch up saccades are seen
- abnormality may indicate CNS involvement
Where are saccadic pulse generators located?
brainstem and cerebellar sites
what are the brainstem and cerebellar sites the saccadic pulse generators are located in?
- paramedian pontine reticular formation
- nucleus of the dorsal raphe
- rostral interstitial nucleus of MLF
- pontine nuclei
- medial vestibular nucleus (medulla)
- vestibulo-cerebellum
What are the cortical and higher level control areas that project onto saccade generators?
- superior colliculus
- frontal eye field
- posterior parietal cortex
- basal ganglia
how to test saccades in the clinic?
- hold object 15-20 degrees from midline
- ask pt to shift gaze from nose to object and back (left, right, up, down)
what are normal and abnormal responses to saccade testing?
normal: 2 movements to get to the target
abnormal
- eyes undershoot more than 10% of the distance or overshoot at all
- hypermetria always indicates CNS involvement
What is vergence?
moves the eyes in opposite directions to keep images at different distances stable on the fovea
what is the vergence triad?
- convergence
- acommodation
- mitosis
convergence
move inward
divergence
move outward
where are the neurons that control vergence located?
distributed in teh rostral superior colliculus of the MIDBRAIN in the same regions as control centers for saccades and pursuit
near the point of convergence
target DOUBLES
6-10 cm
near the point of accommodation
target BLURS
15 cm
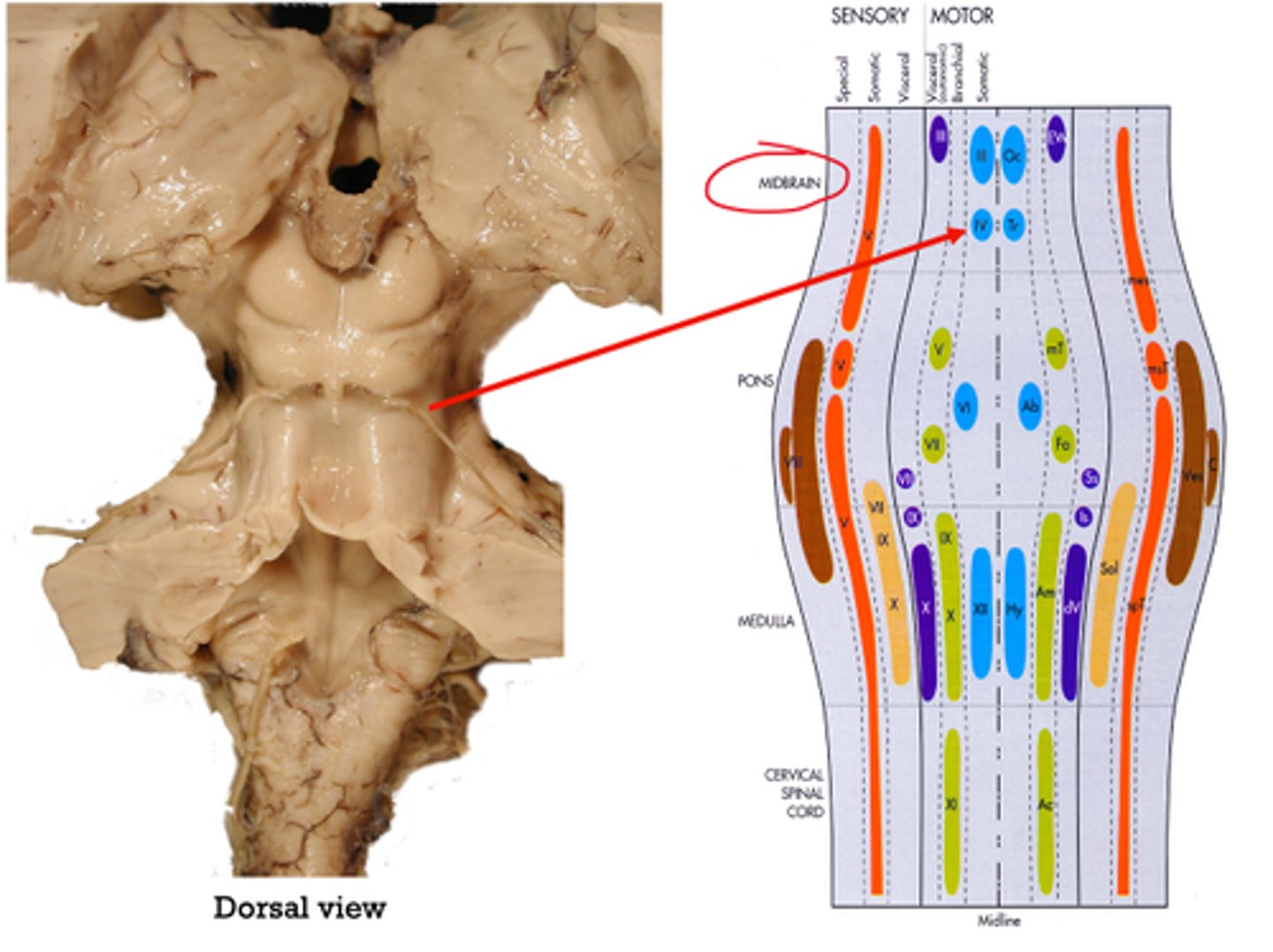
Where does CN III (oculomotor) originate?
