10-12
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
50 Terms
Hyponatremia vs Hypernatremia
Hyponatremia = plasma Na+ <135 mmol/L (usually excess water); Hypernatremia = plasma Na+ >145 mmol/L (usually water deficit), changes plasma ADH levels
ADH (Vasopressin): Origin/Release
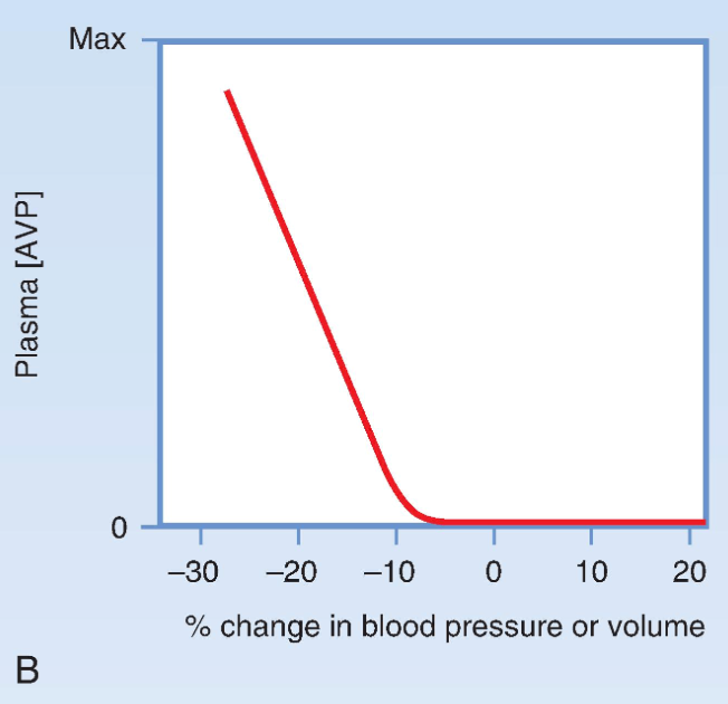
Produced in hypothalamic supraoptic/paraventricular nuclei (connected to OVLT and SFO axons) and released from posterior pituitary in response to ↑ plasma osmolarity or ↓ blood volume/BP
ADH functions
Increases H2O permeability in collecting ducts, increases urea permeability in inner medullar collecting ducts and constricts arterioles in peripheral smooth muscle (increasing blood pressure), produces concentrated, low-volume urine
ADH Receptors
V2 receptors increase water and urea reabsorption in collecting ducts; V1 receptors cause arteriolar vasoconstriction to raise BP
Osmoreceptors (definition)
OVLT and SFO detect plasma osmolarity via mechanosensitive cation channels exposed to blood through fenestrated capillaries
Osmoreceptor Response
Hyperosmolarity shrinks osmoreceptors → ↑ firing → ADH release; hypotonicity swells cells → ↓ firing → suppresses ADH
ADH vs Thirst Threshold
A 1–2% rise in osmolarity stimulates ADH release, 2–3% rise stimulates thirst
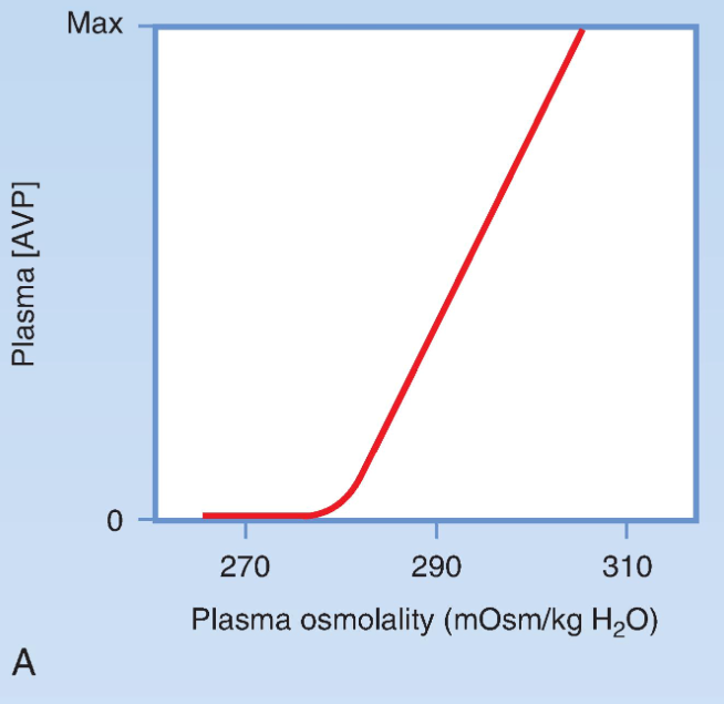
Normal Plasma Osmolarity
Normal plasma osmolarity is ~275–290 mOsm/kg; below threshold ADH secretion is essentially absent
Non-osmotic ADH Control
A 5–10% fall in blood volume/BP activates baroreceptors in the aorta and carotid sinus causing ADH release even during hypoosmolarity to preserve perfusion (blood pressure more important than osmolarity), resets osmostat
Other ADH Stimulators
Nausea pain motion sickness hypoxia strenuous exercise morphine nicotine MDMA and hypoglycemia increase ADH; alcohol suppresses it, thirst stimulated by decrease in blood volume
SFO Functions
SFO contains Ang II-sensitive neurons that stimulate thirst salt appetite and ADH release
Diabetes Insipidus (Central)
Central DI results from inadequate ADH production/release causing polyuria dilute urine and hypernatremia
Nephrogenic Diabetes Insipidus
Normal ADH but kidneys fail to respond causing polyuria dilute urine and hypernatremia
SIADH
SIADH causes excessive ADH leading to water retention hyponatremia low plasma osmolarity and concentrated urine
Sodium Balance: Main Determinant of ECF Volume
Total extracellular Na+ is the primary determinant of ECF volume because NaCl is the major extracellular osmotic solute
Kidney Regulation of Sodium Balance
The kidneys maintain ECF volume by matching Na+ excretion to dietary intake over a wide range
Primary Signals for Na+ Excretion
Vascular volume blood pressure and cardiac output regulate renal Na+ excretion through cardiovascular sensors
Response to Volume Changes
ECF contraction decreases Na+ excretion whereas ECF expansion increases Na+ excretion (natriuresis)
Congestive Heart Failure & Sodium
CHF causes edema with low effective arterial volume so kidneys retain Na+ and water despite increased total ECF volume
Major Baroreceptors
Atria pulmonary vessels carotid sinus aortic arch afferent arteriole and macula densa detect changes in vascular volume/pressure
Renal Sympathetic System
Sympathetic activation decreases GFR stimulates proximal Na+ reabsorption and renin release causing Na+ retention
RAAS Activation
Reduced renal perfusion sympathetic stimulation or decreased NaCl at macula densa stimulates renin release
RAAS Pathway
Renin converts angiotensinogen→Ang I; ACE converts Ang I→Ang II; Ang II stimulates aldosterone secretion
