Herpes Virus
1/29
Earn XP
Description and Tags
NSUOCO
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
30 Terms
What is a commonality for all herpes viruses?
They are enveloped
double stranded DNA
and similar in structure
noted as HHV-# (humans herpes virus)
Characteristics of HSV (Herpes Simplex Virus)
HHV-1 and HHV-2
90% of the US population has antibodies for HHV-1 or HHV-2
causes fever blisters and genital herpes
both infect the epithelial cells (especially oral mucosa and corneal epithelium)
What was believed historically about herpes?
that type I caused fever blisters and type II caused genital infections but now we know that both infect either region
What is there the note about the differences in herpes viruses?
both are very similar with minor antigenic differences on the envelope however TYPE II (HHV-2) is more virulent typically
What is the pathophysiology of herpes HHV-1 and HHV-2?
Entry Point: Herpes infects epithelial cells at the inoculation site and spreads to neurons via the trigeminal (CN V) or sacral nerve ganglia.
Immune Response: Cytotoxic T cells (Tc) clear epithelial infections through MHC I/antigen presentation.
Immune Evasion: Neurons have low MHC I, making them safe havens for the virus.
Dormancy Mode: Low neuron metabolism suppresses viral replication, causing dormancy in trigeminal or sacral ganglia.
Reactivation Triggers for HHV-1: Stress, hormones, UV light, or other stimuli can awaken the virus.
Reinfection Route: Reactivated virus travels along the trigeminal nerve to reinfect epithelial cells.
Ocular Impact: Herpetic keratitis is the most common ocular manifestation, as the trigeminal nerve innervates the entire eye.
Eye Inflammation: HSV can cause anterior uveitis, trabeculitis (IOP spikes), retinitis, and optic neuritis.
Why can HSV infect and inflame any structure of the eye?
because the trigeminal nerve innervates the entire eye.
What is possible with herpes simplex and herpes zoster?
ARTO
Anterior uveitis
Retinitis
Trabeculitis (IOP spikes)
Optic neuritis
What is the treatment of HHV-1 and HHV-2?
oral antivirals like acyclovir, famiciclovir, and valacyclovir
viroptic- topically on cornea
zirgan (topical ganciclovir) ~ similar to acyclovir
What are oral antivirals like acyclovir and famiciclovir?
chain terminators that are similar to AZT but are non-toxic to host cells and only interact with viral enzymes
Viroptic is also a chain terminator, what is it used for and how?
It is used topically on the cornea and it is toxic to human epithelial cells unlike acyclovir/famiciclovir/ and valacyclovir
Characteristics of HHV-3 (Herpes Varicella-Zoster Virus)
95% of US pop exposed by adulthood
causes chicken pox and shingles (by inhalation or contact with lesions)
slower replication cycle than HSV and also has different glycoproteins on envelope and different enzymes
virus stays dormant in dorsal root ganglion and trigeminal ganglion
only the young/immunocompromised adults get the rash
What is the pathophysiology of HHV-3?
Contagious Window: Infected individuals are contagious 2 days before the rash and 4 days after.
Immune Defense: IgG and Tc cells clear the initial infection from epithelial cells, fibroblasts, and blood.
Dormancy: Virus retreats to the dorsal root ganglion (spine) or trigeminal ganglion (head), where it can remain latent for life or reactivate as shingles if immunity drops.
Primary Infection: Mild and self-limiting, but can lead to secondary bacterial infections, viral pneumonia, or encephalitis in immunocompromised patients.
Rash Patterns:
Initial infection: Rash spreads widely due to dissemination from lungs and skin.
Reactivation: Rash follows a dermatome (skin area supplied by one spinal nerve).
Pain vs. Itch:
Initial rash is itchy.
Shingles rash is painful due to involvement of peripheral nerves.
Complications: Ocular complications (e.g., anterior uveitis, retinitis, optic neuritis) are similar to HSV and more common in older adults.
Mnemonic for Key Features:
"Can Immune Defenses Really Protect Often?"
C: Contagious phase
I: Immune response (IgG/Tc)
D: Dormancy in ganglia
R: Rash patterns (itchy vs. painful)
P: Primary infection risks (bacteria, pneumonia, encephalitis)
O: Ocular complications
What is the most common form of HSV ocular infection?
Herpetic Keratitis

Connection of End Bulbs and HHV-1 and HHV-2
Herpetic keratitis occurs when HHV-1 or HHV-2, which lie dormant in the trigeminal nerve (cranial nerve V), reactivates and travels to the cornea, causing infection. The virus damages sensory nerves and structures like the end bulbs of Krause, reducing corneal sensation and leading to pain, redness, and vision issues. Repeated infections can result in corneal scarring and impaired healing.
Treatment of HHV-3 (zoster)
acyclovir/famiciclovir/valacyclovir in the first 48-72 hours (double the dose from HHV-1& HHV-2 (simplex))- the infection responds but DNA transcriptase is less responsive
oral steroids may help also antidepressants
An anterior uveitis is common in and concurrent with what in HHV-3?
a facial rash
What is a common complication in adults with post-herpetic neuralgia?
re-infection, which can last for weeks or months after infection and ranges from tingling to pain
Is there a vaccine available for HHV-3?
kids- varicella (live attenuated)
elderly- zostavax
also elderly and immunocomp. - shingrix
What is the primary vaccine for HZV?
