Characteristics of a Radiation Beam and Field
1/87
Earn XP
Description and Tags
ONCOL 355 - Tx Planning and Dosimetry. University of Alberta
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
88 Terms
Co-60 half-life and photon energies
half life = 5.27 years
photon energies: 1.17 MeV and 1.33 MeV
Why is it important to know the information about half-lives and activity for radiaiton therapy
it is important to choose the most appropriate source for the procedure and to ensure patient safety and effective treatment planning. Understanding these factors helps in predicting dose delivery and optimizing treatment schedules.
When treating with a radioactive source, we calculate a treatment ….
a treatment time
do we calculate a treatment time with LINACs?
no, because of how the x-rays are produced in the linear accelerator, we calculate a monitor unit, not a treatment time
three characteristics of radiation beams
beam divergence+ central axis
inverse square
penumbra
Beam Divergence and Central Axis
As radiation comes from point source, it spreads out after distance.
This is what divercence
The very central ray is not diverging, but further out from field the angle of divergence increases
- Will diverge in all dimensions
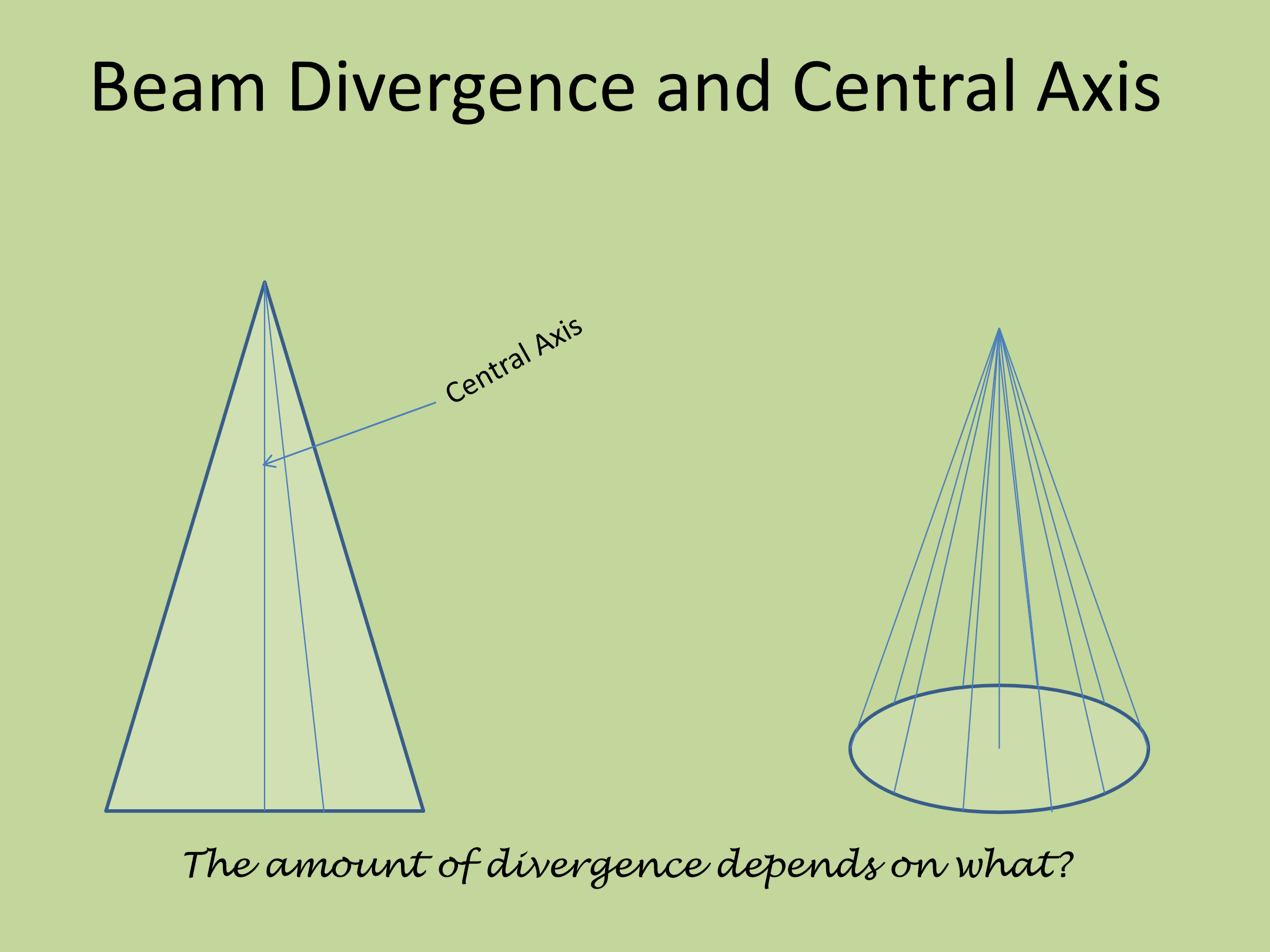
Will the centre ray always be in the exact center of the field?
no, if the field is not symmetrical, the centre ray may not always be in the exact centre
What is the inverse square law
the intensity of the beam varies inversly as the square of the distance from the source
Inverse square law formula
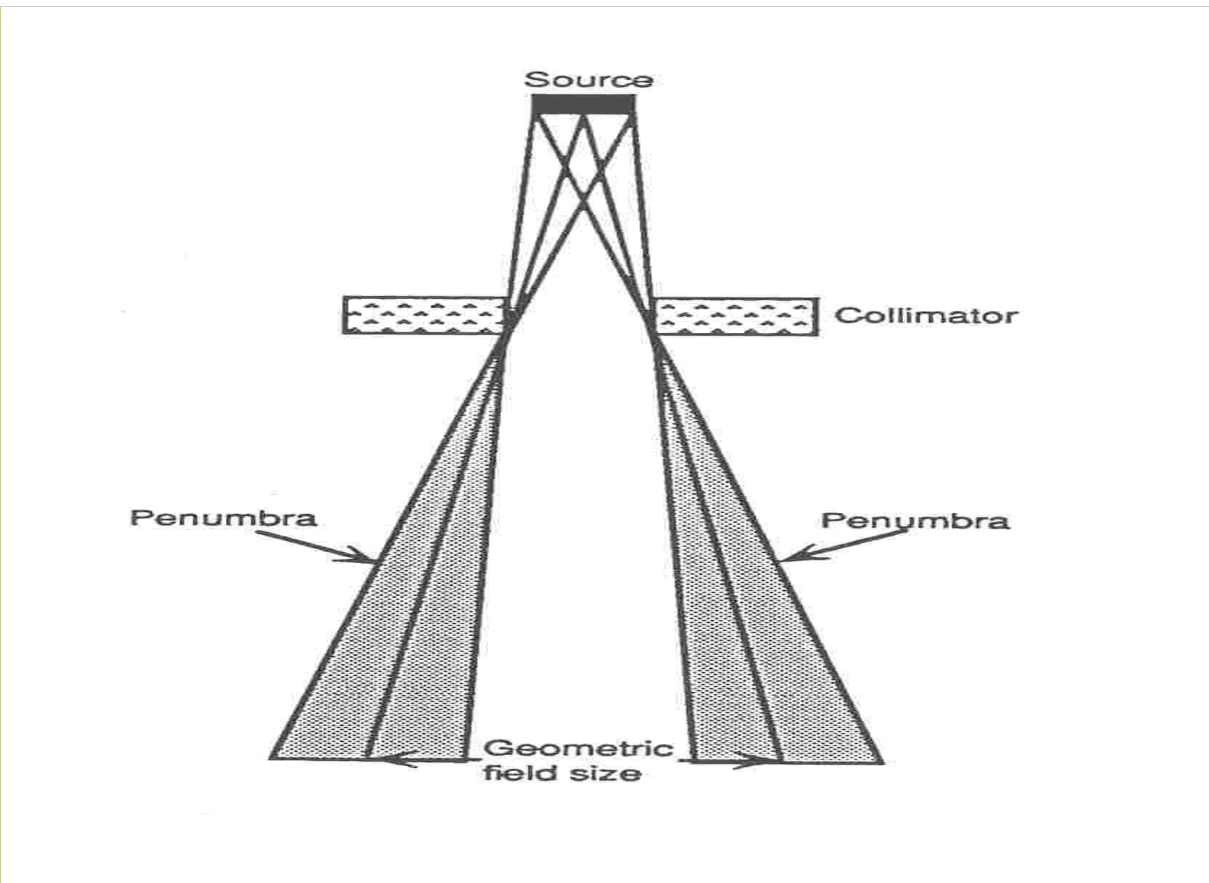
Penumbra definition
the region at the edge of the radiaiton field over which the dose rate changes rapidly at as a function of distance from the beams central axis
the amount of divergence increases further than the central axis, those rays are travelling further than the central ray, thus there is a region where the dose rate is less than what it is at the central axis
The intensity of radiation across a field isn’t ____ and then ____ at the field border
100%, 0%
Geometric penumbra
the term used when referring to the area of the edge of the field which lacks complete dose
we don’t have a full dose, and we don’t have none
what type of photons create geometric penubra
primary photons only
not scatted or secondary photons
just photons diverged from the source
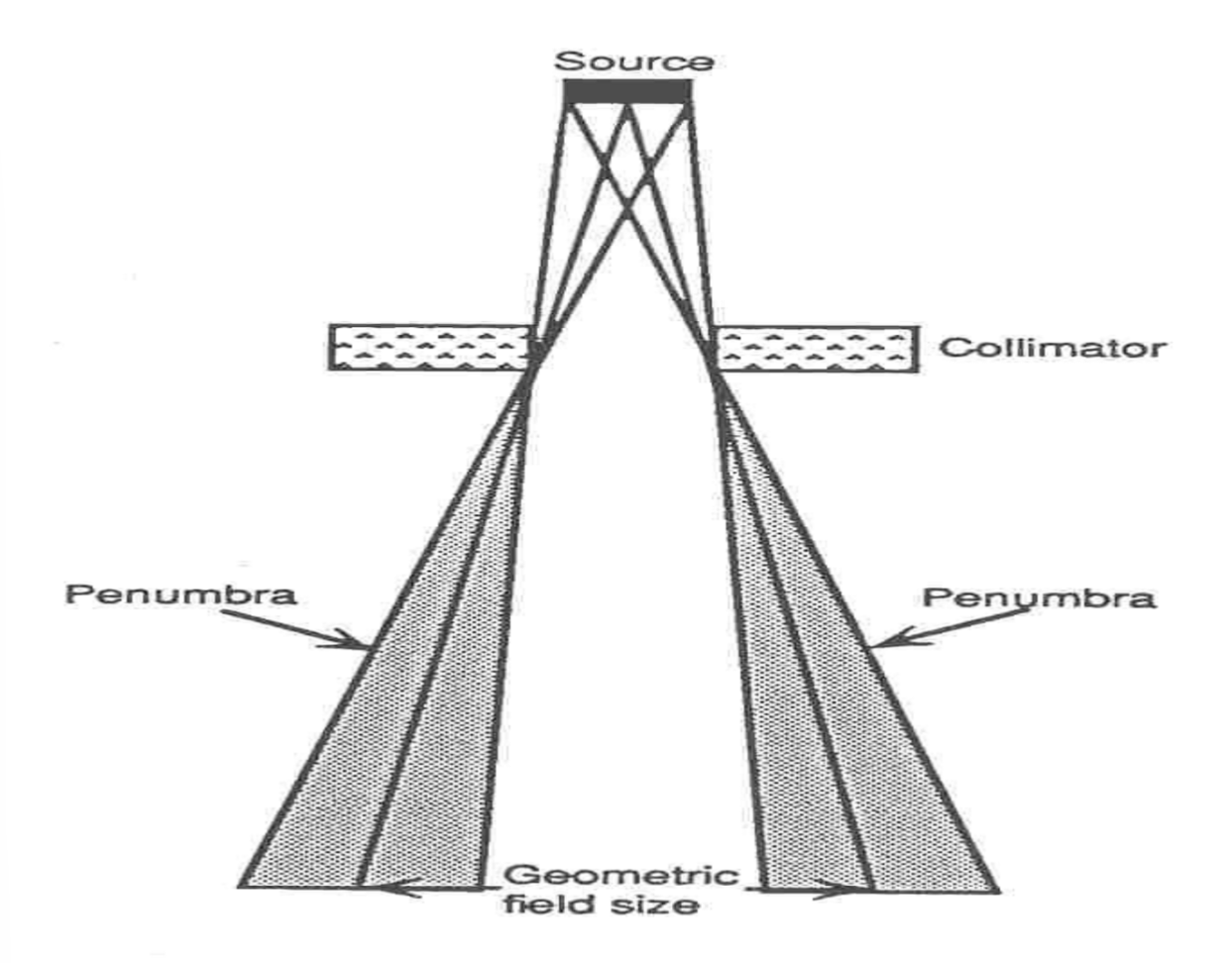
What is the geometric field size
the size of the treatment field = 50% field dose line
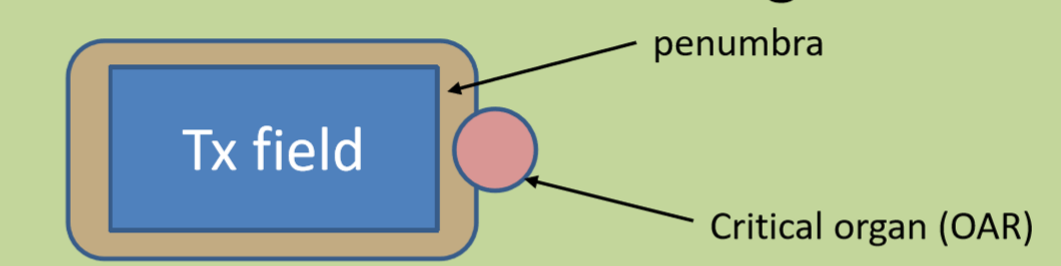
why is penumbra not a great ting?