midbrain
(visible from ventral view)
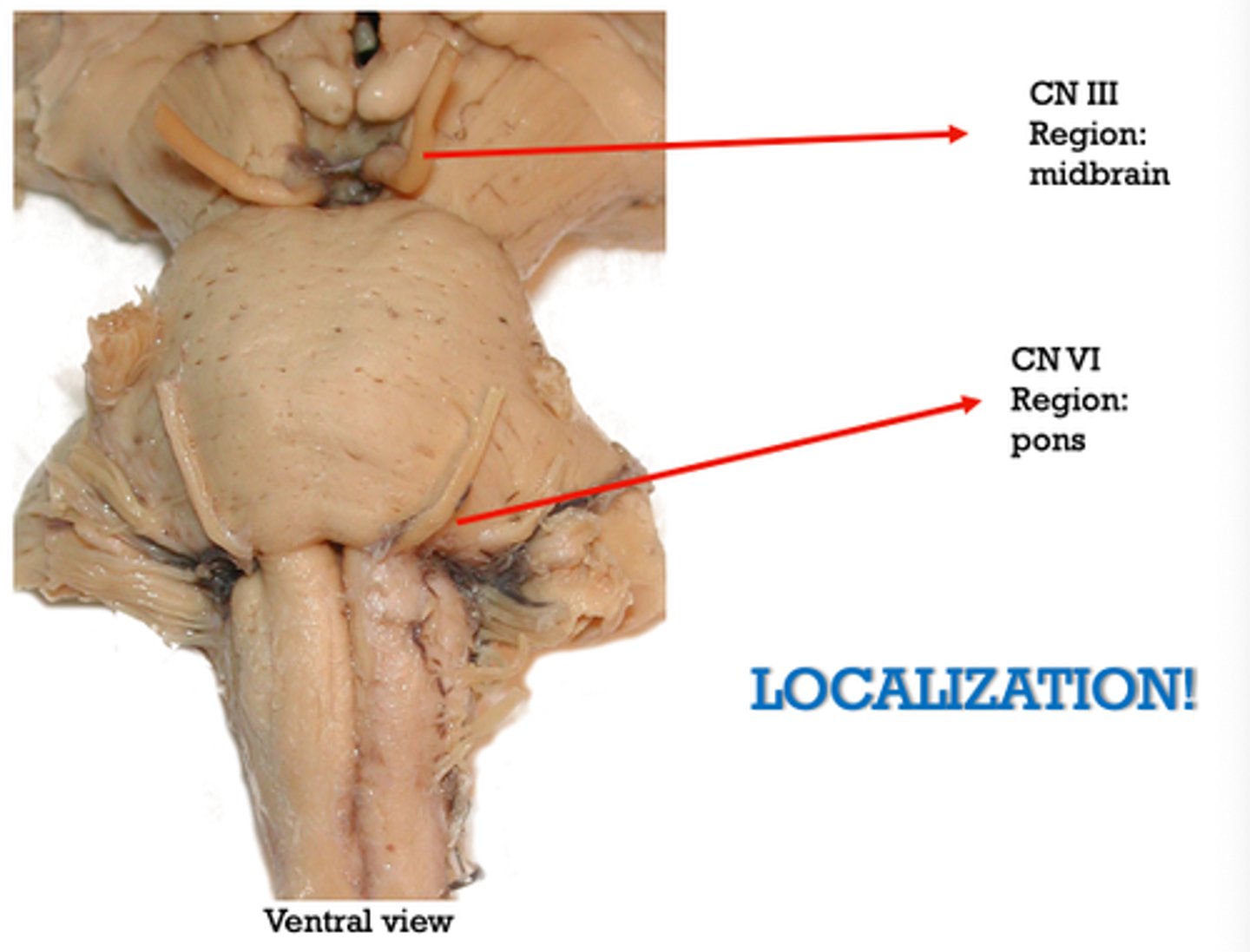
Where does CN VI (abducens) originate?
pons
(visible from ventral view)
where does CN IV (trochlear) originate?
