Patho/Pharm 2 (CH 4) - Neurological Drugs PT 2 CONTINUED
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
atypical antidepressant
Bupropion
Bupropion MOA
atypical antidepressant inhibtits dopamine reuptake
primary use for Bupropion
- depression
- seasonal affective disorder
- adjunct therapy for smoking cessation
seasonal affective disorder
a person experiences depression during winter months and improved mood during spring.
pt education taking Bupropion
- N/V/GI distres (take w/ food)
- weight loss
- high-risk seizures
CNS EFFECTS:
- insomnia
- agitation
- tremors
- psychosis effects (higher in children)
nursing care for pts taking Bupropion
- weight monitoring
- monitor CNS effects (report is symptoms occur)
- monitor psychosis effects
- montior seizure risk/seizure precautions
- do not crush med
cautionary pts on Bupropion
- hx liver/kidney dysfunction
- cardiac disesases
- szhizophrenia
- bipolar disorder
- diabetes
- hx alc abuse
- cimetidine (lowers effectiveness)
contraindications for taking Bupropion
- allergy
- suicidal thoughts
- hand tremors
- CNS tumors
medications contraindicated w/ Bupropion
- MOAI <14days last dose
antiseizure medications:
- phenytonin
- phenybarbital
- carbamepazine
mood stabilizer
Lithium
Lithium MOA
mood stabilizer
- #1 preferred bipolar medication
primary use for Lithium
- acute manic episodes
- bipolar disorder
- preventative for manic/depressive episodes
pt education taking Lithium
- GI upsest
- fatigue
- headache
- confusion
- memory impairment
- polyuria
