Transplant 101 Module 10A Social work
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
Pre-Transplant Evaluations
Look at readiness for transplant
suitable - judgemental
make a plan for people for tranpslant
expectation that are transplant specific resources for transport to and from hopsital - none
introudce to the pre and post tx team
Assesment/Evaluation
come to eval with a support person
can bring potential donor if they are a support person - will not talk about living donation with living donor person in the room
use interpreter for language barriers
people are often confused why transplant social work is necessary - dont know what they dont know about tranpslant
Used to do in person visits for those who are out of province - now that it is virtual - have to get registered with other social work colleges of other provinces
Readiness
Look at if expetations of transplant are realistic
willing for informed consent
Readiness for transplant - support
Some will over or estimate need for support
executing planned support is importance
Readiness for transplant - adherence
see that a patient has been nonadherence0 not helpful
not adherent to med, appointment, treatment
if ask patient will lie sometimes
look to see if they can have a frank convo about adherence
current adherence not a good predictor of future adherence
memorandum of understanding - lay out terms of adherence for tx in black and white
Helpful to know what adherence is composed of for support poepl e
Readiness for transplant - coping skills
how have they dealt with other challenges
stable relationships are they presen t
avoidant coping skilsl not good for tx
map out for what they need for inpatient and outpatien tusport
