6) Cardiac Physiology
1/60
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
61 Terms
True or False: Arteries and veins are defined based on their oxygenation level.
False - it’s based on where they carry blood (to vs away)
Describe the heart's "two pumps."
Low-pressure pump (right side, pulmonary circulation)
Large, high-pressure pump (left side, systemic circulation)
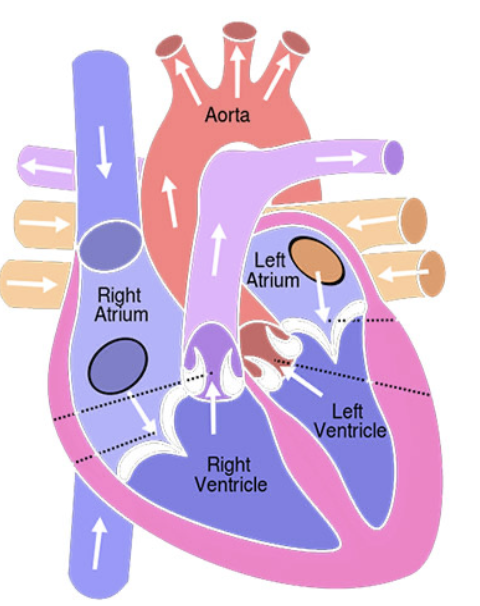
Describe the circulatory pathway.
Deoxygenated blood from the vena cavae enters the right atrium
Deoxygenated blood passes through the tricuspid valve into the right ventricle
Blood is pumped at relatively low pressure from the right ventricle, through the pulmonary (semilunar) valve to the lungs and back to the left atrium
Blood enters the left ventricle through the MITRAL valve
Blood is pumped at high pressure via the aortic (semilunar) valve to the entire body
Returned to the right atrium, via the vena cavae
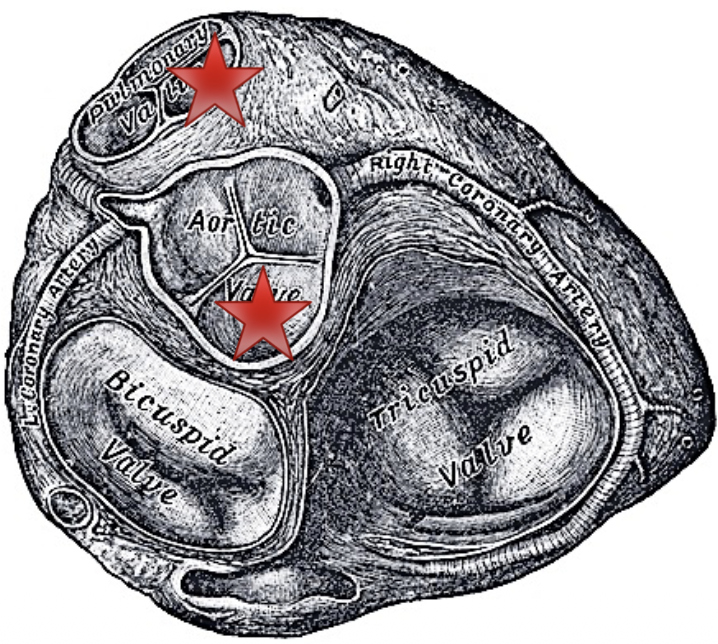
What supports and frames the four heart valves?
fibrous, non-contractile tissue of the heart’s skeleton
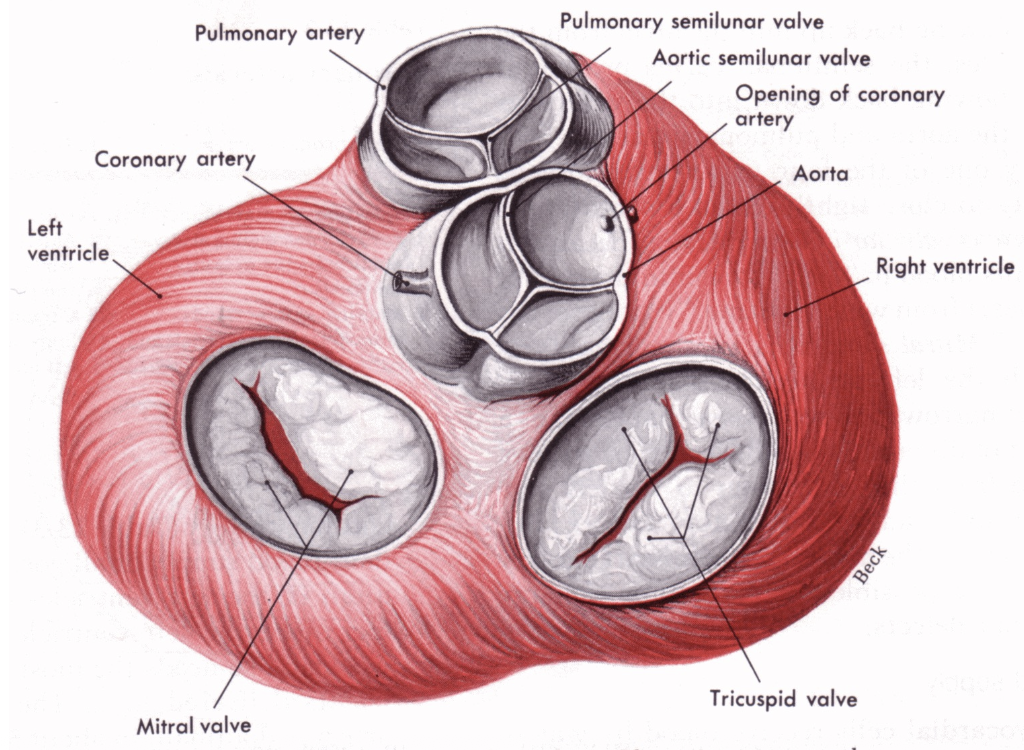
What are the 2 semilunar valves? How do the semilunar valves close?
