Diagnosis: Li-Repac 1980 and Rosenhan 1973 + Parker 2001 , Bolton 2002, Stockman 2003
1/24
Earn XP
Description and Tags
Terms: data triangulation, conceptual vs. practical definitions of abnormality, emic vs etic, DSM vs ICD (or CCMD) reliability, sick role bias, clinical interview, clinical bias
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
25 Terms
Li-Repac 1980
Aim + Procedure
Aim: to test the role of stereotyping in diagnosis
Context: Li-Repac wanted to compare the diagnoses of both white and Chinese-American therapists of both white and Chinese male subjects.
She hypothesized that the therapists would generally agree on the concept of normality as they all had similar training. She hypothesized that differences would exist in the actual diagnoses when diagnosing someone of a different cultural group.
Procedure:
10 patients: 5 white and 5 Chinese all diagnosed with mental illness
Clinicians: The clinicians were 5 white (no prior contact with Asian Patients) and 5 Chinese-American males
Controlled for age, socio-economic status, and level of pathology
Diagnosis of patients
Chinese: 3 schizophrenia,1 neurotic and 1 reactive depressive
White: 2 schizophrenics, one as neurotic, one as character disorder and one as reactive depressive
VIDEOTAPED Semi-structured interview: asked questions such as "How have you been feeling lately?" and "How do you spend a typical day?"
Each Clinician was asked to describe and ideal and FUNCTIONING individual, no significant differences in scores
Clinicians were randomly assigned videos to rate for normality.
Each rater would rate 4 videos - 2 of white patients and 2 of Chinese patients
Clinicians then filled an inventory, describing personal traits and signs of pathology
Li-Repac 1980
Results + Conclusion
Results:
Chinese: tended to see the Whites as being more aggressive. When asked to rate the patients on pathology, there were three significant findings:
Ratings of Pathology
● White raters:
saw the Chinese patients as more depressed and inhibited
Saw Chinese patients as less socially competent and as having less capacity for interpersonal relationships
tended to see signs of lower self-esteem in the Chinese patients.
● Chinese-American raters: reported more severe pathology when judging white patients
Conclusion: although the study does support the idea that there are cultural biases in diagnosis, more research needs to be done to support the findings.
Li-Repac 1980
Evaluation
Evaluation:
Highly controlled experiment
Lacks ecological validity
Lacks validity: can only be used for 2 cultures, small sample size, difficult to generalize findings
No pre-test for stereotypes
White clinicians had no previous experience with Chinese patients, may affect results and diagnosis
Only MALE clinicians
Rosenham 1973
Aim + Procedure
Aim: to investigate how doctors in hospitals are able to diagnose people as "sane" or "insane" and SICK ROLE BIAS in diagnosis
Procedure Study 1:
8 pseudo-patients (one being Rosenhan) both men and women of various ages an professions - that is, confederates - who would act the part of someone seeking help in a hospital.
The participants: were the hospital staff (of 12 hospitals in the USA ) NOT the patients. They were part of the study.
The hospitals did not give consent or know about the first step of the study.
The pseudo-patients told the doctor at the hospital that they were hearing voices.
AT THE TIME based on the DSM II, this would have been considered a clear sign of schizophrenia.
Besides this symptom, they described their lives as they really were except for their actual occupation
Behaved normally and took notes their experience
Had to convince hospital staff they were “sane”
Procedure Study 2:
Hospitals were told that one or more pseudo-patients would try to be admitted to their hospital over a three month period.
Each member of staff was asked to rate all patients who came in on a 1 - 10 scale for "likelihood of being a pseudo-patient."
Rosenhan 1973
Results + Conclusions
Results Study 1:
All of the pseudo-patients were admitted
11 were released with a diagnosis of "schizophrenia in remission," and one with a diagnosis of "manic depressive psychosis."
The length of stay ranged from 7 to 52 days, with an average of 19 days.
The nurse's notes showed that they observed no signs of abnormality during their stay.
Conclusion:
Once the initial diagnosis was made, then the label of schizophrenia remained, even though the pseudo-patients showed no signs of abnormality.
Rosenhan's study challenged the validity of diagnosis and how a diagnosis may influence the perception of staff working with a patient
Results Study 2:
Of 193 patients who were evaluated on the 10 point scale, none were actually pseudo-patients.
