GI 8: Digestion of Fat and Proteins
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
55 Terms
Liver performs many essential metabolic functions, including?
• Carbohydrate Metabolism
• Protein Metabolism
• Lipid Metabolism
• Drug & Hormone Metabolism
liver functions
1. production and secretion of BILE
- essential for the normal digestion and absorption of dietary lipids
- 600-1200 ml/day
2. eliminate certain metabolic waste products such as Bilirubin
- Bilirubin Accumulation = Toxic (Jaundice)
Biliary System
serves to produce and deliver BILE secretions into the GI tract
includes:
- liver
- gallbladder
- duodenum
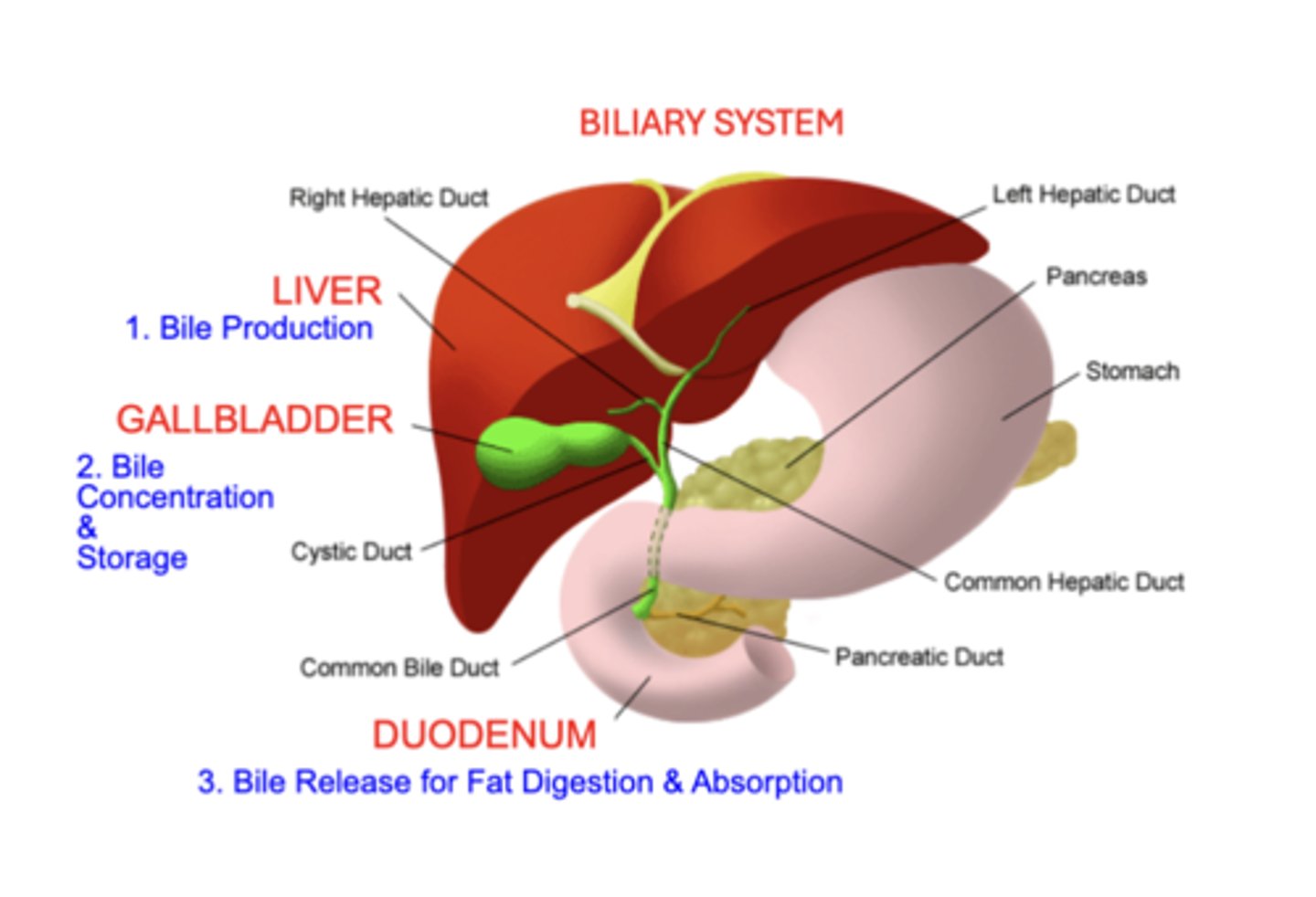
Bile
- produced and excreted by the Liver
- stored and concentrated in the Gallbladder
- released into the Duodenum in response to a meal