Pulmonary valve
Aortic valve
→ backsurge of blood after each pulse opens the leaflets like umbrellas; as they open, their edges push together to form a seal
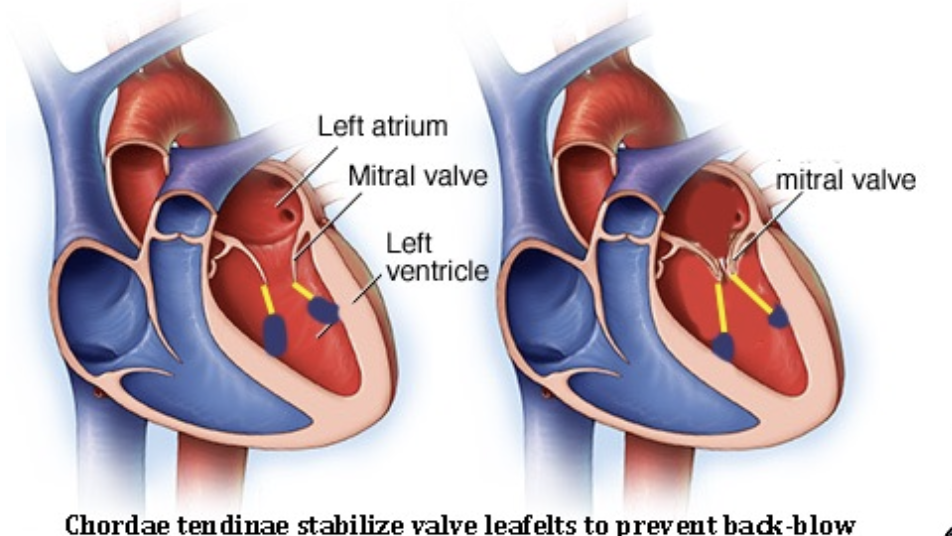
What is the function of papillary muscle contraction in AV valves?
isometric + stabilizes valve leaflets via chordae tendineae to prevent back-flow (it doesn’t pull the valves open)
Unlike skeletal muscle, how does cardiac muscle increase its force since it cannot use "recruitment"?
→ EVERY cell contracts with each beat
if more force is needed, each cell contracts harder via “inotropy”
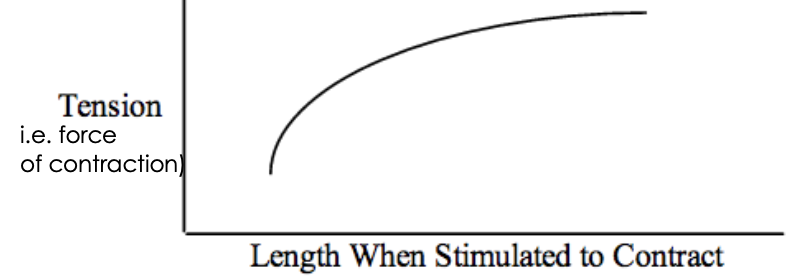
Since ALL muscles are activated, which mechanism can only alter force generation?
Changes in fiber length
preload; length-dependent activation, or how much the fiber contracts
changes in inotropy
length-independent activation, or how rapidly (how hard) the fiber contracts)
↑ inotropy = ↑ contraction strength for the same stretch or preload (muscle length)
What is the difference between a positive and negative inotrope?
