Clinical Chemistry - Lecture 2: Electrolytes/Acid-Base Balance (Case Studies)
1/16
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
17 Terms
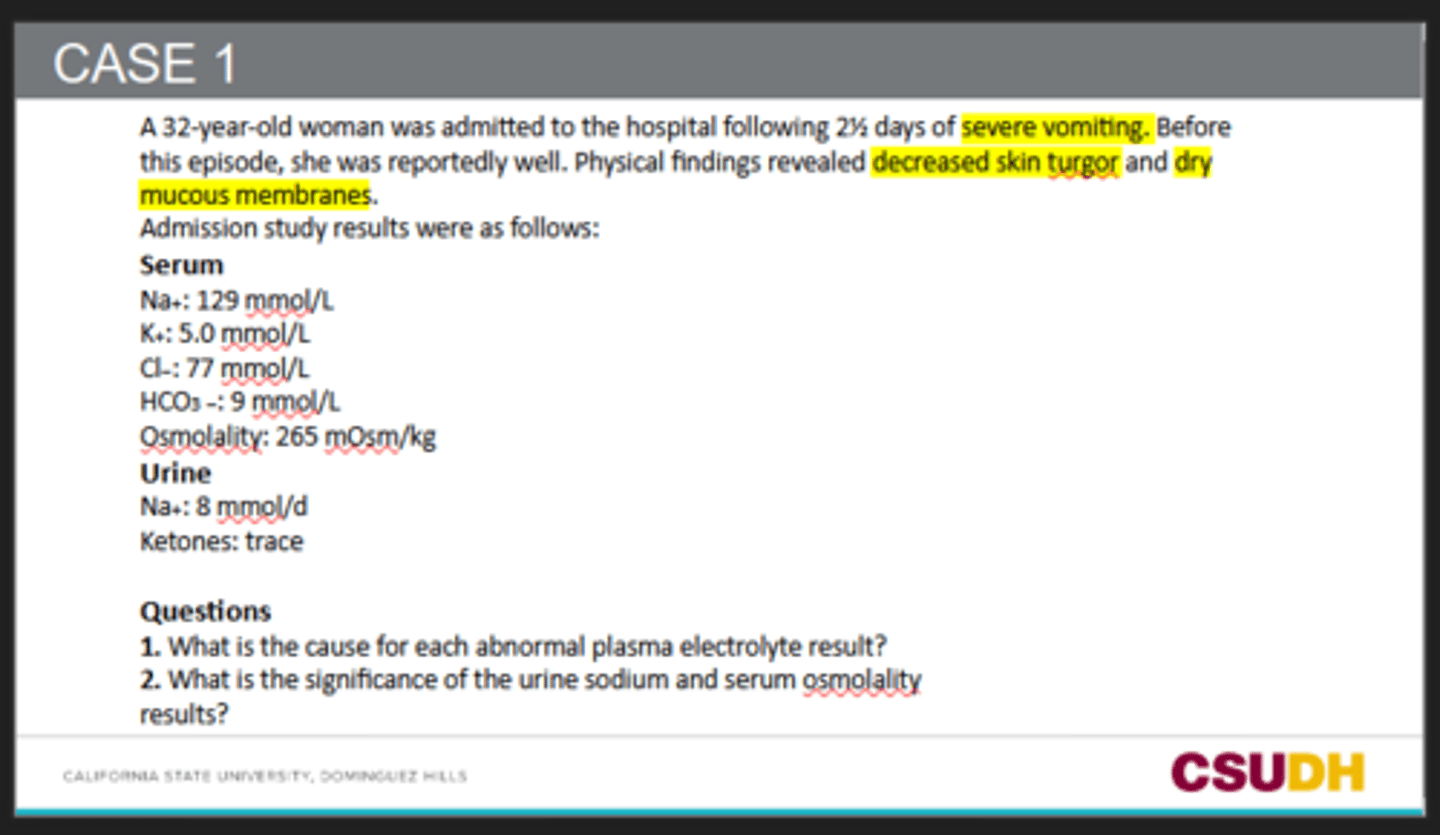
Na⁺ = 129 mmol/L (low → hyponatremia) Caused by loss of sodium and water from severe vomiting plus dehydration. The body also retains water through ADH release, which dilutes sodium levels.
Cl⁻ = 77 mmol/L (low → hypochloremia) Vomiting causes loss of gastric hydrochloric acid (HCl), so chloride is lost from the body.
HCO₃⁻ = 39 mmol/L (high → metabolic alkalosis) Vomiting causes loss of stomach acid (H⁺). Losing acid makes bicarbonate relatively increase, leading to metabolic alkalosis.
Osmolality = 265 mOsm/kg (low) The low sodium level lowers serum osmolality because sodium is a major contributor to plasma osmolarity.
K⁺ = 5.0 mmol/L (upper normal/slightly high-normal) Potassium may appear normal/high initially due to dehydration and shifts caused by acid-base imbalance, even though total body potassium may actually be depleted from vomiting.
1. What is the cause for each abnormal plasma electrolyte result?
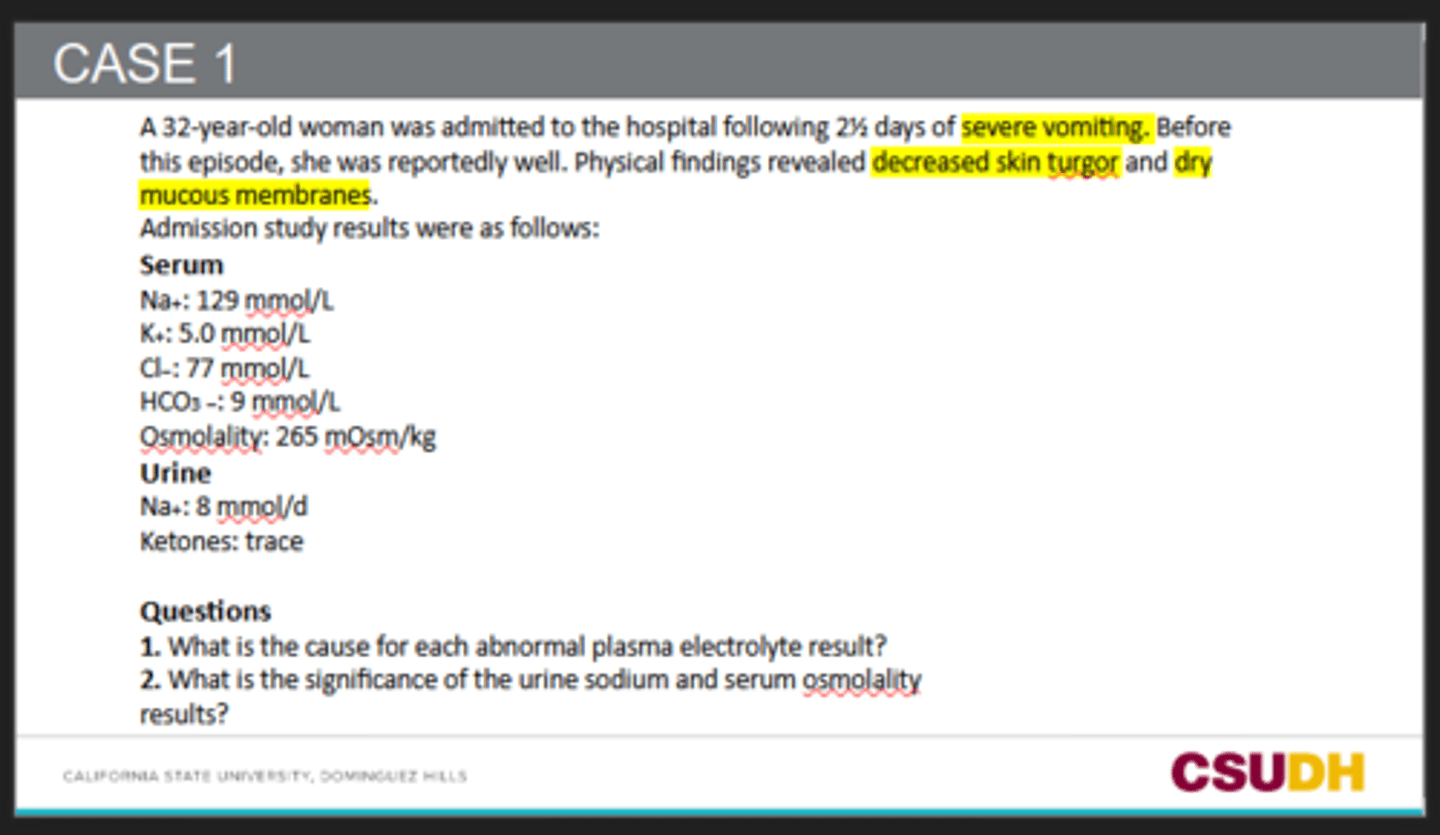
Urine Na⁺ = 8 mmol/day (very low) This means the kidneys are trying to conserve sodium because the patient is volume depleted/dehydrated. The sodium loss is therefore likely outside the kidneys (vomiting), not due to kidney disease.