midbrain
(visible from dorsal view)
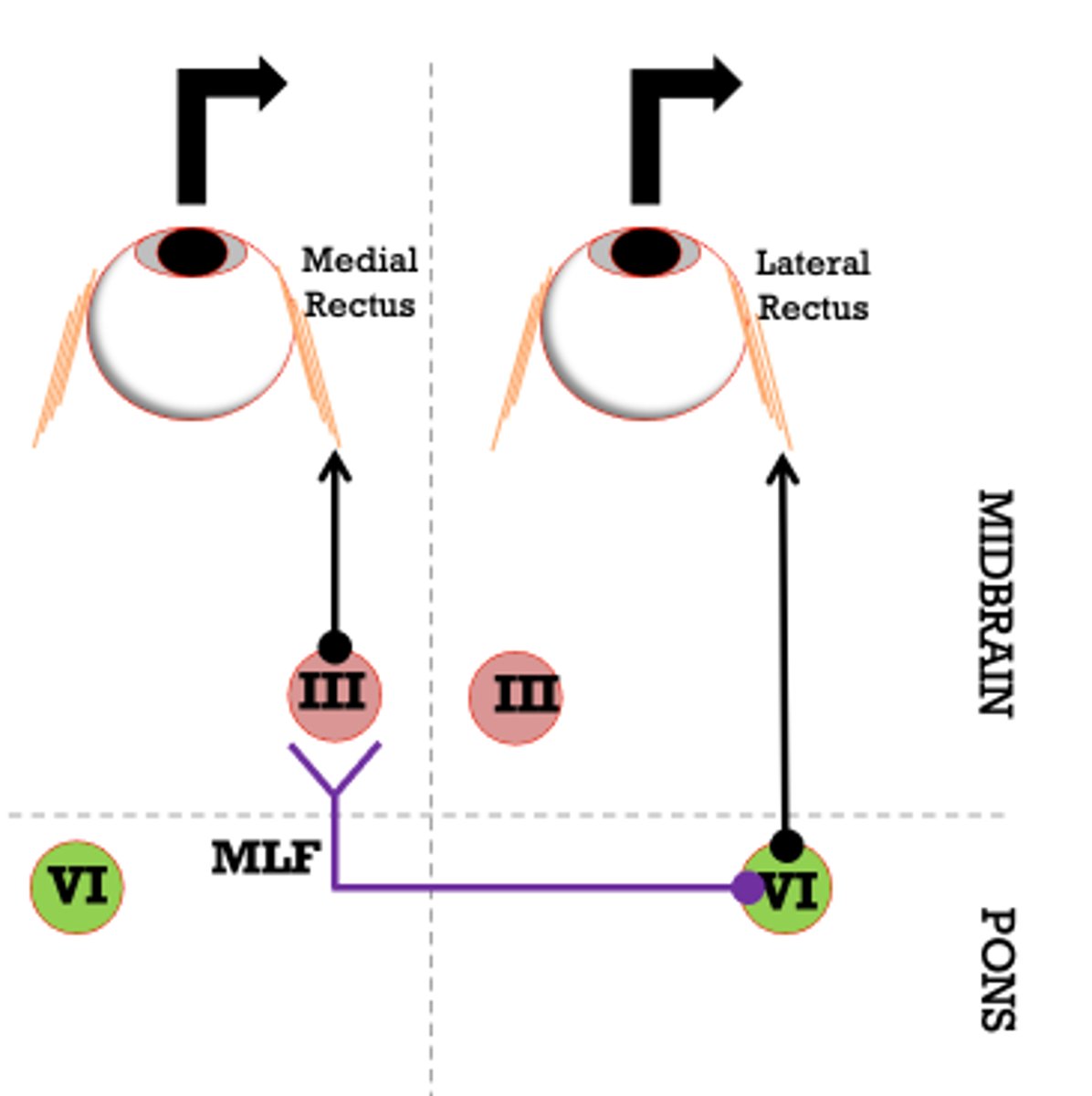
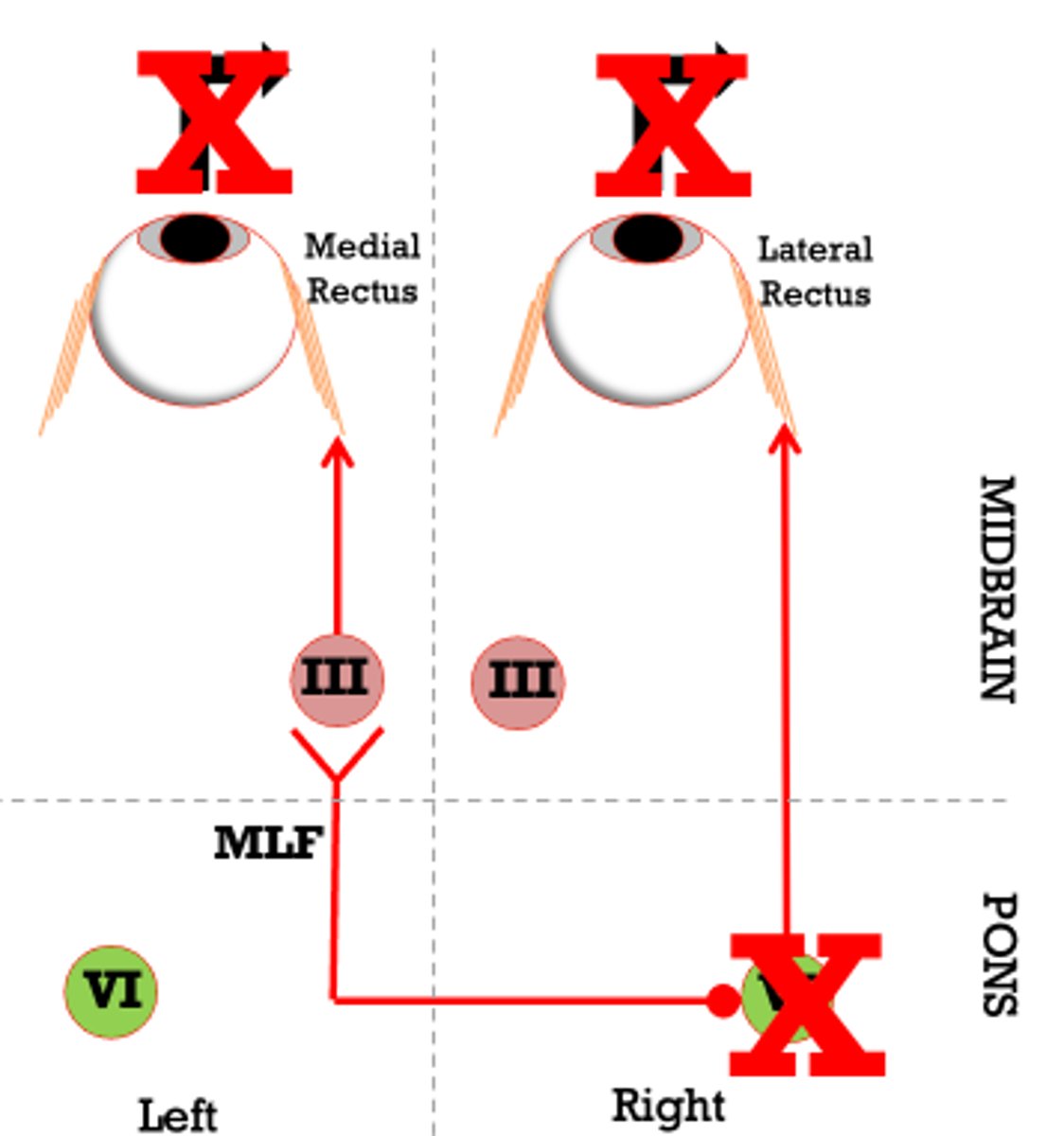
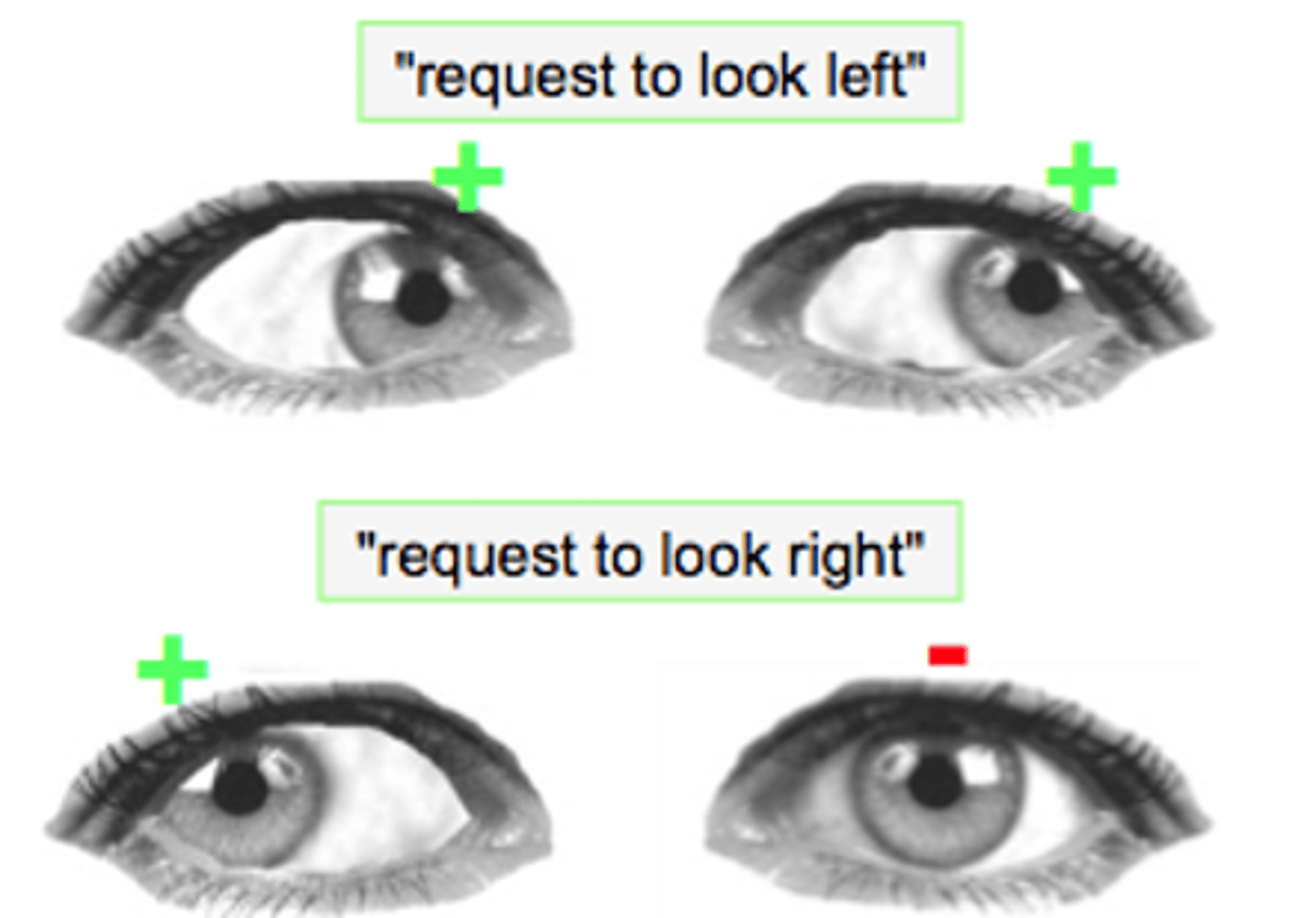
describe the pathway for horizontal conjugate gaze mechanism
