Mayo - Aortic Regurgitation
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
33 Terms
Acute AR vs Chronic AR — which will not show an impressive color jet?
Acute AR may not show a color jet and may need to diagnose with high clinical suspicion, with a vena contract or TEE
FYI LV is usually NOT DILATED in acute AR
Is end diastolic stress high or low in AR
High — implying volume overload (MR leads to this too)
Unlike MR, AR causes peak systolic stress and end systolic stress. What does this tell us?
Aortic regurgitation is a PRESSURE AND VOLUME overload problem (FYI almost never too late to operate on AR).
MR is just a VOLUME overload problem (FYI causes eccentric LVH, LV dilation, low after load).
Remember pressure has to do with _____. While volume has to do with ______.
Pressure = afterload
Volume = preload
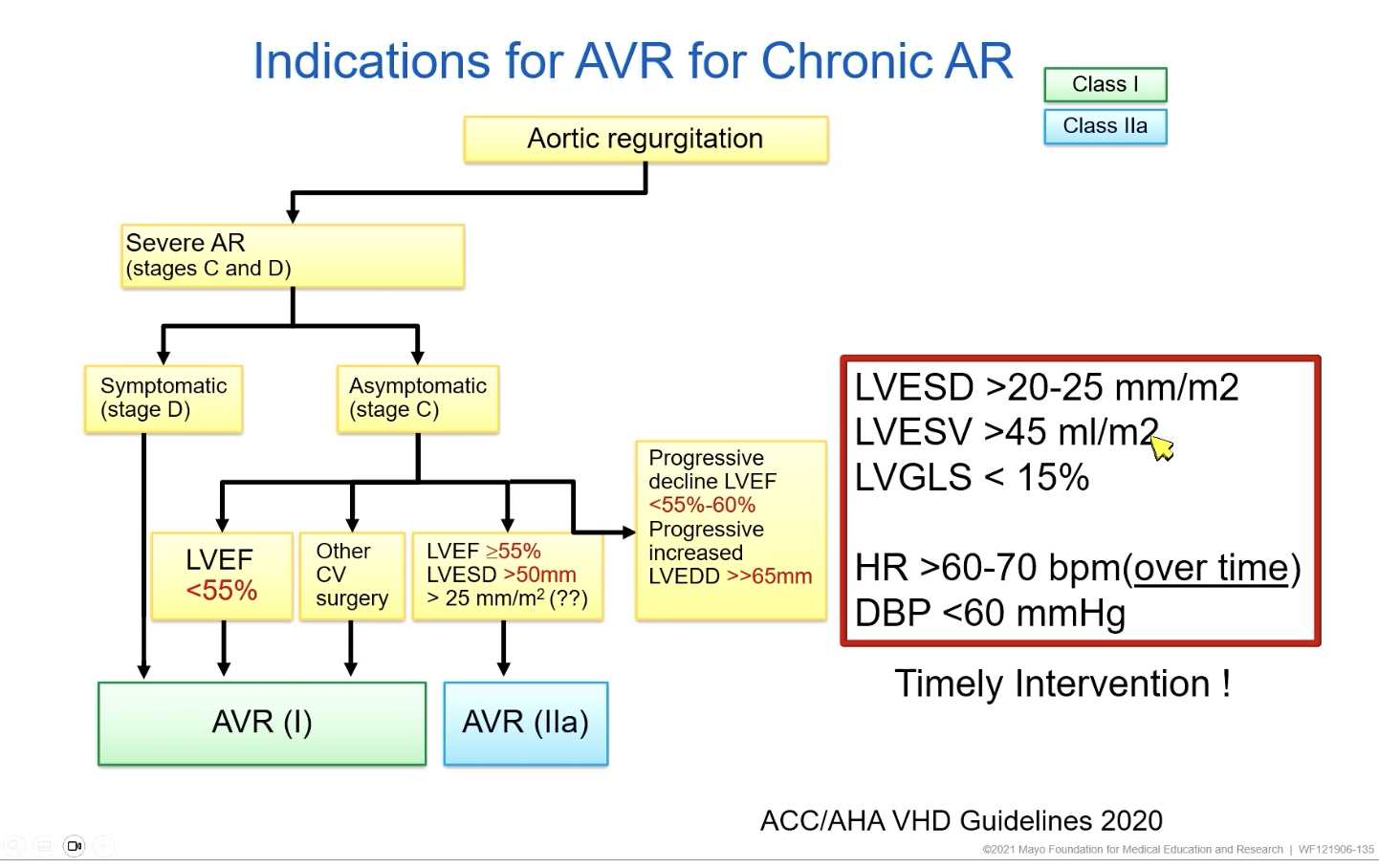
Prognosis without surgery of AR is very poor. But what is the LVEF cutoff for surgery in symptomatic AR patients?
New guidelines — even if EF < 25% they may benefit. So it is REGARDLESS of how low the EF is
If you are asymptomatic AR — you have to monitor with echo closely.
How often do you do an echo for asx mild AR?
How often do you do an echo for asx moderate or severe AR?
