clinical/abnormal psych
1/81
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
82 Terms
Abnormal Psychology
Abnormal behavior is defined as patterns of emotions, thoughts, and actions considered pathological (diseased or disordered) for one or more oft he following reasons:
● Infrequent occurrence
● Personal distress
● Dysfunction
● Unexpectedness
● Violation of cultural norms
Infrequent Occurrence
Use the normal curve to determine the frequency of the suspected abnormal behavior with the frequency of that behavior in the population
Problem of infrequent occurrence
either extreme of behavior is considered to be abnormal (both drinking excessively and drinking not at all, both low intelligence and high intelligence, etc)
Personal Distress
Use individual's judgment of current level of functioning. If the individual feels his/her behavior is abnormal, such as excessive levels of anxiety or depression, then it is
Problem of personal distress
many people deny they have a problem, particularly with substance abuse, and others just may not care (antisocial personalities)
Dysfunction
Individual's behavior is abnormal if his/her behavior is interfering with the ability to function in one's own life and in society.
Problem with dysfunction
not all people with psychological disorders have behaviors that interfere with their social functioning. (Examples are eating disorders, OCD, trichotillomania, etc.)
Unexpectedness
Behavior is unusual, given the circumstances. Many types of psychological disorders include symptoms that are considered unusual by others (hearing voices, inappropriate emotions, etc.)
Problem with unexpectedness
just because a behavior is unexpected doesn't necessarily make it abnormal.(excessive shyness, some minor phobias, sneezing)
Violation of Cultural Norms
Behavior is considered abnormal if it goes against society's rules, norms, or standards.
Problem with violation of cultural norms
cultural norms change. This is over time and across cultures. Also, culture-bound syndromes: disorders that exist only in one (or similar) culture(s). For example, koro and anorexia.
Textbook def of a psychological disorder
A syndrome (collection of symptoms)marked by a "clinically significant disturbance in an individual's cognition, emotion regulation, or behavior"
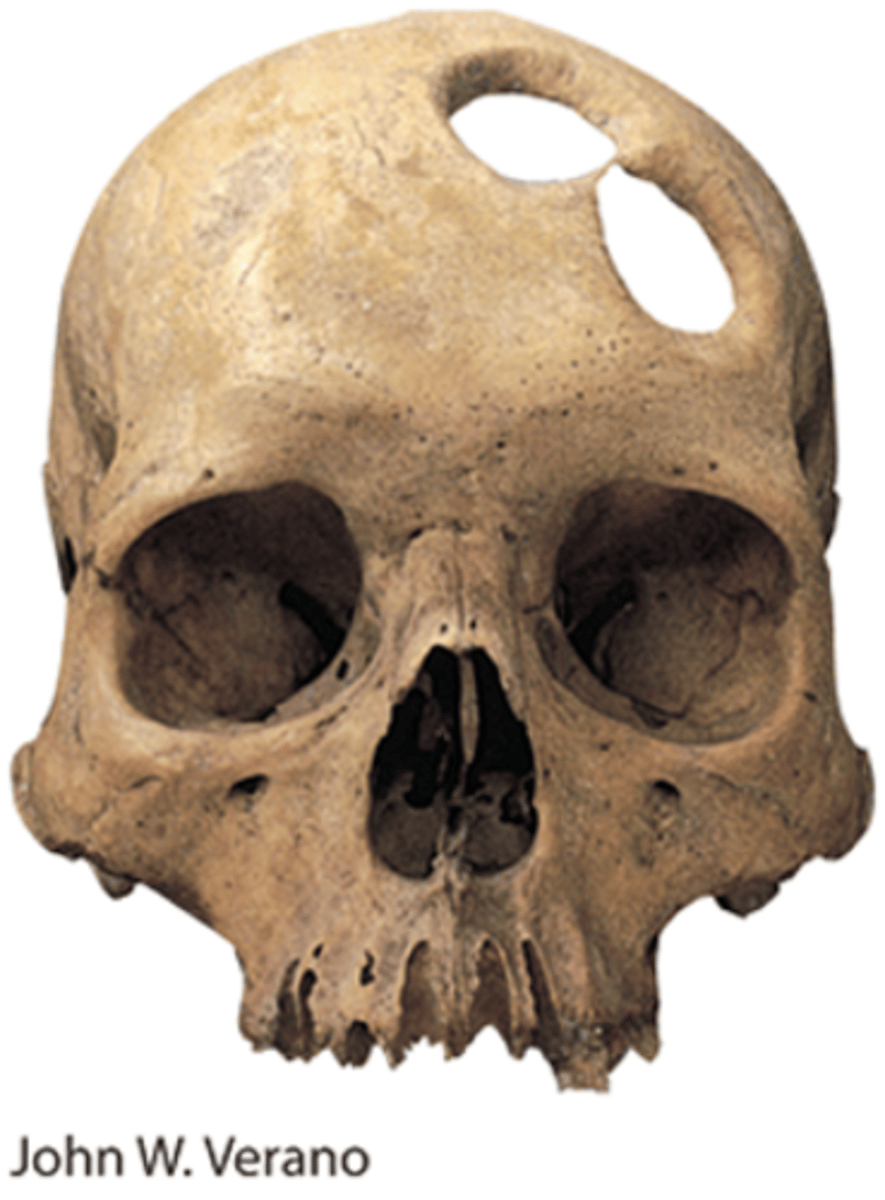
Demonic possession
has been the classic explanation of mental disorders
● Trephining: Stone Age skulls have holes chipped into them, purportedly to release evil spirits
Medical model
suggests a physiological cause for abnormal behavior
● Diathesis-stress model: there is an underlying biological predisposition for a disorder, and stressful life events activate it.