it gives dose beyond a treatment volume, thus it may encroach onto a critical organ
produces a blurred effect at the edges of the field and on treatment images
tumor should not be in this region
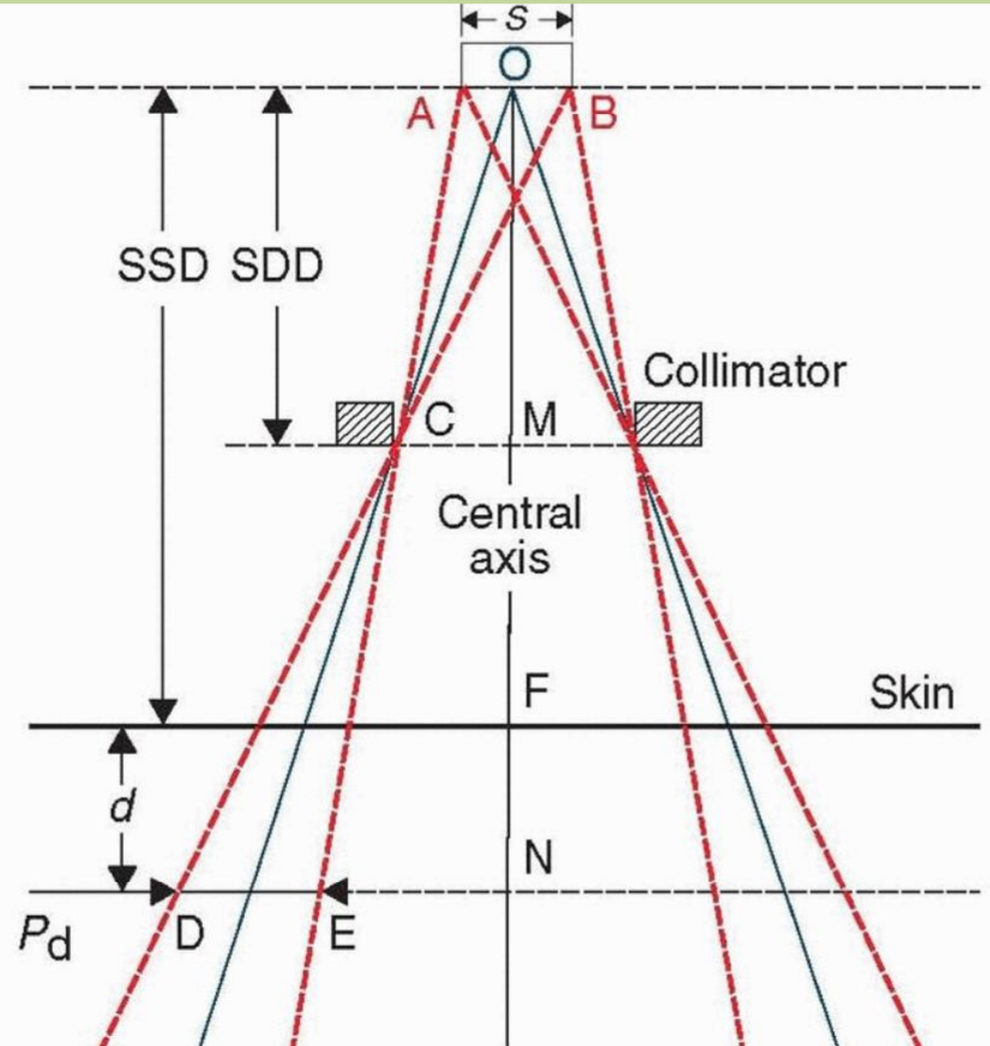
formula for geometric penumbra
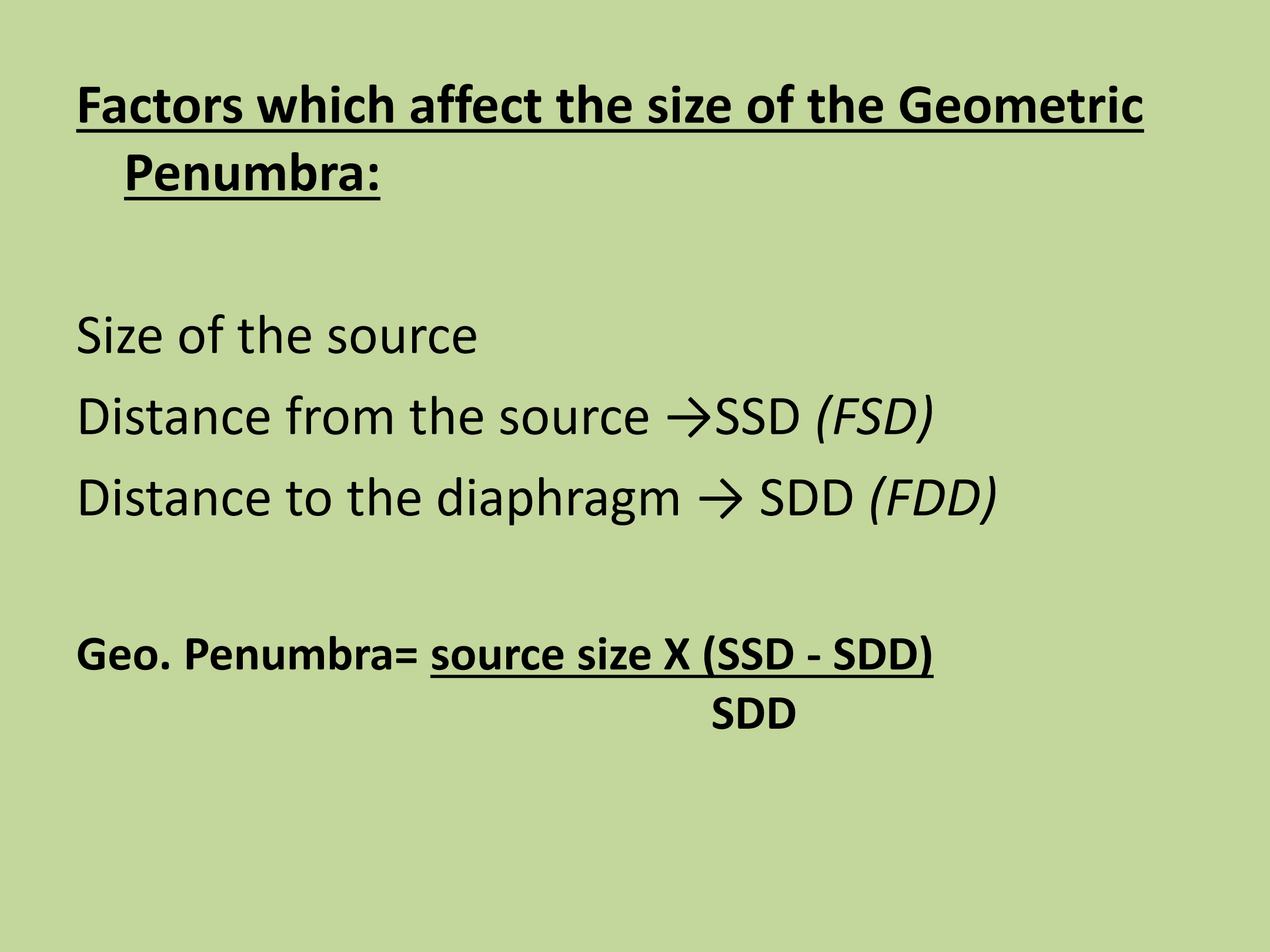
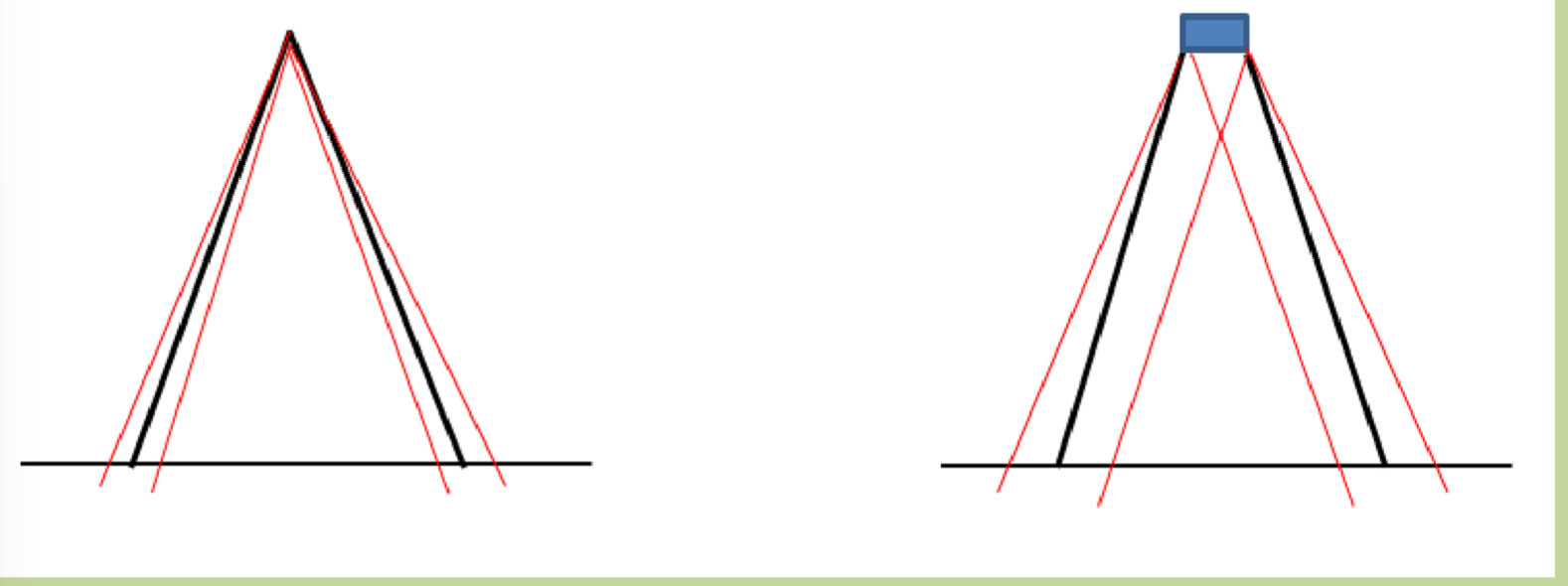
the larger the source size, the ____ the penumbra
larger
the larger the SSD, the _____ the penumbra
larger
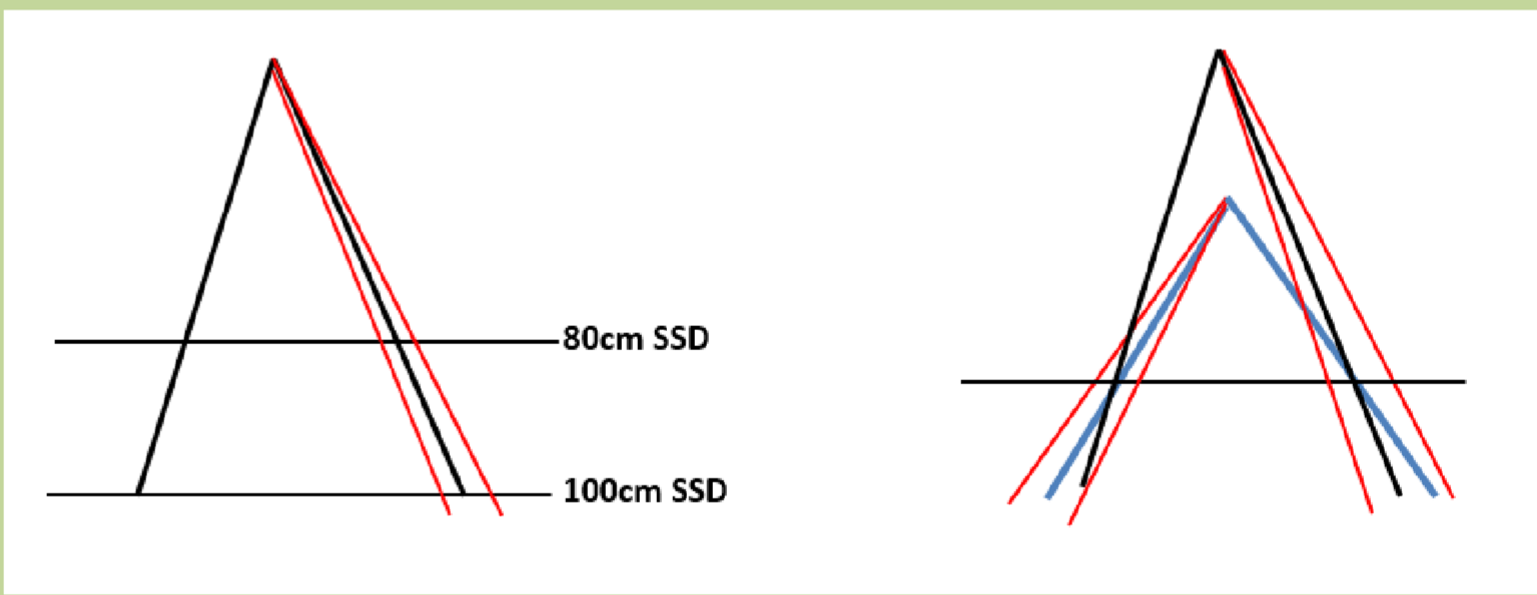
the larger the SDD, the ___ the penumbra
smaller
are photons direcly or indirectly ionizing?
indirectly ionizing
Photons travel through patient before transferring energy to electrons in patient which cause the damage
electronic equilibrium definition
the point at which the number of electrons leaving a volume equals the number entering it
Where does electronic equilibrium occur
at dmax
the depth at which 100% of dose is deposited