- information arises to abducens nucleus
- CN IV activates ipsilateral lateral rectus
- information also crosses to contralateral MLF to oculomotor nucleus
- this activates CN III to activate contralateral medial rectus
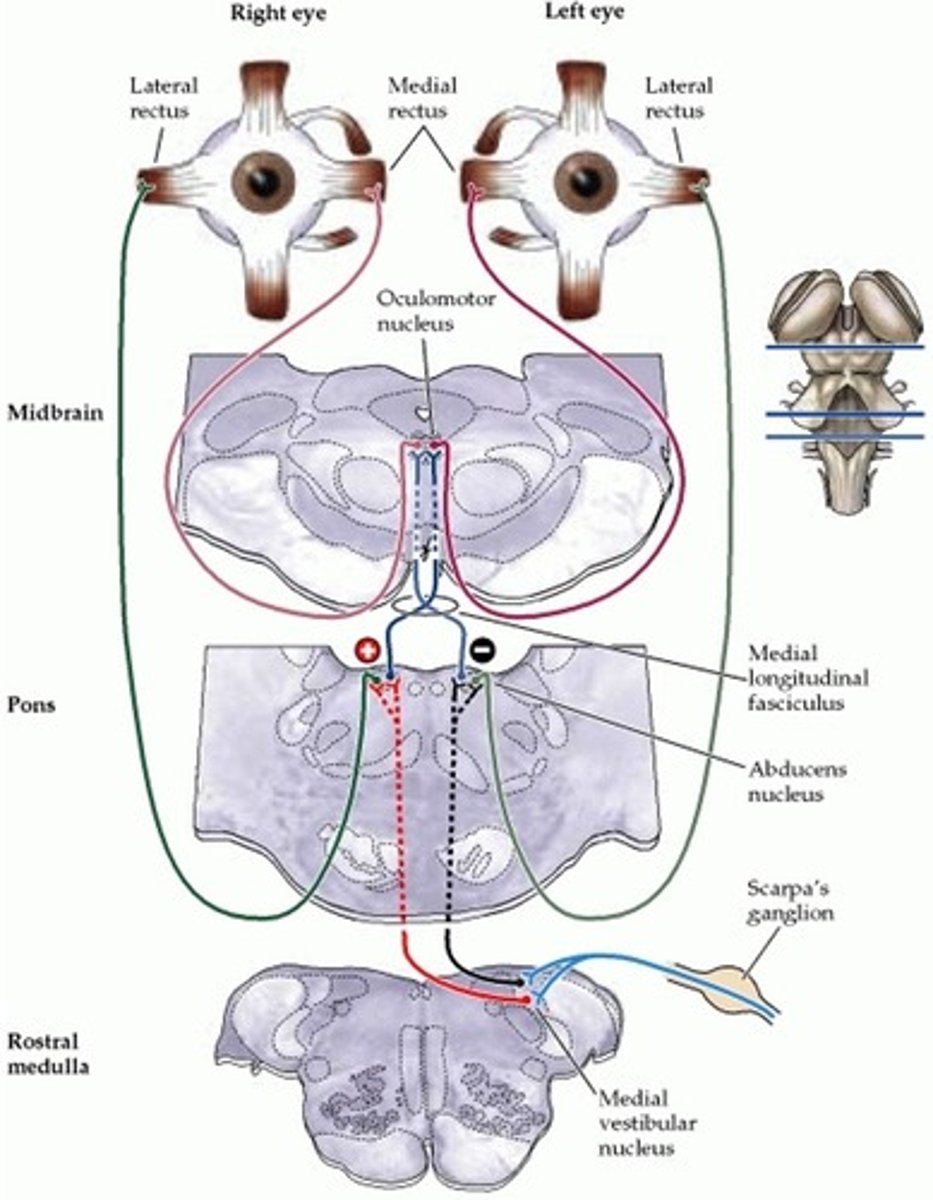
Why is it difficult to localize source of impairment with deficits in horizontal conjugate gaze mechanism?