Mild AR — every 3 years
Moderate or severe AR — every 12 months
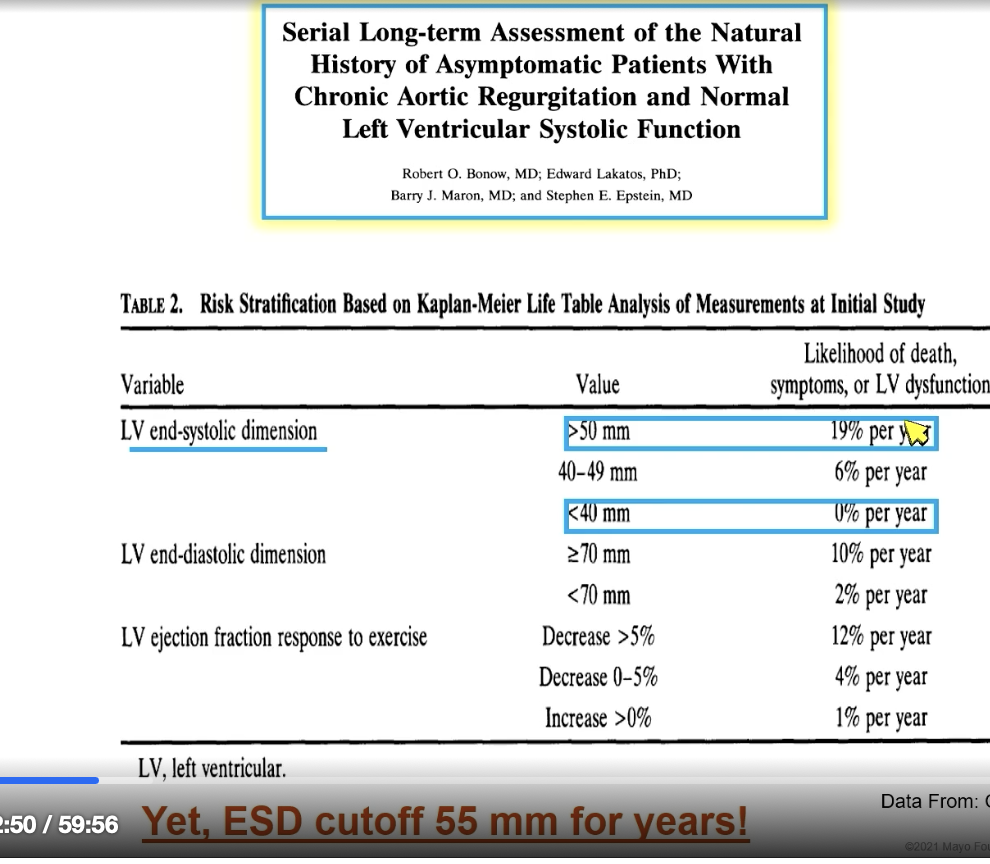
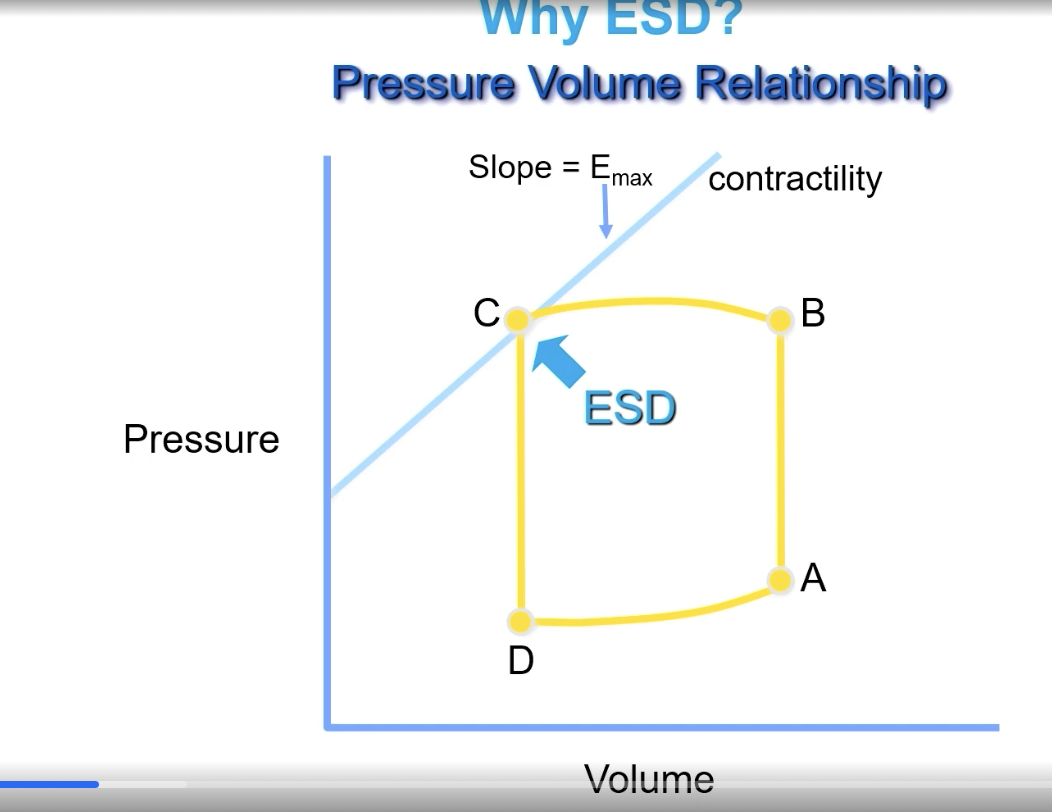
End systolic diameter is the “poor mans” measurement of…
contractility
FYI this is because people die of sudden cardiac death (typically young Males) from this— but then how can you predict who will die faster? Well, LV end systolic dimension. Value of > 50 mm associated with higher likelihood of death.
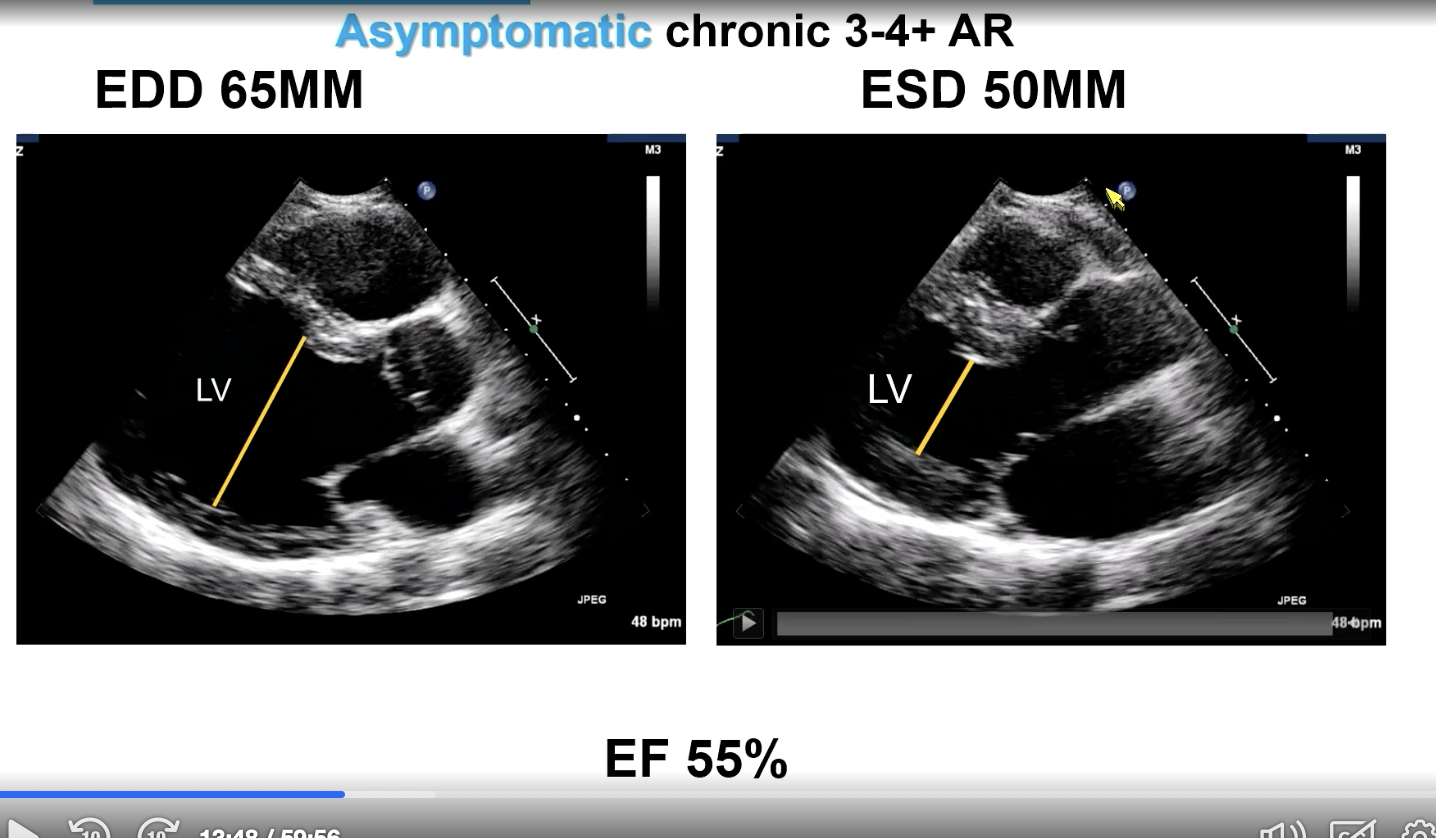
For asymptomatic chronic 3-4+ aortic regurgitation, what is the end diastolic LV diameter and end systolic LV diameter cut offs (assuming EF 55% or more)
EDD — 65 mm
ESD — 50 mm