when EE occurs, dmax is acheived
Dmax for 6 MV
1.5 cm
Dmax for 10 MV
2.5 cm
Dmax for 15 MV
3.0 cm
What two factors determine Dmax?
beam energy
field size
what is the advantage of a deeper dmax
the skin sparing effect
if max dose is deposited below the skin, we can spare the skin from the higher dose that occurs at dmax
what happens after Dmax?
electrons continue to travel deeper into the tissues depositing their doses at various depths
as beam energer increases …
the penetration of the ability of the beam increases, and there is decreased absorption at shallower depths
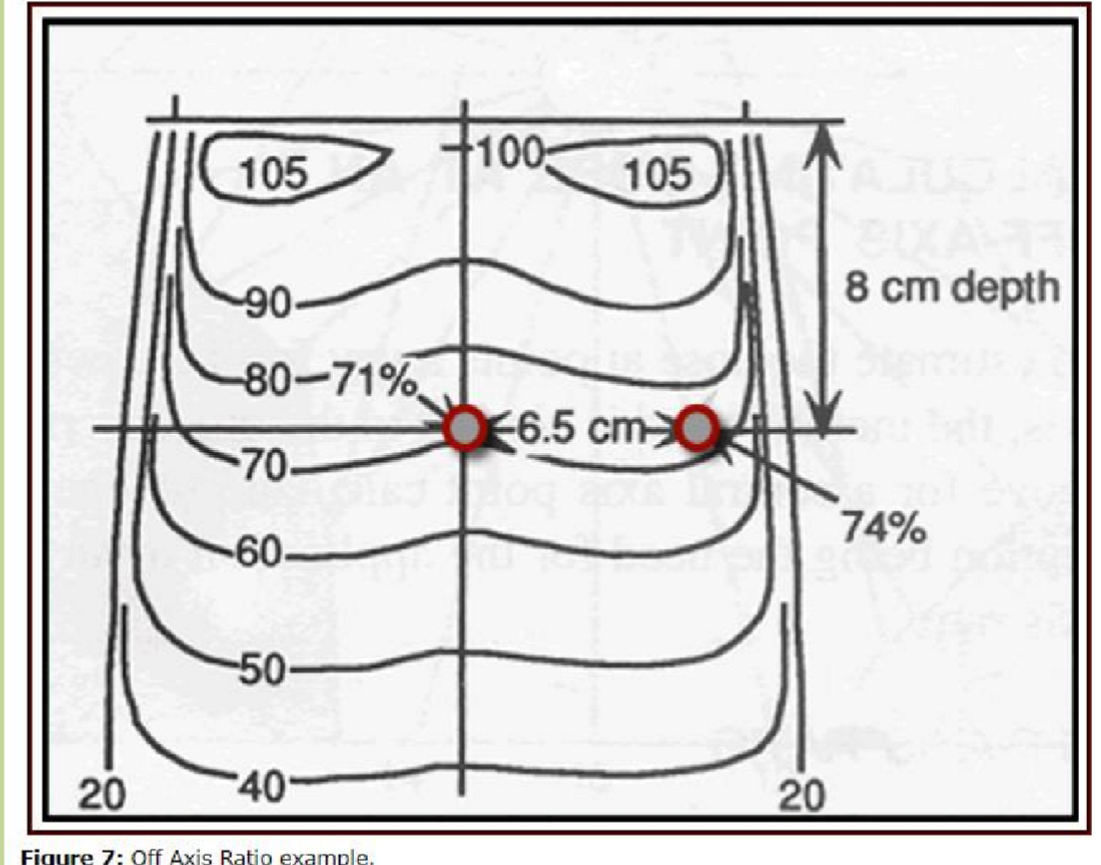
what do we use to visualize dose depostion/attenuation
isodose charts
a locus of points at equal dose value
three things isodose charts show
dose distribution on/off the central axis
fall off rate of a particular energy
shape of the isodose curves
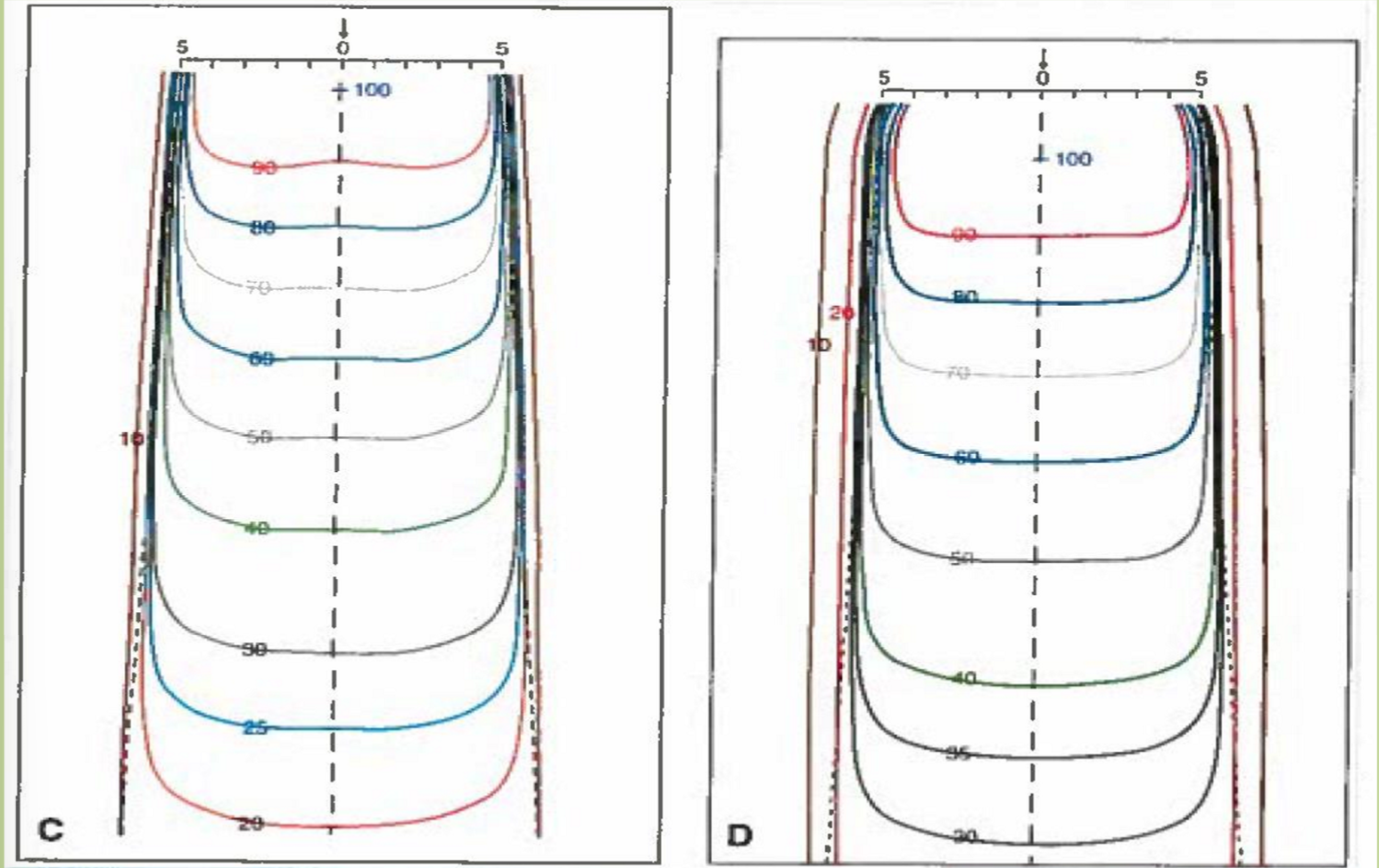
why are the lines curved in isodose charts?