Bile Production & Secretion
Bile: 600-1200 ml/day
• Digestion & Absorption of Lipid from GI Tract
Bilirubin Elimination
• Accumulation = Toxic (Jaundice)
Liver histology
- basic functional units of the liver: Liver Lobules
- Groups of lobules are organized around a Central Hepatic Venule
- Sinusoids
- Other types of sinusoids termed Bile Canaliculi
Liver Lobules
- a peripherally located system of blood vessels (Portal Vein & Hepatic Artery)
- secretory Bile Duct branches
- "plates" of hepatocytes (liver cells)
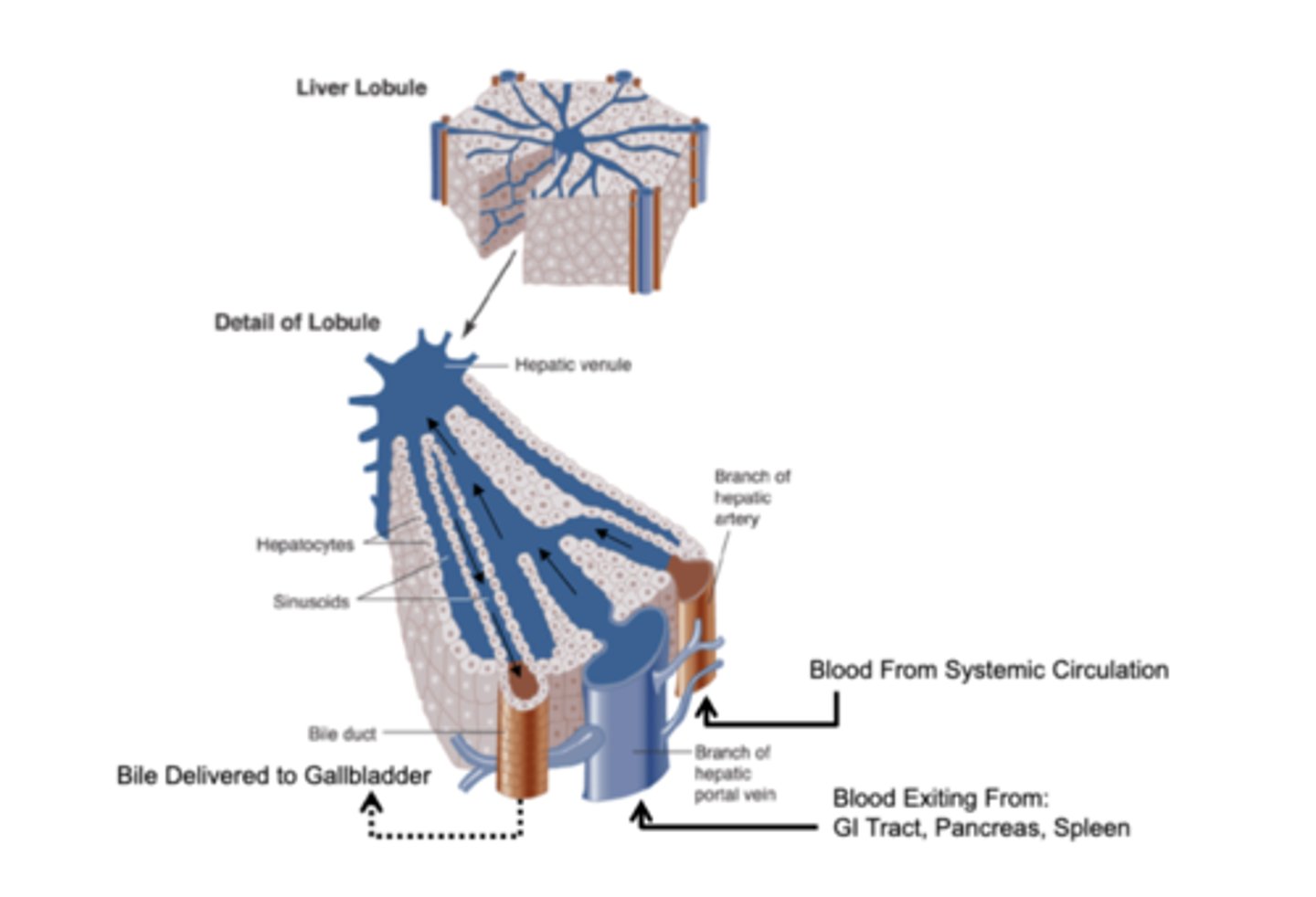
Sinusoids
formed by blood vessels and ducts extending branches between and within the plates of hepatocytes
- function to distribute blood to hepatocytes
Bile Canaliculi
Other types of sinusoids
- located between adjacent rows of hepatocytes