Measure in parasternal long
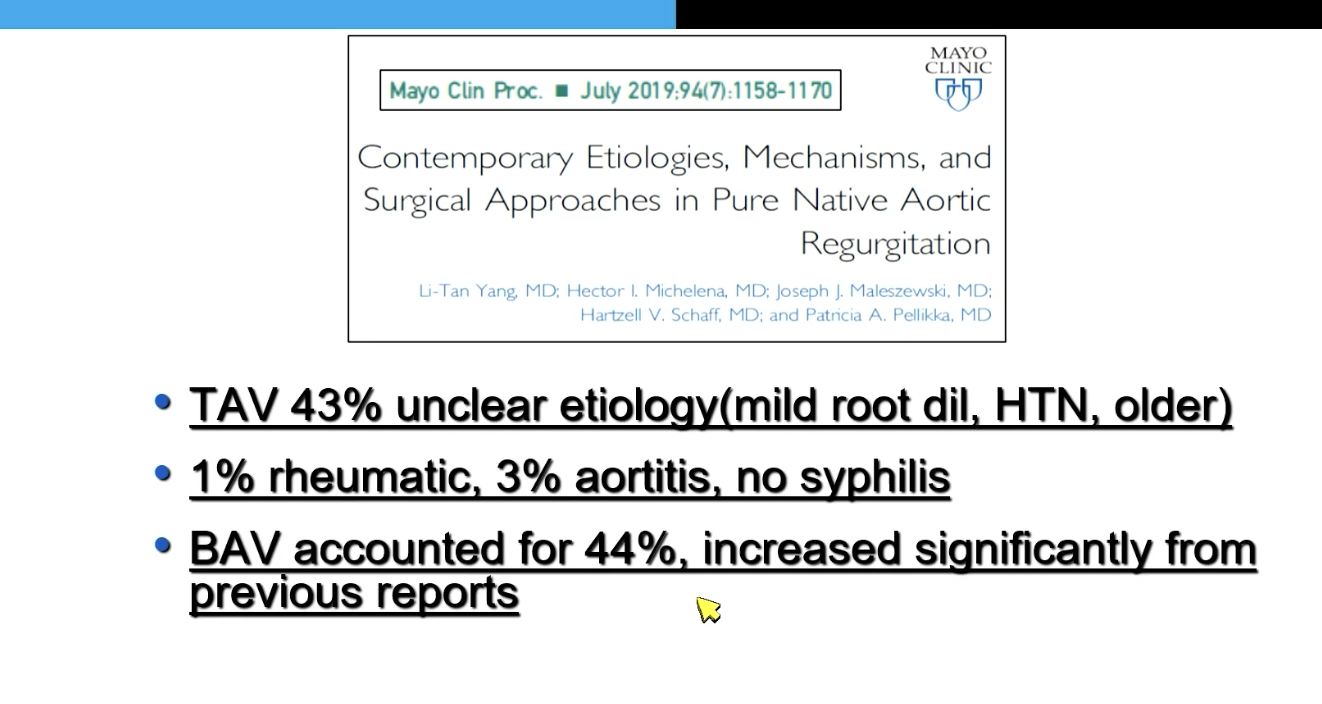
44% of pure native aortic regurgitation is accounted for by…
Bicuspid aortic valve
What three things do you look at for chronic aortic regurgitation for evaluation and follow-up on echo?
Define anatomy (BAV vs tricuspid AV)
Mechanism/severity
LOOK AT THE AORTA
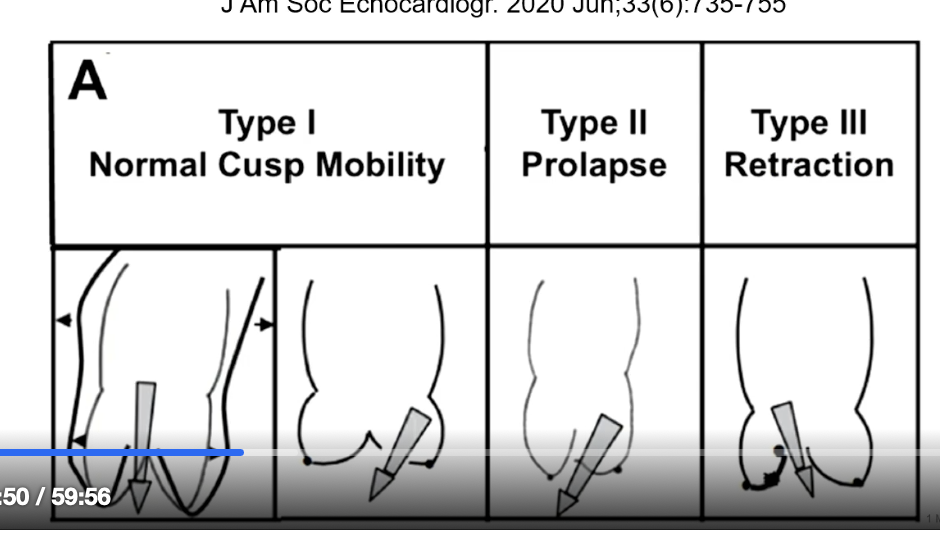
Type I AR cause
Normal cusp mobility
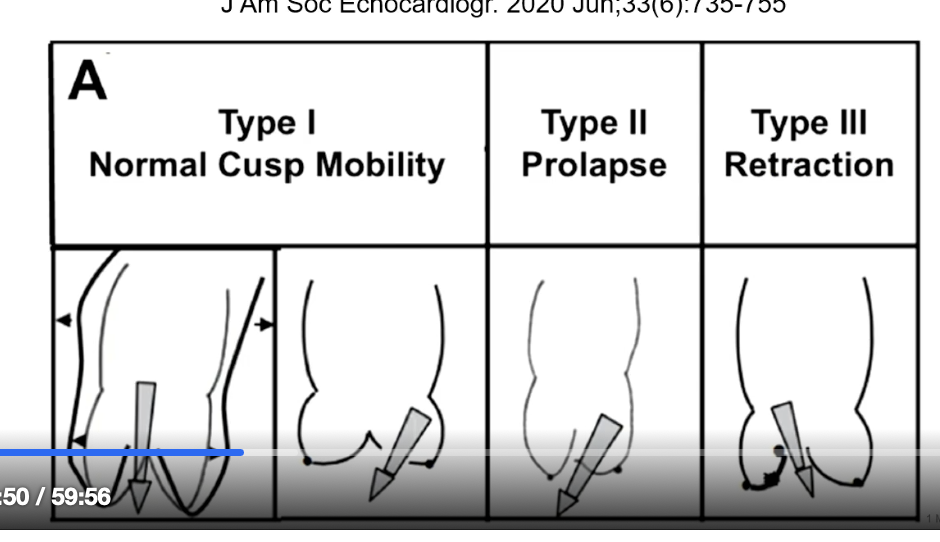
Type II ART cause
prolapse
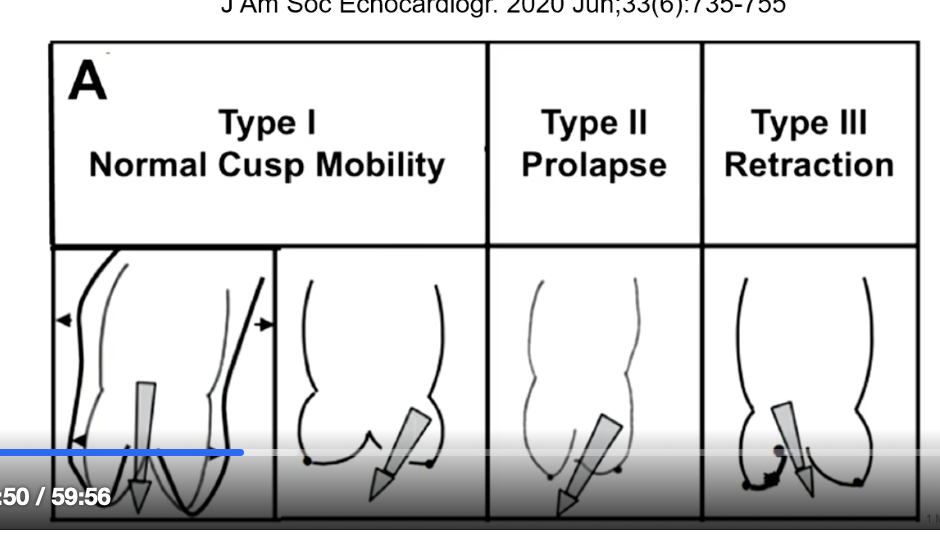
Type III AR cause
Retraction
To define chronic significant (>/= 3) AR, what must you have?
BIG LV
Define this by
ESD
EDD
LV Volumes
or just get a cMRI