can't clearly differentiate between midbrain and pons
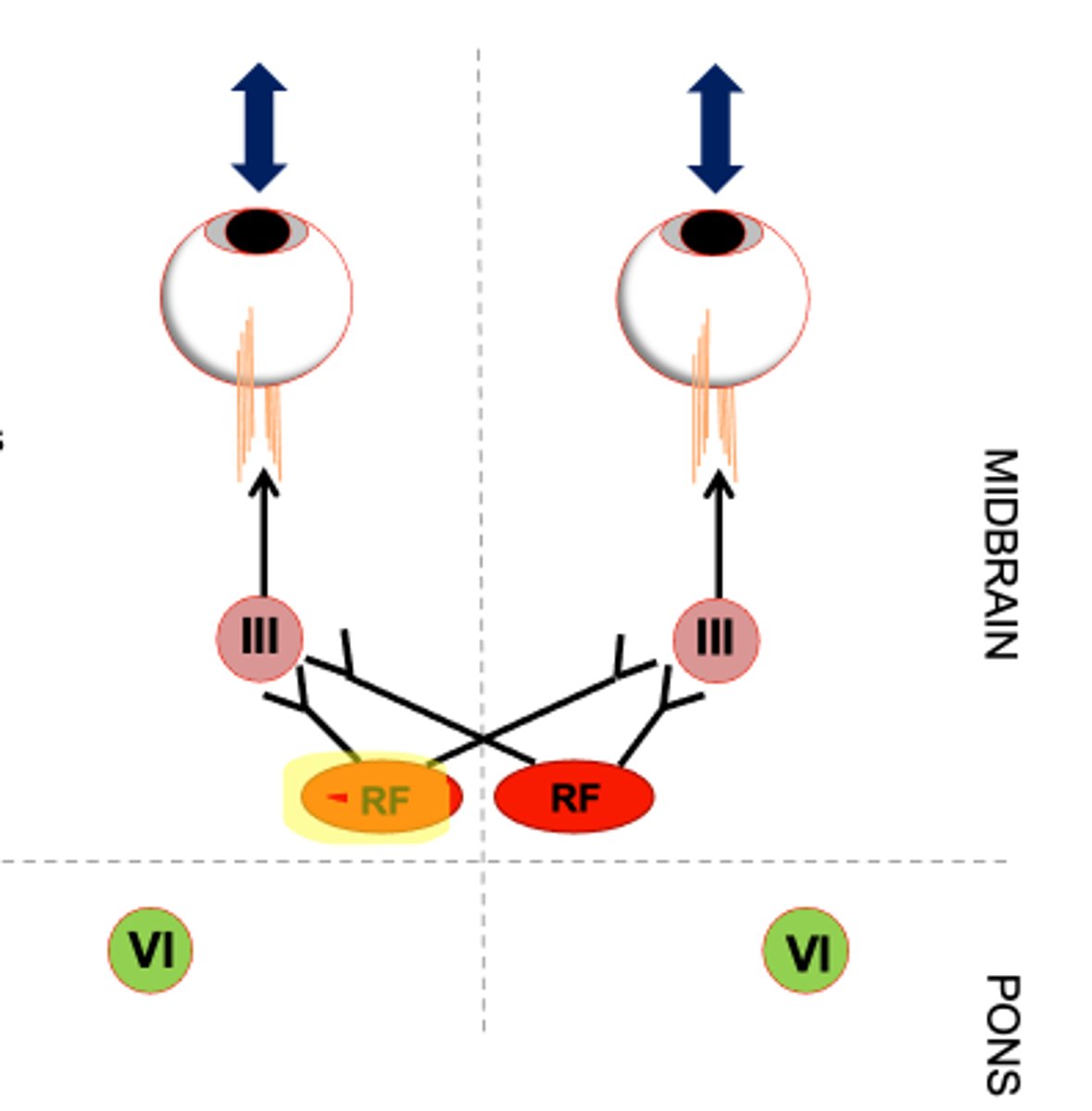
If a patient is having deficits with vertical conjugate movements where is the lesion?
midbrain
(not vestibular)
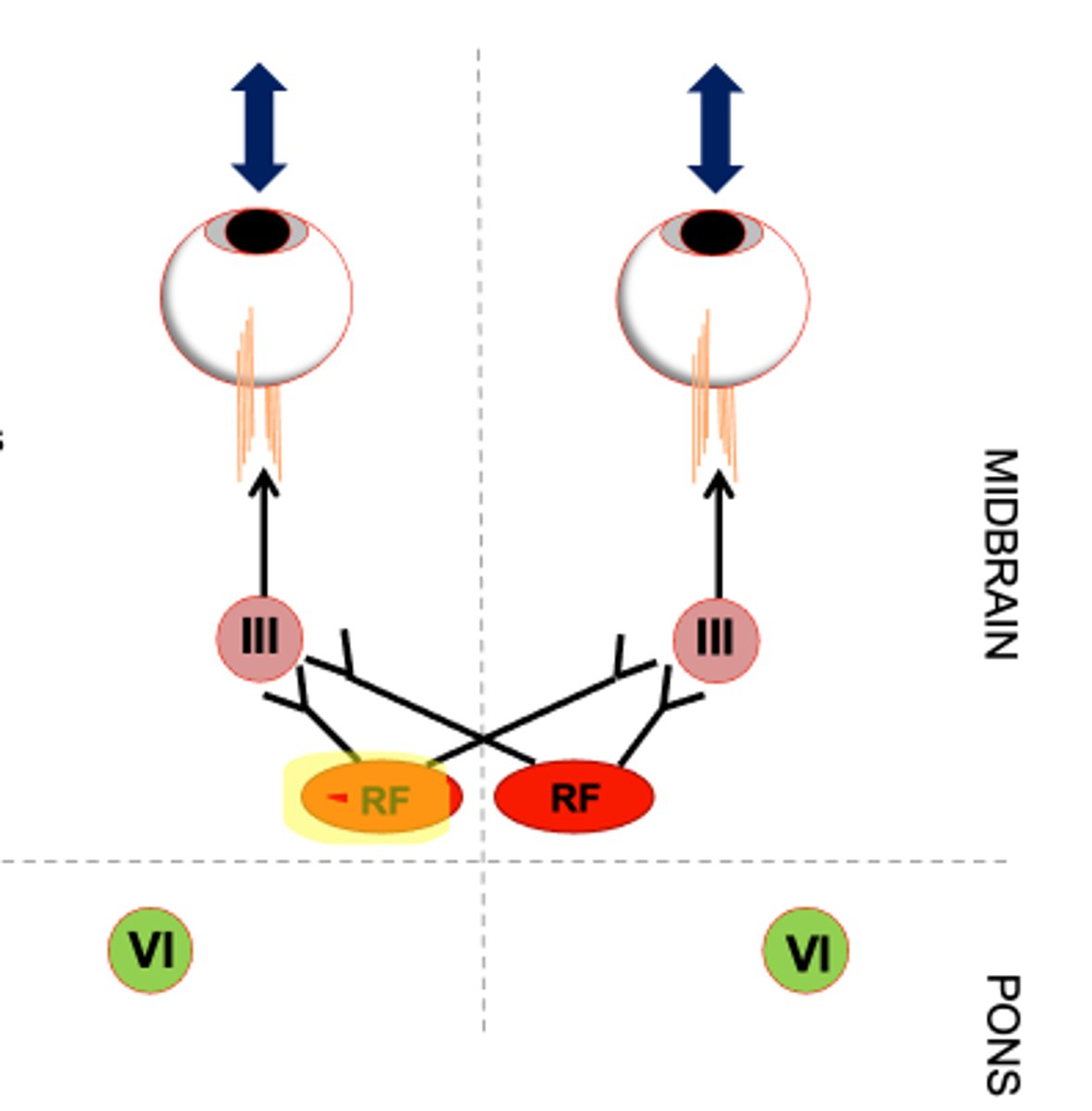
oculomotor neurons are recruited (bilaterally/unilaterally?) for vertical eye movements?
bilaterally