- high risk hyperthyroidism/thyroid storm/goiter
- Lithium toxicity s/s
- s/s of low lithium levels
- hyponatremia worsens lithium toxicity --> increase fluids 2-3L/day
lithium toxicity levels vs lithium withdrawel levels
> 1.2 = severe lithium toxicity
< 0.6 = withdrawel/ manic episodes
nursing priorities for pts taking Lithium
- monitor lithium levels agressively
- I/O
- electrolyte levels
- hyperthyroidism s/s
- monitor tumor growths
- kidney function tests
- take w/ milk + food
- do not crush
Hyperthyroidism
overactivity of the thyroid gland causing:
- lethargic
- bradycardia
- low body temp
cautionary pts taking Lithium
- hx thyroid issues
- hx seizures
- diabetes
- urinary retention issues
- suicidal thoughts
- older adults
contraindications for taking Lithium
- pregnancy (teratogenic fetal heart defects during 1st trimester)
- lactating
- renal insufficiency
- cardiac disorder
- dehydration/hyponatremia
- hx angioedema
medications contraindicated w/ Lithium
- NSAIDS (besides aspirin)
TOXICITY LEVELS:
- tetracyclines
- diuretics
- meldopa
- probenacid
- antihypertensives
INCREASES URINARY RETENTION
- phenothiazine
- haloperidol
traditional antipsychotics
chlorpromazine
haloperidol
chlorpromazine/ haloperidol MOA
- 1st generation traditional antipsychotic
- blocks CNS receptors
primary use for chlorpromazine/ haloperidol
- schizophrenia
- manic episodes bipolar disorder
pt education taking chlorpromazine/ haloperidol
- AKATHISIA
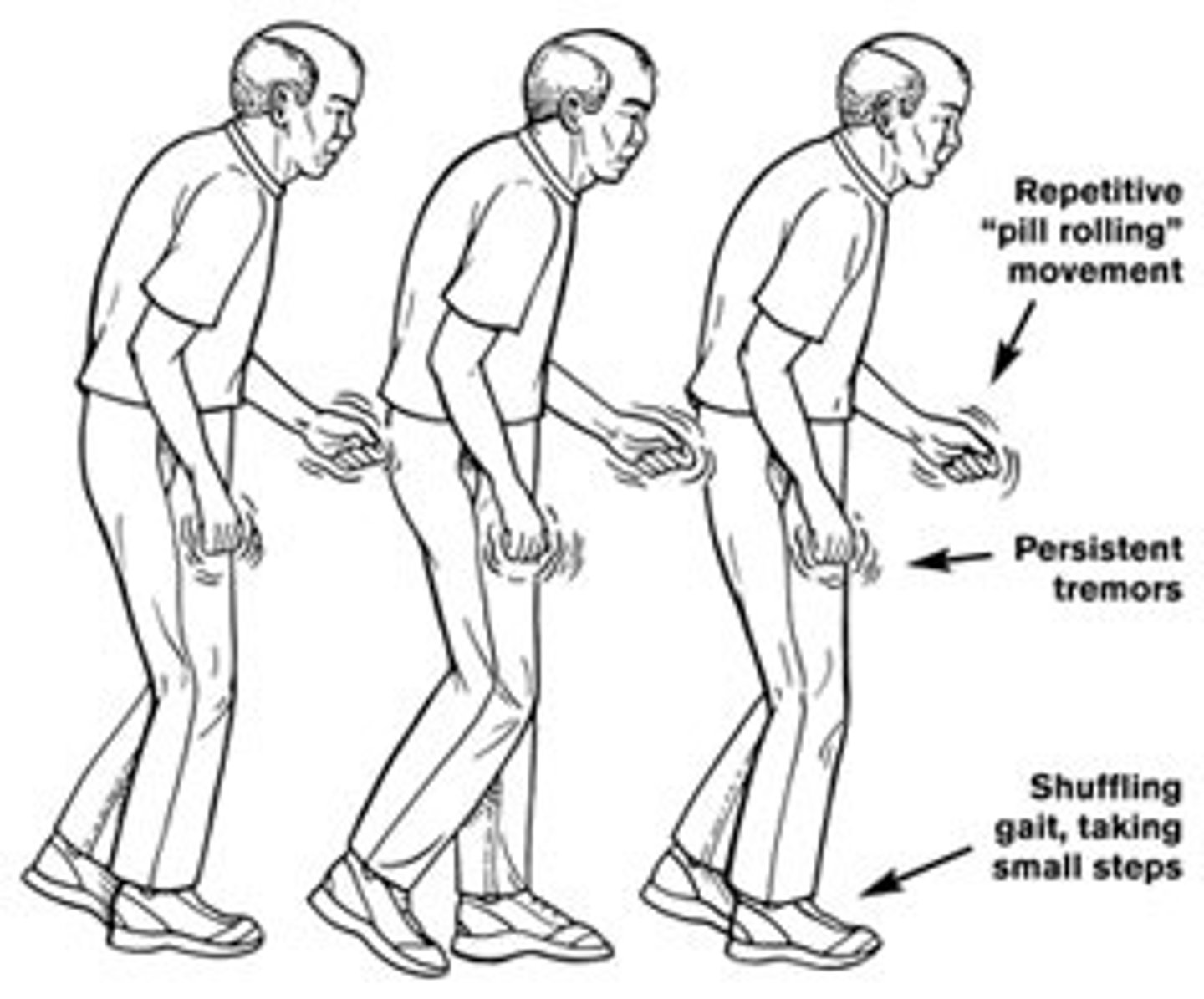
- PARKINGSONSISMS
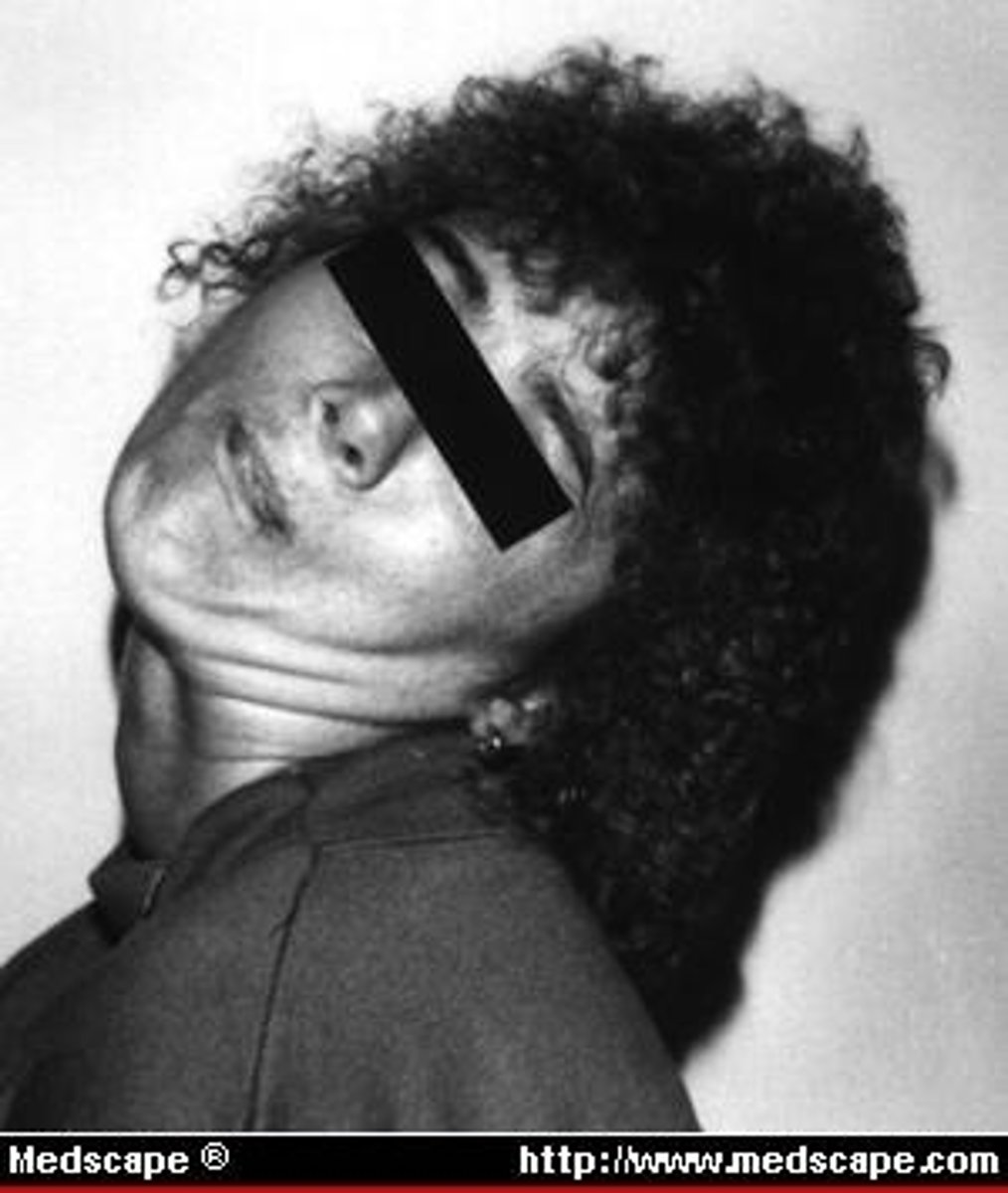