open to communicating with team
Readiness for transplant - substance use
Line between substance use and abuse = poor control, cannot happen
marijuna is not a contraintradication in kidney tx but is in lung

SIPAT
tool used at end of visit to asses readiness for tx objectively
each organs are differnt - transplant follow differs
psychosocial domains weight differently for differnt organ groups = some may be more hung up on issues like past substance use
Psychiatric screening
look for suicide risk
look for stability for psych illness referal to pschy if needed
hospitalization a trigger
screen for anxiety and depresison
how might mental health impact adhernce - plan incase for issue
Powers of Attorney
think about who they want having this in place in case of bad events
ensure finnancial life keeps coming
back to work only if appropriate
Follow up social work care
introduce them to stuff downstrem
ask them a lot of questions - listening for health literacy, informed consent
lots of education
help them fill in the blanks - understand aspects of their care
Plans for transplant
come out of assement with plan for transplant
follow up with patietn many times to get in place
plan for questions they get called in for interepters and support people if needed
have a good plan to get to tgh at all hours
plan for visitors during hospitalization
figure out if hospitalization triggers trauma or anxiety
Post transplant social work care
in patient sw - help with discharges that are complex and referals to rehab
help to organize visits to clinic, labs and tets
retrun to work - help to return to work for recipients
support people also may have to take time off
Donor social work team