(+) inotropes (e.g., Digoxin) ↑ contraction strength (without increasing its length/pre-load)
(-) inotropes (e.g., Beta blockers) weaken it
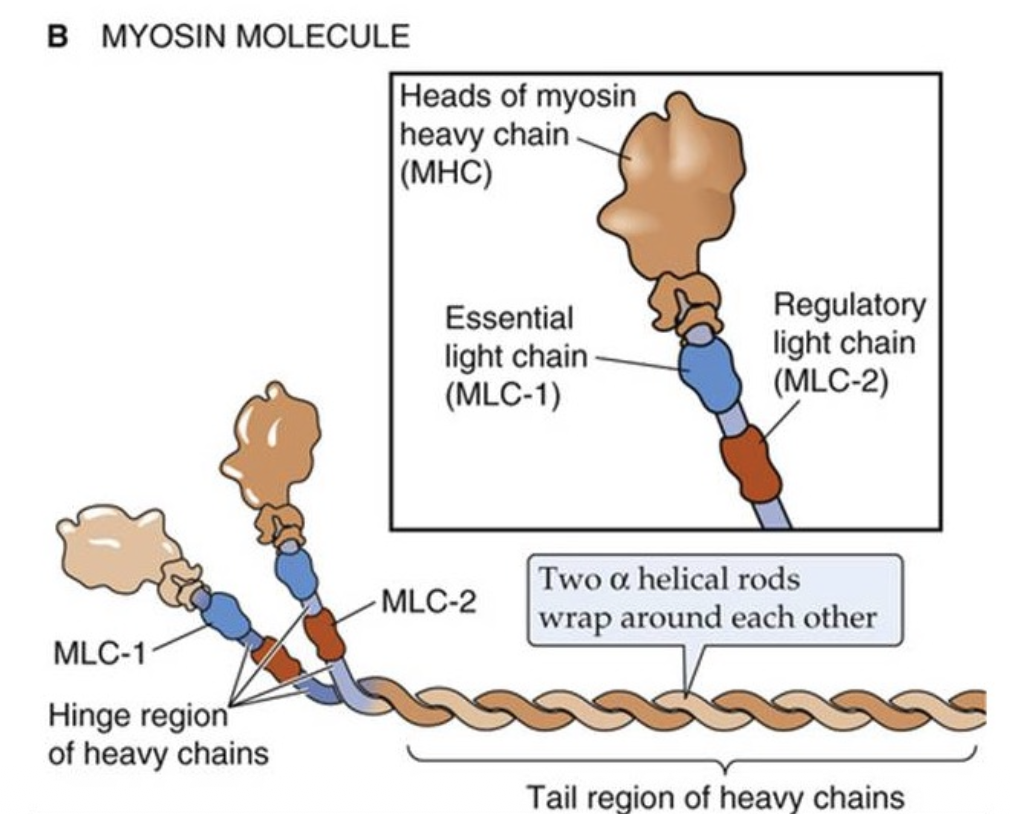
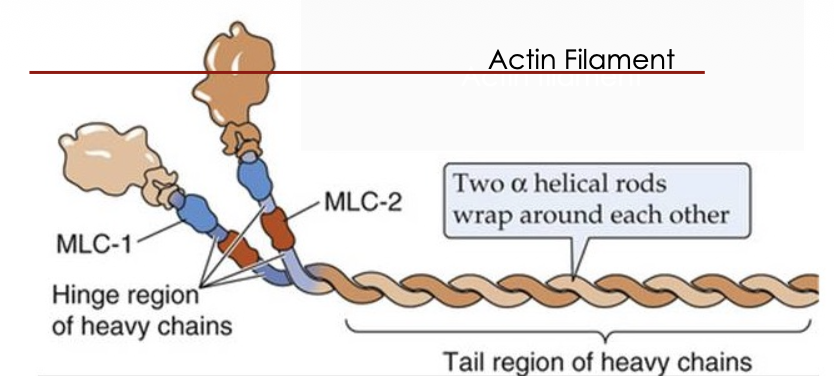
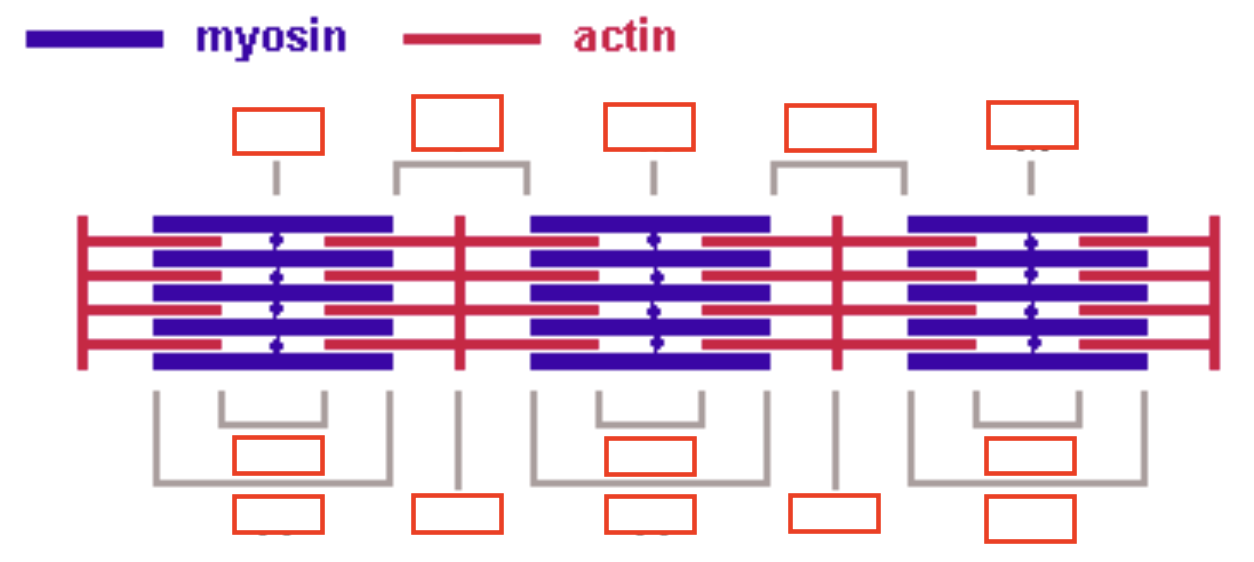
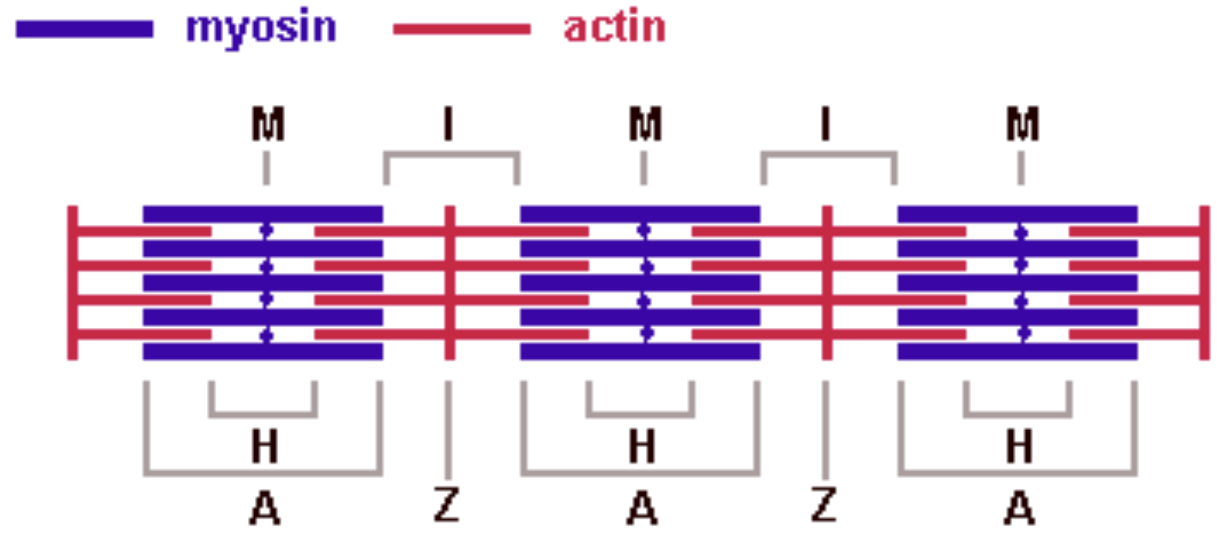
What are thin & thick fibers of Sarcomeres composed of?
Thick fibers
Myosin
Thin fibers
Actin – globular protein with myosin-binding site
Tropomyosin – runs along actin to block myosin binding site
Troponin – globular protein which binds Ca2+
Once bound, a conformational change occurs that removes tropomyosin’s inhibition, allowing contraction
What is the function of T-tubules in cardiac myocytes?
membrane invaginations that carry AP to the SR for Ca2+ release
Where are t-tubules of cardiac myocytes located?