Shingrix, it’s a recombinant sub-unit vaccine
How can you diagnose HHV-3?
usually by the physical signs of the disease but you can get RIA, ELISA and agglutination test for antibodies
What is a rare complication after initial HHV-3 infection?
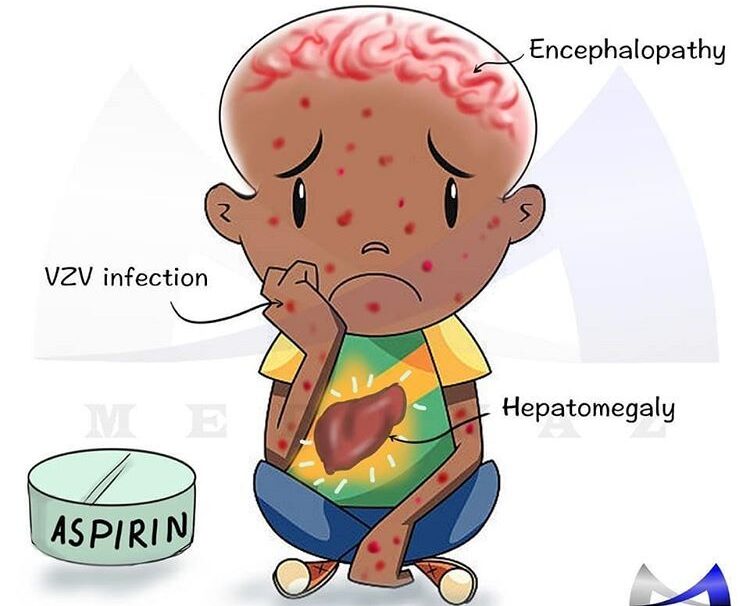
Reye’s syndrome
also seen with varicella and influenza
in kids under 12 that take aspirin during infection
early symptoms - nausea and lethargy (mainly stops here)
1/3 of the time it progresses to an enlarged liver and change in mental status, death, and even coma can ensue
there’s no specific treatment by hydration and steroids can be administered
What is Epstein-Barr virus (HHV-4) characteristics? How is it spread?
a type of lymphocryptovirus (dsDNA) that causes mononucleosis
which is less contagious than other HHV in early life but 90% will contract by 25 years of age
spread by bodily fluids
What bodily fluids cause HHV-4?
saliva, blood, semen
HHV-4 infects what?
it infects the parotid lymph node and gland
local B cells (which are attacked by Tc)
the cell count reveals this disease because you can be asymptomatic
HHV-4 (Epistein Barr Virus) has a correlation with what diseases?
Hodgkin’s Lymphoma and maybe multiple sclerosis
theory that it may cause Burkitt’s lymphoma
tumor of B cells in the parotid and mandible
prevalent in Africa and concurrent with malaria (immune response is impaired by malaria and virus has time to alter B cells and DNA)
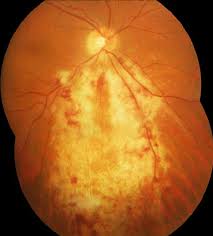
Cytomegalovirus causes a what?
bushfire retinopathy
CMV (HHV-5) pathophysiology
Target cells: Epithelial cells, fibroblasts, and macrophages.
Initial infection: Typically asymptomatic or causes mild sore throat and malaise.
In immunocompromised hosts: May cause viral pneumonia, viral encephalitis, or viral hepatitis.
Common ocular complication: CMV chorioretinitis (“brushfire retinopathy”), especially in AIDS patients.
Most common ocular secondary infection: In HIV/AIDS patients, affecting 7% and second only to HIV retinopathy.
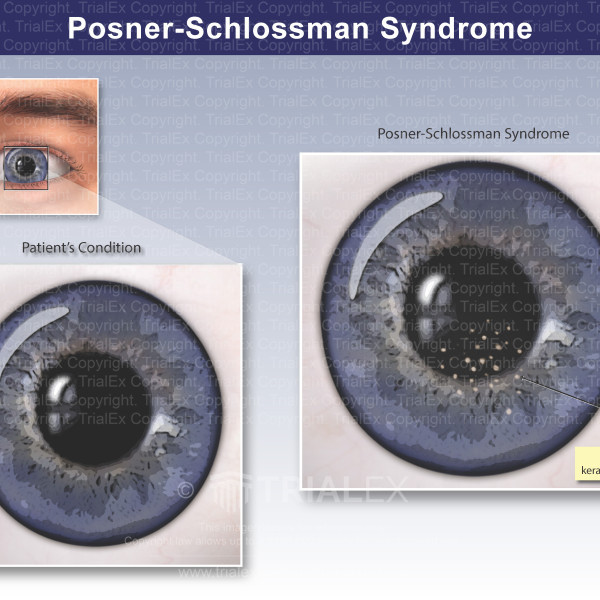
Possible causative agent: In anterior uveitis (with high intraocular pressure) and Posner-Schlossman syndrome (trabecular meshwork inflammation), even in relatively immunocompetent patients.
What is the most common ocular infection in HIV, and what is the secondary most common ocular manifestation behind it?
The most common: HIV retinopathy
The secondary most common: CMV choriretinitis (‘brushfire retinopathy’)
What may CMV (HHV-5) be a causative agent in?
In immunocompetent patients:
anterior uveitis (high IOP)
Posner-Schlossman syndrome (inflammation of the trabecular meshwork)
What is the treatment for HHV-5?
gangciclovir or forcarnet