conflict of interest in seing both donor and reipeint
look for any coercion for donatoin
link to resources
look at motivation
help to ensure robust and informed consent
reiterate program requirements
anonymous requirements if living donor is anonymous and non directed
Social Work Intervention
anticipatory grief - some may sturggle with the lack of clearness of whether they will live or dye - recipients prep for both
inpatient unit - only work with complex uses - can arrange family meetings and refer to toerh team memenrs
opeate on referal bases post tx- only funded for two years post tx but will see whenever
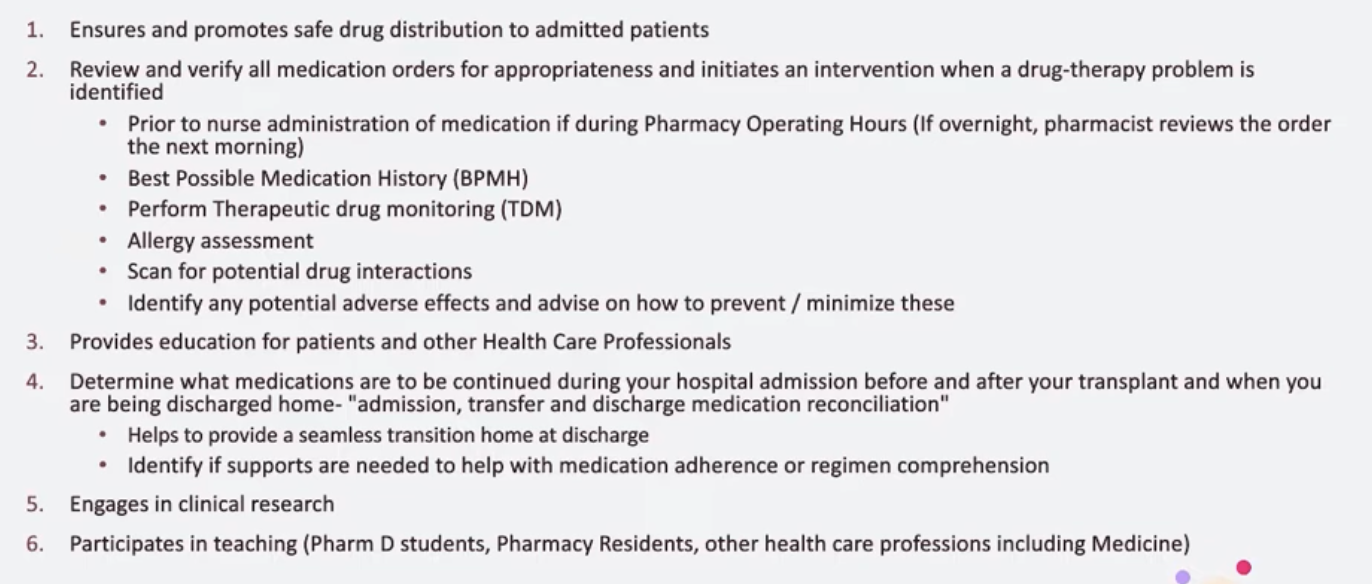
Transplant pharmacist
promote safe drug distrinbution for patien
review drug orders and point out if safety issue comes up- befor nurse given - cannot access by nurs before pharmacist looks at it - encourage nurse to not overrride
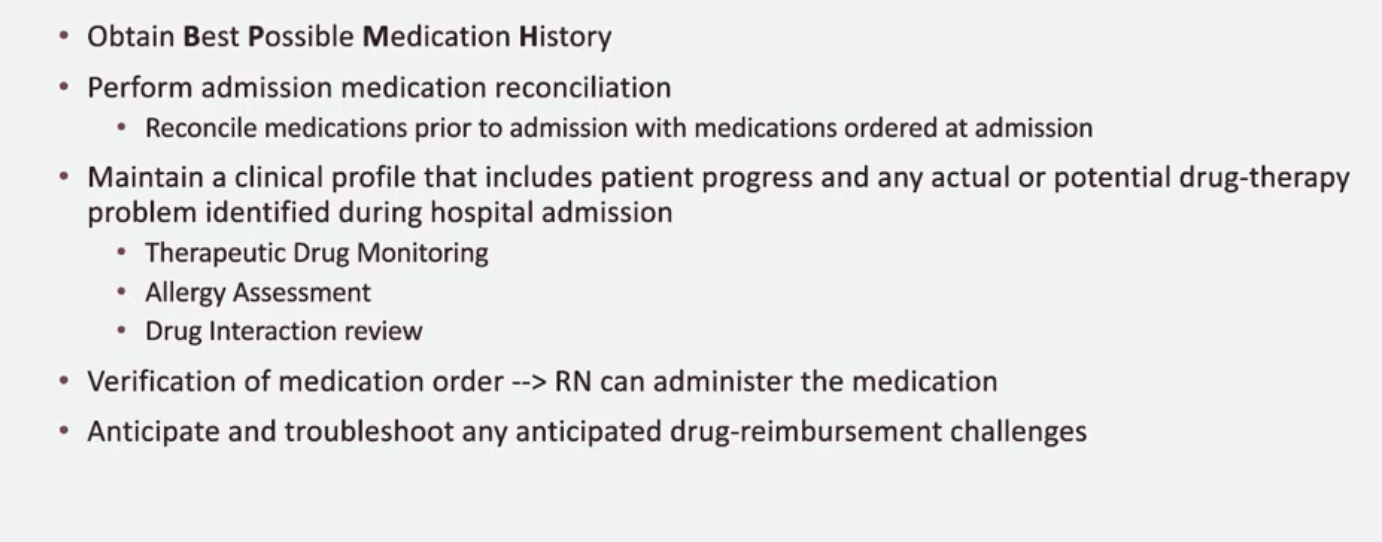
obtain a medication history - use pharmacy record, goverment billing - patient or person redocrd - at least 3 sources
look for drugs like vancomyocin that have a narrow therapeutic window
patient and provider education
determine what meds to be continued during admision in hopsital and what going home on
second pair of eyes
identify supports for adherence
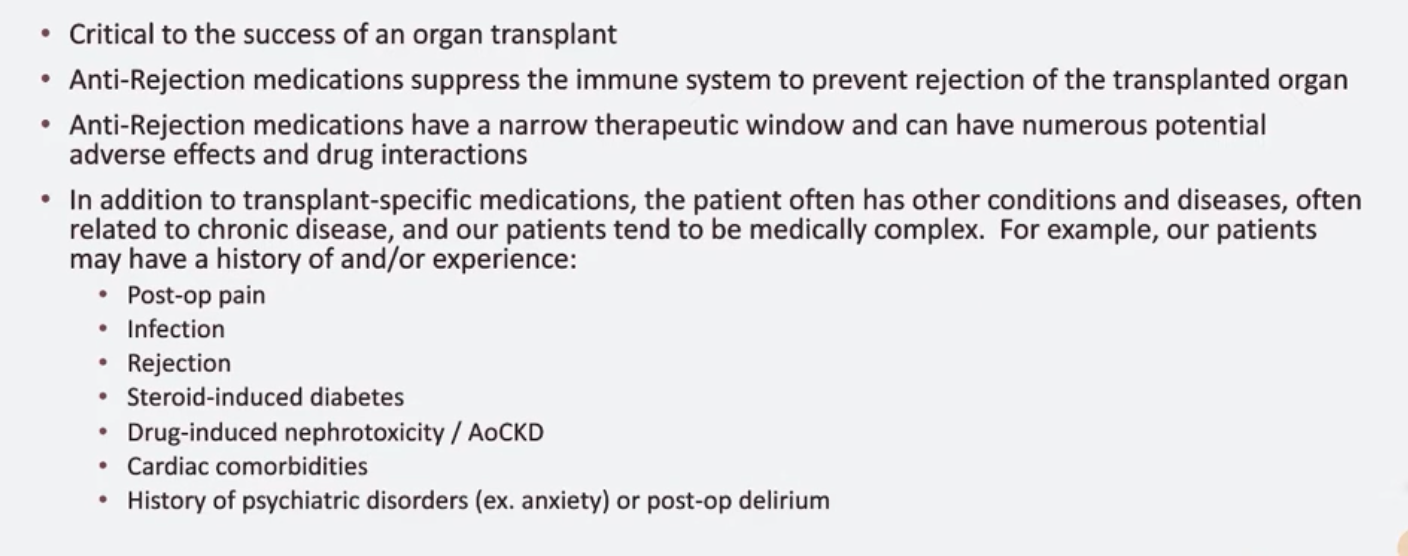
Transplant medications
meds and med aherence critical to success
meds have narrow therapeutic windo
patients have other conditions that need to be managed alongside tranpslant - high rate of comorbidities
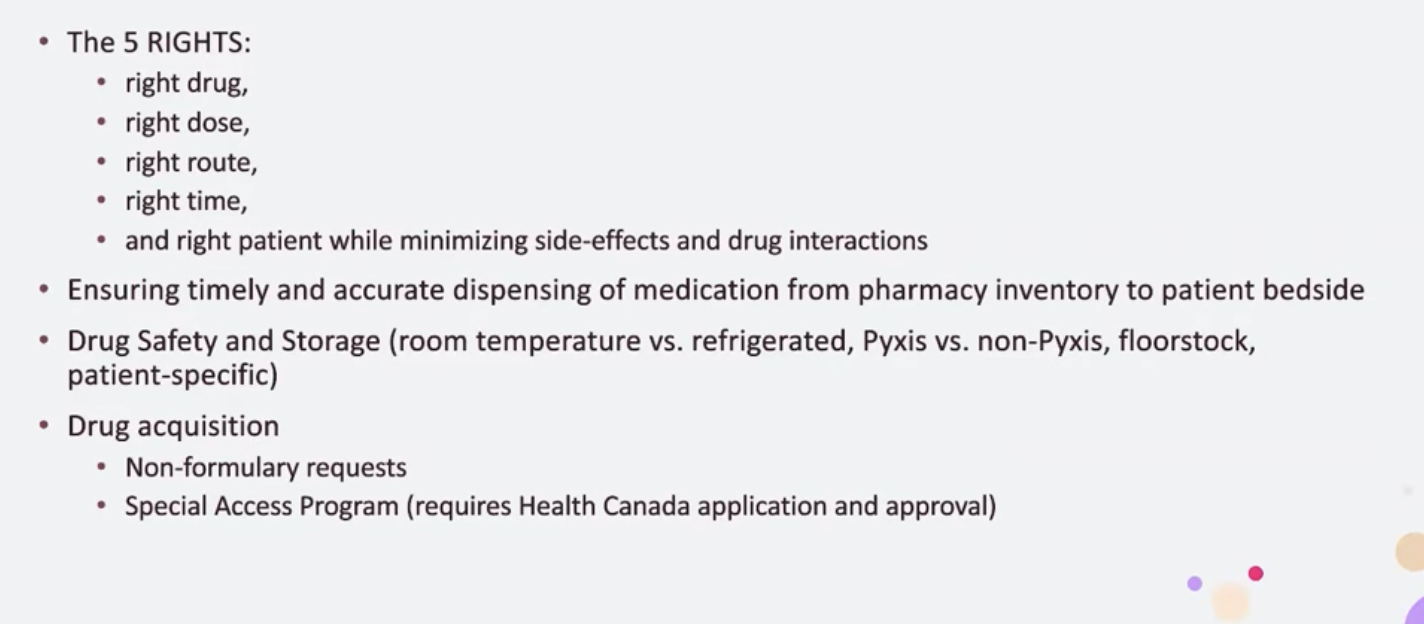
Drug distribution
very complex operational system
has to be a chain of command and safety checkpionts