Low serum osmolality (265 mOsm/kg) Confirms a hypotonic state, mainly due to hyponatremia and excess water retention from ADH release during dehydration.
2. What is the significance of the urine sodium and serum osmolality
results?
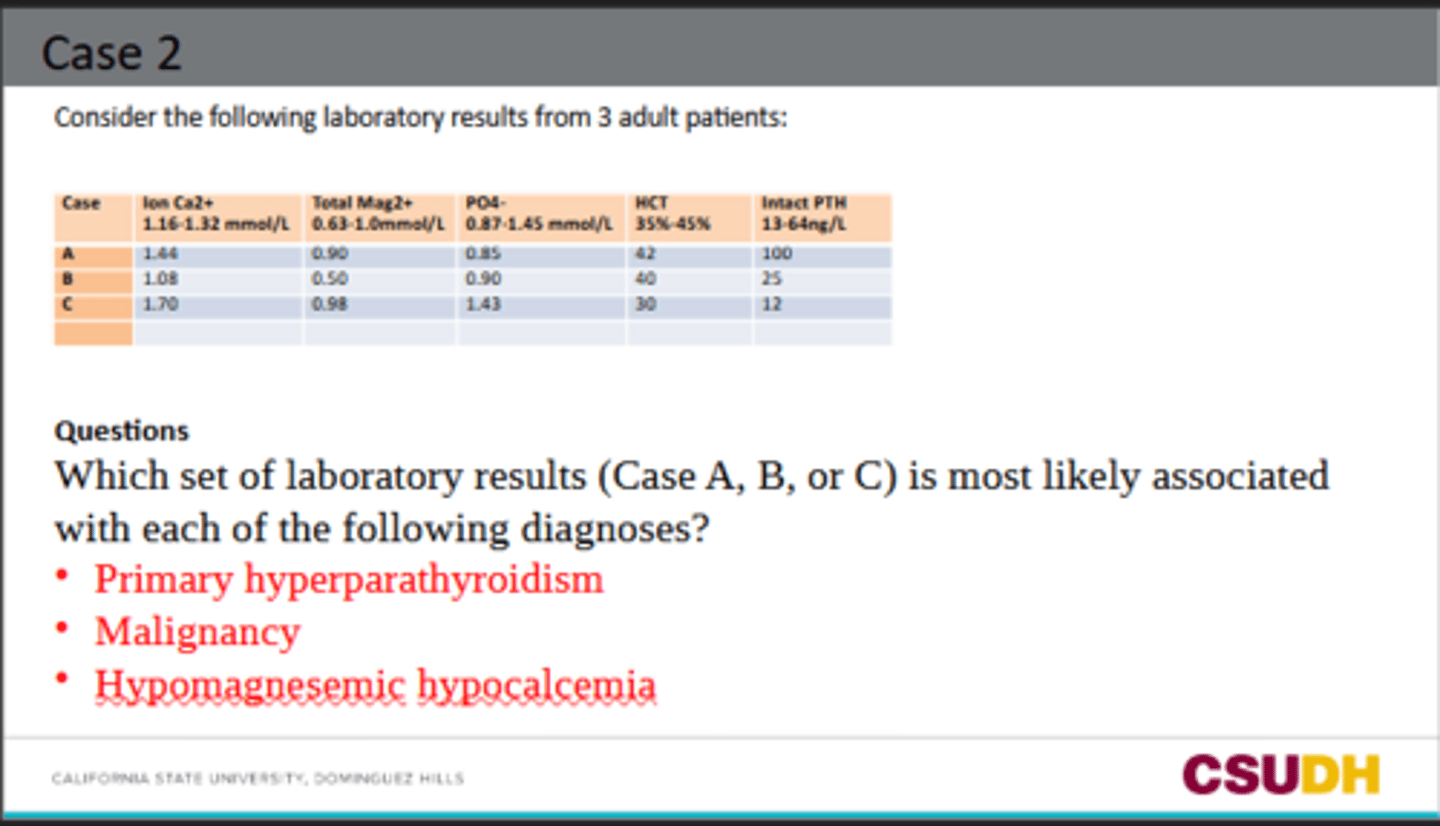
Primary hyperparathyroidism → Case A
High ionized calcium
Low phosphate
High intact PTH
This fits because excess PTH raises calcium and lowers phosphate.
Malignancy → Case C
High ionized calcium
Low PTH
Low Hct
This fits because cancer can cause hypercalcemia, but the parathyroid is not the cause, so PTH is suppressed.
Hypomagnesemic hypocalcemia → Case B
Low ionized calcium
Low magnesium
PTH is not appropriately elevated
This fits because low magnesium can impair PTH secretion/action, causing low calcium.
Which set of laboratory results (Case A, B, or C) is most likely associated with each of the following diagnoses?
Primary hyperparathyroidism
Malignancy
Hypomagnesemic hypocalcemia
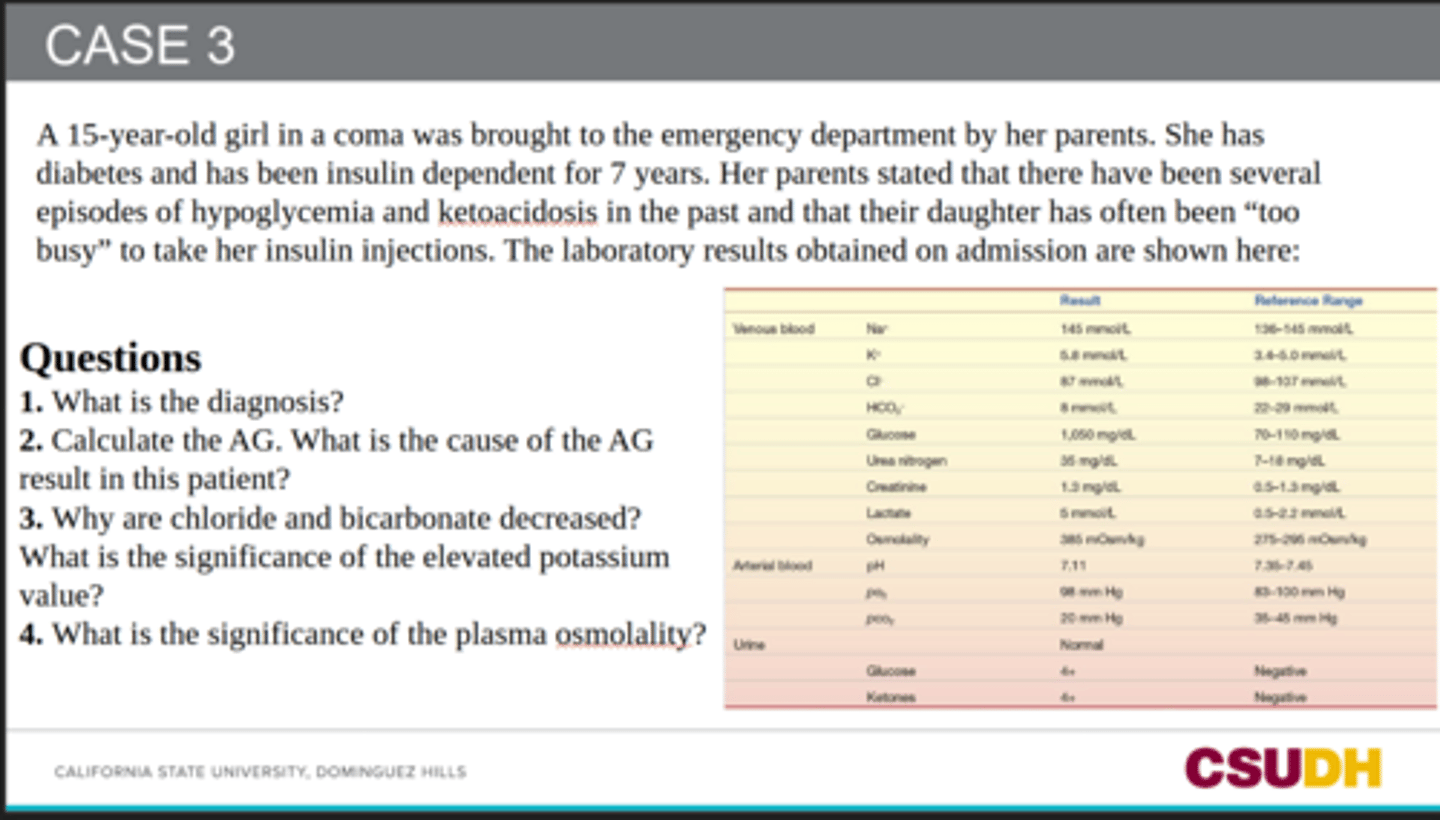
Diabetic ketoacidosis (DKA).