a lesion of Abducens Nucleus will result in a loss of....
- ipsilateral lateral rectus
- contralateral medial rectus d/t effect on contralateral MLF
A lesion of the Abducens nucleus will result in what gaze deficit?
no ipsilateral horizontal gaze (toward side of lesion)
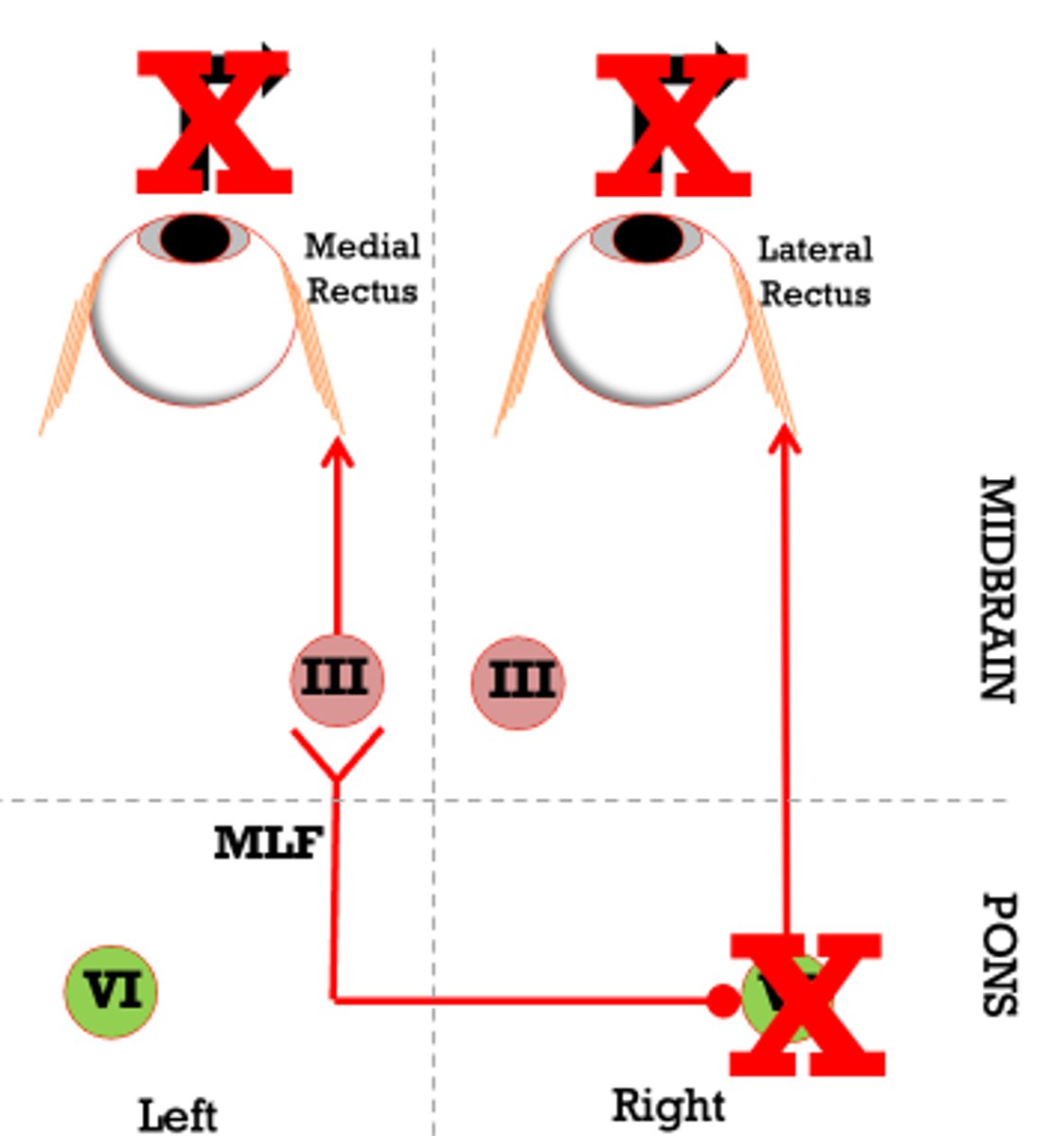
A lesion of Abducens Nucleus will result in what primary gaze deficit?