pharm tech and drug information team
clincial pharmicist on floor
some drugs have storage nees like refrigeration to be met
pyxis - drug dispenser used by nurse to distribute
drug aqquition - formulary worked within - how to access outise of formulary
special access health canada - get drugs for using drug not approved in canada
Review of Medication Orders
team of 9 inpatient pharmacist to look over patients
look for therapeutic drug monitoring and issues for drug to drug inteaction
Patient education
Patients struggle to adjust from dialysis to wrap their mind around having tx
help patient learn new normal
self medication program
sometimes patietns struggle to understnad how to make a dose change
have patients practice taking meds under nurse for the rest of stay
practice changing meds for when they go home
TMITT - virtual patient education platform for tx meds

Discharge planning
reconcile meds given in hospital and choose which ones going home
help patient set up dossette or blister pack
have the only tranplant pharmacy in canada - do blister packing - support patient bring up
Clinical nutrition team
diffrent dietians for differnt organ groups
nephrology dietitian - help with patients on dialysis again adjust diet
diet technician - knows hospital menu - brings food to patients
RD Role
see patients through tranpslant process
Dietetics before transplant
lung and liver assesd
lung is asses as there is a narrow weight range to make the transplant surgery safe
look at weight history and changes - see if had a lot of weight gain or lost
look at medical history - concernts like
food acces and preparation - patients with lung disease cannot go to grocery during covid - can they prep food.