Classifying Disorders
An original classification system dating from the late 1800s included two main divisions of mental disorders:
Neurosis
Psychosis
Neurosis
a condition involving excessive anxiety
Psychosis
a condition involving a loss of contact with reality
Diagnostic and Statistical Manual of Mental Disorders (DSM-5)
Since 1952, the main classification system of mental disorders.
It was developed by (and is revised by)the American Psychological Association(APA), and is used to diagnose and describe abnormal behaviors.
Currently, we are on the DSM-5-TR,which was published in 2022
According to the DSM-5-TR, what must a mental disorder be?
1. Be a clinically-significant detriment. The behaviors must involve distress or impair functioning in such a manner that professional intervention is warranted.
2. Derive from an internal source (biology, thoughts, learning)and not just the immediate environment.
3. Have an involuntary manifestation - the behavior is not a deliberate, voluntary, decision to act in this manner.
What's the difficulty with diagnosis?
The DSM-5-TR only provides a description of psychological disorders.
● As such, a person can be diagnosed as having different disorders, even with the same symptoms, depending on who is doing the diagnosing.
● In addition, the label of "abnormal behavior," once applied, tends to stay with the person that has been labeled in this manner.
Medical Student's disease
Hopefully, you have a degree of skepticism about the appropriate labeling of psychological disorders "Medical student's disease." This refers to the tendency to diagnose yourself with the disorders about which you learn.
Behavior is on a continuum
It is the degree of disruption in life that is important in diagnosis.... not the presence or absence of a characteristic
anxiety disorders
Type of abnormal behavior characterized by unrealistic, irrational fear.
● Generalized anxiety disorder
● Panic disorder
● Phobias
All of these disorders show a genetic influence; they tend to run in families
Phobia
Types of anxiety disorders characterized by intense, irrational fear and avoidance of objects or situations.
● Agoraphobia
● Specific phobia
● Social anxiety disorder
The individual realizes the fear is irrational, but cannot stop it.
Agoraphobia
Literally, the fear of open spaces or unfamiliar spaces. Often follows the onset of panic disorder, because the person fears having a panic attack in public. However, in the DSM-5 agoraphobia is its own diagnosis and need not accompany a diagnosis of panic disorder.
Specific phobia DSM Checklist
1. A persistent fear lasting at least six months
2. Immediate anxiety by exposure to the object
3. Recognition that the fear is excessive or unreasonable
4. Avoidance of the phobia
5. Significant distress or impairment
Social phobia DSM checklist
1. persistent fear of social or performance situations lasting at least six months
2. Anxiety produced by exposure to the social situation
3. Recognition that the fear is excessive or unreasonable
4. Avoidance of social situations
5. Significant distress or impairment
Panic Disorder
Type of anxiety disorder characterized by sudden and inexplicable attacks of intense fear.
Symptoms include difficulty breathing, heart palpitations, dizziness, trembling, terror, and feelings of impending doom.
Studies have linked a tendency towards catastrophizing with panic disorder.
