Chest - regional anatomy
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
26 Terms
bones of the thorax
sternum
costal cartilages
24 ribs
12 thoracic vertebrae
diagram of bones of thorax
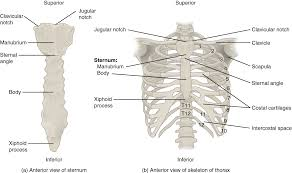
features of thoracic cage
sternum - long flat bone, composed of manubrium, body and xiphoid process
true ribs - ribs 1-7: articulates with sternum directly
false ribs - ribs 8-12: articulates to costal cartilages of the ribs above
floating ribs - ribs 11 and 12: articulate with vertebrae only
boundaries of thorax - thoracic inlet
boundary between neck and thorax. Bounded posteriorly by T1, anteriorly by manubrium, and laterally on each side by 1st rib
boundaries of thorax - anterior and lateral walls, and floor
Anterior wall - formed by sternum, costal cartilages and anterior ends of the ribs and intercostal muscles
lateral wall - formed by ribs and intercostal muscles
floor - formed by diaphragm
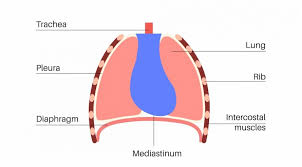
contents of thorax - pleural cavities
right and left pleural cavities
pleura - visceral, parietal
right lung - 3 lobes
left lung - 2 lobes
each lung has; apex, base, costal surface and medial surface with a hilum
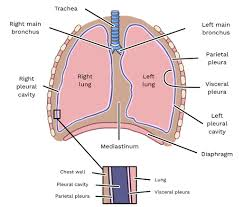
contents of thorax - mediastinum
The potential space between lungs, consists of organs/structures of following systems;
cardiovascular
respiratory
digestive
lymphatic
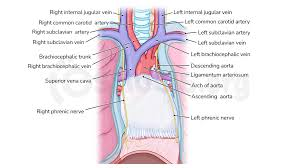
superior mediastinum
Lies above an arbitrary line drawn between the manubriosternal junction and the lower border of T4. Contents;
aortic arch and main branches
brachiocephalic artery and veins
part of superior vena cava
trachea
oesophagus
upper part of thoracic duct
thymus gland
vagus nerve
phrenic nerve
diagram of contents of superior mediastinum
Antero mediastinum
Lies in front of heart and pericardium. Contents;
loose fatty tissue
lymph nodes
internal mammary arteries
Middle mediastinum
Lies behind antero mediastinum. Contents;
heart and pericardium
ascending aorta
superior vena cava
pulmonary a
Posterior mediastinum
Lies behind middle mediastinum. Contents;
descending thoracic aorta
oesophagus
azygos veins
lymph nodes
Anatomical landmarks of Thorax
sternal notch - depression on upper border of manubrium. At level T2/3
sternal angle - Junction of manubrium and body of sternum. Level T4
Xiphoid process - small cartilaginous part of sternum which gradually ossifies during adult lift
xiphisternal joint - junction xiphoid process and body of sternum. T9
Inferior angle of scapula - lower, pointed part of scapula
lower costal margin - lower edge of thorax formed by inferior edge of ribcage. L3
Reasons for referral
lung cancer diagnosis
trauma
? pneumothorax
pericardial effusion
heart/valve disease
pneumonia
pleural effusion
shortness of breath
weight loss
chest pain
RCR reasons for referral (royal college of radiologists)
acute onset or chronic chest disease
acute chest pain
trauma
occupational health screening
pre operative assessment
post thoracic surgery
ventilated patients
Clinical conditions RCR 1998
Myocardial infarction (MI) - assessment of heart size
chest pain - exclude other causes, rarely diagnostic
acute aortic dissection - CT more helpful
chest trauma - query pneumothorax
pneumonia follow up - confirm resolution (>10 days)
Haemoptysis - +lateral
Intensive Therapy Unit (ITU) - symptomatic change
pulmonary embolus - CT or Nuclear medicine more definitive
pericarditis
pericardial effusion - US more helpful
chest trauma - if ? pneumothorax
NICE (2015) guidance changes
no longer require persistent signs or symptoms (lasting more than 3 weeks)
guidance now relates to patients over 40
Urgent CXR referral (USC)
people aged 40 and over, if they have 2 or more of these unexplained symptoms, or smokers/ex smokers if they have 1 or more;
cough
fatigue
shortness of breath
chest pain
weight loss
appetite loss
NICE (2015) urgent request for any of the following
persistent or recurrent chest infection
finger clubbing
supraclavicular lymphadenopathy or persistent cervical lymphadenopathy
chest signs consistent with lung cancer
thrombocytosis
contraindications (where something isn’t medically advised)
non specific chest pain - main purpose is reassurance
suspected rib # - doesn’t change management
pre employment screening - only justified in high risk (eg. divers)
upper respiratory tract infection - follow up after treatment only valuable after 10+ days
chronic obstructive lung disease - only if symptoms change
PA Chest
patient erect facing bucky
centre midsaggital plane of patient to midline of IR
relax and roll forward shoulders
upper border of IR is 5cm above shoulder
raise chin and place back of hands against lower hips and roll shoulders forward (or hug bucky if unstable or elderly) (this clears scapulae off lung fields)
Area covered in PA chest
lung fields
apices
costophrenic angle
heart
PA chest collimation
Include 5ch above shoulder to include upper airway. Ensure lung bases included.
Include acromioclavicular joints (AC joints) laterally.
Anatomy visualised on chest radiograph
heart
lung parenchyma
pleura
chest wall
diaphragm
mediastinum
hilum
chest - 10 point checklist
correct examination undertaken
patient ID
hospital identification
correct anatomical marker positioned in primary beam
correct area included on image
adequate breath in
adequate exposure
artefacts
pathology
inspiration
cardiothoracic ratio
ratio of max horizontal cardiac diameter to max horizontal thoracic diameter. Normal <50%