Staff judged 41 to be pseudo-patients by at least one staff member
23 were suspected by one psychiatrist
19 were suspected by a psychiatrist and a staff member.
Conclusion:
This shows that validity can be affected when a doctor's credibility is at risk.
They were less likely to make a diagnosis, fearing that they would make a mistake.
Rosenhan 1973
Evaluation
Evaluation:
Rosenhan concluded that psychiatric diagnoses lacked validity and that hospitals fostered environments where patient behaviors were easily misinterpreted due to diagnostic labels.
However, the study faced significant limitations.
The small sample size of eight pseudo-patients across 12 hospitals, many with psychiatric training, restricted generalizability.
Ethical concerns were also raised, as hospitals and staff were deceived, diverting resources from real patients, and pseudo-patients experienced potentially stressful conditions.
Additionally, researcher bias may have influenced observations, particularly interpretations of staff notes.
Despite its flaws, the study shed light on the limitations of psychiatric diagnoses at the time and sparked reflection on mental healthcare practices.
Definition: Data Triangulation
you use multiple data sources to answer your research question.
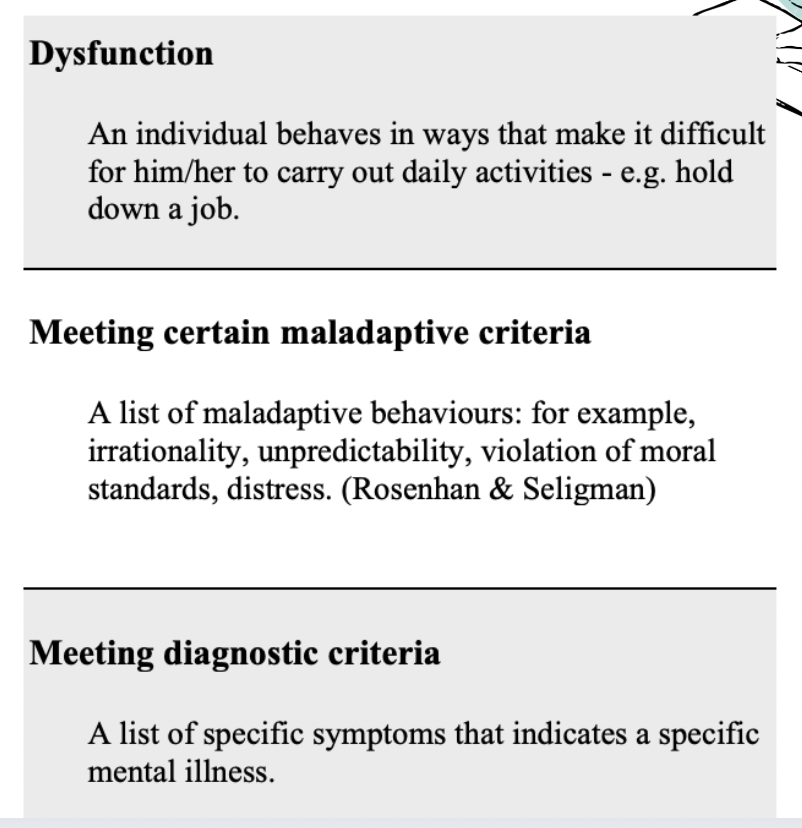
Definition:Conceptual definition of abnormality
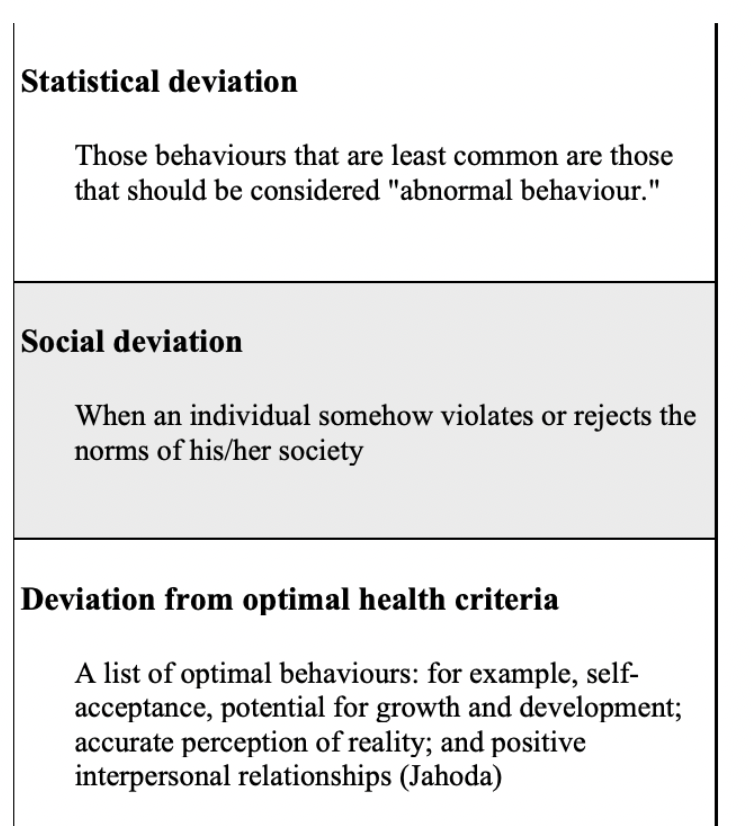
Definition: Practical definitions of abnormality
Definition: Emic vs. Etic approach
Etic Approach: research that studies cross-cultural differences
Emic: research studies only one culture
Definition: DSM vs. ICD
DSM:a reference book on mental health and brain-related conditions and disorders. The American Psychiatric Association (APA) is responsible for the writing
ICD: a classification system for all physical and mental diseases produced by the World Health Organization (WHO)
Definition: Sick role Bias
The individual is automatically labeled as a "patient."
This means that the psychiatrist is "looking for evidence of abnormal behavior."
If a person is seeking assistance, they must have a mental disorder.
Definition: Clinical Interviews
a dialogue between psychologist and patient that is designed to help the psychologist diagnose and plan treatment for the patient.
Parker 2001
Aim + Procedure
Aim: to investigate if the symptoms for depression are the same in Chinese and Australian culture
Procedure:
The sample was made up of 50 Malaysian participants of Chinese heritage and 50 Australian participants of Caucasian, Western heritage.