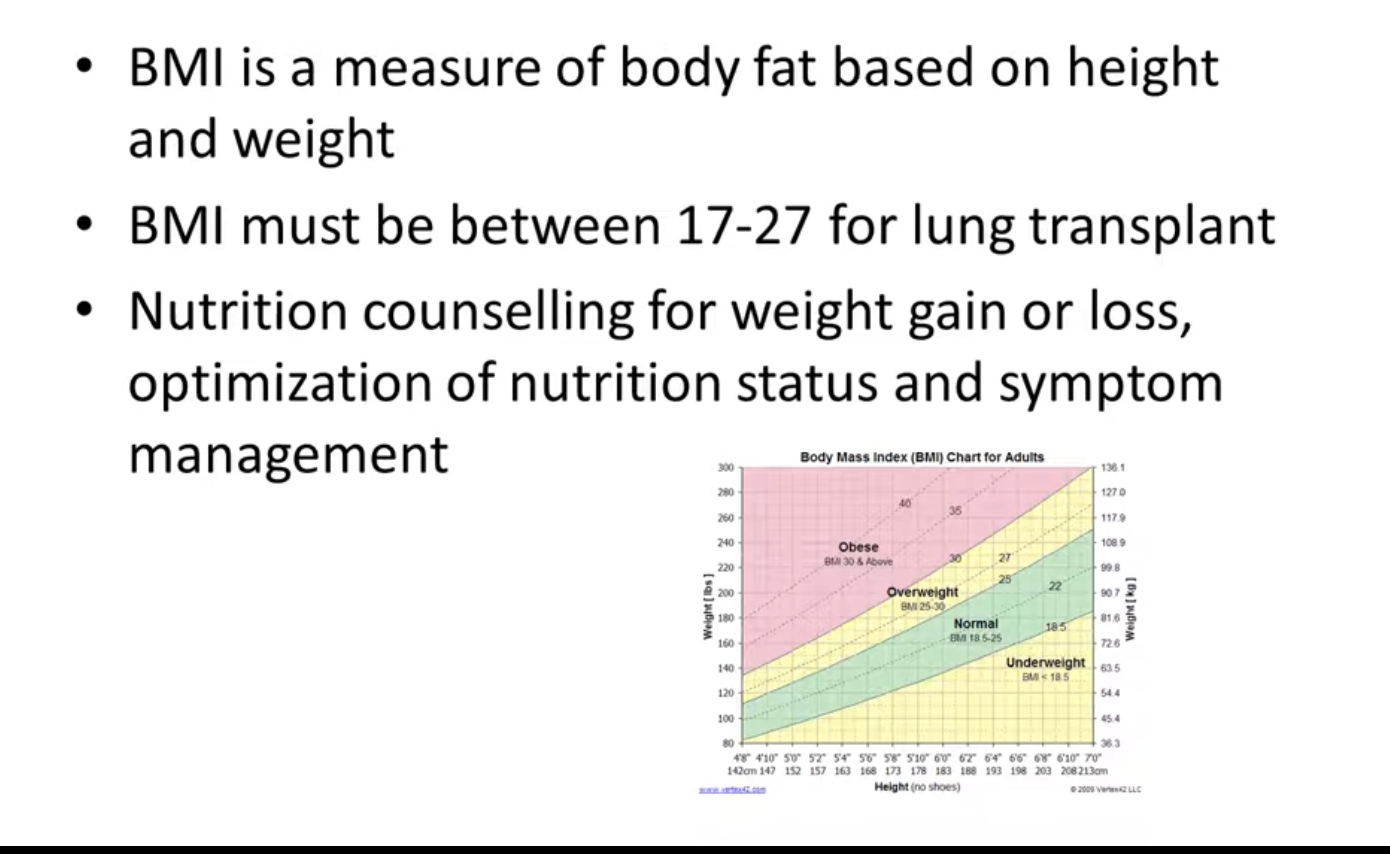
BMI
healthy bmi - better tranpslant outcome s
sometimes patients struggle to have enough weight to get thorugh tranpslan t
help patients eat healthy
Dietetics post op as an inpatient
low nutrition befor transplant - cannot eat before or after tc - issues with nutrition
gastroparesis - slow stomach empyting - patients struggle to keep weight on
getting patients to a point where if tey are on liquid nutrition or an ng tube work with slp to add in oral food safely
Types of nutrition through ng tube
special one to be usef for renal patient s

After discharge
nurse will flag patietns with dietitan issues
sterois increase appetite - patients eat more because they are feeling better
low physical activity post tx
low potassium and collestal
how tomanage blood sugar and vitamin c to stop loss of bone
support food safety as it can be really bad for patients
Food safety
avoid unpasteruex milk or yogurt
no runny eggs, soft chese or raw sprouts