penumbra
scatter
beam divergence and inverse square
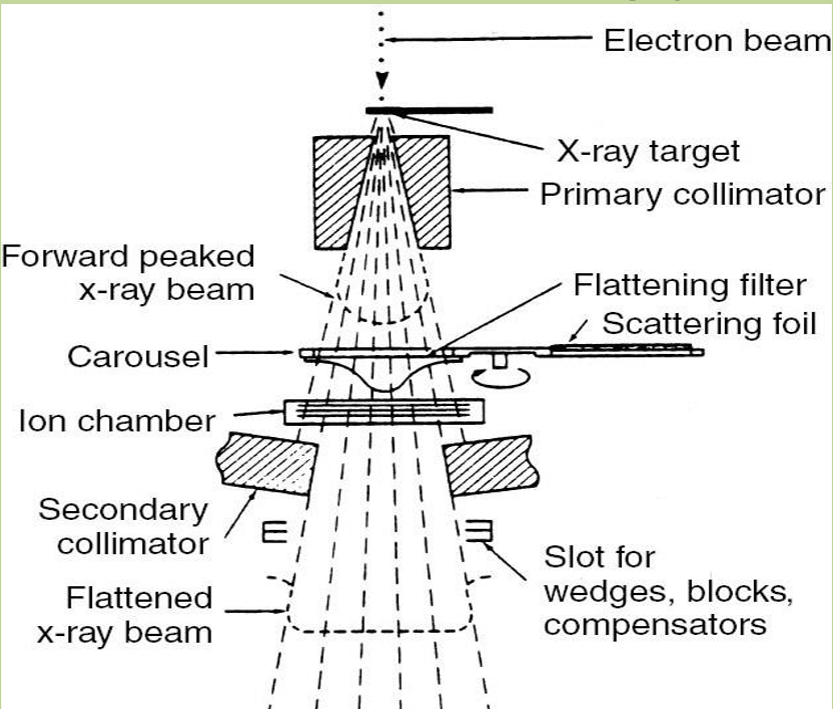
what effect to flattening filters have on isodose charts
Flattening filters create a smoother dose distribution across the treatment area, reducing dose variations and improving uniformity in the output of radiation beams.
horns are also created as a side-effect
without flattending filter, isodose is more bow shaped
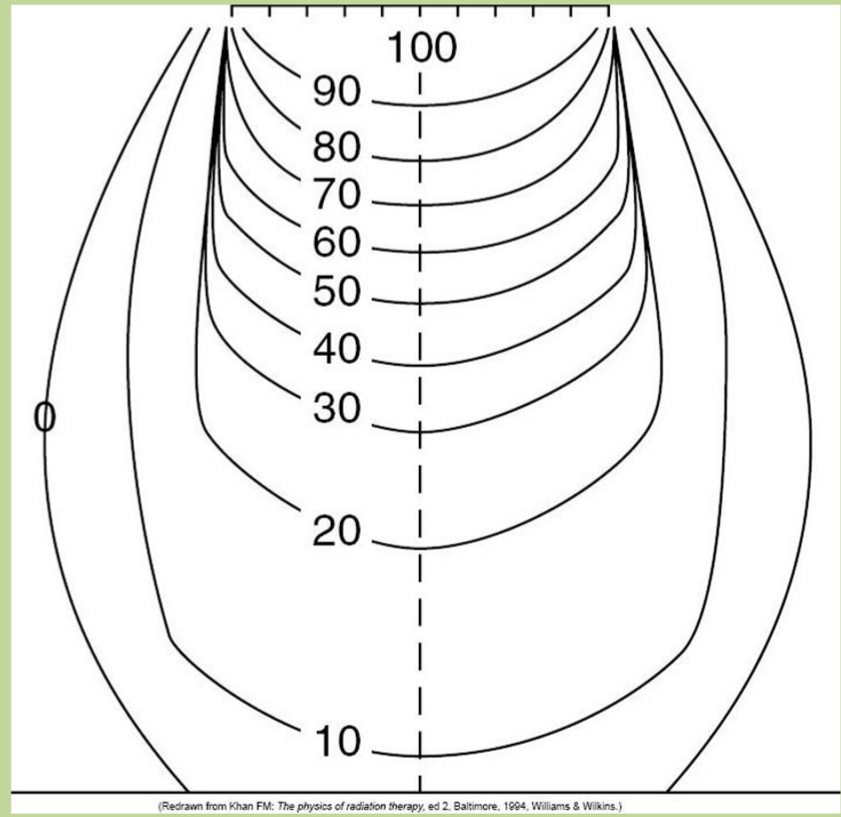
200 kVp orthovoltage isodose
Lots of dose going outside of field size
- Have lots of back scatter and field scatter with lower energies
- Must take OAR into consideration (such as eye for inner canthal treatment)
Co-60 Isodose chart
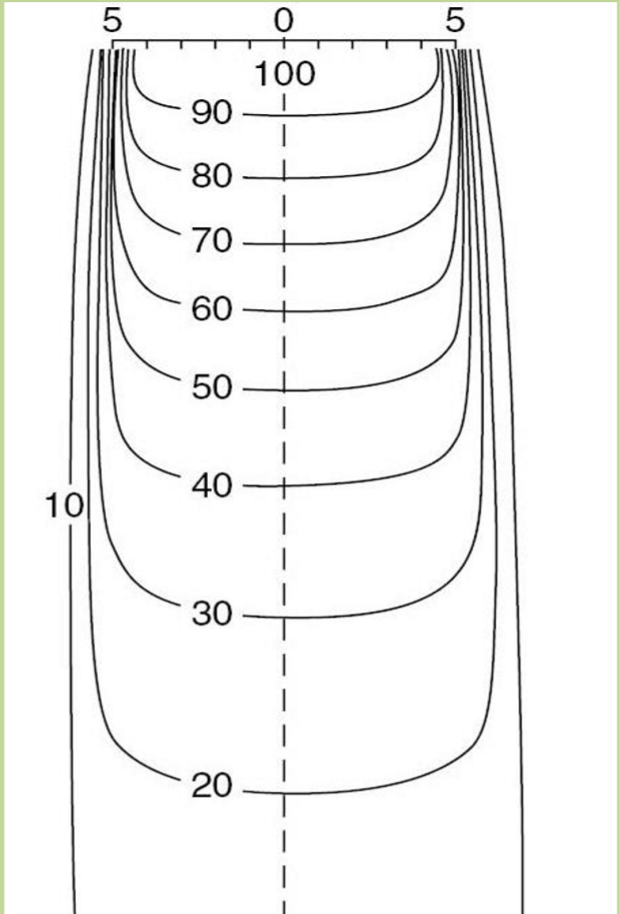
the larger the energy the ___ the penumbra
sharper
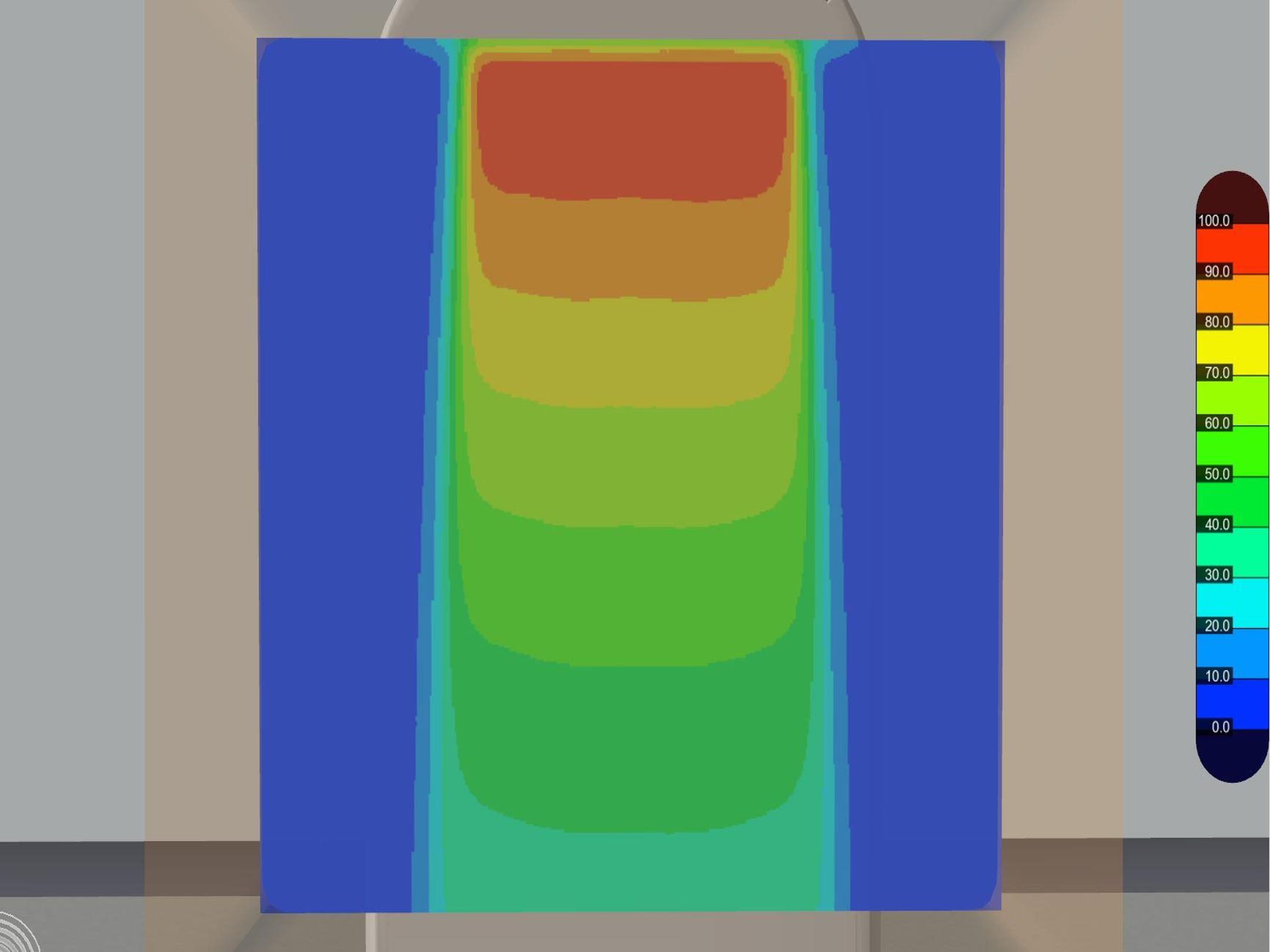
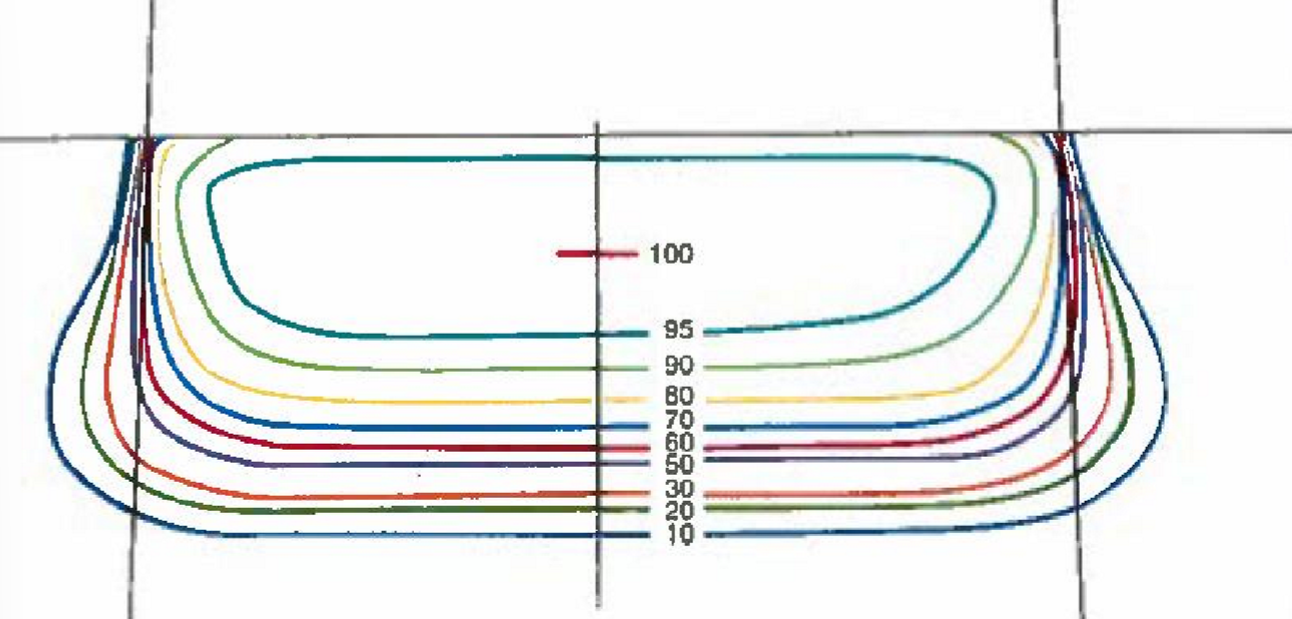
electron beam isodose chart
Barely gets through 4 cm of skin
Rapid fall off after 80%
Still get bulge underneath surface
- Large penumbra in electrons
Isodose curves are affected by:
energy
type of radiation
source size (penumbra)
SDD (penumbra)
SSD (penumbra)
flattening filter
shape of patient
patient inhomogeneities
normalization point
Geometric Field Size
Roughly passes through the centre of the geometric penumbra, and corresponds to the 50% isodose value at skin surface