What is the diagnosis?
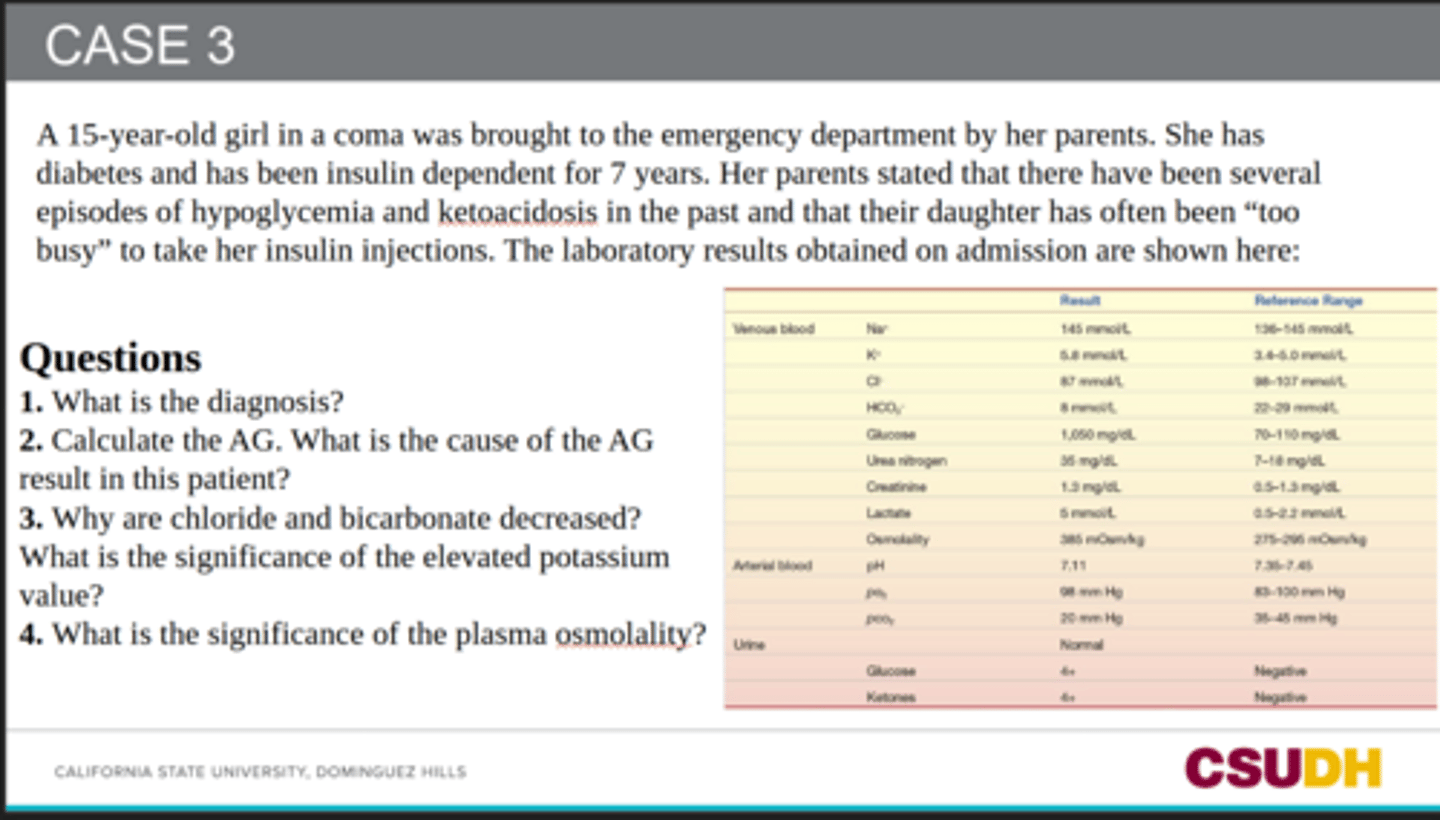
50 (very high)
AG = 145 − (87 + 8) = 50.
Ketoacids from diabetic ketoacidosis, plus lactic acid.
Calculate the AG. What is the cause of the AG result in this patient?
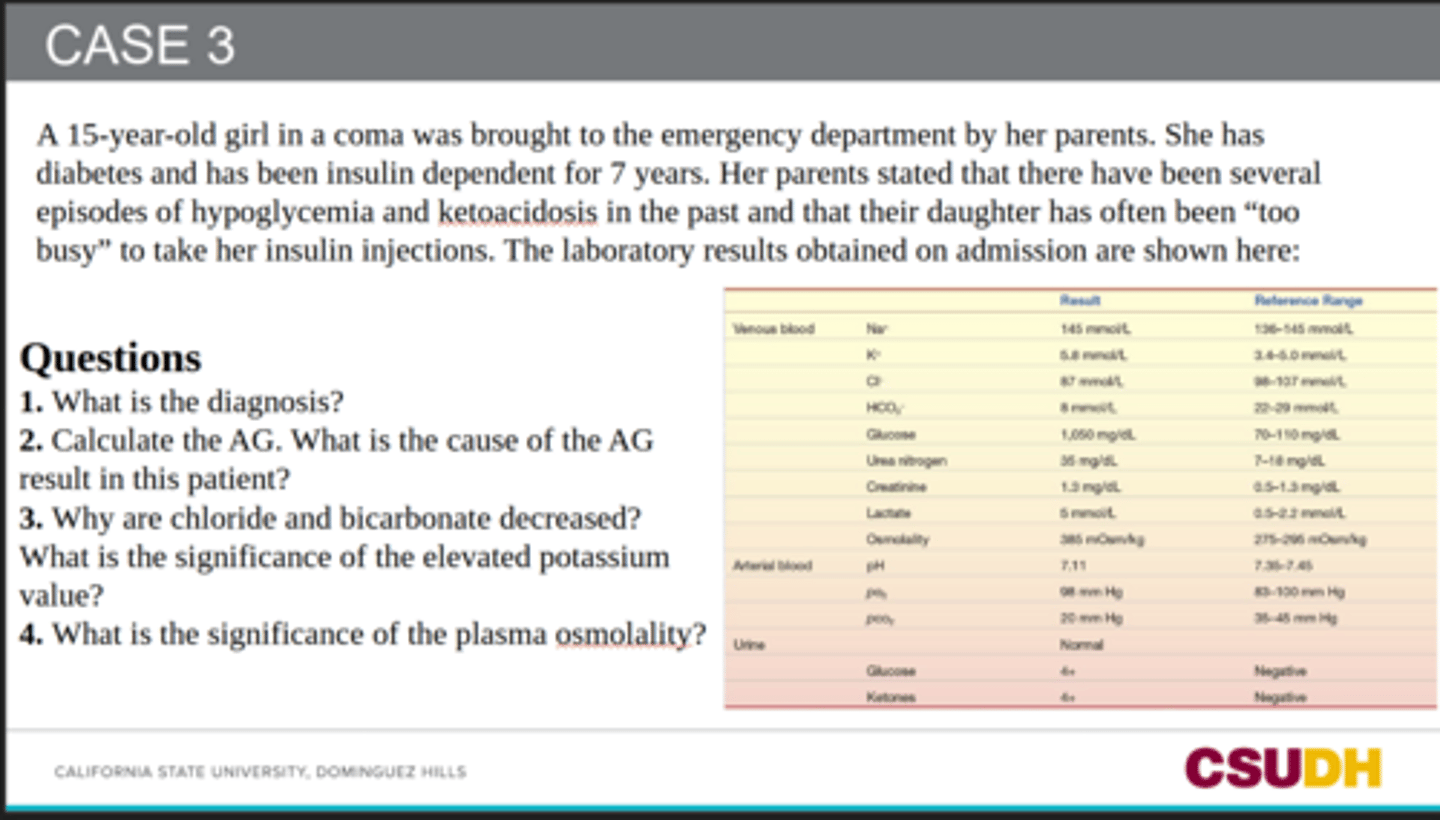
Chloride is low because the patient has a high anion gap acidosis, where unmeasured anions like ketoacids replace chloride. & Bicarbonate is used up buffering excess ketoacids.
Why are chloride and bicarbonate decreased?