Panic Disorder DSM checklist
1. Recurrent unexpected panic attack
2. A month or more of one of the following after one of the attacks:
(a). Persistent concern about having additional attacks
(b). Worry about he implications or consequences of the attack
(c). Significant change in behavior related to the attacks
Generalized Anxiety Disorder
Type of anxiety disorder characterized by chronic, uncontrollable, and excessive worry.
The anxiety is not focused on any particular object or situation. It is "free-floating" anxiety
Generalized Anxiety Disorder DSM checklist
1. Excessive or ongoing anxiety and worry, for at least six months
2. Difficulty controlling the worry
3. At least there of the following symptoms:
restlessness\easy fatigue
irritability
muscle tension
sleep disturbance
4. significant distress or impairment
Obsessive-Compulsive Disorder
In the DSM-5, obsessive-compulsive disorder (OCD) was moved from the anxiety disorders to its own classification. A disorder characterized by intrusive thoughts (obsessions) and urges to perform repetitive, ritualistic behaviors (compulsions.)
OCD has been linked to over-activity in the caudate nucleus of the basal ganglia.
Often treated with drugs that increase serotonin levels, which seems to reduce activity in the caudate nucleus.
Obsessive-Compulsive Disorder DSM checklist
1. Recurrent obsessions/compulsions
2. Past/Present recognition that the obsessions/compulsions are excessive or unreasonable
3. Significant distress/impairment or disruption by symptoms for more than one hour a day
Post-Traumatic stress Disorder
In the DSM-5, PTSD was moved from the anxiety disorders to a new category of stress and related disorders.
This disorder is characterized by the uncontrollable "re-living" of a traumatic event or events, as well as sleeplessness, guilt, and irritability.
Since up to 90% of individuals experience PTSD after severely traumatic events, many individuals feel that this should not be considered "abnormal" behavior.
Post-Traumatic stress Disorder DSM Checklist
1. A history of having experienced/witnesses/confronted event(s) involving death/serious injury/threat to yourself or other. Reaction of intense fear/helplessness/horror produced by event
2. Event persistently reexperienced in at least one of the following ways:
(a) Recurrent distressing recollections
(b)Distress caused by reminders of event
(c) physical arousal produced by reminders of event
3.At least two marked symptoms of increased arousal:
(a) difficult sleeping
(b) irritability
(c) Poor concentration
(d) Hypervigilance
(e) exaggerated startle response
5. Symptoms lasting at least one month
Theoretical Causes of Anxiety, OCD, & PTSD Disorders-Behavioral and Social Learning theory
both cognition and learning have been implicated in the anxiety-related disorders. Many individuals with anxiety-related disorders appear to be hypervigilant: constantly on alert for signs of danger in their environment. Additionally, fears can be learned through classical and operant conditioning
Theoretical Causes of Anxiety, OCD, & PTSD Disorders-Biological
genetically inherited overactive autonomic nervous system; amygdala & prefrontal cortex
Theoretical Causes of Anxiety, OCD, & PTSD Disorders-Sociocultural
Western society has become very fast-paced and stressful. Since the reaction to stress, regardless of its source, is activation of the autonomic nervous system, particularly the sympathetic nervous system, it is not unusual to note the sharp rise in diagnosed anxiety-related disorders over the past 50 years in the USA.
Dissociative Disorders
Stress-related disorders characterized by a splitting apart of conscious experience to escape the memory of a painful experience.
● Dissociative amnesia
● Dissociative fugue (changed to a specifier of dissociative amnesia in DSM-5)
● Depersonalization-derealization disorder
● Dissociative identity disorder (DID)
dissociative amnesia
Dissociative disorder characterized by an inability to recall personal past due to psychological distress. The amnesia can relate to a specific experience, or to a more global loss of personal identity.
dissociative fugue
Dissociative specifier for dissociative amnesia characterized by leaving past life and assuming a new identity. If the original identity is ever recovered, all memory of the intervening time interval is lost.
Depersonalization-derealization disorder
This is a disorder new to the DSM-5 in which the individual experiences a persistent detachment from thoughts, feelings, or body sensations.
Dissociative Identity Disorder
Dissociative disorder characterized by the presence of two or more distinct personalities within the same person.
All of the dissociative disorders are controversial; DID is particularly so.
Before 1970, only 100 cases of DID world-wide appear in the scientific literature; by 1999, there were 30,000 reported cases in North America alone.