what is the function of collimator jaws (secondary collimators)
they move to create various field sizes when there is no shielding used
how many sets of jaws
two sets of jaws: x and y
Y1 and Y2
X1 and X2
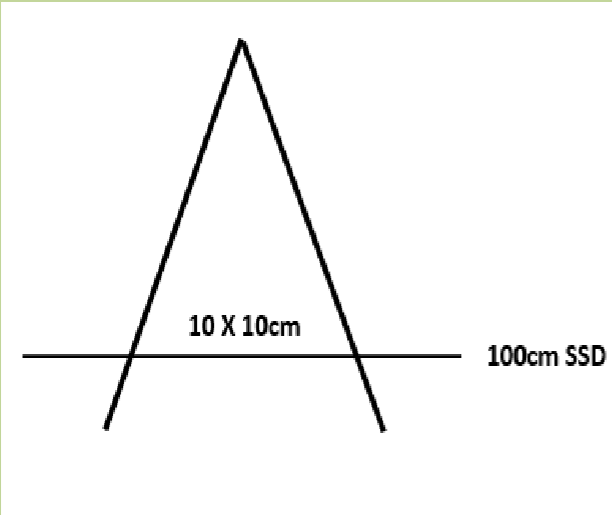
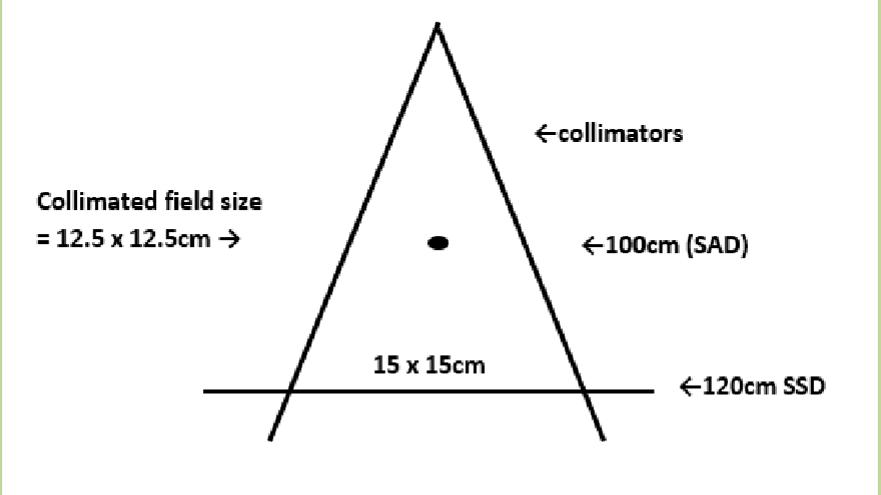
How is the field size defined with the SSD technique
it is determined at the treatment SSD (skin surface)
used for single fields or extended fields
isocentre is on skin surface/outside
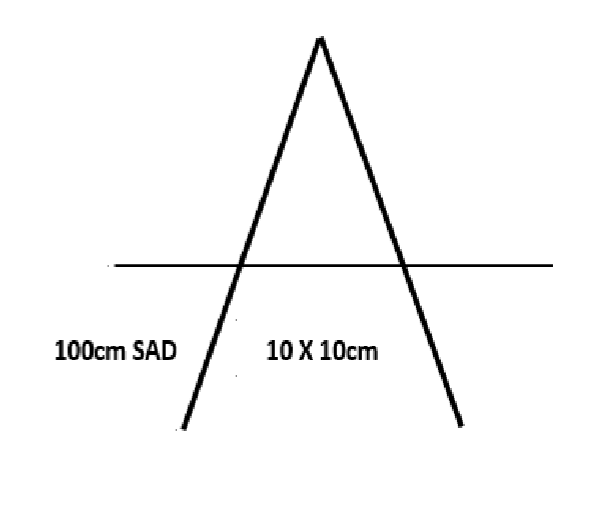
How is the field size defined with the SAD technque
it is defined at the treatment depth (inside the patient)
isocentre is within the patient, typically in the tumor volume
field size on skin is irrelevant
when is the field defined as the collimator size?
when the defined location is at the isocenter distance
no shielding in treatment field
when is the field not defined as the collimator size?
when extended SSD technique is used
have to make 12.5×12.5 to get a 15×15 at 120 cm SSD
shielding is used in the treatment field
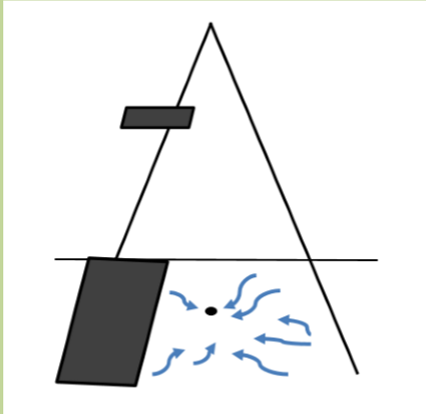
What is shielding?
physical devices put into the path of the radiation to block it from reaching the patient
why do we shield out some of the treatment field
to protect tissue/organs that don’t need treating or those that are critical structures and to shape the field
what three things can we used to create shielding?