- function as a conduit to deliver bile secreted from hepatocytes to the bile duct
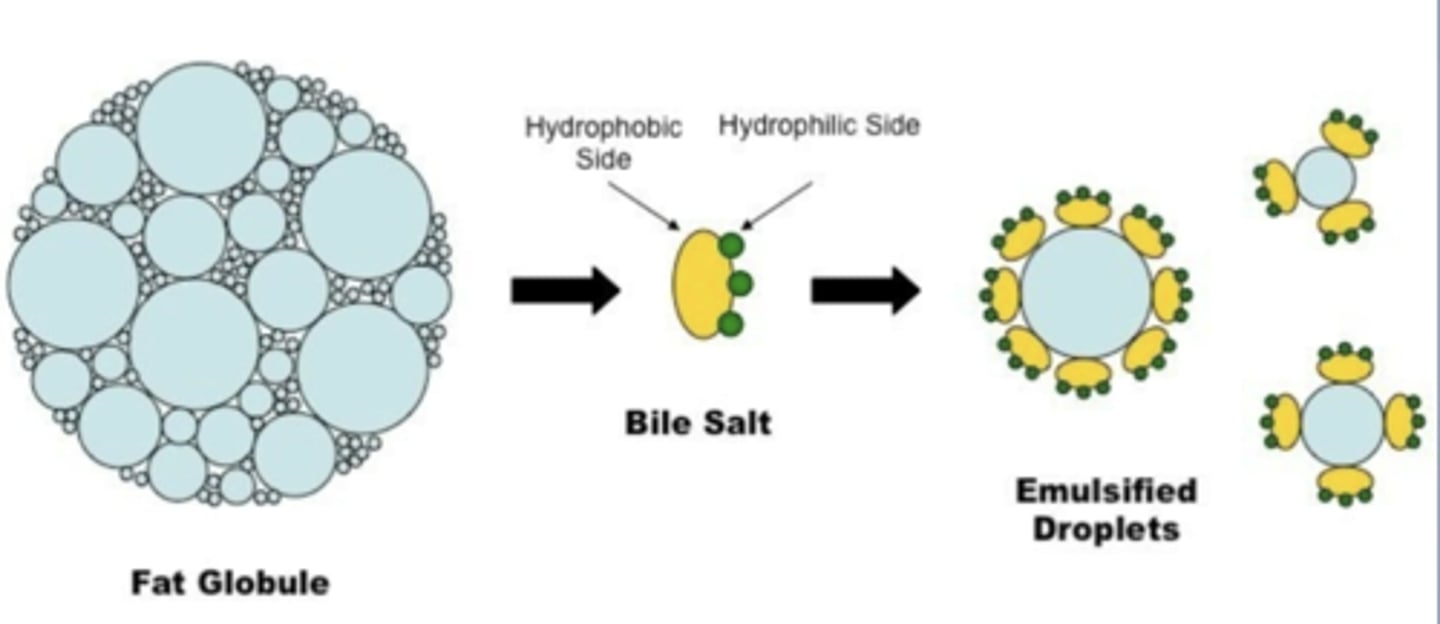
Functions of Bile
1. Lipid Digestion
- Bile Acids: are responsible for Fat Emulsification (like detergent action)
- allows digestion by pancreatic Lipase
- Dietary Fat is Insoluble in the aqueous GI fluids
2. Lipid Absorption
- solubilize fat digestion products (e.g. monoglycerides & fatty acids) into Micelles
- important for the fat absorption
3. Waste Elimination
- Cholesterol and Bile Pigments (Bilirubin) as well as some drugs and heavy metals
Composition of bile
About 1 L/day of Bile fluid
• Bile Salts (conjugated bile acids)
• Phospholipids
• Cholesterol
• Bile Pigments
- Combined with an alkaline isotonic fluid secreted from Bile Duct epithelial cells
• H2O & Electrolytes
• HCO3-,
• Ca++, K+, Cl-, Na+