Theories of dissociative identity disorder
The Childhood-Trauma Theory of DID: severe abuse in childhood (usually before age 10)
The Culturally-Conditioned Iatrogenic Theory of DID: DID became more common after a book and movie were created about it; most DID is "discovered" in therapy, usually involving hypnosis (iatrogenic means "doctor-induced")
Dissociative amnesia DSM checklist
1. One or more episodes of inability to recall important personal information
2. Significant distress or impairment
Dissociative fugue DSM checklist
1. Sudden unexpected travel away from home/work, with inability to recall one's past
2. Confusion about personal identity
3. significant distress or impairment
Dissociative identity disorder DSM checklist
1. The presence of two or more distinct identities/states
2. Control of the person's behavior recurrently taken by at least two identities/states
3. An inability to recall important personal info that is too extensive to be explained by ordinary forgetfulness
Depressive Disorders
Type of abnormal behavior characterized by persistent depressive states.
● Major depressive disorder (unipolar disorder)
● Seasonal affective disorder (SAD)
There is a strong genetic component in the depressive disorders.
Major depressive disorders
Type of mood disorder characterized by a long-lasting depressed mood that interferes with the ability to function, feel pleasure, or maintain interest in life.
The feelings are without apparent cause and are excessive for the given situation, and must be present for more than two weeks.
Often treated with antidepressant drugs which boost available serotonin and norepinephrine levels.
Major Depressive episode DSM checklist
1. The Presence of at least five of the following symptoms during the same two-week period:
Depressed mood most of the day nearly every day, Markedly diminished interest or pleasure in almost all activities most of the day, significant weight loss or weight gain or decrease/increase in appetite, insomnia or hypersomnia, psychomotor agitation, fatigue or loss if energy, reduced ability to think or concentrate/indecisiveness, recurrent thoughts of death or suicide/suicide attempt/ or plan for suicide
2. Significant distress or impairment
Major Depressive Disorder DSM checklist
1. The presence of a major depressive episode
2. No history of a manic or hypomanic episode
Dysthymic Disorder DSM checklist
1. Depressed mood for most of the day, for more days than not, for at least two years
2. Presence, while depressed, of at least two of the following: Poor appetitive/overeating, insomnia/hypersomnia, low energy/fatigue, low self-esteem, poor concentration or difficulty making decisions, feelings of helplessness
3. During two-year period, symptoms not absent for more than two months at a time
4. No history of a manic or hypomanic episode
5. Significant distress or impairment
Genetic component/Gender differences of depressive disorders
People with a history of major depression have a higher genetic liability.
Females are more likely to be affected by a depressive disorder.
Circularity of Depression
Depressed thinking(negative thoughts) <-> Depressed action (withdrawal from enjoyable activities) <-> Depressed mood(Miserable feeling) <->*back to beginning
Anxious thoughts vs. Depressed thoughts
"What if I get sick and become an invalid?" vs. "I'm worthless"
Seasonal affective disorder
Type of mood disorder characterized by experiencing depression in relation to the amount of available sunlight. (winter depression)Treated by sitting in front of a bank of full-spectrum lights for a couple of hours a day. May be another subtype (summer depression) that is heat related.
Biological cause of depressive disorders
changes in the functioning of the brain and the levels of available neurotransmitters have been associated with mood disorders. The right frontal lobe is more active (which is linked to negative emotions) and the left frontal lobe is less active during depressive episodes. The neurotransmitters serotonin and norepinephrine are imbalanced in depressions.
Psychological cause of depressive disorders
the various psychological perspectives see the root of depression as stemming from various areas.
● Psychoanalytic: anger turned on self
● Humanistic: blocked personal growth
● Behaviorism/cognitive psych: learned helplessness - repeated exposure to negative stimuli that cannot be avoided and over which one has no sense of control results in animals (including humans) which "give up" and become listless, apathetic, and withdrawn. Additionally, humans can think about their inability to affect their environment(attributions) and thus intensify this effect.
Bipolar disorders
Type of mood disorder characterized by episodes of mania (excessive and unreasonable elation and hyperactivity), usually followed by even longer episodes of depression. Bipolar disorder was moved into its own category in the DSM-5.
There seems to be a strong genetic component of bipolar disorders. They are often treated with lithium, a common salt.
Bipolar 1
experience mania and major depressive episodes
Bipolar 2
experience hypomania (mood elevation which is not as extreme as mania)and major depressive episodes.