lead blocks
cerrobend blocks
both these essentially obsolete in LINACS, used in ortho/e-
Multi-leaf collimators
main type of shielding used today
Pros and Cons of Pb
pro: good attenuator
Cons: high melting point, toxic, not practical for customization
Pros and Cons of Cerrobend
pros: low melting point, practical for customization
cons: toxic, custom blocks are time consuming
Divergent blocks
blocks that matched the divergence of the radiation beams
the further the block was from the central axis, the more angled it needed to be because of increased beam divergence
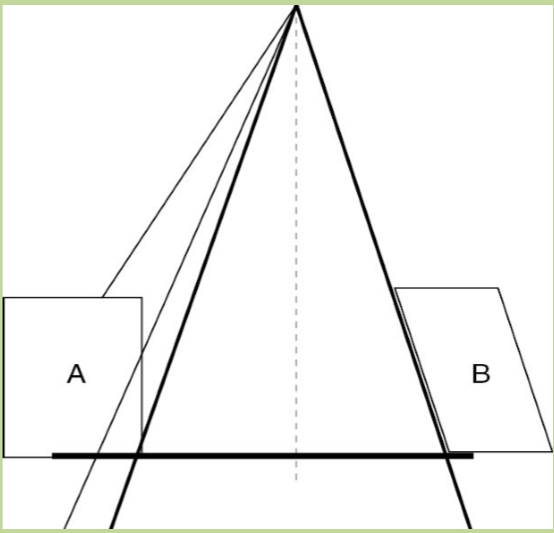
Non-divergent blocks
striaght sided blocks
this is what the lead blocks were
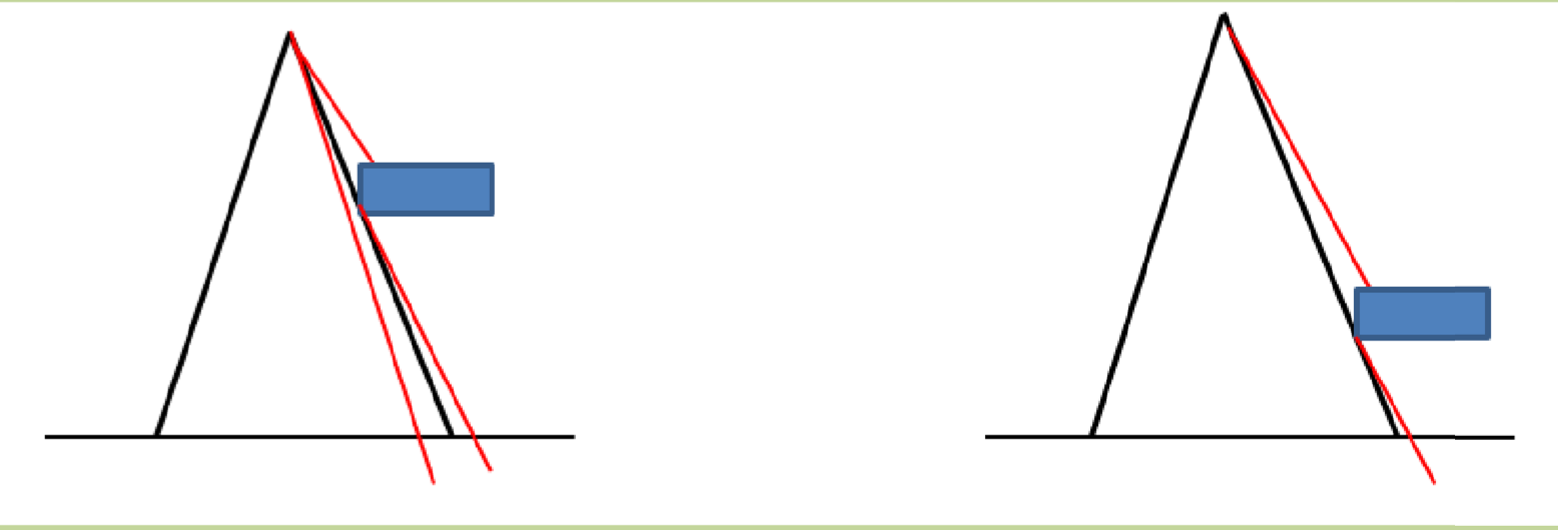
do divergent blocks or non-divergent blocks cause more transmission penumbra
non-divergent blocks
Transmission Penumbra
the region irraddiated by photons which have traversed part of the thickness of the collimator/shielding blocks
side A shows a non-divergent block creating transmission penumbra
physical penumbra
the sum of the transmission penumbra + geometric penumbra
this is the full penumbra the reduces the dose at the field edge due to a decrease in side scatter
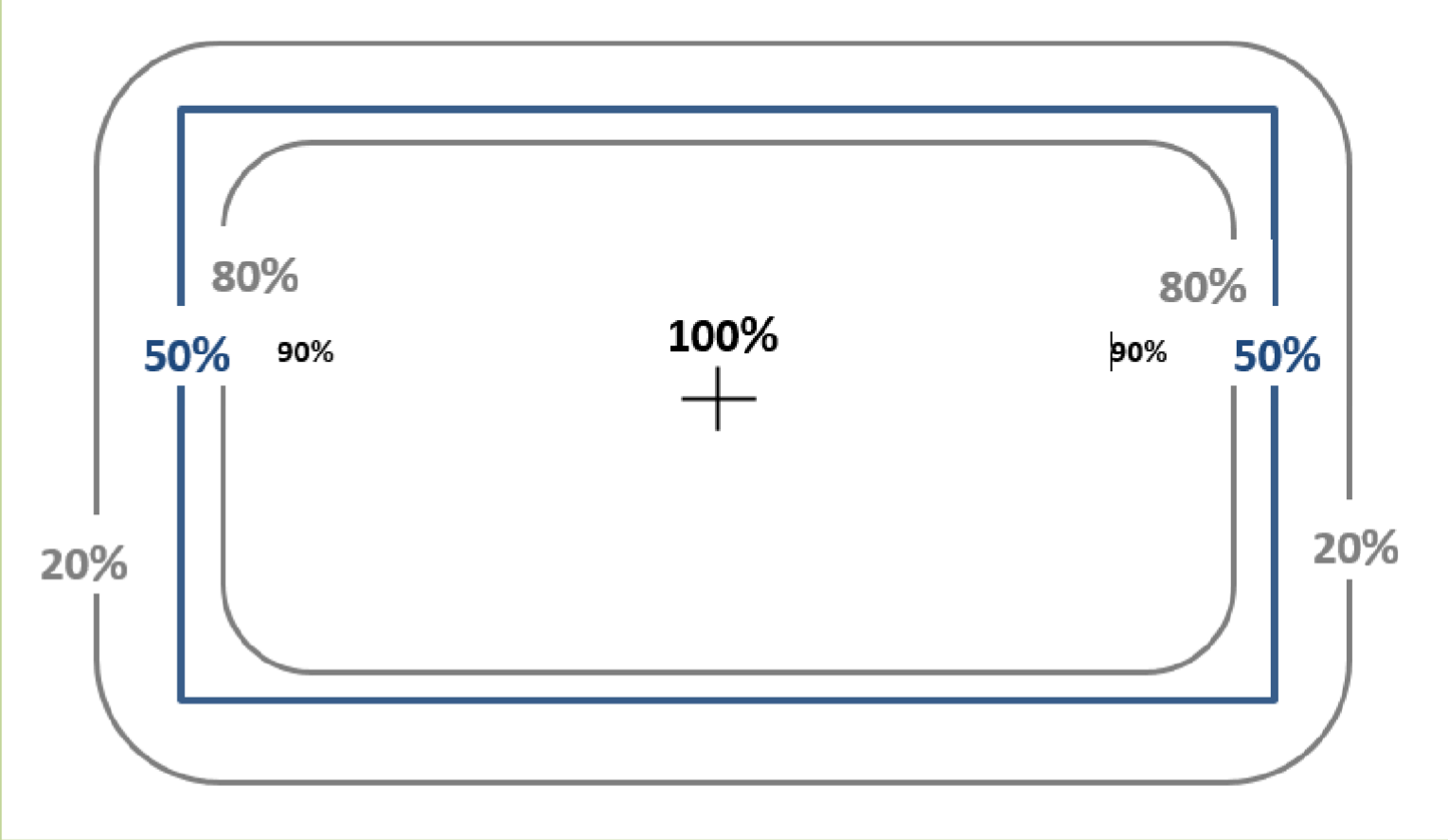
what is the physical penumbra measurement
between 90-20% isodose lines @ dmax
clinical penumbra
between 90-50% isodose lines @ dmax
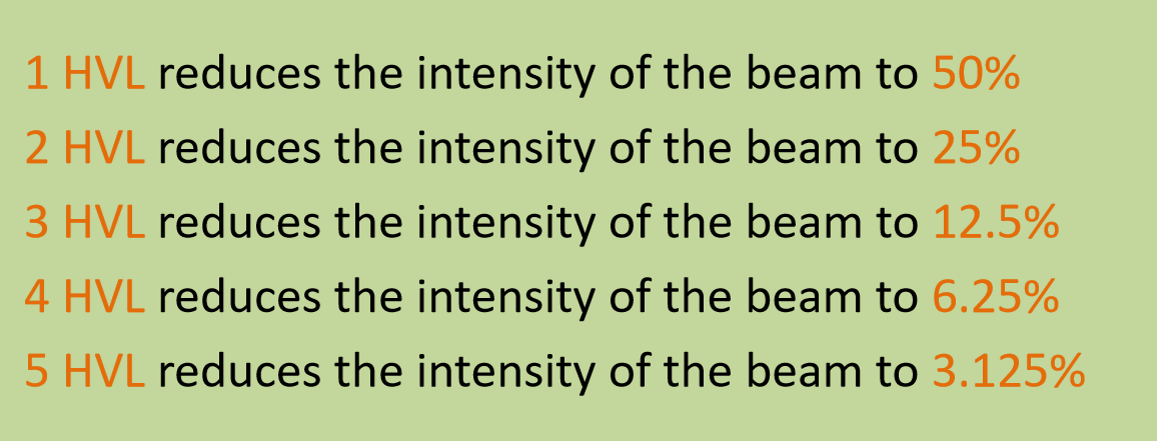
HVL
the thickness of an attenuator that reduces the intensity of the intensity of the beam to half of it’s original value
what does HVL depend on
energy of the beam
larger energy = larger HVL
type of attenuating material
5 HVL reduces the intensity of the beam to …
3.125% of its original value.