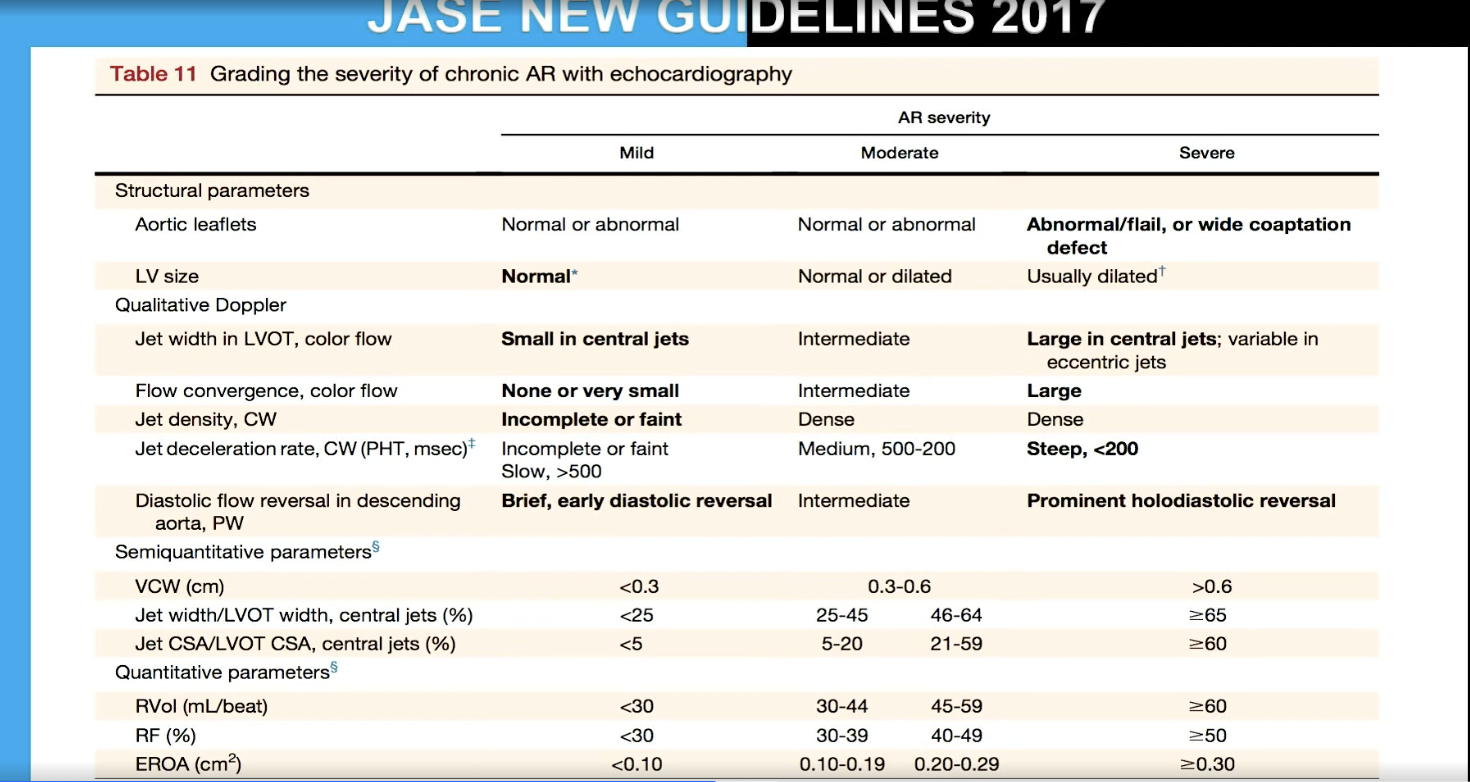
What parameters to define 3/4+ AR?
Vena Contracta
Supportive signs include — flow diastolic reversal in the aorta and PHT
Quantitative parameters
ERO
RVol
RF (compares severity of the vol overload relative to size of the ventricle)

In PW aorta, shows brief early diastolic reversal
Mild AR (versus severe which has prominent holodiastolic reversal)
What is pressure half time in severe AR? What is the caveat?
Steep < 200
FYI caveat is that if you have CHRONIC severe AR that is compensated, it won’t be that fast?? PHT is good in acute AR. The pitfall of using PHT for AR is that is depends on LV and Ao pressure.