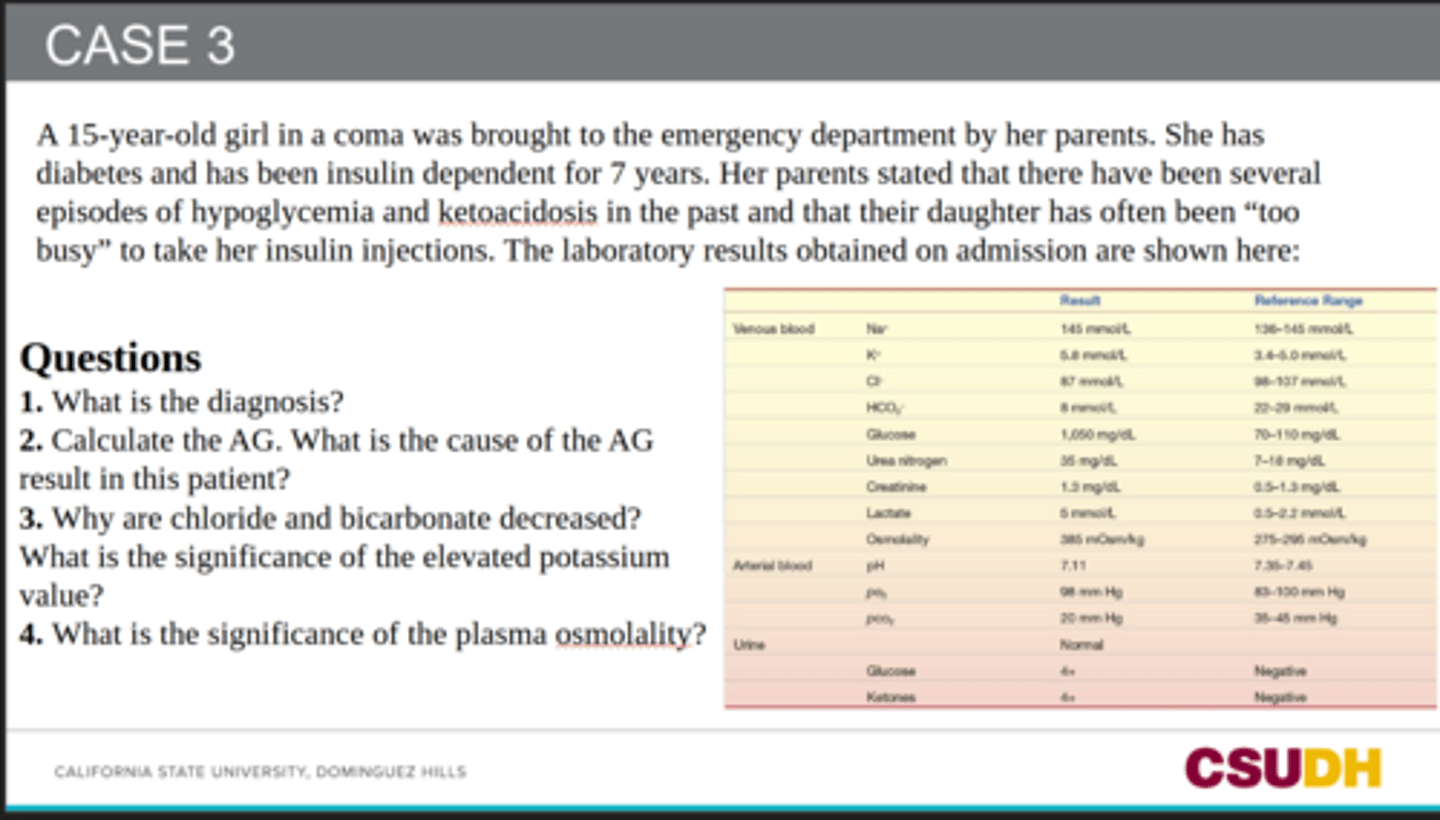
Acidosis and lack of insulin cause potassium to shift out of cells into the blood.
What is the significance of the elevated potassium value?
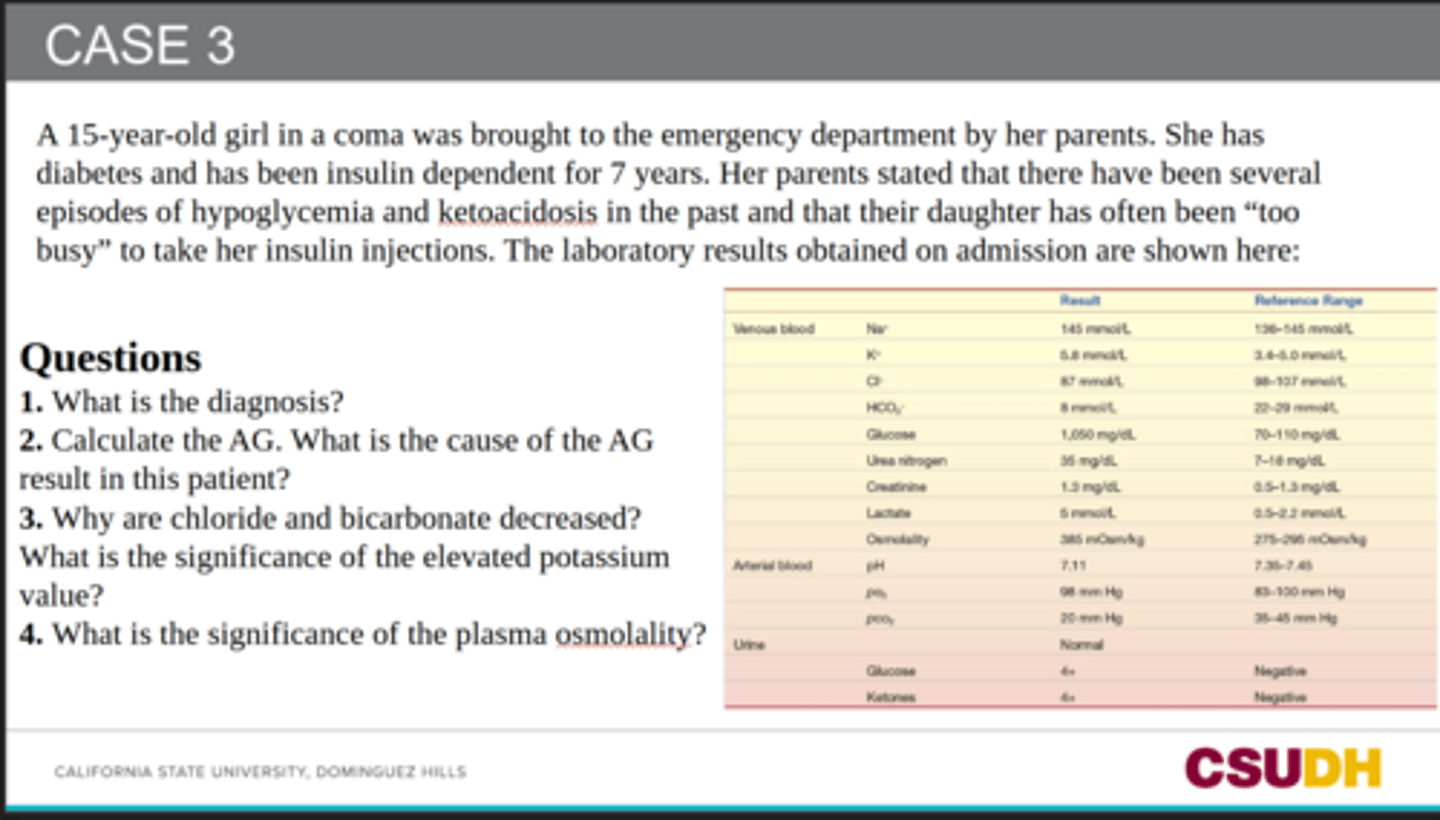
It shows severe dehydration and a hyperosmolar state caused by very high glucose.
The very high glucose pulls water into the blood and causes osmotic diuresis, leading to dehydration.
What is the significance of the plasma osmolality? & why is it high?