- ACUTE DYSTONIA
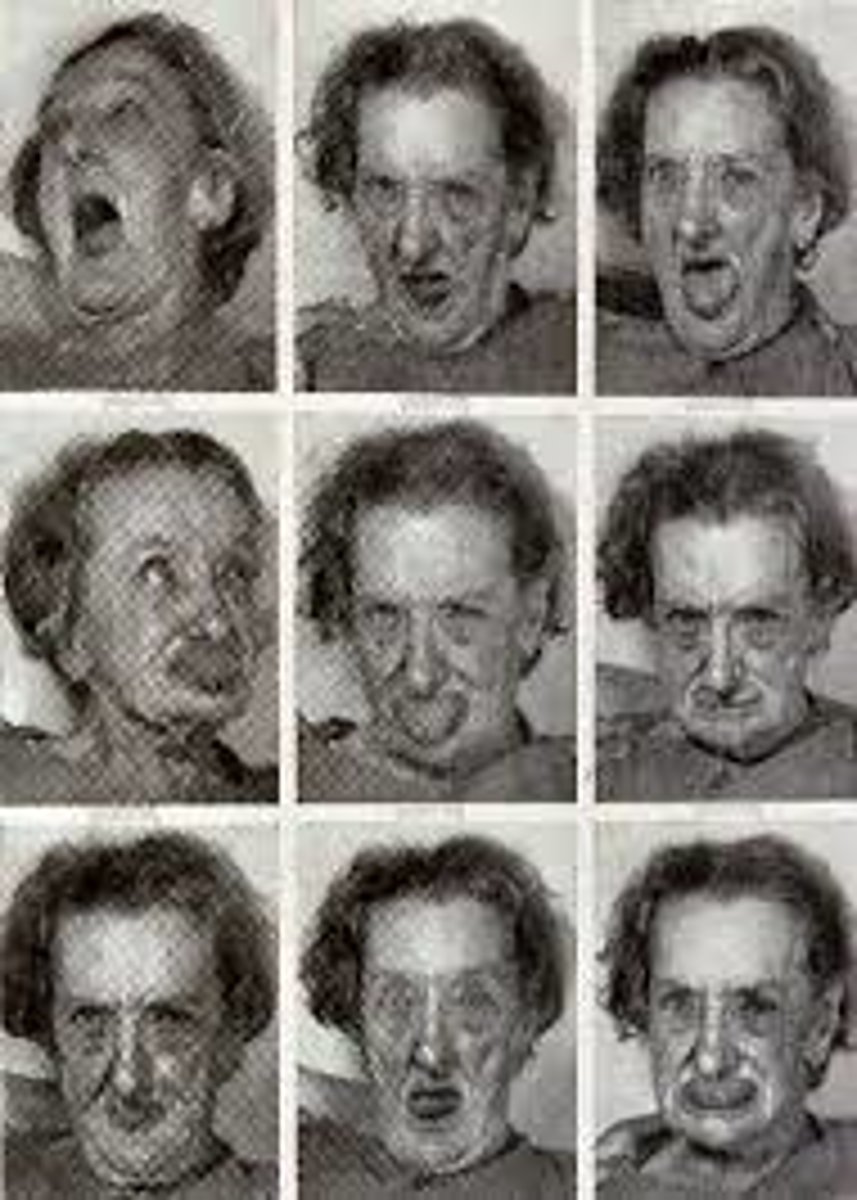
- TARDIVE DYSKINESIA
- sexual dysfunction
- severe dysrhythmias
- dermatitis
- neurolytic malignant syndrome
- anticholinergic effects
akathisia education for pts on chlorpromazine/ haloperidol
- within 2 months med therapy
- med can still be continued even if symptoms progress
causes =
- uncontrolled constant movements
- restlessness

parkingsonsisms education for pts on chlorpromazine/ haloperidol
- within 1st month med therapy
- parkinsons meds can reduce manifestations
- contraindicated w/ levidopa/carbidopa (neurtilizes antipsychotic effects)
causes =
- rigidity
- tremors
- sluggishness
acute dystonia education for pts on chlorpromazine/ haloperidol
- within first few hrs --> days med therapy
- anticholingerics help this effect
- requries IMMEDIATE ATTENTION
causes =
- severe painful muscle spasms
- neck/body spasms
tardive dyskinesia education for pts on chlorpromazine/ haloperidol
- within months to years med therapy
- decrease dose to lower effects
- IN SOME CASES tardive dyskinesia CAN BE PERMANENT
causes =
- withering movements of tongue and neck
neurolytic malignant syndrome
life threatening RARE manifestation of traditional antipsychotic med therapy (specifcally haloperidol/chloropomazine) causes =
- high fever
- muscle rigidity
- usstable vitals
- loss of consciousness
nursing care for pts taking chlorpromazine/ haloperidol
- monitor muscle disorder s/s
- Beta-blockers/ benzos help muscle manifestations
- Monitor anticholinergic effects