Bile Acids
• 50% of the organic component of bile
• emulsify lipid material in the intestine through Micelle formation
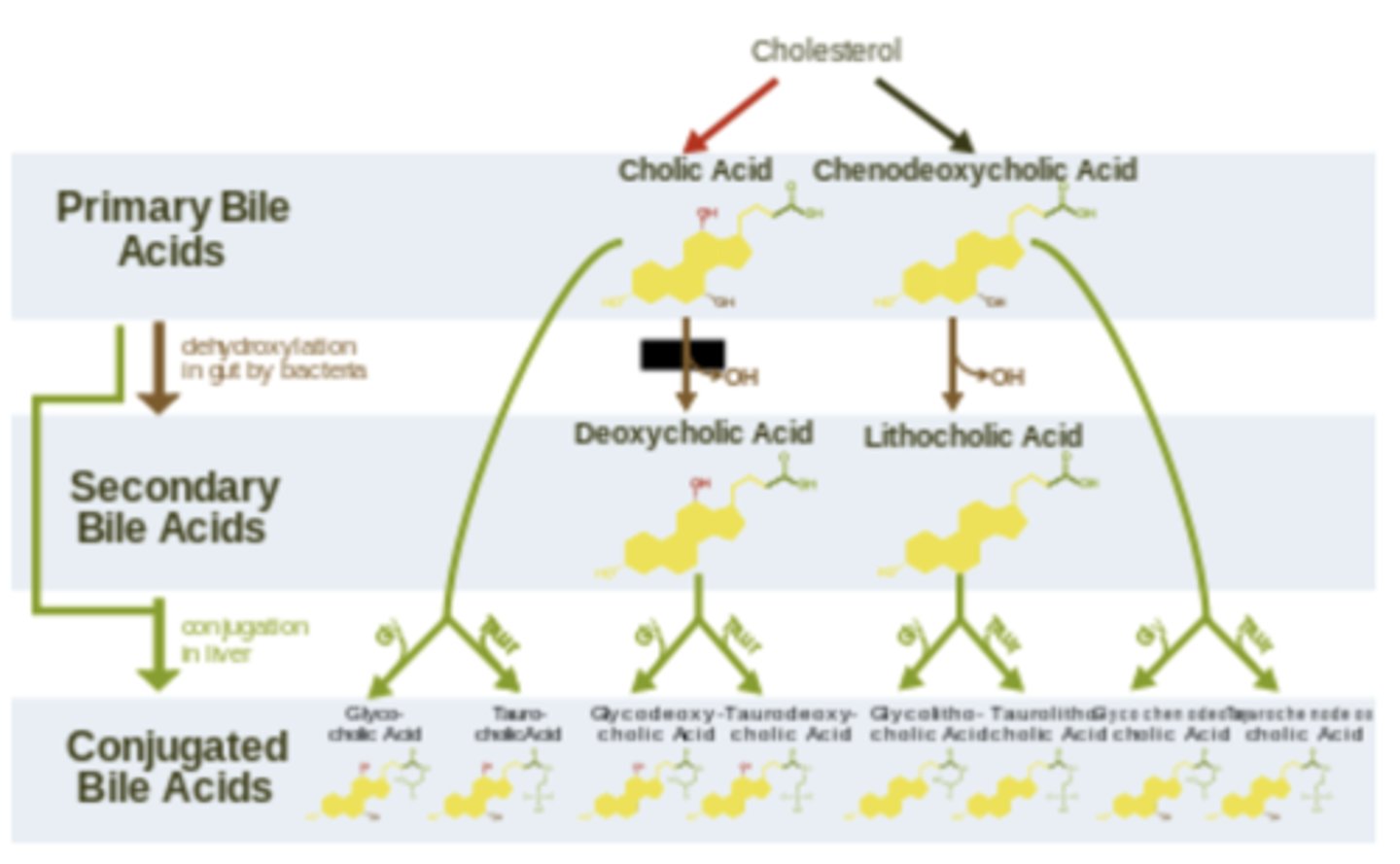
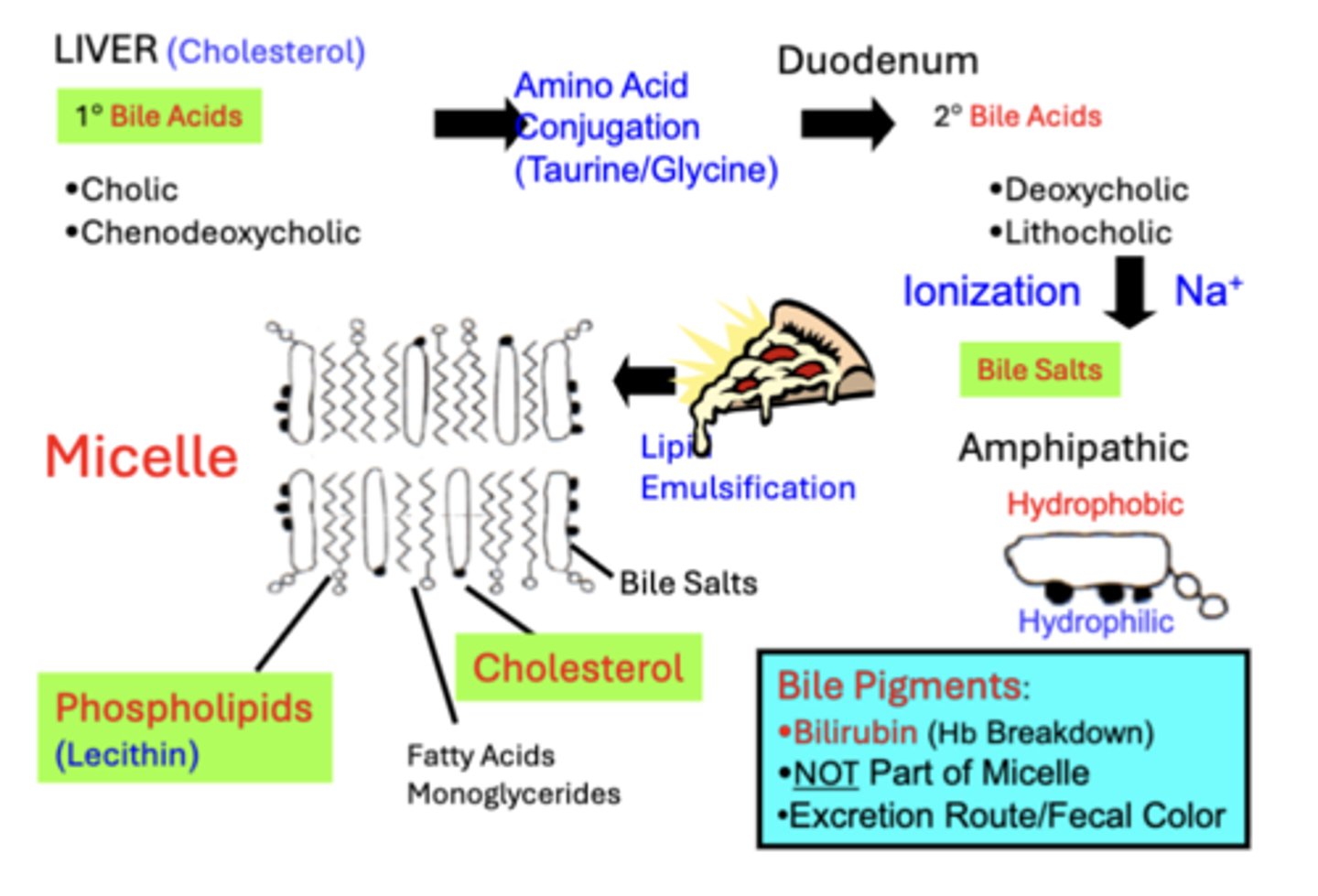
Primary (1°) Bile Acids
• synthesized in the Liver from Cholesterol
• secreted into the Duodenum
• a fraction is converted to 2° Bile Acids by ileal bacteria
Bile salts
• Amino Acid Conjugation & Ionization convert Bile Acids into more water-soluble Bile Salts
• the actual participants in micelle formation
• Bile salts are Amphipathic (Hydrophobic & Hydrophilic), which is important for forming Micelles
Phospholipids
contribute to 30-40% of organic bile
- Lecithins
- Interact with bile salt to support micelle formation
Cholesterol
contributes to 4% of bile
- can only be excreted through bile
- regulates body stores of cholesterol
Bile pigments
do not contribute to lipid emulsification or micelle formation
o Secretion of the bile pigment bilirubin
o Serves as a route for its excretion in feces
o Main cause of characteristic brown fecal coloration
Bile Components & Functions Overview
Bile Secretion
- produced continuously by Liver Hepatocytes
- after secretion, additional H2O, HCO3- and Other Electrolytes, are secreted by the Bile Duct
- regulated by Secretin
Functions of Gall Bladder
- between meals, serves as a storage site
- ready release of bile in response to a meal
− concentrates the fluid by reabsorbing H2O and electrolytes (Na+, Cl-, HCO3-) until release is stimulated
Bile Expulsion: Gall Bladder Contraction
− Stored bile is released into the duodenum when the gallbladder is stimulated to contract.