Z-lines (intercalated discs)
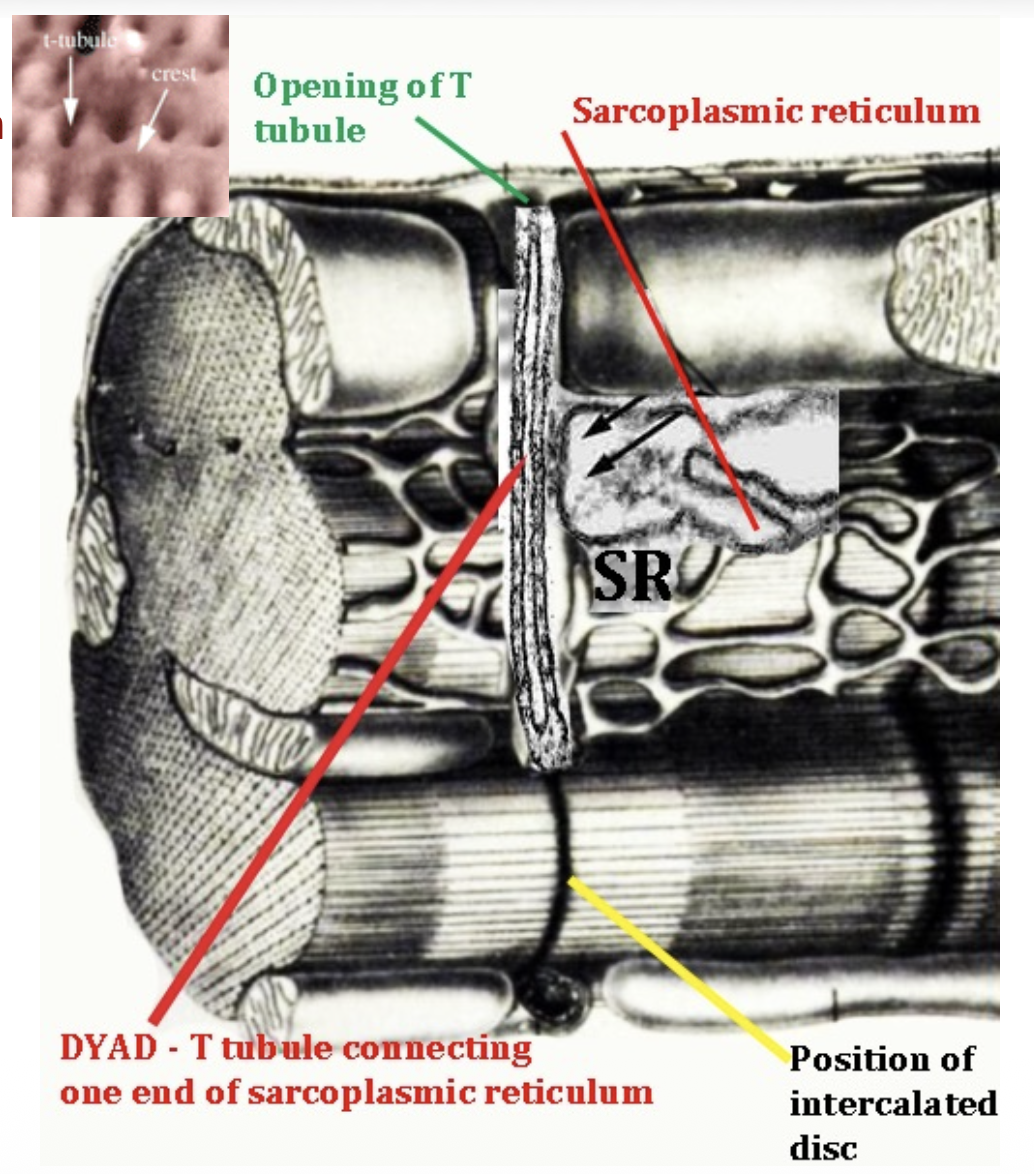
Describe what occurs when AP travels down the the T-tubules at the dyad.
Ca2+ release
AP triggers Ca2+ release from the SR to the cytoplasm
Ca2+ binds to troponin, which moves the tropomyosin, exposing myosin binding sites
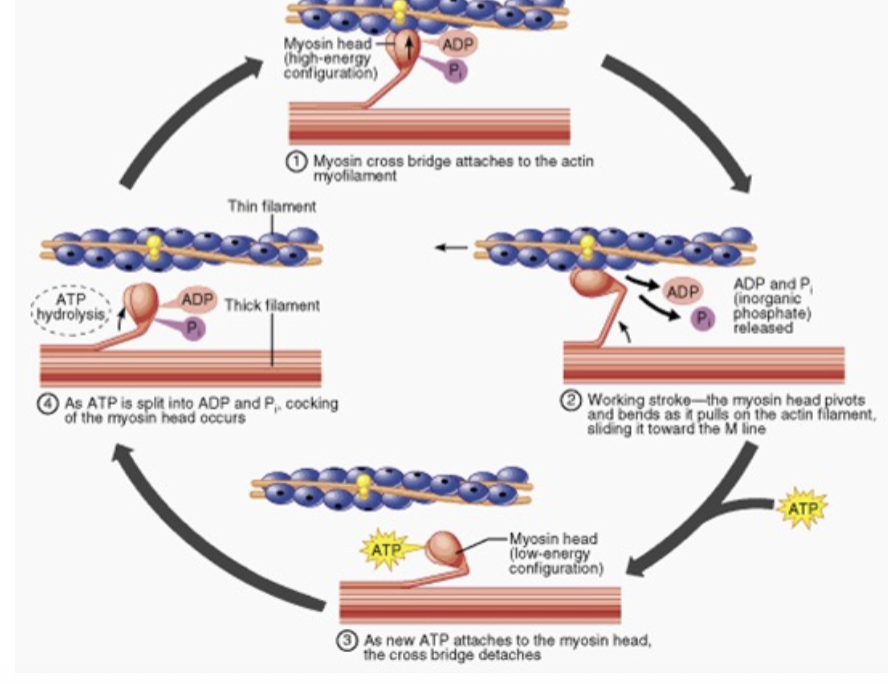
Sliding filament theory
Myosin head attaches to actin myofilament
Working stroke - myosin head pivots and bends as it pulls on the actin filament, sliding it towards the M line
ATP binds to myosin head, detaching it from cross bridge
ATP → ADP + Pi
Myosin head cocks up
Repeat cross-bridge cycle
Ca2+ uptake
As [Ca2+]intracellular falls, Ca2+ dissociates from troponin
Tropomyosin goes and blocks myosin binding sites
Ca2+ leaves cytoplasm to SR, during prolonged relaxation period
Fill this out.
