HCP CPR, Obstructed Airway
1/29
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
30 Terms
Obstructed Airway and Choking
In a life-threatening emergency, an airway may be blocked by food, blood, vomit, or the victim’s tongue falling back. Manual airway procedures (head-tilt chin lift or jaw thrust) or the recovery position can resolve these issues. For conscious victims, abdominal thrusts are used to dislodge food or particles. For unconscious victims, chest compressions are performed.
Choking victim
conscious victim
Unconscious
Conscious choking
Ask the following questions:
Are you choking?
Can I help you?
Are you pregnant (if appropriate)?
Note: Infants & small children who cannot speak (because they are not old enough) should be visually assessed for:
Skin color.
Muscle tension (flaccidity indicates airway obstruction).
Ability to cry or make sounds (weak cry indicates significant obstruction)
Determine degree of obstruction (see below)
Start first aid for a conscious chocking victim (see below).
Unconscious choking
Pinch & Shout
If unresponsive call 911
Open Airway (use appropriate method) Assess for spontaneous respirations (no more than 10 seconds)
If no spontaneous respirations attempt to provide 2 breaths, breaths should be over 1 second with just enough air to make the chest rise.
If the first breath does not make visible chest rise, re-attempt to open the airway and re-attempt to provide ventilation.
Start first aid for an unconscious chocking victim (see below).
Degrees of airway obstruction
good air exchange
poor air exchange
No air exchange
Good air exchange
The person can speak.
Coughing and gagging are effective and forceful.
Facial color is reddish.
Encourage to cough
Poor air exchange
the person cannot speak.
coughing and gagging are ineffective and weak.
you may hear a high-pitched whistle when he/she tries to cough or breath.
facial color becomes bluish due to decreased oxygen.
Start first aid for choking
No air exchange
The person cannot speak.
Coughing and gagging are impossible.
There will be no sound as the person cannot breathe.
Facial color is bluish due to lack of oxygen.
Start first aid for choking. Continue until Emergency Service arrives and take over.
First aid choking (adult and child victims)
conscious
Unconscious victim
Conscious (choking adult, child)
Consider calling 911
Landmark for abdominal thrusts.
Position yourself behind the victim.
Place one of your feet between the victims’ feet.
Lean the victim slightly backwards onto your shoulder.
Imagine a line across their hips; place the inside of a closed fist on the imaginary line. Use your free hand to cover your “fisted hand” and direct the abdominal thrusts.
Note: For small children if your fisted hand” is too large straighten out your fingers and use the “blade” of your hand (guided by your free hand) to perform abdominal thrusts.
Perform abdominal thrusts (inward & upward).
direct thrusts into the abdomen and
up into the diaphragm / chest
Note: Abdominal thrusts should be done forcefully with the intent to dislodge the obstruction.
Continue abdominal thrusts until the victim’s airway is cleared or the victim becomes unconscious.
If the obstruction is relieved refer the casualty to medical assistance.
If the victim becomes unresponsive call 911 and begin first-aid for an obstructed airway.
Unconscious victim (choking adult, child)
Scene Management & assessment as outlined above (obtain consent);
Call 911
Perform a tongue-jaw lift.
Look for the obstruction.
Perform a finger sweep only if you can see the obstruction.
Attempt to ventilate - If no air goes in, re-position the head and attempt to ventilate again.
Give 30 chest compressions (same landmark as CPR).
Repeat step 1 (A. B. C. & D.), until the obstruction becomes dislodged, or Emergency Service arrives and take over.
Note: If the obstruction is cleared (i.e. you are able to ventilate the victim) reassess the victim and perform artificial or assisted ventilation or CPR as required based on patient assessment. Place the spontaneously breathing & moving victim into the recovery position to maintain airway.
First aid choking (obese, pregnant)
If the victim is obviously pregnant, you want to avoid abdominal thrusts because they will be ineffective at clearing the airway. Alternatively, you can do chest thrusts on this conscious victim.
In order to landmark for chests thrusts on a conscious casualty,
Position yourself behind the victim.
Place one of your feet between the victims’ feet.
Lean the victim slightly backwards onto your shoulder.
Have her extend her arms horizontally out to her sides and landmark for chest compressions:
You must extend your arms forward under her arms.
Bring your hands together in front of her in the same formation you would for abdominal thrusts on a conscious casualty and center your fist on the sternum of her chest (same position as CPR).
Pull straight back to depress the chest 1.5-2 inches.
If the victim becomes unconscious lower them to the ground and initiate first-aid for an unconscious chocking victim as previously outlined.