Manic episode DSM checklist
1. Last at least one week
2. Persistence of at least 3: Inflated self-esteem or grandiosity, decreased need for sleep, more talkativeness than usual or pressure to keep talking, flight of ideas or the experience that thoughts are racing, distractibility, increase in activity or psychomotor agitation, excessive involvement in pleasurable activities that have ahigh potential for painfuls consequences.
3. Significant distress or impairment
Bipolar 1 DSM checklist
1. The presence of a manic, hypomanic, or major depressive episode
2. If currently in a hypomanic or major depressive episode, history of a manic episode
3. Significant distress or impairment
Bipolar 2 DSM checklist
1. The presence of a hypomanic or major depressive episode
2. If currently in major depressive episode, history of a hypomanic episode. If currently in a hypomanic episode, history of a major depressive episode. No history of a manic episode.
3. Significant distress or impairment
What happens in the brain with bipolar disorders
PET scans show that brain energy consumption rises and falls with the patient's emotional switches. Red areas are where the brain rapidly consumes glucose. See slide 65 on powerpoint
Schizophrenia Disorder
A group of psychotic disorders involving major disturbances in perception, language, thought, emotion, and behavior. One percent of the population world-wide experiences a schizophrenic episode at least once in their lives. Schizophrenia is usually a young-adult onset disorder
Perceptual disturbances
Hallucinations: sensory perceptions that occur without an external stimulus. Most common are auditory (hearing voices) although visual and haptic hallucinations can occur as well.
Auditory->VIsual->Tactile->Smell/taste
Language disturbances
Words lose their usual meanings and associations.
Word salad: words strung together in a jumbled manner
● "The same children are sent of a rose, sweet smelling perfume thatgives us peace and parts and whole."
● "The sad kind and peaceful valleys are of the mind come beckoningunder rivers."
Neologisms: creation of new words by combining existing words.
● "splisters": combination of splinters and blisters
● "smever": combination of smart and clever
Thought disturbances
Delusions: mistaken beliefs maintained in spite of strong evidence to the contrary. Most common are delusions of persecution, delusions of grandeur, and delusions of being controlled.
Emotional Disturbances
Flattened affect: almost no response of any kind
Inappropriate emotions
Behavioral Disturbances
Odd behaviors
● Catatonic: nearly immobile positions
● Waxy flexibility: tendency to maintain whatever posture is imposed
Schizophrenia DSM Checklist
1. At least two of the following present for a
significant portion during a one-month period:
a. Delusions
b.Hallucinations
c. Disorganized speech
d. grossly disorganized or catatonic behavior
e. negative symptoms
2. Functioning markedly below the level achieved prior to onset
3. Continuous signs of the disturbance for at least six months
Positive symptoms of Schizophrenia
distorted or excessive activity (delusions, hallucinations, inappropriate emotions, word salad, excessiveor bizarre movements)
81%Delusions-> 58%Hallucinations-> 22%Disorganized thoughts
Negative symptoms of Schizophrenia
behavioral deficits or loss of activity (flattened affect, social withdrawal, poverty of speech, catatonic posture)
85%Avolition/apathy -> 65%Flat affect -> 30% Alogia/poverty of speech
Biological causes of schizophrenia
● Genetics
● Prenatal and perinatal conditions
● Dopamine hypothesis
● Brain structural changes
Psychosocial Causes of schizophrenia
● Stress
● Family communication
Genetics for Schizophrenia
there appears to be a genetic predisposition for schizophrenia. What is believed to be inherited is a propensity to develop schizophrenia under certain environmental conditions(stress)
Prenatal & Perinatal conditions for Schizophrenia
● Viral (flu) infections during the 5th month of pregnancy
● difficulties during the birthing process
Dopamine Hypothesis
symptoms of schizophrenia are caused by overactivity of dopamine neurons. (Positive symptoms)
(Brain Structure) Enlarged ventricles:
some people diagnosed with schizophrenia have excessively large ventricles (fluid-filled cavities in the brain.) (Negative symptoms)
Family communication
or those already biologically predisposed towards schizophrenia, disorganized, hard-to-follow, critical or negative, and/or highly emotional communication styles may increase the risk of developing schizophrenia
yesterday's "therapy"
-Through the ages, psychologically disordered
people have received brutal treatments, including the trephination evident in this Stone Age skull.
-Drilling skull holes like these may have been an
attempt to release evil spirits and cure those with
mental disorders
posttraumatic growth
positive psychological changes as a result of struggling with extremely challenging circumstances and life crises