The magnitude of a cardiomyocyte contraction is proportional to what?
[Ca2+]intracellular
List 3 junctions of the Intercalated discs. Mention their functions.
Desmosomes– ensure fibers stay attached in a line during contraction
Gap junctions - allow AP to spread along a linear row of cardiomyocytes during contraction
Fascia adherens – anchoring sites for actin
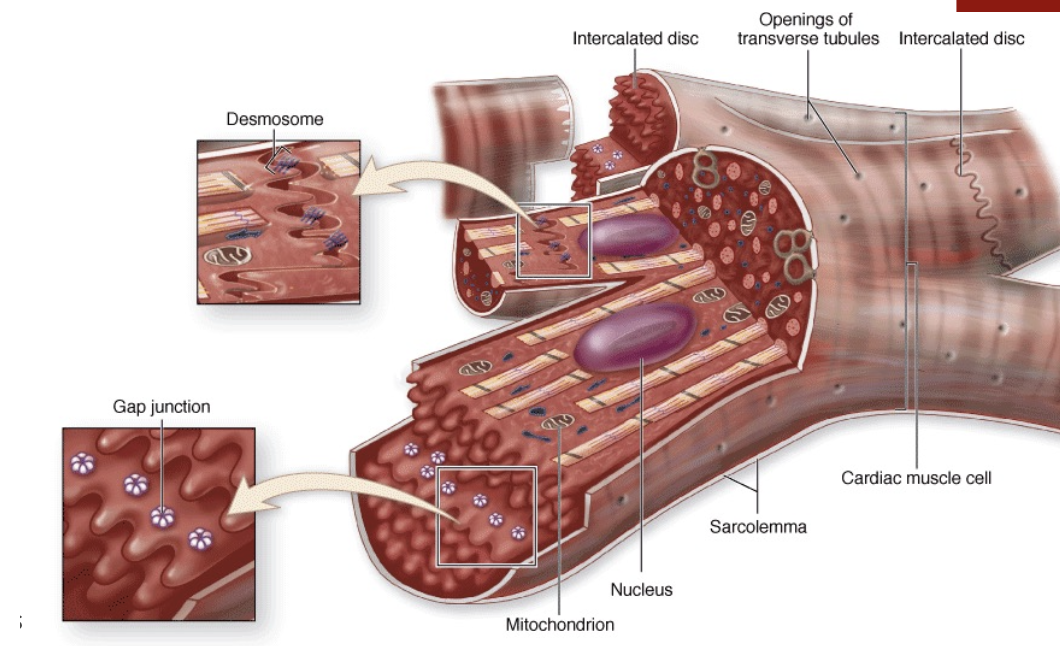
Why can AP readily pass from 1 cardiac muscle cell to the next?
they have very low electrical resistance
What ion movement causes depolarization (muscle contraction) in cardiac cells?
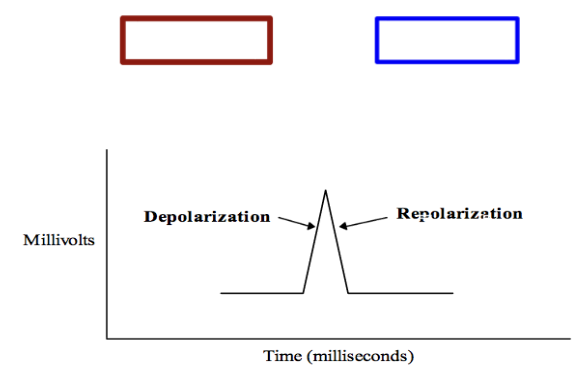
Opening of:
Fast voltage gated Na+ channels → Na+ enters
Slow voltage gated Ca2+ channels → Ca2+ enters
What ion movement causes repolarization (muscle relaxation) in cardiac cells?
Opening of:
Voltage gated K+ channels → K+ exits
Slow voltage gated Ca2+ channels → Ca2+ enters
Is action potential the signal to contract or is it the contraction itself.