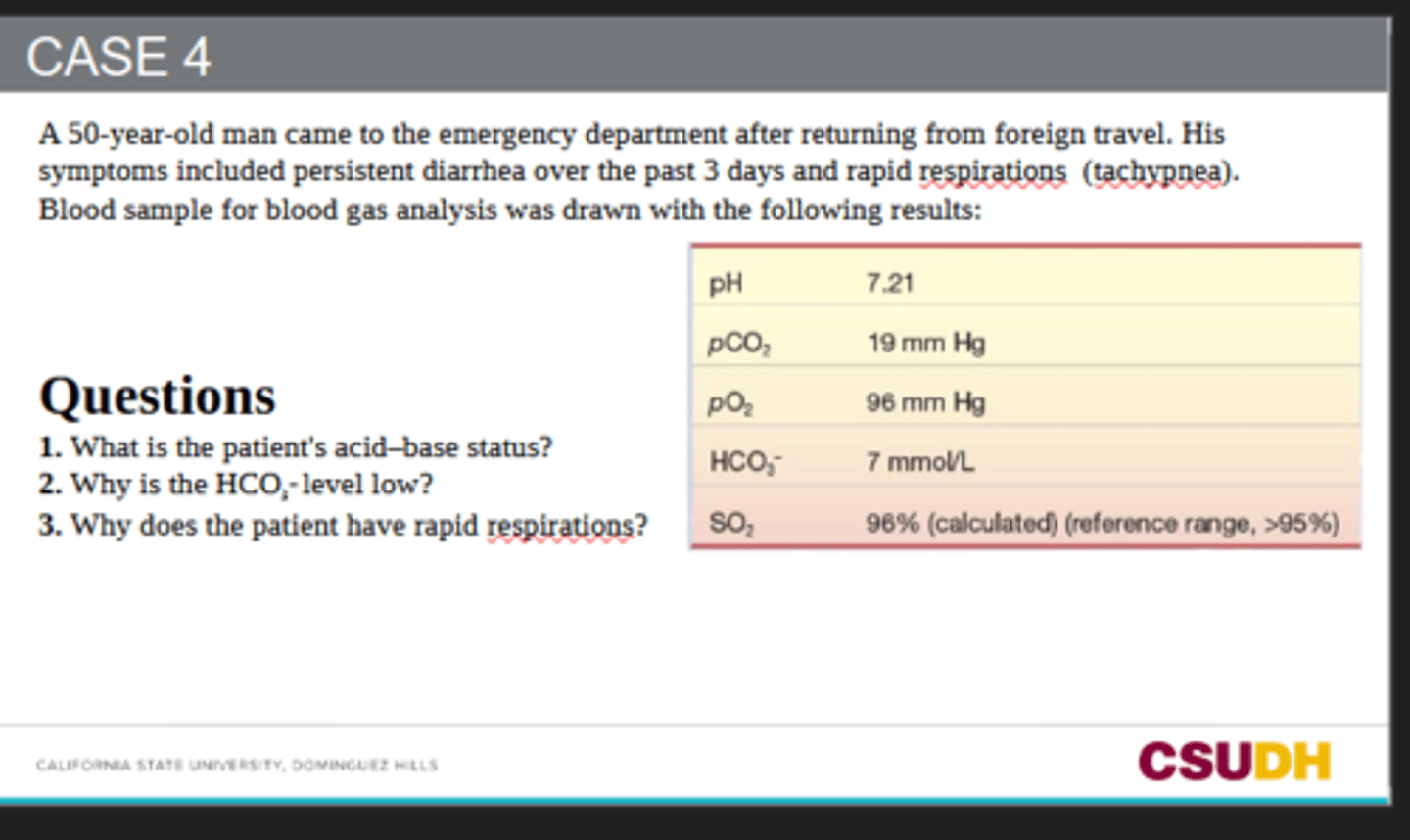
1) The patient has metabolic acidosis with respiratory compensation.
2) HCO₃⁻ is low because it is being used up to buffer excess acid. (Because he has persistent diarrhea, he is also likely losing bicarbonate through the GI tract.)
3) He is breathing rapidly to blow off CO₂. (CO₂ acts like an acid in the blood, so removing CO₂ helps raise the pH and compensate for the metabolic acidosis.)
1. What is the patient's acid-base status?
2. Why is the HCO3- level low?
3. Why does the patient have rapid respirations?
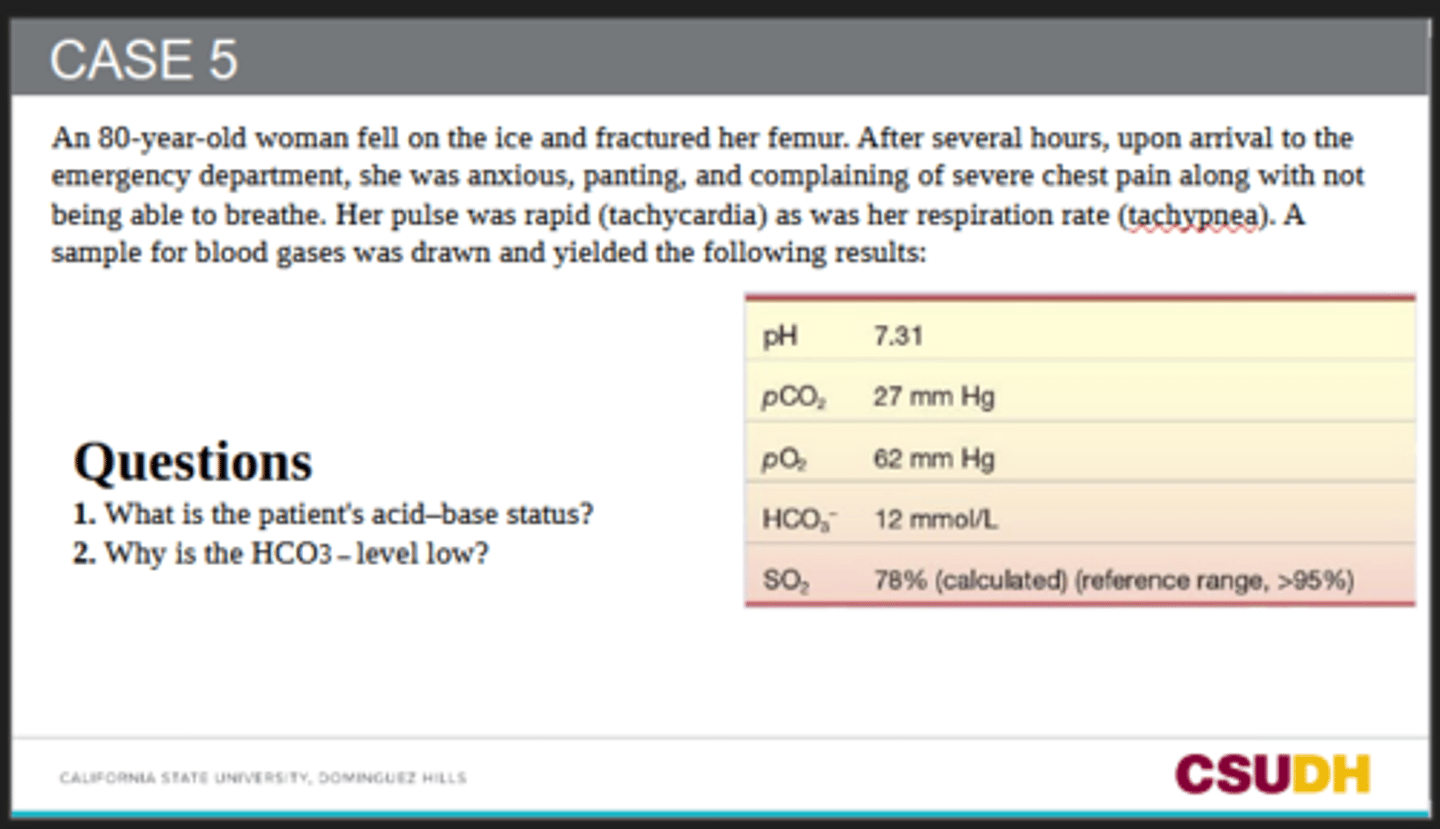
1) The patient has metabolic acidosis with respiratory compensation.
pH = 7.31 → acidotic
HCO₃⁻ = 12 mmol/L → low, indicating metabolic acidosis
pCO₂ = 27 mmHg → low because the lungs are compensating by blowing off CO₂
2) HCO₃⁻ is low because it is being used up buffering excess acid produced from poor oxygen delivery to tissues.
The patient likely developed lactic acidosis due to hypoxia and poor tissue perfusion after trauma, which caused bicarbonate consumption.
Low pO₂ = 62 mmHg
Low O₂ saturation = 78%
These findings support inadequate oxygenation leading to anaerobic metabolism and lactic acid production.