Australians all had English as their first language, the Chinese were a mix of Chinese (80%) and English (20%) as their first language
All participants were out-patients who had been diagnosed with Major Depressive Disorder, but who did not have other diagnoses as well, such as drug addiction or schizophrenia.
Two Set questionnaire:
1: set of mood and cognitive items common in Western diagnostic tools for depression.
2: a set of somatic symptoms commonly observed by Singaporean psychiatrists.
The questionnaire was translated to establish credibility
Patients were asked to judge the extent to which they had experienced each of the 39 symptoms in the last week.
Four options: all the time, most of the time, some of the time and not at all.
Asked to rank the symptoms that they experienced in order of how distressing they were.
Parker 2001
Results + Conclusion
Results:
When looking at which symptom led them to actually seek help, 60% of the Chinese participants identified a somatic symptom, compared to only 13% of the Australian sample.
There was no significant difference in the number of somatic symptoms indicated by each group as being linked to their depression.
Chinese: participants were significantly less likely to identify cognitive or emotional symptoms as part of their problem. They were less likely to rate feeling helpless and hopeless, a depressed mood, having poor concentration, or having thoughts of death
Conclusion:
The role of culture is evident: in Western culture it is more appropriate to discuss one's emotions and depression is seen as linked to a lack of emotional well being;
Chinese culture: it is less appropriate and even stigmatized if one speaks about a lack of emotional health.
Parker 2001
Evaluation
Evaluation:
The study developed a questionnaire based on cultural evidence relevant to participants, rather than a standardized western questionaire.
They chose participants based on the DSM-IV criteria for Major Depressive Disorder.
The study demonstrates an imposed etic approach to research.
Eliminated people from thes sample who did not fullfill the western view of depression.
Questionnaire was backtranslated to establish credibility.
Bolton 2002
Aim + Procedure
Aim: to investigate the local validity of western mental illness concepts in Ruanda - that is, was a Western diagnosis of depression or PTSD accepted by the local community as a valid description of their response to trauma?
Procedure:
Interviewers generated free lists by asking 40 local people to name all the problems that had resulted from the genocide and to briefly describe each one.