Vena contracta is the smallest diameter you can measure between…
the flow convergence (“the head” or the starting chamber of the jet; for AR would be in aorta) and the jet (“the legs” or in the chamber the jet goes to)
Vena contract for mild AR
< 0.3 cm
Vena contracta for severe AR
>/= 0.6 cm
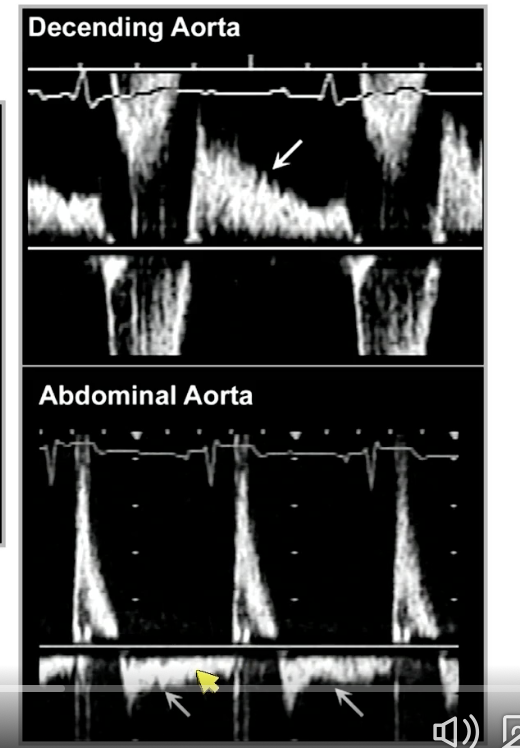
holodiastolic flow reversal in aorta — severe AI
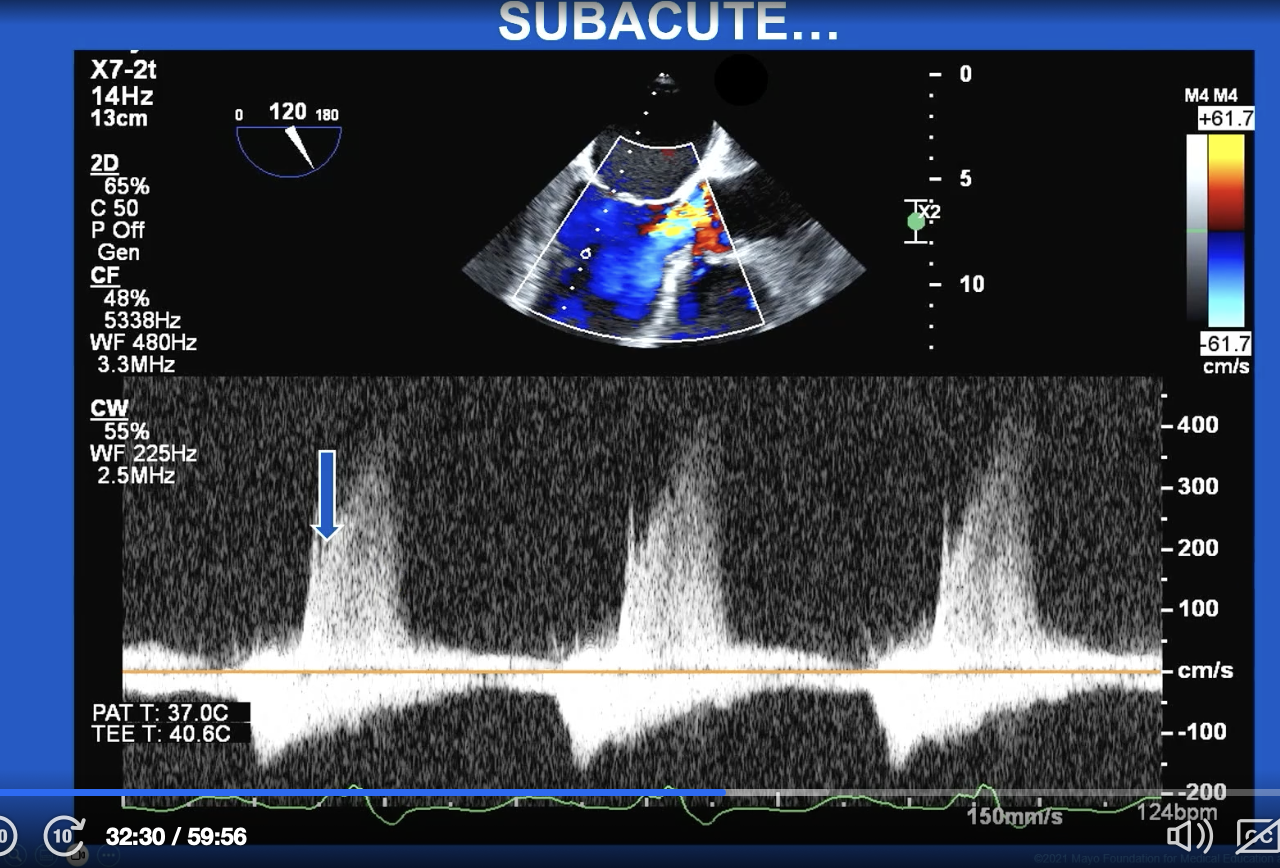
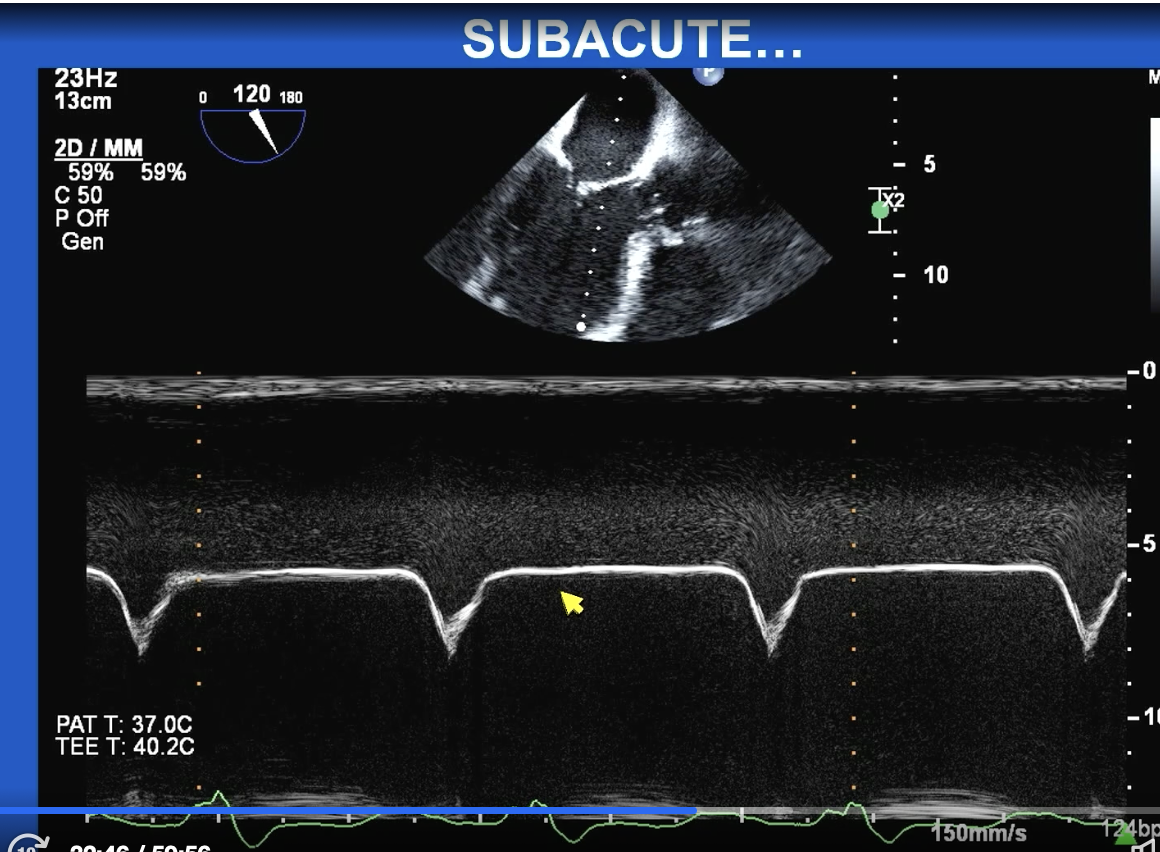
Subacute AR
— First picture arrow is showing early closure of the mitral valve and after it shows some end diastolic MR
— M Mode of mitral valve shows this “M” sign type thing but basically the AR is so bad that it shuts the mitral valve for so long because the pressure in the LV is so overwhelming.