1. What is the patient's acid-base status?
2. Why is the HCO3 - level low?
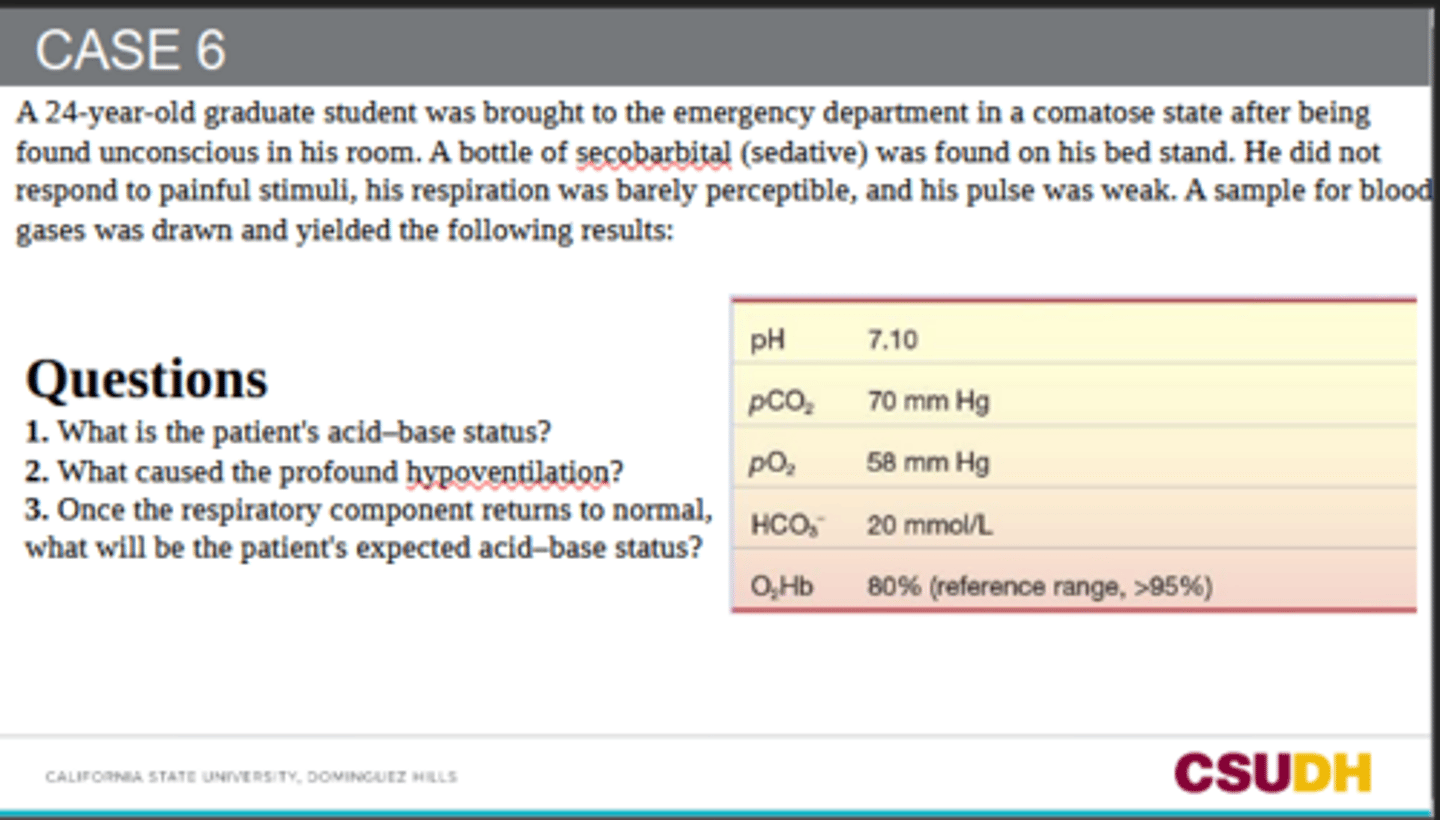
1) The patient has respiratory acidosis.
pH = 7.10 → acidotic
pCO₂ = 70 mmHg → high, causing the acidosis
HCO₃⁻ = 20 mmol/L → not elevated, so there is little/no compensation yet
2) The secobarbital overdose depressed the respiratory center in the brain, causing very slow/shallow breathing.
This made CO₂ build up in the blood.
3) The patient will likely have metabolic acidosis because HCO₃⁻ is low at 20 mmol/L.
Once pCO₂ is corrected back to normal, the remaining low bicarbonate may keep the pH low.
1. What is the patient's acid-base status?
2. What caused the profound hypoventilation?
3. Once the respiratory component returns to normal, what will be the patient's expected acid-base status?
At home in the Himalayas/high altitude:
pO₂: low
pCO₂: low from hyperventilation
pH: closer to normal or slightly high
HCO₃⁻: low, around 15 mmol/L, because kidneys excrete bicarbonate to compensate
In the US/lower altitude:
pO₂: increases
pCO₂: returns closer to normal
pH: normalizes
HCO₃⁻: increases back toward normal, here 24 mmol/L
At high altitude, the curve shifts right due to increased 2,3-BPG.
This helps hemoglobin release oxygen more easily to tissues.
1. How would his blood gases results (pH, pCO2, HCO3−) differ between home and the US?
2. Which direction does the oxygen dissociation curve shift at altitude?
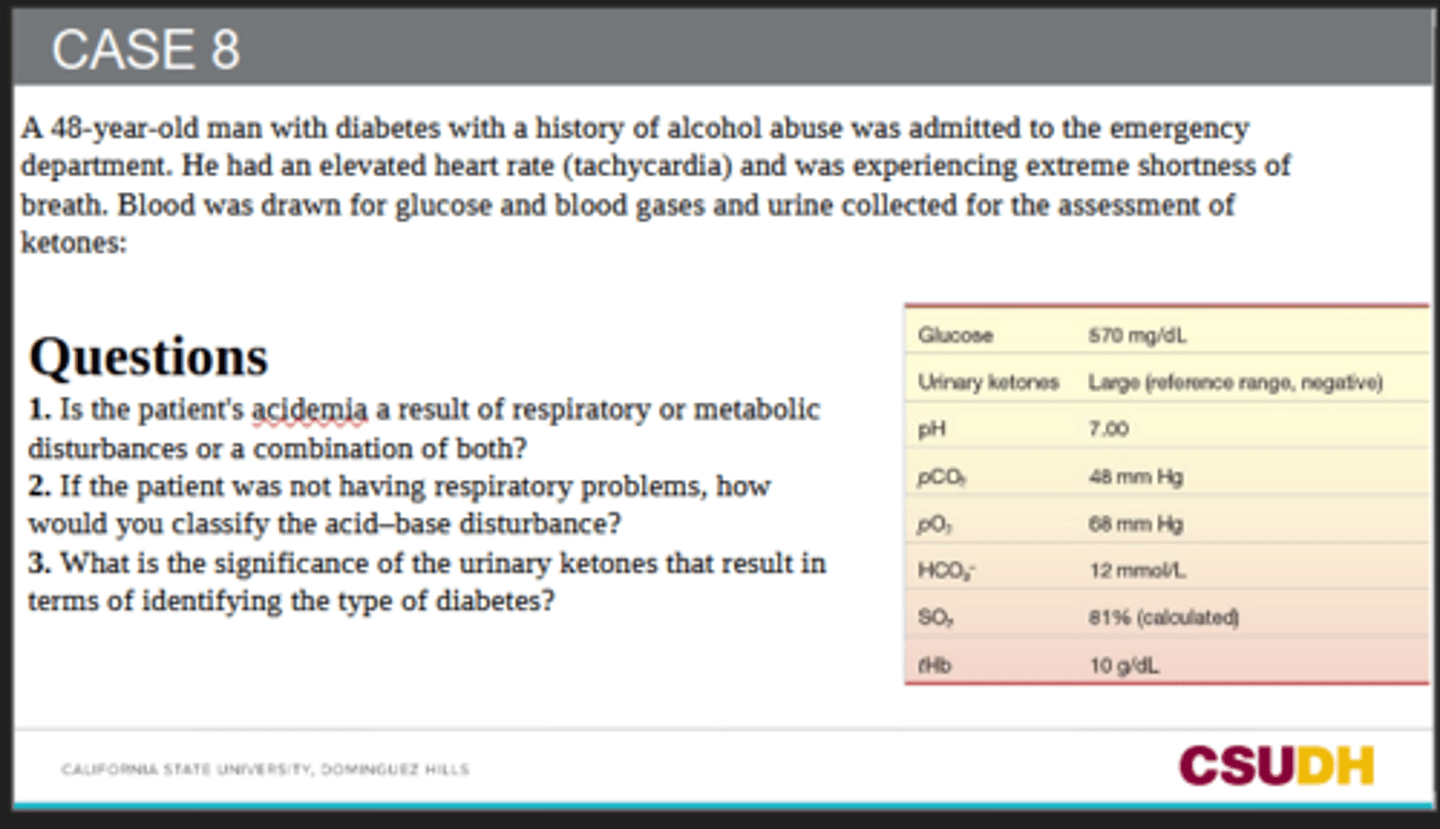
It is a combination of metabolic and respiratory acidosis.
pH = 7.00 → severe acidemia
HCO₃⁻ = 12 mmol/L → metabolic acidosis
pCO₂ = 48 mmHg → elevated, indicating respiratory acidosis
Large urinary ketones support ketoacidosis.
