BIOL 2200 Module 8: Neurological Disorders
1/64
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
65 Terms
Consciousness
State of being aware of one’s self and the environment, plus being capable of orienting to new stimuli
Which two components is consciousness divided into?
Arousal (wakefulness) + content and cognition
Arousal (wakefulness)
State maintained by the reticular activating system (RAS)
Reticular Activating System (RAS)
Diffuse network involving the brainstem and a functioning cerebra cortex
What does a loss of arousal indicate?
It indicates injury to the RAS or to both cerebral hemispheres
Does injury to one cerebral hemisphere typically lead to loss of arousal?
Injury to one cerebral hemisphere typically does not lead to loss of arousal
Selective attention
The ability to selectively process certain information
Executive attention
The ability to sustain attention, remember instructions, and possess self-control
Coma
Unarousable state
Stupor
State only arousable to pain
Obtundation
“Sleepy” state
Delirium
State of restlessness, hallucinations, and delusions
Glasgow Coma Scale
A scale that scores patients based on eye opening, verbal response, and motor response to indicate their LOC
Is a Glasgow Coma Scale score of 0 possible?
A score of 0 is NOT possible!
Brain death
State where no recovery is possible, and the brain cannot maintain homeostasis. No motor reflexes, cannot breath properly, lack of other causes (e.g. shock)
Cerebral death
Irreversible coma where brain stem may maintain homeostasis
Persistent vegetative state
Unawareness of self or surrounding environment, BUT sleep-wake cycles and brain stem reflexes are intact
Minimally conscious state
State where individuals can follow simple commands and gesture
Locked-in syndrome
Full paralysis of voluntary muscles EXCEPT eye movement
Cheyne-stokes breathing
Result of higher brain injury, characterized by periods of apnea and tachypnea, in response to levels of carbon dioxide in blood (irregular breathing pattern)
Neurogenic hyperventilation
>40 breaths/minute from midbrain injury where inspiratory/expiratory centers are continuously stimulated
How do pupils appear in severe hypoxia?
They appear dilated and fixed
What does damage/pressure to one oculomotor nerve cause?
A “blown” or non-responsibe pupil
Oculocephalic reflex
Movement opposite from head movement. Abnormal if eyes follow head movement or move independently (only assessable in comatose patients)
Decorticate posture
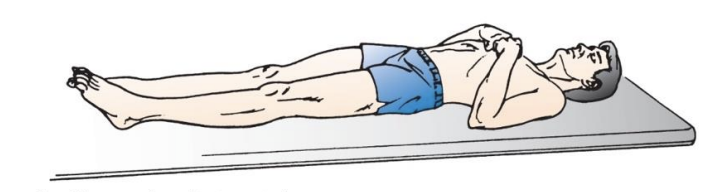
Posturing where upper extremities are flexed at elbows and lower extremities are rotated inwards and extended (gasp)
What typically causes decorticate posture?
Severe cerebral hemisphere damage
Decerebrate posture
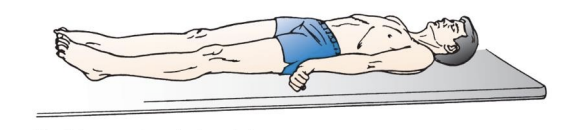
Increased tone in certain muscles, clenched jaw, extended neck. All four limbs rigidly extended
What typically causes decorticate posture?
Brain stem lesions
Seizure disorder
A sudden, extreme, and abnormal discharge of cerebral neurons causing a temporary change in brain function. E.g. uncontrollable convulsions
Focal seizure
Seizure beginning at one side of the brain
Generalized seizure
Seizures involving both sides of the brain
Staring spells
Generalized seizure where the body does not shake. Often goes unnoticed
Agnosia
Inability to recognize form/nature of objects. Typically only affects one sense
Hemineglect
Inability to react to stimuli coming from the opposite side of damage. Will not orient or reach to neglected side
Dysphasia
Inability/insufficient ability to understand words or symbols. From dysfunction in left cerebral hemisphere
Aphasia
Inability to communicate. Interchangeable with dysphasia
Broca’s aphasia
Damage to brain area responsible for language production (speaking)
Wernicke’s aphasia
Damage to brain area responsible for language comprehension (understanding)
Common causes of Increased Intracranial Pressure (ICP)
Tumors, edema, hemorrhage
Monro-Kellie hypothesis
Hypothesis stating that increased intracranial pressure is compensated by reduction in other cranial contents. E.g. blood volume or CSF
Stage 1 of intracranial hypertension
CSF is displaced into spinal subarachnoid space → Compression of venous system
Stage 2 of intracranial hypertension
Swelling increases in ICP → decrease in brain tissue perfusion → hypoxemia → confusion * Cushing’s reflex
Cushing’s reflex
Systemic vasoconstriction in response to overcome decreased flow in the brain. Associated with intracranial hypertension
Effects of Cushing’s reflex on BP, HR, RR
BP → increases
HR & RR → decreases
Stage 3 of intracranial hypertension
Cerebral perfusion pressure falls → hypoxia and hypercapnia of brain tissue → deterioration in functions
Stage 4 of intracranial hypertension
Brain tissue herniates 9shifts) from the compartment of higher pressure to a compartment of lower pressure. ICP equals systolic arterial pressure
Consequence of ICP equalling systolic arterial pressure
Cerebral blood flow ceases, causing death
Brain herniation
Where increased pressure pushes brain tissue out of its normal position. Such as from ICP
Cerebral edema
Increased fluid content causing increased brain tissue volume
Vasogenic edema
Where increased blood-brain-barrier permeability leads to leak of plasma proteins and increased tissue water content
Which brain matter does vasogenic edema typically occur in?
White matter
Which brain matter does cytotoxic edema typically occur in?
Grey matter
Hydrocephalus
Excess fluid in ventricles and/or subarachnoid space. Caused by excess CSF or little CSF reabsorption
Noncommunicating hydrocephalus
Where obstruction (inflammation) prevents CSF from reaching arachnoid villi and being reabsorbed
Communicating hydrocephaluw
Failure of CSF reabsorption from reduced or scarred arachnoid villi from meningitis.
Also overproduction of CSF by adenomas of choroid plexus
Muscle tone
Normal muscle tension that enables controlled movement