Severe AR by ERO
> 0.3 cm2
FYI both severe AR and MR have same regurgitant volume but severe AR is considered >0.3 cm2 and severe MR is considered with >0.4 cm2 is because AR occurs during diastole. Thus, you only need a smaller hole to leak 60 cc because diastole is LONGER.
FYI for TR, severe is considered ERO > 0.4 cm2 but the RVOL is 45 cc and this is because you just need that size hole to release 45 cc and that is considered a lot of volume on the low pressure side of the heart
Severe AR by regurgitant volume
>60 cc per beat
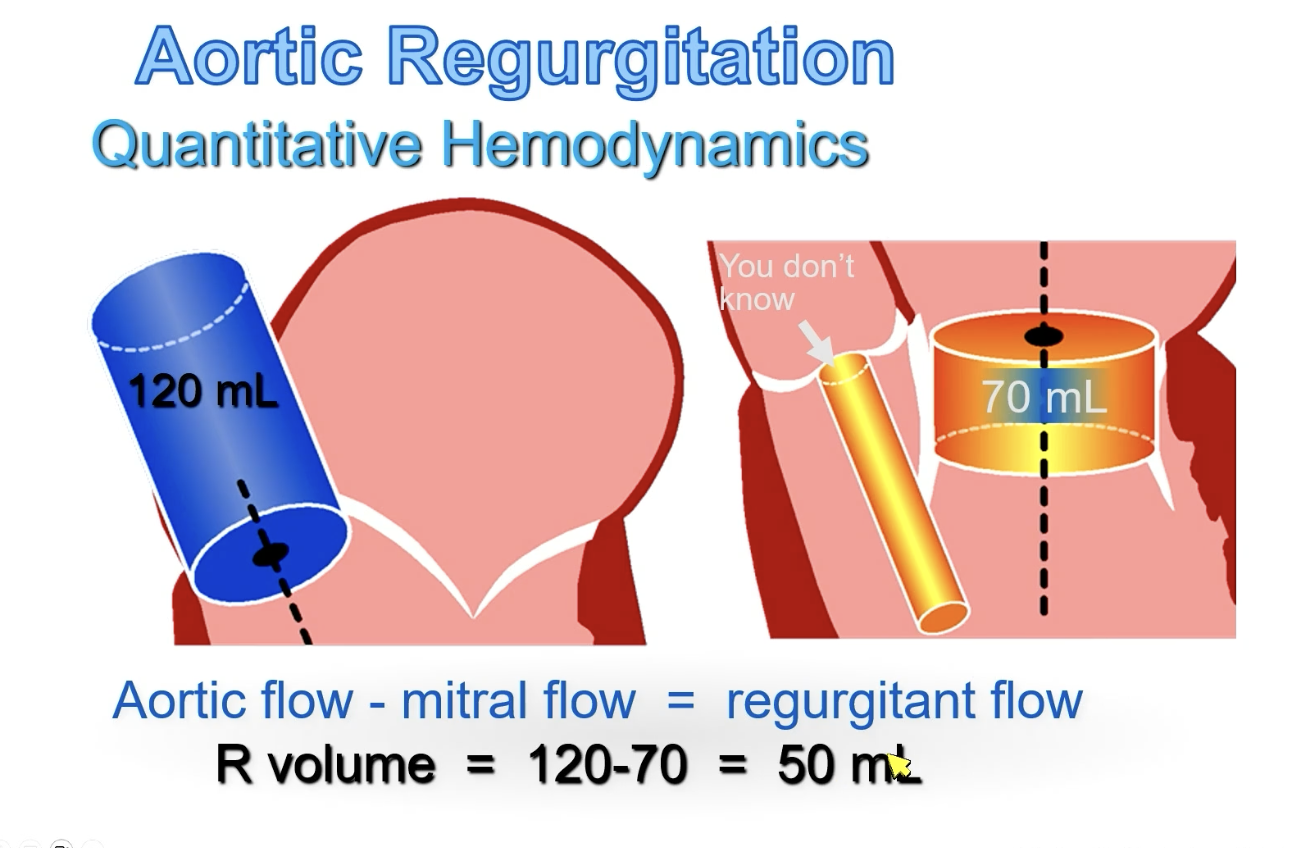
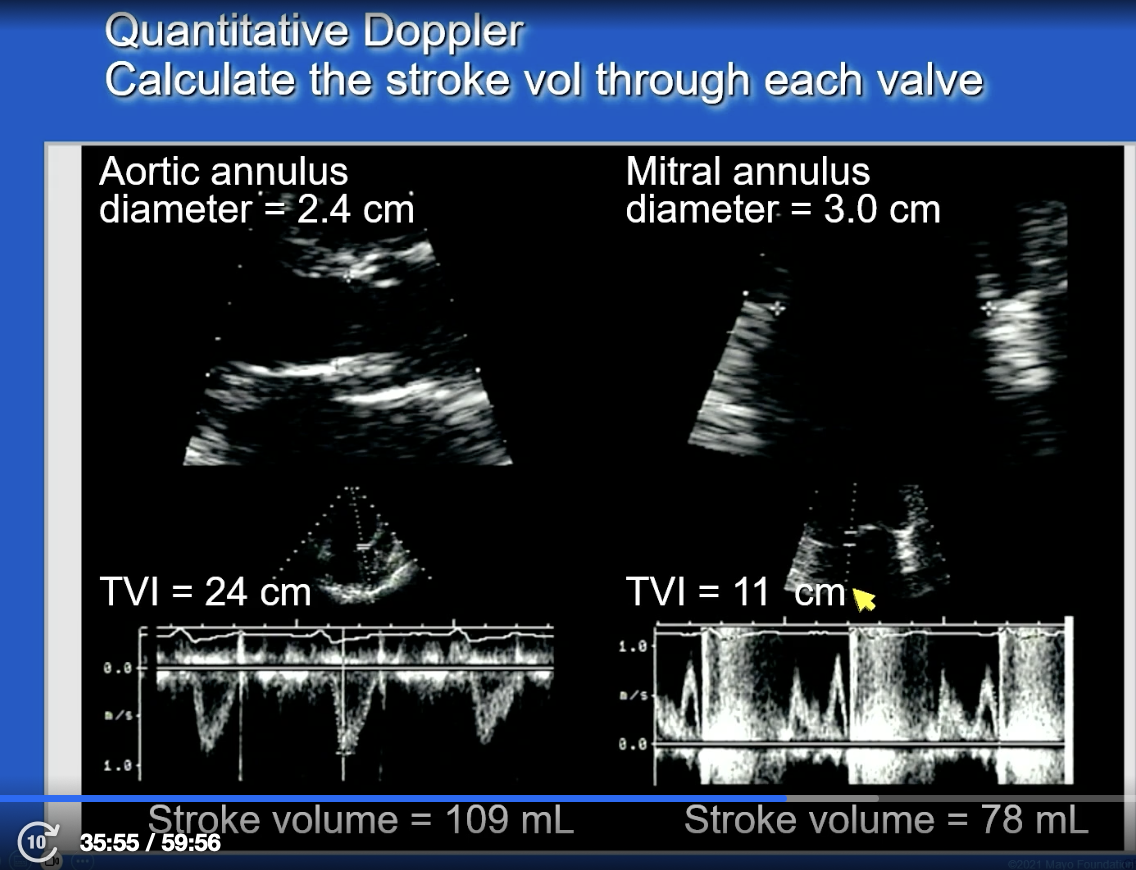
Don’t forget
shortcut for SV is