1. Is the patient's acidemia a result of respiratory or metabolic disturbances or a combination of both?
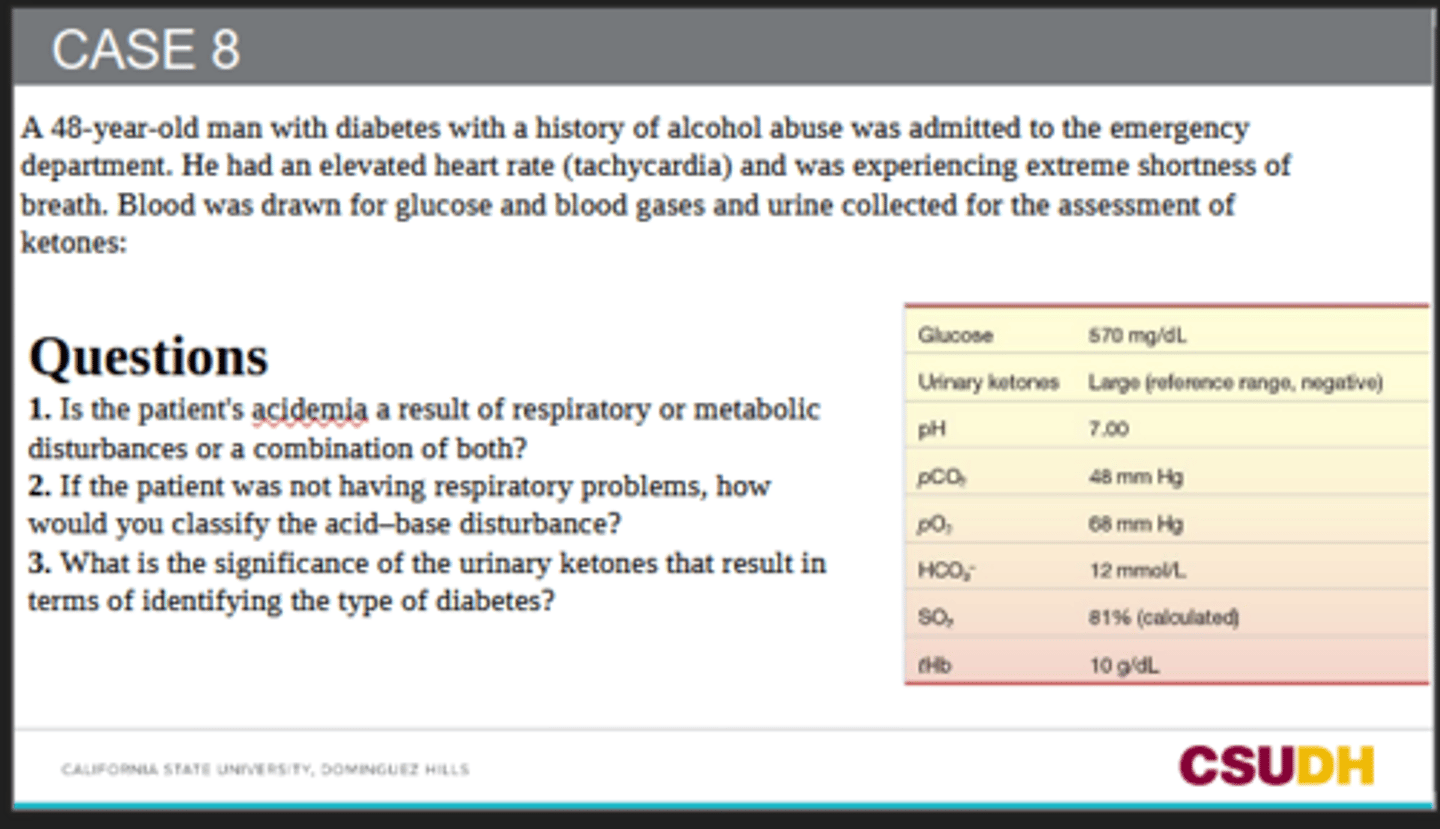
It would be classified as metabolic acidosis with respiratory compensation.
Normally, the lungs should hyperventilate to lower pCO₂ and compensate for the metabolic acidosis. However, this patient is retaining CO₂ instead.
2. If the patient was not having respiratory problems, how would you classify the acid-base disturbance?
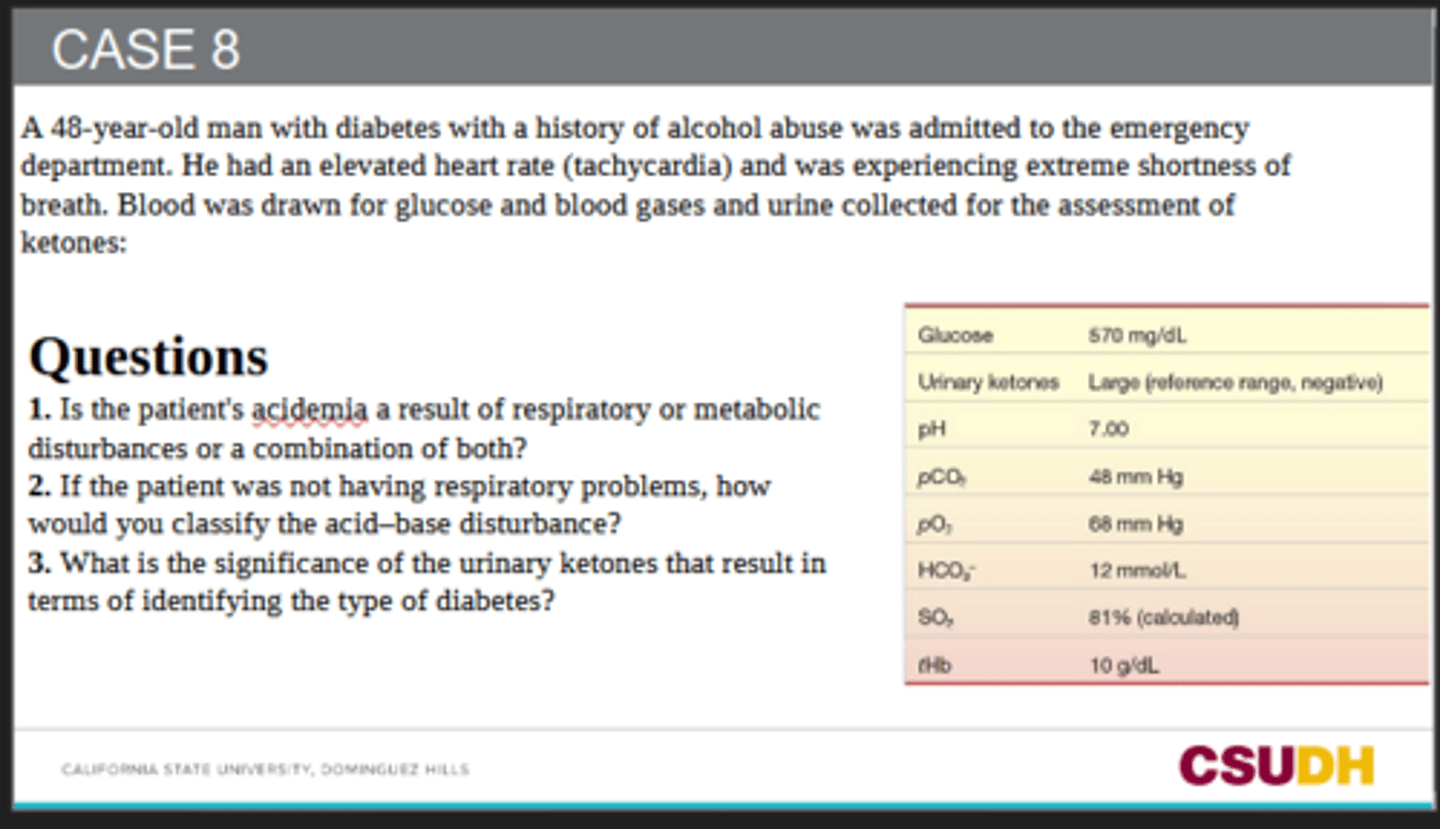
Large urinary ketones suggest diabetic ketoacidosis (DKA), which is more commonly associated with Type 1 diabetes.