- monitor sexual dysfunction
- frequent vital signs/ EKG checks
- Wear gloves
- Keep pt in recumbent 30 min after IM/IV therapy
- CHECK COMPATIBILITY W/ OTHER MEDS
neurolytic malignant syndrome nursing care
fever > 105 =
- cold compresses
- aspirin/acetaminophen
- IV dantrolene/bromocriptine
contraindications for chlorpromazine/ haloperidol
- allergy
- alc withdrawels
- bx bone marrow supression
- CNS depressants
- pregnancy
- lactation
cautionary pts taking chlorpromazine/ haloperidol
- hx COPD
- hx glaucoma
- diabetes
- liver dysfunction
- thyroid disorders
- protate hypertrophy
- HTN
MEDS 2hrs before:
- CNS depressants
antacids
antidiarrhea
2nd generation antipsychotic
risperidone
risperidone MOA
2nd generation antipsychotic
- blocks dopamine receptors + serotonin
primary use for risperidone
- schizophrenia
- bipolar episodes
- autism
pt education taking risperidone
CNS effects:
- drowsiness
- insomnia
- dizziness
EXTRAPYMIDAL effects:
- weight gain
- dyskinesdia
- akathesia
- parkinsonsims
nursing care for pts taking risperidone
- monitor CNS effects
- monitor extrapymidal effects/report immediatly
- weight check
- avoid w/ soft drinks/tea/caffine
contraindications for taking risperidone
- allergy
- lactation
- severe CNS disorders
- dementia psychotic episdes
- stroke risk
- children <13y/o
- parkinsons disease
- hx live/kidney disorders
- antihypertensives (antipsychotic increase toxicity)
cautionary medications w/ risperidone
LOWERS EFFECTIVENESS:
- phenytoin
- carbamepazine
- clozapine
- phenobarbital
- rifampin