Signal to contract
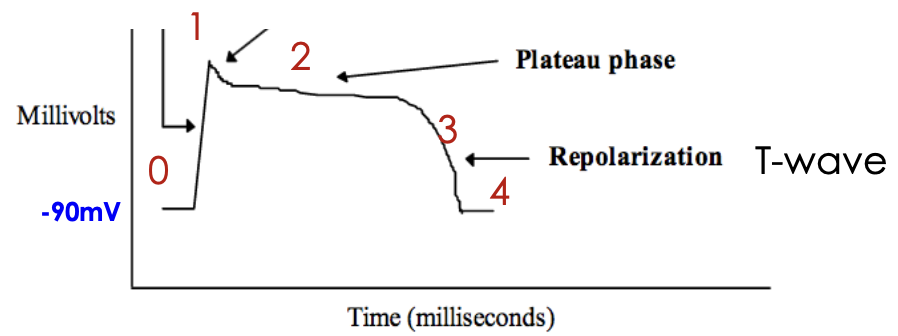
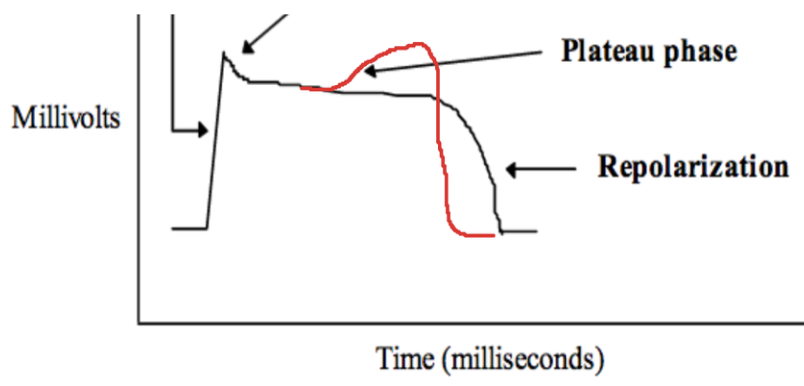
Describe the 4 phases of the heart’s action potential.
Phase 0: fast Na+ channels open → Na+ flows into the cell (depolarizes) → rapid upstroke (Q)
Phase 1: Na+ channels close (partial repolarization)
Phase 2: K+ efflux; Ca2+ influx (plateau phase)
Phase 3: K+ efflux > Ca2+ influx (repolarization) → membrane potential decreases to baseline
Phase 4: Resting phase
Define an ECG in relation to myocardial cells.
summation of the depolarization wave across all the myocardial cells
Define Inotropy.
force of contraction during systole
Define Lusitropy.
amount of relaxation during diastole
Define Chronotropy.
heart rate
True or False - Both Sympathetics and Parasympathetics affect the SA and AV nodes.
True
True or False: Both Sympathetics and Parasympathetics affect the ventricles.
False - ventricles receive only sympathetics
How does sympathetic stimulation affect the ventricles?
↑ NE
Amount of depolarization/↑ force of contraction = ↑ inotropy
Opens an ATP channel that allows SR to soak up Ca2+ = ↑ lusitropy → shortens recovery time
↑ Chronotropy
How does Verapamil specifically affect the heart?
blocks Ca2+ entry needed to sustain the plataeu phase→ ↓ contractility → ↓ HR & ↓ blood volume pumped
Treatment: tachycardia & A-fib
Which parts of the heart's conduction system have intrinsic autorhythmicity?
SA node
AV node
Purkinje fibers
What is the discharge rate of the SA node in a denervated heart?
~100x/min
Why is there an insulating ring (non-conductive tissue) between the atria and ventricles?
ensure they contract in sequence, not together, to move blood effectively
What structures depolarize the ventricles?
Purkinje fibers (modified cardiac muscle cells) within the bundle branches
What is the normal HR range?
60-100bpm
How long does 1 beat last?
0.6-1 sec
How does depolarization appear in the ECG waveform?
(+) upward deflection
What does the P-wave represent?
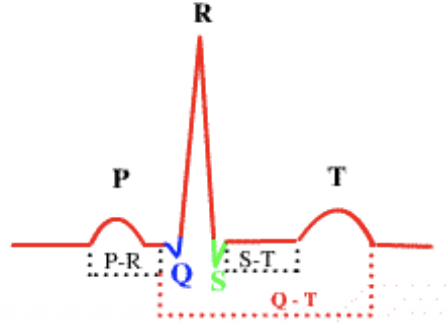
atrial depolarization and contraction via SA node
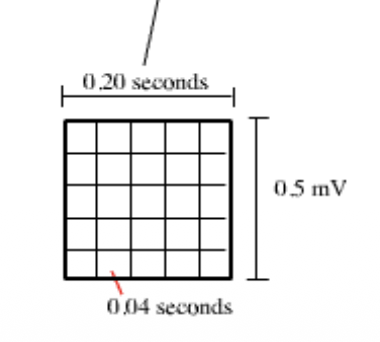
What does the PR interval represent? What is its duration?
→ AV conduction time (delay b/w atrial contraction & ventricular contraction)
Duration time is 0.12 to 0.20 seconds (1 large box)
What does the QRS complex represent? What is its duration?
→ ventricle depolarization via AV nodes
not longer than 0.10 seconds (less than 3 small boxes)
What is the maximum normal duration for a QRS complex?
0.10 seconds (less than 3 small boxes)
What does the T wave represent?
ventricle repolarization
What is an ST segment?