- contraction is stimulated in response to a meal
Major stimulants of gall bladder contraction during excretory phase:
• Cholinergic Vagal Stimulation (ACh)
• Cholecystokinin (CCK)
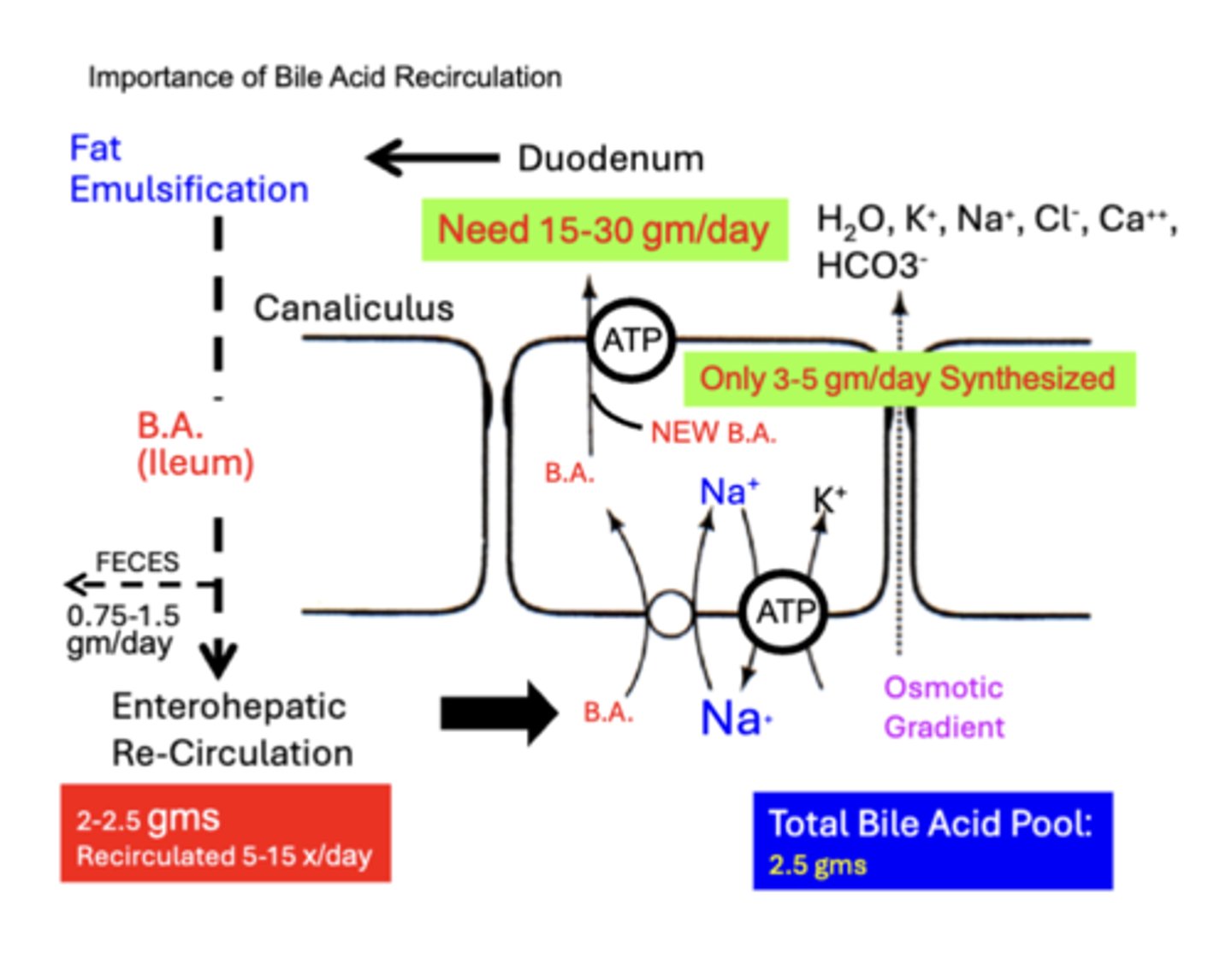
Bile Acid Recycling: The Enterohepatic Circulation
• Most (95%) Bile Acids released into the intestine are Reabsorbed mainly in the ILEUM through passive and active processes
• reabsorbed bile acids are then returned to the liver via the Portal Blood, where they are extracted from the blood by hepatocytes.
• small fraction (5%) of bile acids lost in Feces is replaced through hepatic synthesis of new bile acids

Bile acid recirculation
TOTAL bile acid pool in the human is only 2.5 gms
• However, between 15-30 gms/day of bile acids typically enters the Duodenum
• discrepancy is compensated for by the fact that most of the bile acid pool is reabsorbed through Enterohepatic Re-Circulation (2-2.5 gms) through the biliary system between 5-15 x/day
- only small amounts normally need to be newly synthesized by hepatocytes (New B. A.-) to replace amounts lost in the Feces (0.75-1.5 gm/day)
- importance of the enterohepatic recirculation of bile acids is underscored by the fact that the liver can maximally synthesize only 3-5 gms/day of new bile acids
Impairment of bile acid recirculation
Complications are related to:
• excess H2O & electrolyte loss (Osmotic Diarrhea)
• bile salt excretion and/or impaired fat digestion (Steatorrhea)
Clinical Manifestations of Impairment of bile acid recirculation
related to the severity of impaired bile acid recirculation:
1. Mild to Moderate impairment of ileal reabsorption
- e.g. Infection/Inflammation
- causes excess bile acids to reach the colon
- inhibits colon absorption of electrolytes & H2O due to the osmotic effect of unabsorbed bile acids