this is the standard accepted level of transmission, so shielding blocks were made with 5 HVLs
Lead HVLs for various energies of lead
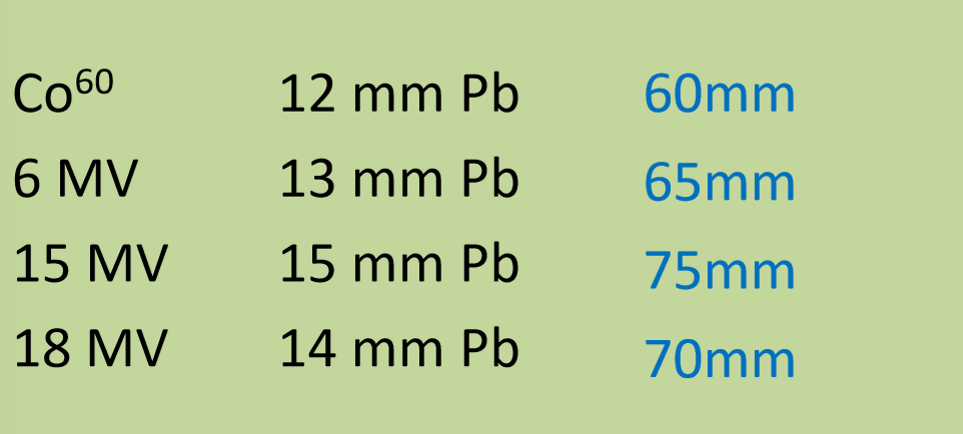
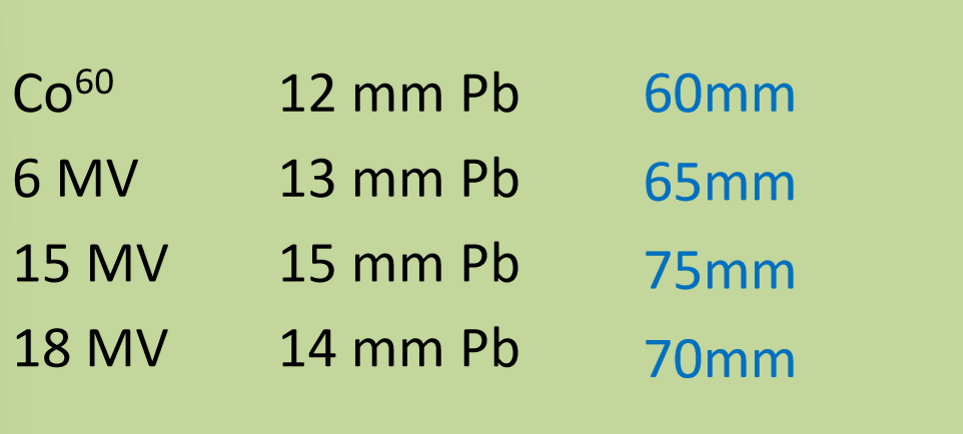
why is the HVL for 18 MV less than 15 MV
we get more pair production at 18 MV
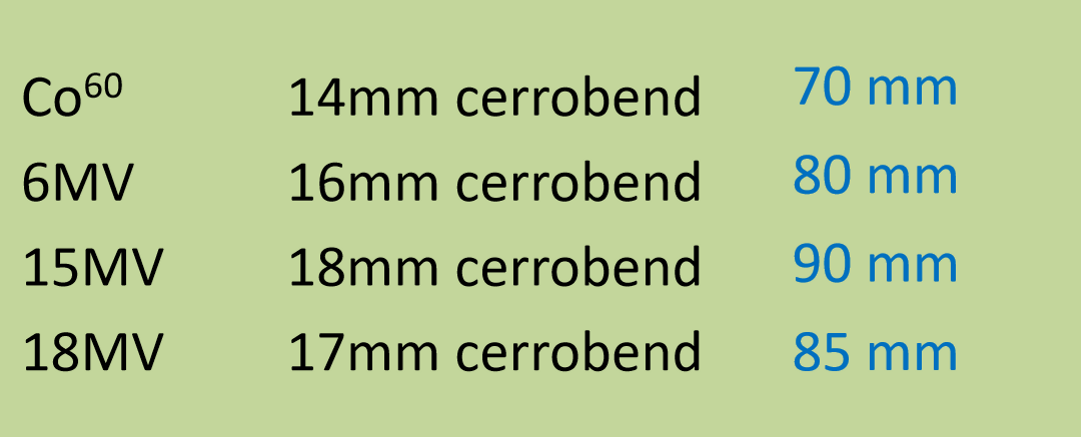
HVLS for various energies using cerrobend
not as good as an attenuator as lead, thus the blocks had to be larger
although blocks are nearly obsolete, when would we use cerrobend and lead
field shaping in electron/ortho for superficial treatments
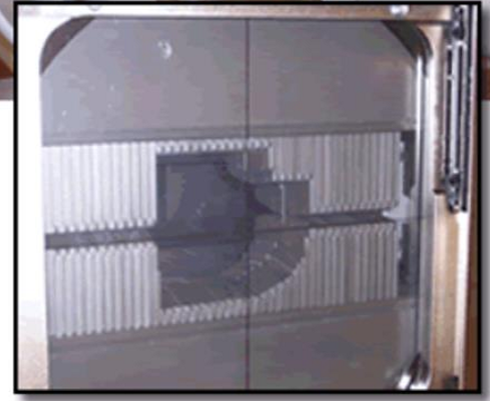
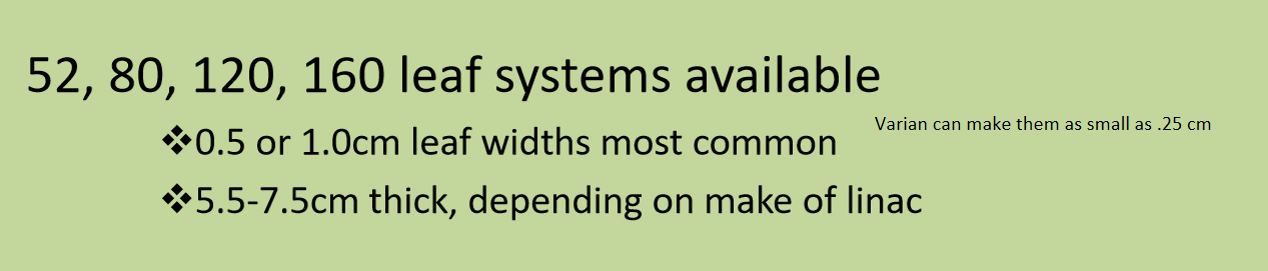
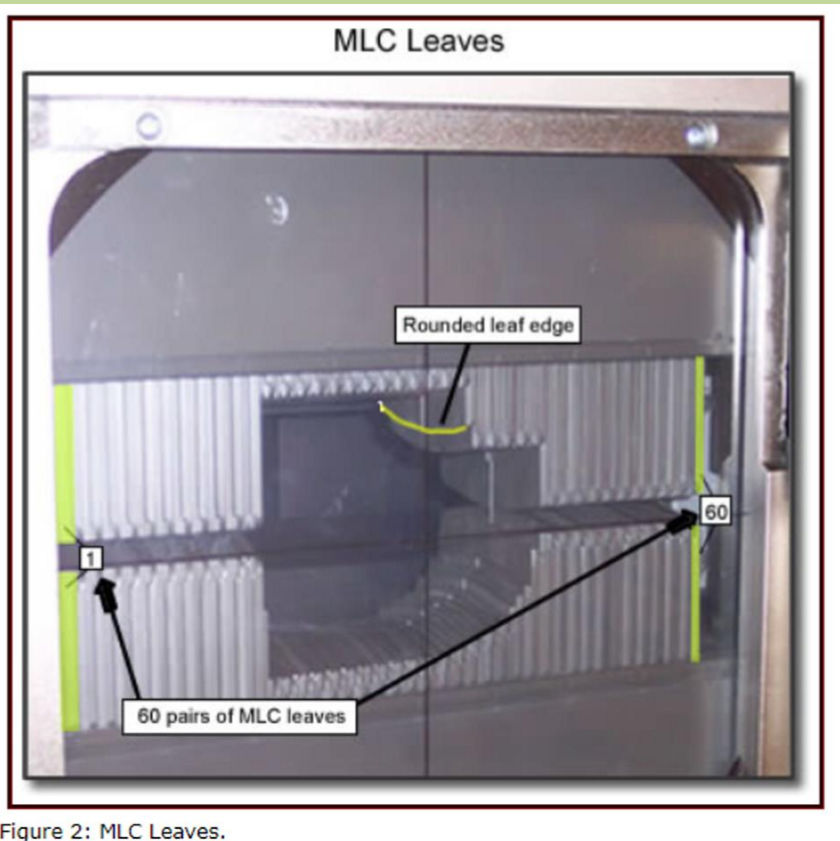
What are MLCs
tungsten leaves/rods which move independently in and out of the field to shape it
located in the head of gantry after the collimator jaws
if there are 120 leaves, the machine is called caled ‘60 pairs’
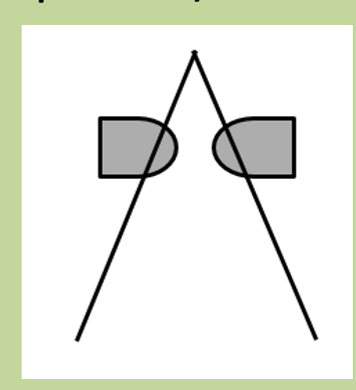
are MLCs divergent or non-divergent
non-divergent
Advantages of MLCs over blocks
tungsten = good attenuator
don’t need to lift heavy block
no storage issues
not toxic
Disadvantages of MLCs compared to blocks
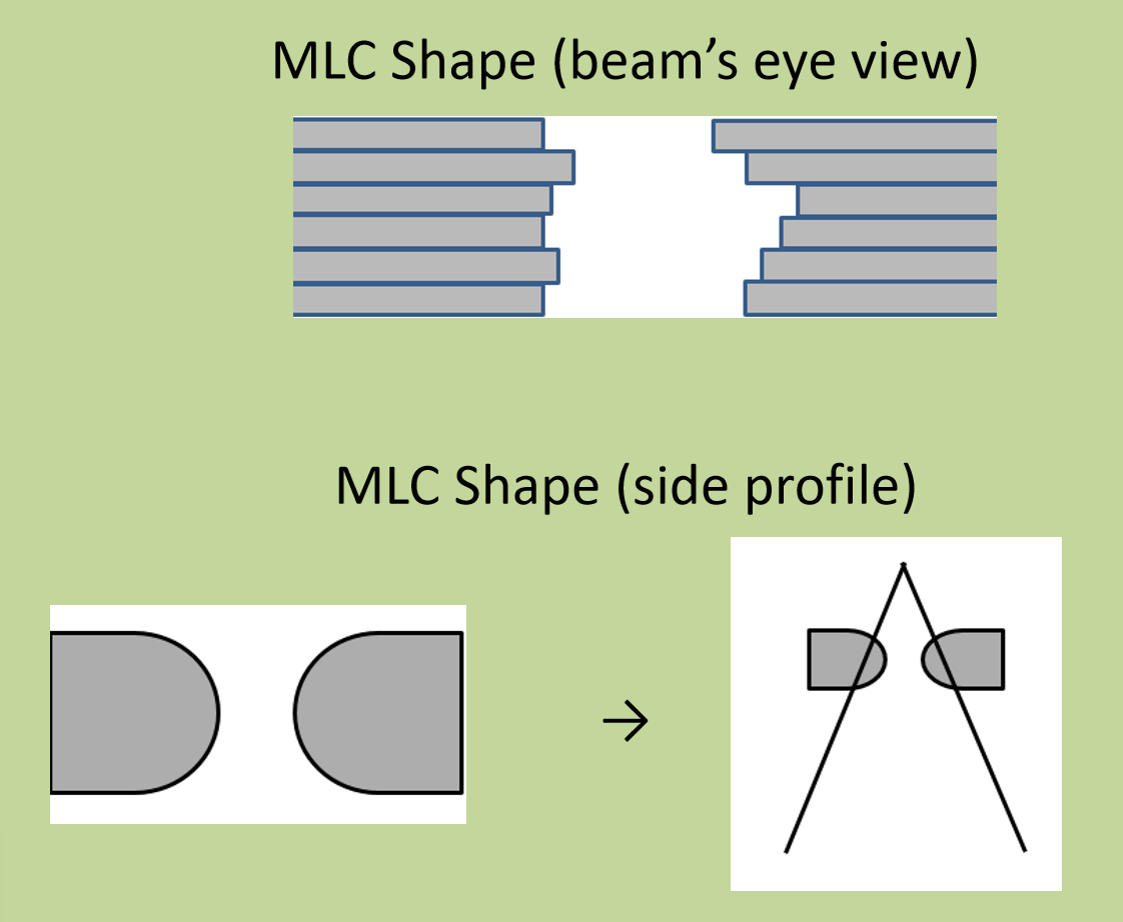
jagged shaping causes squared off ends
not necessarily a problem, but needs to be accounted for
not beam divergent (since the ends of the MLC leaves are rounded)
roundal shape and penumbra effects
can experience mechanical isues
planning considerations that need to be taken into account with MLCs
shaping considerations
Non-Divergen MLC leaves
single plane MLC system
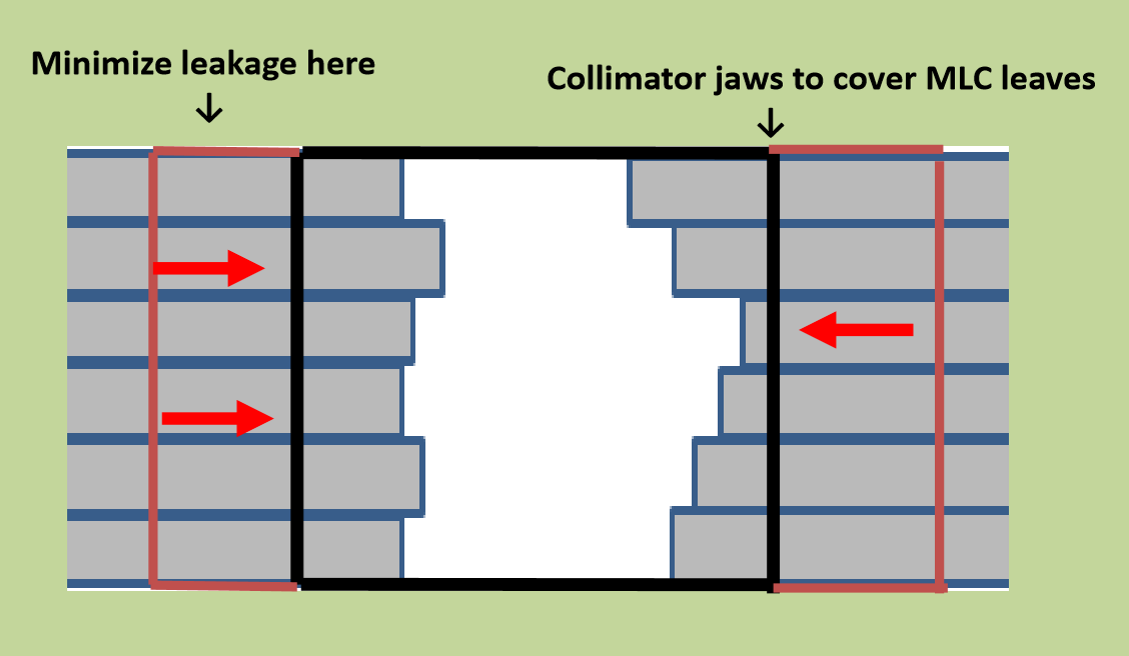
leakage between leaves
If there is leakage between leaves, how can this be fixed
fix with collimator jaws to adjust the beam margin
Primary Radiation
photons have not interacted with anything other than air before they reach the patient
scatter radiation
primary photons have hit something and interacted
involves a change in direction of the particle
not useful for tx purpopses
is there lots of scatter with with primary photons once inside the tissue
Yes, once primary photons enter tissue, they scatter significantly, reducing the effectiveness of the beam.