IPSILATERAL esotropia
Only the ipsilateral eye to the lesion will be affected with esotropia, why?
- contralateral eye has only lost ability for conjugate gaze because its not getting input from MLF
- medial rectus holds in primary gaze
A lesion of the MLF (PONS OR MIDBRAIN) will cause what oculomotor deficits?
ipsilateral eye cannot ADDuct d/t lack of input to ipsilateral medial rectus
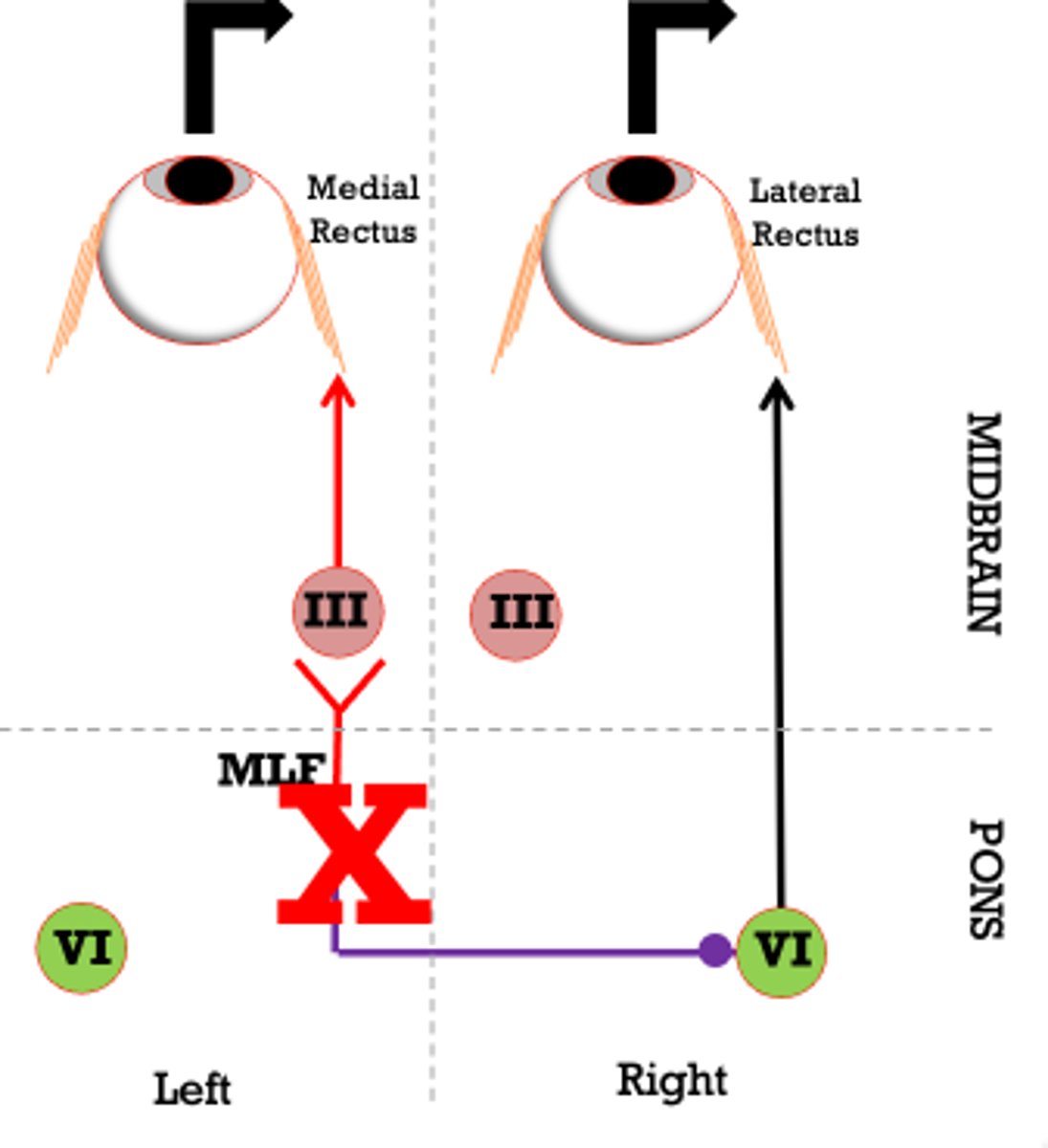
what would a lesion of L MLF look like in clinical exam?
what is the primary gaze deviation associated with lesion of MLF (pons or midbrain) internuclear ophthalmoplegia (INO)
there is no primary gaze deviation