Guhahamuka: Insomnia, suicidal thoughts, inability to pray, acting without thinking, feelings of epileptic episodes
Agahinda gakabije: Isolation, issues with alcohol, lack of self care, difficulty with social interactions (marginalisation)
Inductive content analysis: they pulled out symptoms that were related to mental health.
Key informant interviews:
Participants were asked for the names of people in the community who were knowledgeable of these problemsfurther interviews were then carried out. Local healers where seen as knowledgable.
Pile Sorts:
A set of cards was created which included the mental health symptoms that were identified in the initial interview as well as the symptoms that identify depression as outlined in the DSM.
The healers were asked to sort the cards based on similarity between the symptons and a kmental health disorder and included three symptoms with the DSM diagnosis of depression: lack of trust in others, loss of intelligence, and mental instability.
Used these local symptoms in questionnaire to determine prevalence levels of depression in the community.
Bolton 2002
Results + Conclusion
Results:
After the questionnaire: 93 people were identified as having mental health issues in the community.
When interviewed: 70 were diagnosed by local healers as showing the symptoms of local symptoms
30 of those then tested positive for signs of depression after completing the questionnare.
Conclusion:The relationship between agahinda and depression was the same as that between grief and depression in the Western world.
However, the DSM and its symptoms for depression cannot be applied within the local community
Bolton 2002
Evaluation
Evaluation:
Emic approach: makes use of local resources to help with the diagnosis of mental health issues,
considers how the various components of culture have shaped an individual's health and help to determine an appropriate treatment.
Data triangulation to strengthen the credibility of the findings.
Back translation used to establish credibility.
Reliant on determining which Western disorder most resembles the locally defined problems.
Emic approaches are also limited to the community that is studied limiting generalizeability
Use of cross-cultural psychiatry: fails to recognize that cultures are dynamic,
complex social constructs that defy easy measurements.
Definition: Classification Systems
Classification systems identify patterns of behavioral or mental symptoms that consistently occur together to form a disorder
Definition: Anchoring Bias
Peoples tendency to rely to heavily on the first piece of information they have on a topic.
Stockman 2003
Aim + Procedure
Aim: to determine the role of anchoring bias in diagnosis.
Procedure:
The researchers carried out an experiment using a sample of 46 US clinicians.
The clinicians were a combination of psychiatrists, psychologists, and social workers from private practice, university, and community clinics.
The researchers used a repeated measures design.
The research question was whether giving significant evidence of mental illness in an early interview would have more influence on a final diagnosis and prognosis than giving that same evidence in a later interview.
Clinicians were given two different case studies.
Joanne was a severe case of depression with a rather dramatic suicide attempt;
Gina was less severe with some symptoms of anorexic behaviours.
Each participant read five consecutive interviews per case.
Participants were asked to evaluate the level of functioning and the prognosis after each
interview. The score after the final interview is what was compared. The study was counter-balanced.
Some read Joanne first, some read Gina first.
When reading the case studies, the "time" at which the important information was revealed was different for each condition.
In the "early" condition, information about Joanne's suicide attempt or Gina's disordered eating was discussed in the first interview that was read.
In the "late" condition, this information was revealed in the fourth (the next to last) interview.
Stockman 200
Results
Results:
In the less severe condition, the participants that read the evidence of mental illness in the first interview indicated a lower level of functionality and a poorer prognosis than the clinicians that received the information later.
It appears that the early exposure to the symptoms and the subsequent rating of the client influenced the final diagnosis.
However, in the group that had more mild symptoms in the first interview, the rating that they gave also served as an anchor which resulted in a less severe diagnosis and a better prognosis.
In the more severe case, although the initial diagnosis ratings were also different, they did not show a significant anchoring effect. In other words, regardless of when they read about the suicide attempt, there was no effect on their final diagnosis and prognosis.
Conclusion: Results among an experienced sample of clinicians indicated significant anchoring in one case but not the other, which suggests a clinical bias to disregard pathognomonic data about a client who is seen initially as less disturbed.
Stockman 2003
Evaluation
Normality vs. abnormality
normality refers to behaviors, thoughts, and emotions that align with typical societal norms and expectations, while abnormality describes significant deviations from those norms, often leading to distress or impairment in functioning.