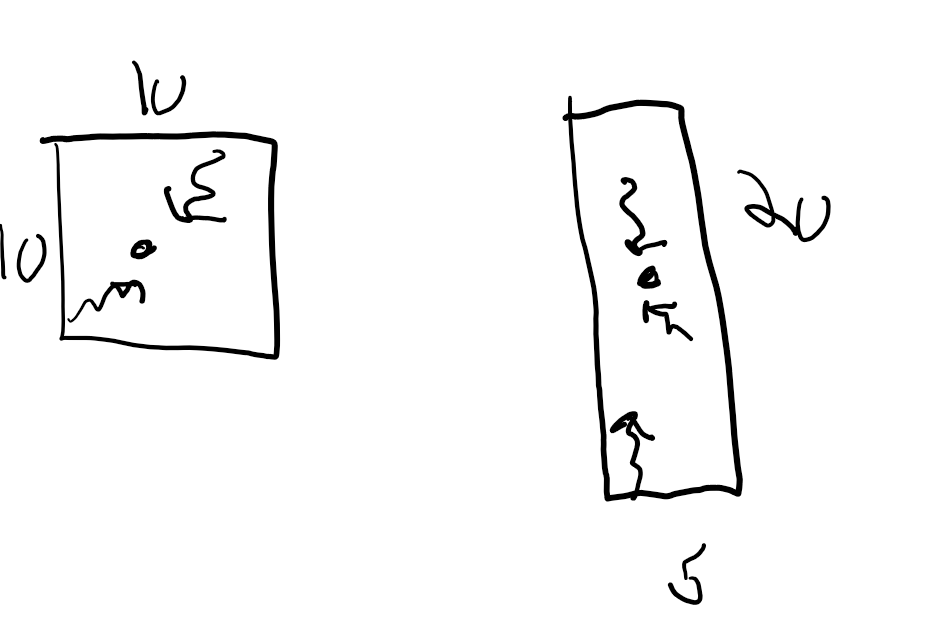
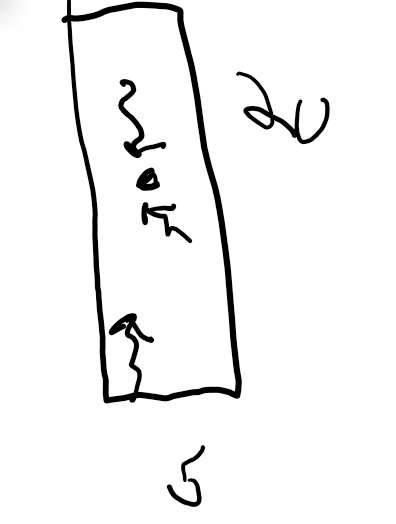
how does scatter differ with field size
Long rectangular field scatter may not get back to the calc point like the 10×10 field will
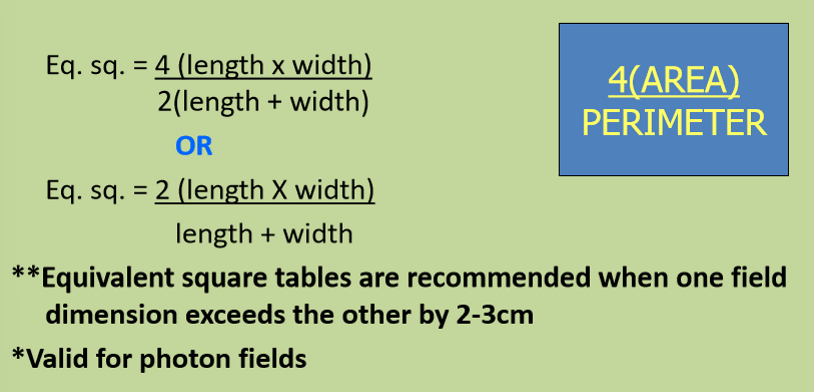
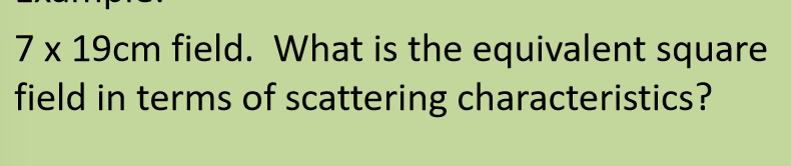
What is the equivalent square
there is a square field for every non-square field size in terms of radiation characteristics
formula for equivalent square
What is the equivalent square for a (20×5) field
Eq square = (4x(20×5)/(2(20+5)) = 8 cm x 8cm
What happens to the equivalent square when we have shielding to a field
the volume of tissue irradiated with an open beam is different than the total volume of tissue irradiated when shielding is used to block out parts of the beam
there is also a change in scatter in the treated volume
shielded area definition
the total area of all shielding within a field size
treated area definition
the remaining unshielding area within a field size
Effective field size
the equivalent rectangular field dimension of the treated area with shielding accounted for
Blocked equivalent square
the equivalent square field with shielding accounted for at the calculate depth
this is the size used in our MU calculations for tissue absopriton factors
see math problem on notes
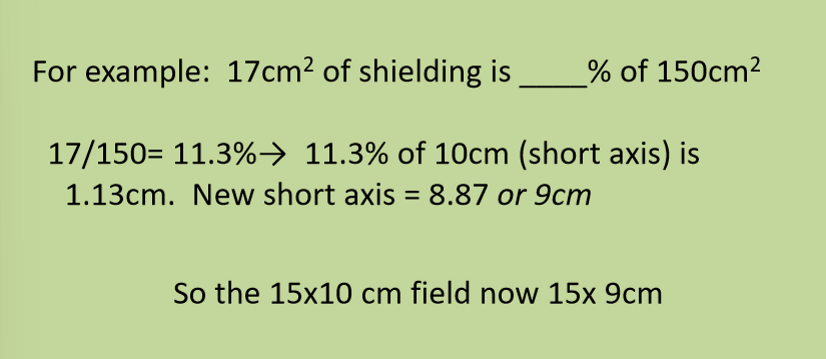
% shielded
the ratio of the total shielded area to the area of the opening field
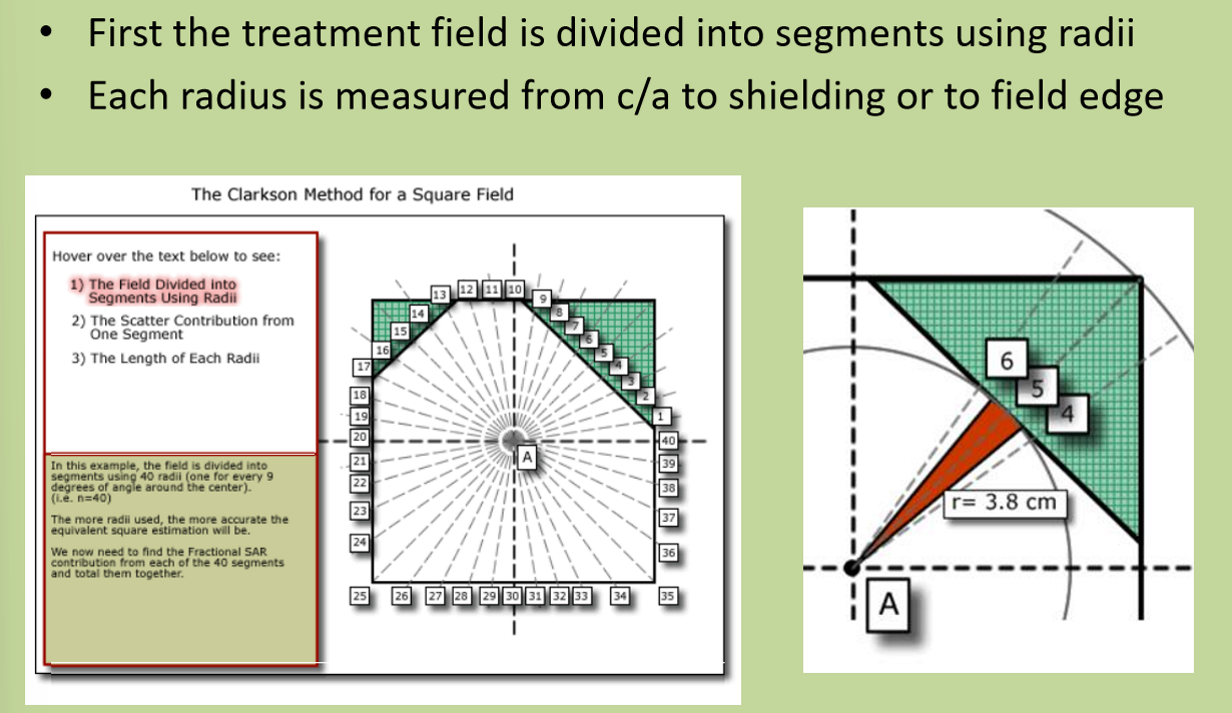
What is the Clarkson method
A technique used in radiation therapy for calculating dose distribution and patient geometry within a non-uniform field, accounting for the impact of irregular field shapes and patient contours.
this accounts for the location within the field not accounted for in blocked equivalent square method
What ratio does the Clarkson Method use
the Scatter air ratio (SAR) is used to figure out what the effect of in field shielding has on the calc point
Describe how the Clarkson Method was used to calculate the equivalent square
first the treatment field is divided into segments using radii
every 9 defrees is measured from calculation point to shielding or a field edge
using a SAR data table, each radius is looked up and an SAR is found at the depth of interest
all the SARs are added up and then divided by the # of segments (Radii) to find the average SAR
the field size with the same SAR is the equivlaent square is used in treatment calculations
when shielding is used we need to account for the change in the area being treated, and the subsequent change in scattering within the field. what needs to be done then?
the effective field size is converted to an blocked equibalent square, which is the size to be used in tx dose calculations