Note: If a pregnant victim becomes unresponsive the steps remain the same as outlined above. Consider raising or placing something (at the upper hip and abdomen), such as a rolled blanket to raise the right side of the victim. This will shift the unborn baby off of the main vein returning blood flow to the heart. In some cases, blood flow back to the heart can be reduced by up to 40% if a pregnant victim is left flat on her back.
** Choking procedures can and do save the lives of people choking, but there are some risks involved. Occasionally, the patient experiences internal injury. Although this is not always the case, we must always insist that they be checked out at a hospital. You do not want to wait if there is something wrong. That is also why we only simulate the procedure in practice.
First aid choking (birth → year)
Conscious (with poor or no air exchange)
Unconscious infant
Conscious (with poor no air exchange) - choking infant
Scene Management & assessment as outlined above (obtain parental consent);
Consider calling 911
Carefully turn the conscious infant into a front and face down position and administer back blows followed by chest thrusts (you will need to turn the infant again).
Back blows – Place your arm between the infant’s legs with the infant’s jaw in your hands, supporting the jaw firmly. Brace your forearm against your thigh with the infant’s head lower than its body. Use the heel of your hand to give 5 back blows between the infant’s shoulder blades.
Chest thrusts – Continue to hold the infant in the same position as above, placing your free arm along the infant’s spine (sandwiching the infant). Support the head as you turn the infant over against your thigh. The baby will now be face up. With its head lower than its body, use two fingers in the center of the breastbone, 1 finger width below an imaginary horizontal line across the nipples. Give 5 quick chest thrusts ½ - 1” deep.
Continue with the sequence of 5 back blows and 5 chest thrusts until the obstruction is dislodged or the infant goes unconscious.
If the infant becomes unconscious, call 911 and place the unconscious infant on their back on a firm flat surface. Go to unconscious infant choking protocol.
Unconscious infant (choking - infant)
Scene Management & assessment as outlined above (obtain parental consent);
Call 911
Perform a tongue-jaw lift.
Look for the obstruction.
Perform a finger sweep only if you can see the obstruction.
Attempt to ventilate - If no air goes in, re-position the head and attempt to ventilate again.
Landmark and perform CPR as previously outlined within this program. After 30 compressions repeat step 1 (see above) in an effort to clear the obstruction before ventilating.
Statement regarding first aid for unconscious choking victims
Unfortunately, once a victim of choking becomes unresponsive or is initially found unconscious it is very difficult to clear their airway. The procedures for adults, children, and infants outlined above give first-aid providers the best chance at relieving the obstruction and clearing the airway. Often unconscious victims of choking require advanced medical procedures to relieve and clear their airway. Remember the chain of survival; call 911 as soon as possible.
CPR
is a simple emergency first aid procedure (chest compressions and rescue breaths) for a victim of cardiac arrest; it is part of the Chain of Survival. CPR is also performed as part of the choking protocol if all else has failed.
Chain of survival
Refers to four universal steps that increase the chance of saving a victim of cardiac arrest when followed. Like all chains, the Chain of Survival is only as strong as its weakest link. The chain of survival OHCA – Out of Hospital Cardiac Arrest

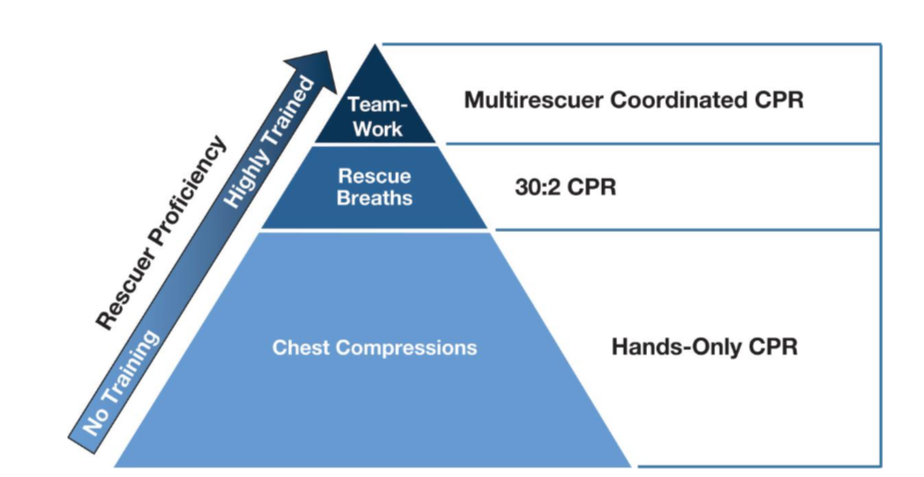
Rescuer proficiency
Guidelines for CPR
Infant victims (less than 1 year of age).
Child victims (between 1 and 8 years old).