Ketones indicate the body is breaking down fat for energy because there is insufficient effective insulin.
3. What is the significance of the urinary ketones that result in terms of identifying the type of diabetes?
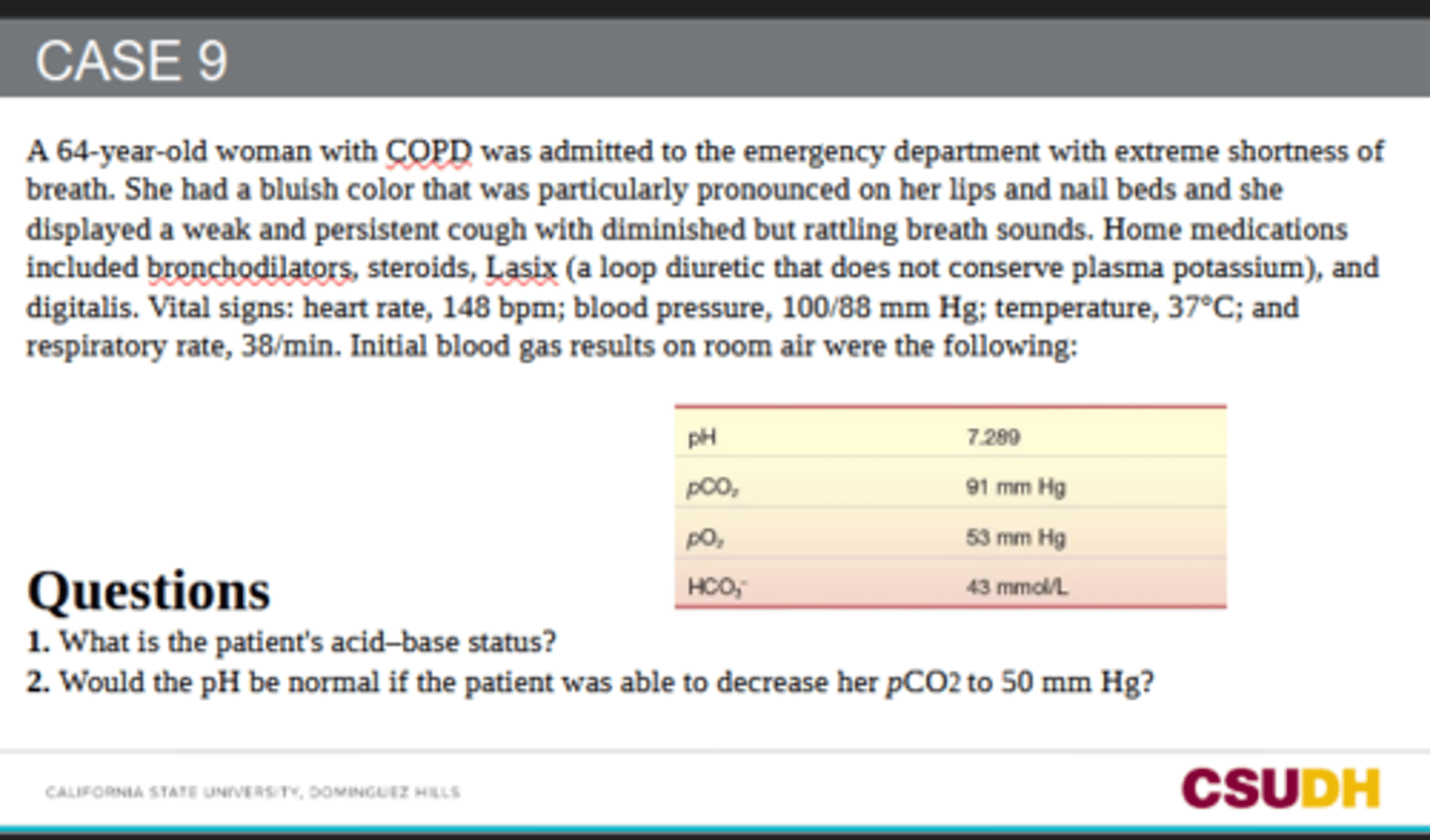
She has respiratory acidosis with metabolic compensation.
pH = 7.289 → acidotic
pCO₂ = 91 mmHg → very high, causing respiratory acidosis
HCO₃⁻ = 43 mmol/L → high, showing renal/metabolic compensation
1. What is the patient's acid-base status?
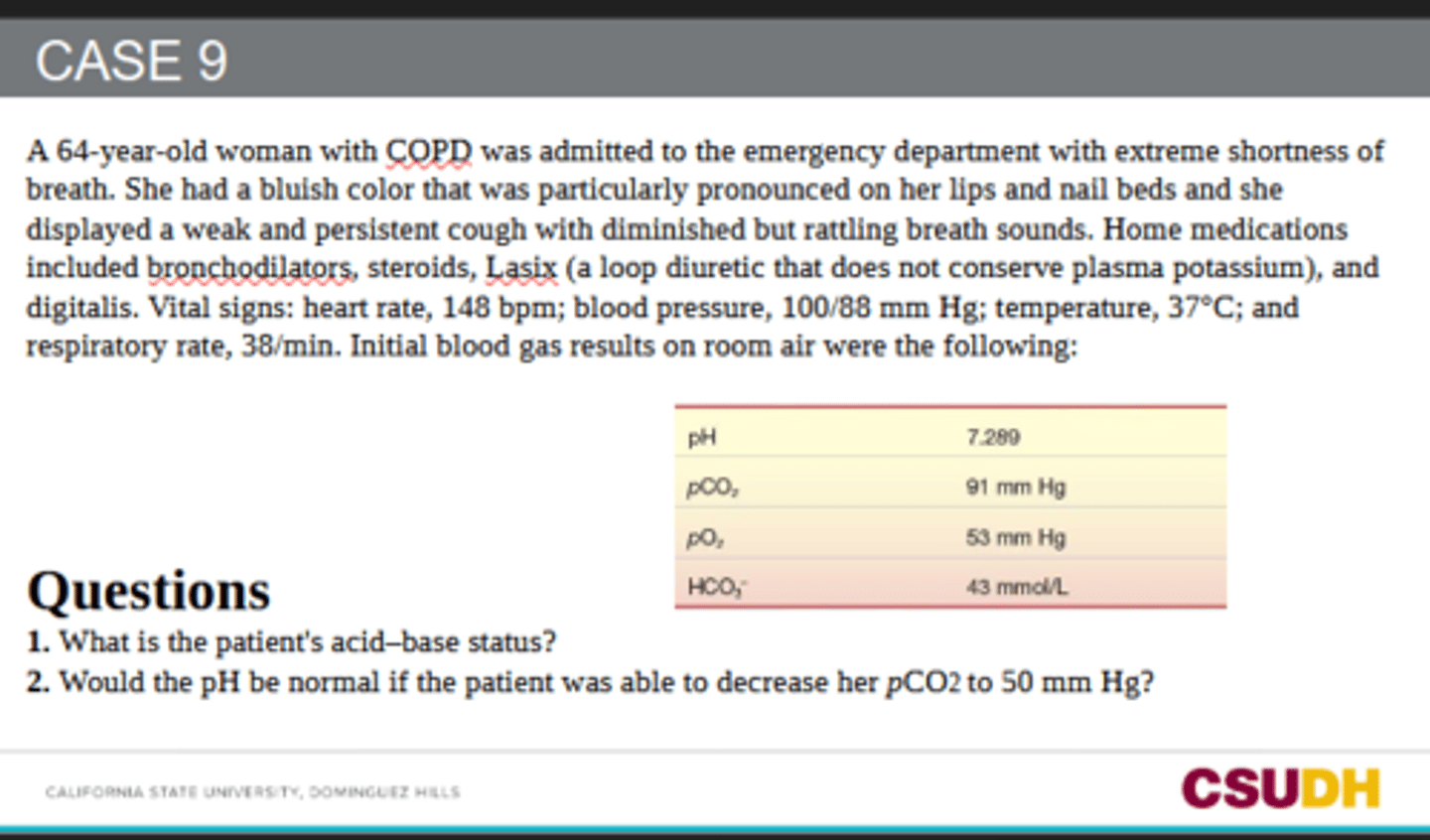
No. With HCO₃⁻ still high at 43 mmol/L, lowering pCO₂ to 50 would likely make the pH alkalotic, not normal.
Using the HH relationship: pH ≈ 6.1 + log(43 / (0.03 × 50)) ≈ 7.56
So she would have metabolic alkalosis from the elevated bicarbonate.
2. Would the pH be normal if the patient was able to decrease her pCO2 to 50 mm Hg?