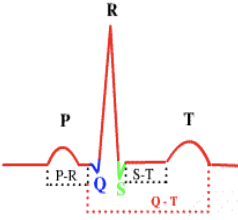
early ventricular repolarization
What is a QT interval?
→ measured from the Q (initiation of ventricular contraction to the end of the T (repolarization)
represents ventricular depolarization and repolarization (Na+ influx and K+ efflux)
What is total time of a normal ECG?
0.6-1.0 sec (5 large boxes=1 sec)
A regular heartbeat is said to have a _________.
A regular heartbeat is said to have a Sinus (node) Rhythm
Define Pre-load. What determines pre-load?
→ magnitude of “pre-stretching” of the cardiac muscle fibers
Left ventricular end-diastolic volume (LVEDV) determines preload
How does ventricular filling affect preload?
More blood in the ventricle at the end of diastole → greater ventricular wall stretch → increased preload
What is the relationship between preload and cardiac contraction?
↑ preload = stronger & faster contraction
Define After-load.
pressure the ventricle must overcome to eject blood during systole (resistance)
When is afterload measured?
During ventricular ejection = when the aortic valve is open and the left ventricle and aorta share the same pressure
What factors increase afterload?
↑ PVR (e.g., hypertension)
↑ pulmonary blood flow resistance (e.g., lung disease)
What is the core concept of the Frank-Starling Mechanism?
↑ venous return (pre-stretch/preload) → ↑ force of contraction & ↑ SV
Define Stroke volume. What is its average value?
→ volume of blood leaving the ventricle with each beat
70 mL
Define Ejection Fraction. What is its average value?
→ fraction of the EDV ejected in each stroke
50-55%
Ejection Fraction = SV / EDV
Define Cardiac output. What is its average value?
→ total volume ejected from the left ventricle per unit time
CO = SV x HR
Factors affecting CO. List 3
HR
SV
Contractility
Remember: CO = SV x HR
Where does fluid back up in right-sided vs. left-sided heart failure?
Right-sided failure → backs up in the body (gravity dependent)
Left-sided failure → backs up in the lungs
can also lead to right sided failure (cor pulmonare)
Several types of cardiac enzyme tests done when a heart attack is suspected. What enzymes are they detecting? Why?
creatine phosphokinase (CPK) or creatine kinase (CK)
CK-MB (specific form of CPK/CK)
Myoglobin & Troponins I and T levels
Reason: these substances are released from the heart muscle cells into the bloodstream, when the heart muscle is damaged
Of the different enzymes detected, which ones are cardiac specific?
Troponins (cardiac specific)
CPK/CK (works for all damaged tissues)
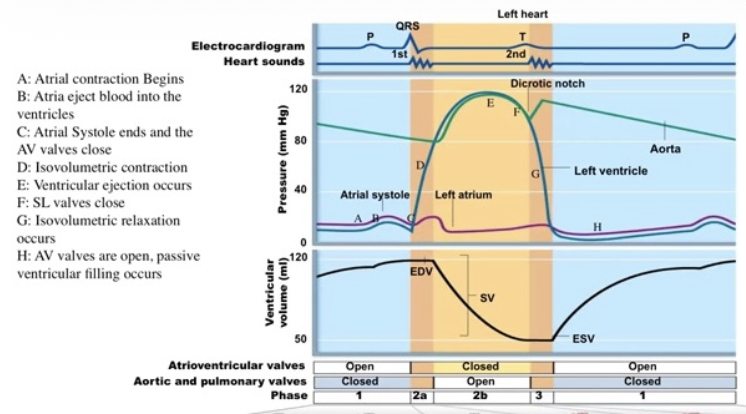
Describe the main events of the Wigger’s Graph.
1) Atrial Systole (Ventricular Filling Completed)
Atrial depolarization (P wave) precedes atrial systole
Atrial systole increases atrial pressure enough to open the AV (mitral/tricuspid) valves and push the final amount of blood into the ventricles
Ventricles reach their maximum volume (EDV)
Atrial pressure then falls as the ventricle fills
→ Ventricle is now fully loaded with blood and ready to contract
2) Isovolumic Contraction
Ventricular depolarization (QRS complex) initiates ventricular contraction
Ventricular pressure rises rapidly (volume stays the same)
When ventricular pressure exceeds atrial pressure: AV valves close → producing the First Heart Sound (S1)
Both AV and semilunar valves are closed
3) Ventricular ejection
Ventricular pressure continues rising.
When ventricular pressure exceeds aortic pressure: Aortic valve opens
Blood is ejected from the ventricle into the aorta
↓ Ventricular volume from EDV toward ESV
↑ Pressure in ventricle & aorta rises to a “systolic peak”
4) End of Ventricular Ejection
↓ Ventricular pressure
Aortic pressure becomes greater than ventricular pressure
Aortic valve closes
What are Asteroid Hyalosis?
→ development of yellow/white glistening “asteroid bodies” in the vitreous
made of lipid and Ca2+
move with vitreous gel and return to their original position when eye stop moving
usually over age 50
unilateral
asymptomatic with no vision change