SV = 0.785(diameter)2 x VTI
FYI:
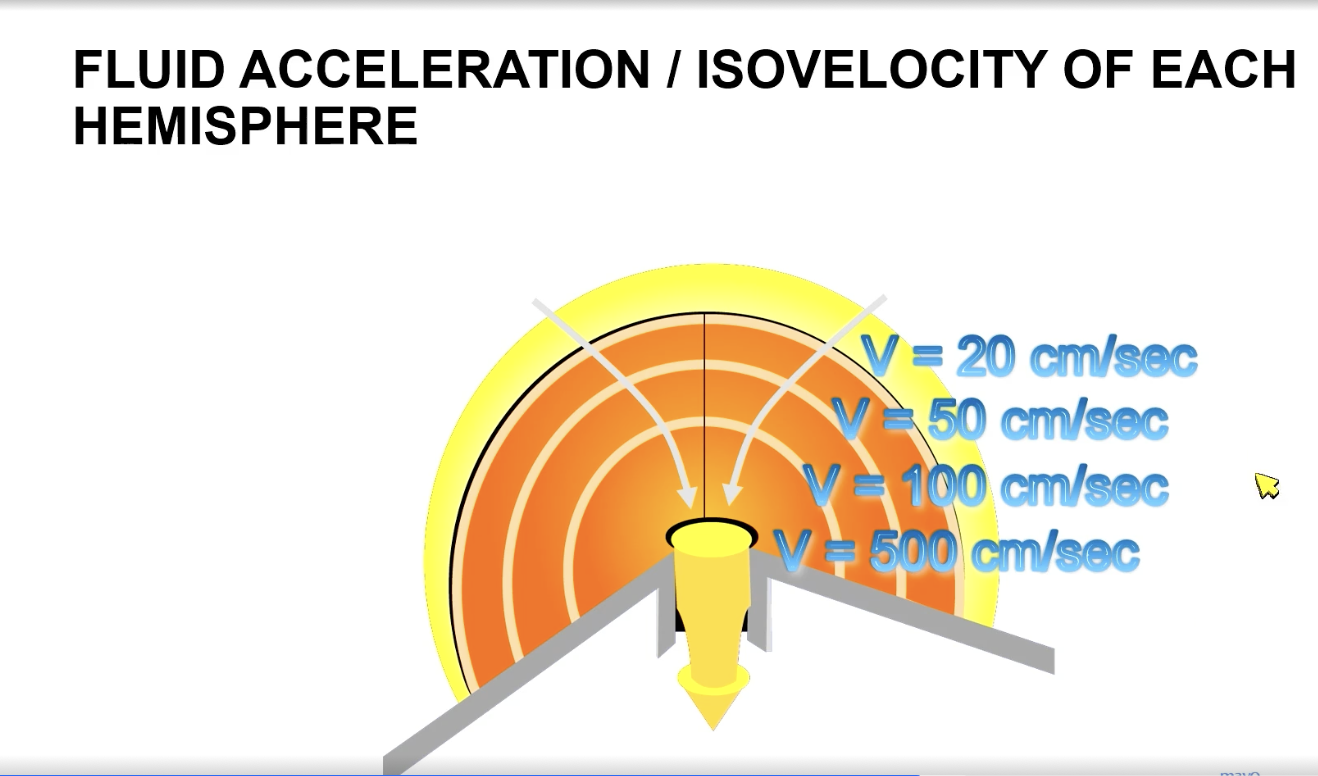
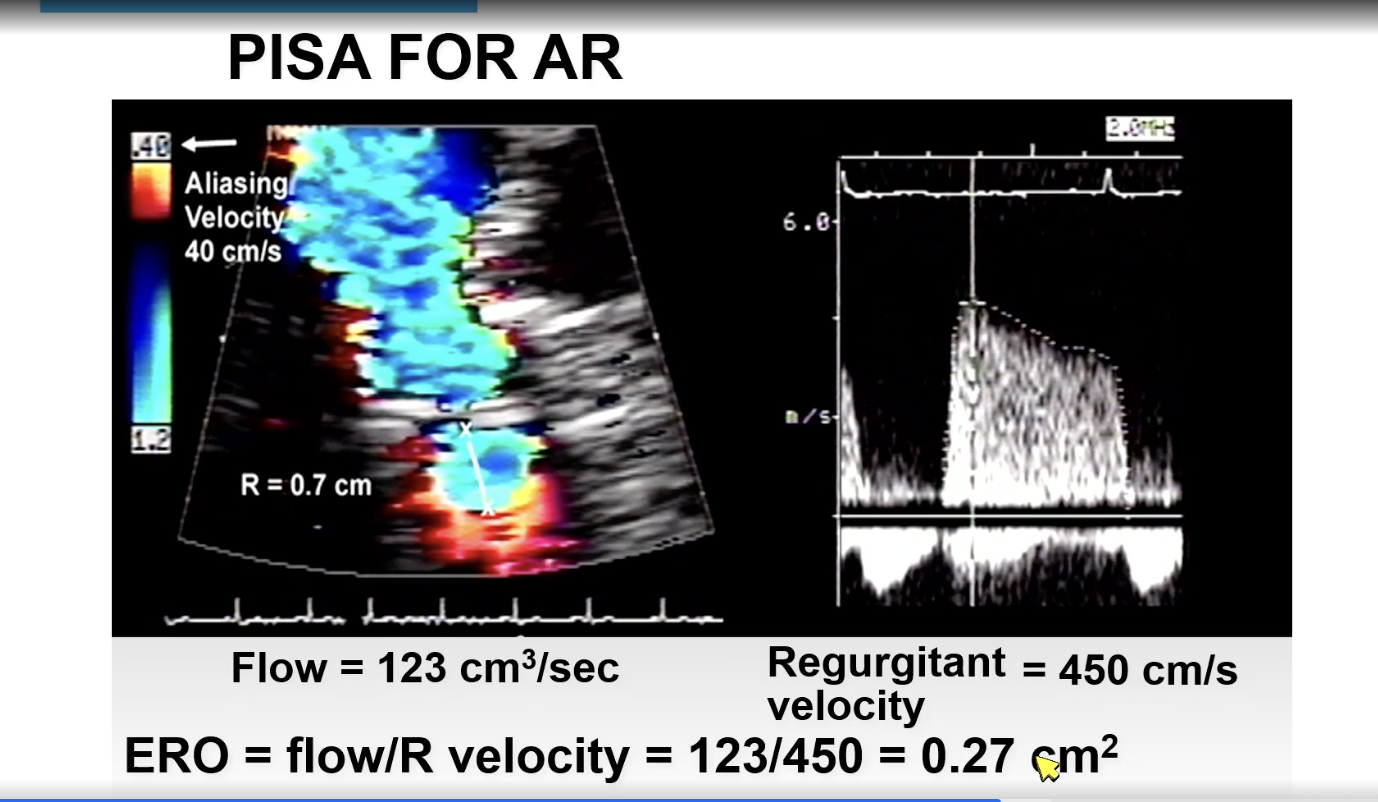
For PISA, as flow is going through a narrow orifice, it produces hemispheres. The velocity within each hemisphere is the same. The hemispheres closest to orifice will be fastest.
FYI must measure parallel (versus VC of AR you get perpendicular in PLAX). FYI in an eccentric jet, may have to find weird views to get parallel to the jet for a PISA
FYI you move the aliasing velocity baseline bar in direction of the jet
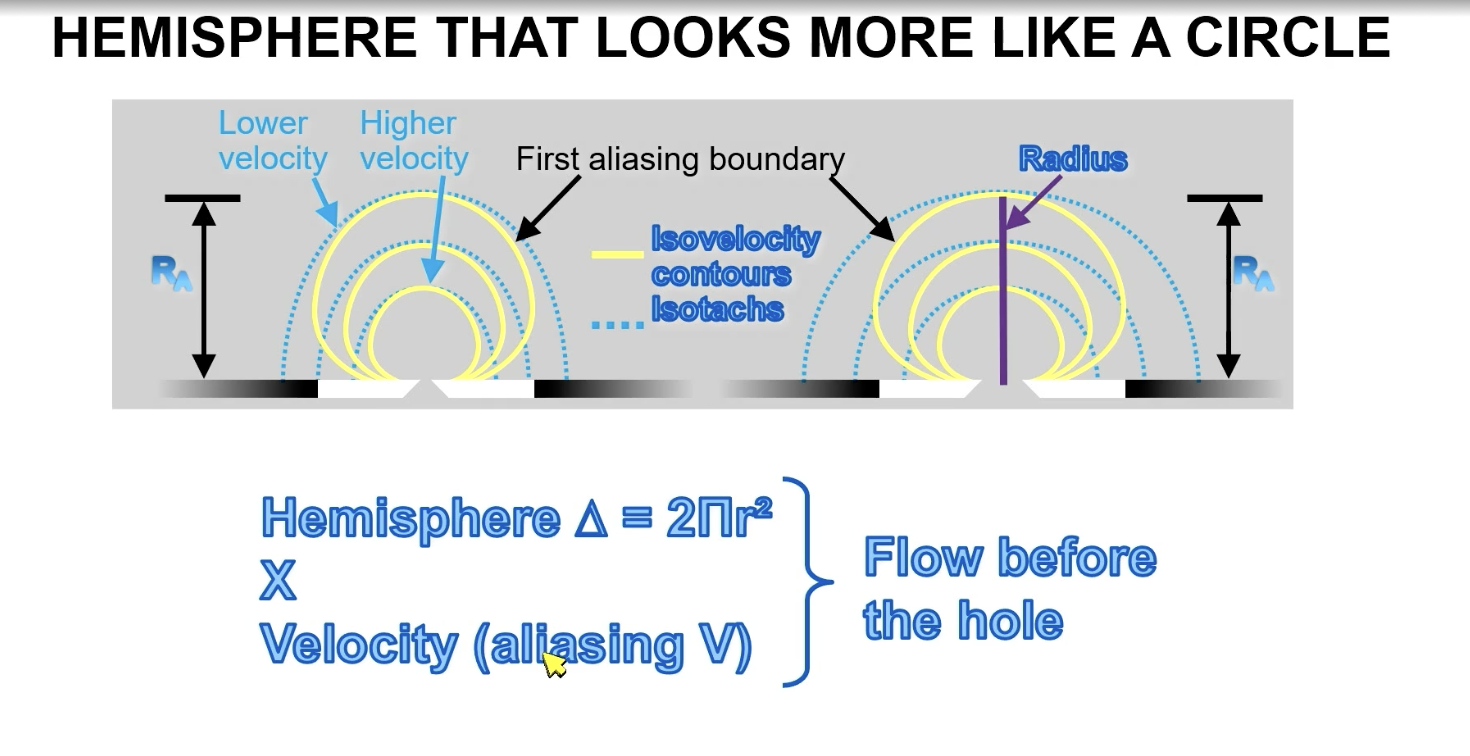
Shortcut for calculating ERO from flow (cm3/sec) and regurgitant velocity (cm/s)
ERO (0.27 cm2) = flow/regurgitant velocity
Wide pulse pressure with systolic hypertension.
Bounding carotid pulses
Descrescendo murmur
Sit forward and hold breath in expiration
Corrigan (bounding carotid pulse), Quinke (see the pulsations in the nails), Duroziez, de Musset, Muller, function Ao ejection murmur (to and fro), Austin flint
Severe AR
What End Systolic Diameter Index (indexed for BSA) is associated with higher mortality?
ESDi > 20 mm/m2
What LV end systolic volume index (LVESVi) is associated with higher mortality?
> 45 mL/m2
What LV GLS in severe AS patients is cutoff regarding all cause mortality?
<15%
Management of AR