Major Actions of Angiotensin II
Causes vasoconstriction stimulates aldosterone ADH thirst salt appetite and increases proximal tubule Na+ reabsorption
Aldosterone Function
Aldosterone increases collecting duct Na+ reabsorption expanding ECF volume while promoting K+ secretion
ANP: Origin & Stimulus
Produced by atrial myocytes and released in response to atrial stretch during volume expansion
ANP Actions
ANP increases GFR inhibits renin aldosterone and ADH and increases Na+ and water excretion
Euvolemia
Euvolemia exists when renal Na+ excretion equals dietary intake with collecting duct Na+ reabsorption regulated mainly by aldosterone
Hypovolemia vs Hypervolemia
Hypovolemia activates sympathetic nerves RAAS and ADH to retain Na+/water; hypervolemia activates ANP and suppresses RAAS
Potassium Balance: Distribution
About 98% of body K+ is intracellular so small shifts between ICF and ECF greatly alter plasma K+
Normal Plasma Potassium
Normal plasma K+ ≈4 mEq/L; hypokalemia
Internal vs External K+ Balance
Internal balance shifts K+ between cells and ECF while external balance is regulated by renal excretion matching intake
Importance of Cellular Buffering
Rapid cellular uptake after meals prevents life-threatening hyperkalemia because renal excretion is relatively slow
Factors Moving K+ Into Cells
Insulin β2 agonists α antagonists alkalosis and aldosterone shift K+ into cells causing hypokalemia
Factors Moving K+ Out of Cells
Insulin deficiency β2 antagonists α agonists acidosis hyperosmolarity cell lysis and exercise shift K+ out causing hyperkalemia
Insulin & Potassium
Insulin stimulates Na+/K+-ATPase causing rapid K+ uptake into cells after meals; insulin deficiency predisposes to hyperkalemia
Adrenergic Effects on Potassium
β2 stimulation promotes K+ uptake whereas α stimulation promotes K+ release from cells
Acid-Base Effects on Potassium
Acidosis shifts K+ out of cells increasing plasma K+; alkalosis shifts K+ into cells decreasing plasma K+
Hyperosmolarity & Potassium
Hyperosmolarity pulls water from cells increasing intracellular K+ concentration and promoting K+ exit
Cell Lysis & Exercise
Cell lysis releases intracellular K+ while strenuous exercise transiently raises plasma K+
Aldosterone & Potassium
Aldosterone stimulates Na+/K+-ATPase promoting cellular K+ uptake; excess causes hypokalemia and deficiency causes hyperkalemia
Renal Handling of Potassium
K+ is freely filtered; ~65% reabsorbed in proximal tubule ~20% in thick ascending limb with variable secretion/reabsorption distally
Collecting Duct Potassium Secretion
Principal cells secrete K+ via apical K+ channels after uptake by basolateral Na+/K+-ATPase
Driving Force for K+ Secretion
High intracellular K+ plus a negative tubular lumen favor K+ secretion into tubular fluid
Aldosterone & Renal K+ Secretion
Aldosterone increases ENaC Na+/K+-ATPase and K+ channel expression enhancing K+ secretion largely by increasing Na+ reabsorption
Acid-Base Effects on Renal K+ Handling
Alkalosis increases renal K+ secretion whereas acidosis decreases secretion by altering Na+/K+-ATPase and K+ channel activity
High Potassium Diet
High K+ intake increases intracellular K+ in principal cells increasing the driving force for urinary K+ secretion
Low Potassium Diet
Low K+ intake decreases principal cell secretion and stimulates α-intercalated H+/K+-ATPase to reabsorb K+
α-Intercalated Cells
Reabsorb K+ through apical H+/K+-ATPase during K+ depletion helping conserve body potassium
Major Regulators of Renal K+ Secretion
High dietary K+ aldosterone and alkalosis increase secretion whereas low dietary K+ and acidosis decrease secretion