Adult victims (over 8 years old).
Age guided classifications
have been maintained for lay rescuers. This was done to maintain consistency with previous guidelines and to allow for focus to be concentrated around more important aspects of CPR regarding lay rescuer CPR programs. Rescuers use the following guidelines to determine the most appropriate CPR protocol for victims of cardiac arrest.
Infant victims (less than 1 year of age).
Child victims: Child CPR guidelines for healthcare providers apply to victims from about 1 year of age to the onset of adolescence or puberty (about 12 to 14 years of age) as defined by the presence of secondary sex characteristics.
Adult victims are those that no longer meet the above-mentioned child victim criteria.
Note: Hospitals (particularly children’s hospitals) or pediatric intensive care units may choose to extend the use of Pediatric Advanced Life Support (PALS) guidelines to pediatric patients of all ages (generally up to about 16 to 18 years of age) rather than use onset of puberty for the application of ACLS versus PALS guidelines.
CPR
(The victim is unresponsive, and has no spontaneous respirations, and no signs of circulation).
The most current research regarding CPR
good quality CPR improves a victim’s chance of surviving cardiac arrest. HCPs should work through this updated material and practice the principles outlined within it.
The critical concepts to remember and assimilate into CPR procedures are:
Push hard, push fast.
Allow full chest recoil after each compression.
Minimize interruptions in chest compressions; make every effort to keep interruptions to less than 10 seconds.
Avoid hyperventilation.
How many people can do CPR
performed by one or two rescuers; because brain cells start to die in as little as 4 minutes without adequate oxygenation, it should be started quickly and must be performed adequately. Practice makes perfect!
CPR (adult)
Position the victim on their back, on a firm flat surface to facilitate the delivery of CPR.
Deliver adequate chest compressions (100-120 per minute, 5-6 cm deep with full chest recoil between compressions), followed by two (2) ventilations.
For Adult victims with one or two rescuers, provide thirty (30) compressions at a rate of up to 120/min, 2” in depth, followed by two (2) ventilations. Ensure an open airway prior to ventilating (after 30 compressions).
Compressions should be 2 inches deep, but not more than 2.4 inches in depth.
CPR (child)
provide thirty (30) compressions at a rate of at least 120/min. 1.5” in depth for children and 140/min, 1” in depth for infants, followed by two (2) ventilations. When two rescuers are available, (for children & infants) one should deliver fifteen (15) chest compressions (at a rate of 100/min), the second should maintain an open airway and deliver 2 ventilations during the brief pause after compression delivery.
Compressions should be 1/3 the depth from the anterior (front) to the posterior (back) of the victim.
For small infants consider using the 2-thumb encircling hand technique if trained to do so.
Most effective two person
To ensure adequate compression delivery is maintained, the two rescuers should switch between ventilation and compression roles frequently. The switch should be done with as little interruption (in compressions) as possible. If the second rescuer arrives after one rescuer has started CPR, they should ensure 911 have been called prior to assisting with the delivery of CPR.)
Critical concepts of
Chest compressions should be delivered HARD & FAST; however, it is equally important to ensure adequate/full chest recoil between each compression.
Interruptions in chest compressions (for ventilation, switching rescuers, etc.) should be kept to a minimum (not more than 10 seconds) because every interruption decreases the amount of manually circulated blood in the victim’s body.
Studies show that HCPs as well as lay rescuers are unable to reliably detect a pulse and at times will think a pulse is present when there is no pulse. For this reason, if you do not definitely feel a pulse (i.e. there is no pulse or you are not sure you feel a pulse) within 10 seconds, proceed with chest compressions. HCPs should try to palpate a pulse (brachial in an infant, carotid or femoral in a child, carotid in an adult). Take no more than 10 seconds!
Recovery position
A maneuver which rolls an unconscious, breathing victim on to their side to maintain an open airway and allow for drainage of saliva and vomit out of the mouth instead of down into the lungs. The recovery position is appropriate when a victim is unconscious but has not suffered cardiac arrest (they are still breathing and have good signs of circulation) or for a victim that received CPR and/or AED treatments and began to breath on their own with spontaneous movement of limbs. The technique for placing a victim into the recovery position is.
Kneel beside the victim at their chest.
Place their arm closest to you upward lengthwise along their head.
Bend their knee on the opposite side to you to make an A- frame.
While cradling the head and keeping the head and neck in alignment with their shoulders pull the “A-frame” bent knee towards you and down and turn the victim onto their side.
Adjust the victim’s top arm so that their hand is resting under their cheek to keep the airway open.
Monitor the victim closely for cardiac arrest (re-assess frequently), if this occurs turn them on to their back and start CPR.