2. Severe Loss
- e.g. Ileal Resection
- outpaces new bile acid synthesis
- results in impaired digestion and absorption of long chain triglycerides.
- result in H2O & Electrolyte Loss AND the Undigested Fat Loss in stool (Steatorrhea)
If synthesis of new bile acids by the liver keeps pace with fecal loss...?
fat digestion remains normal
- clinical manifestations are primarily H2O & Electrolyte Loss, but NO Fat Loss in stool (Osmotic Diarrhea)
Steatorrhea can be improved by?
substituting medium-chain triglycerides for long-chain triglycerides in the diet
- small triglycerides do not require micelle formation for absorption
Gall bladder function
primarily functions in Bile Storage & Concentration after it is secreted from the hepatocyte and transported through the bile ducts
Gall bladder Filling
• Bile is produced continuously by hepatocytes and flows into the gallbladder (via bile ducts)
• Between meals, bile diversion into the gall bladder is also facilitated by the high tone of the Sphincter of Oddi, preventing immediate passage into the duodenum
Gall Bladder Capacity
volume capacity of the human gallbladder is limited to 20-60 ml
• total volume of bile secreted from hepatocytes before the gallbladder empties may be many times this amount
• Bile that is initially secreted from hepatocytes (Liver) greatly increases in volume due to the addition of electrolytes (mainly HCO3-) and H2O from bile duct cells
Gall Bladder Bile Concentration
discrepancy between gallbladder capacity and total bile secretion is accounted for by the gallbladder's ability to Concentrate bile 20-fold
- concentrates bile by actively reabsorbing Na+, Cl-, & HCO3-
- H2O follows passively down the osmotic gradient created by electrolyte movement
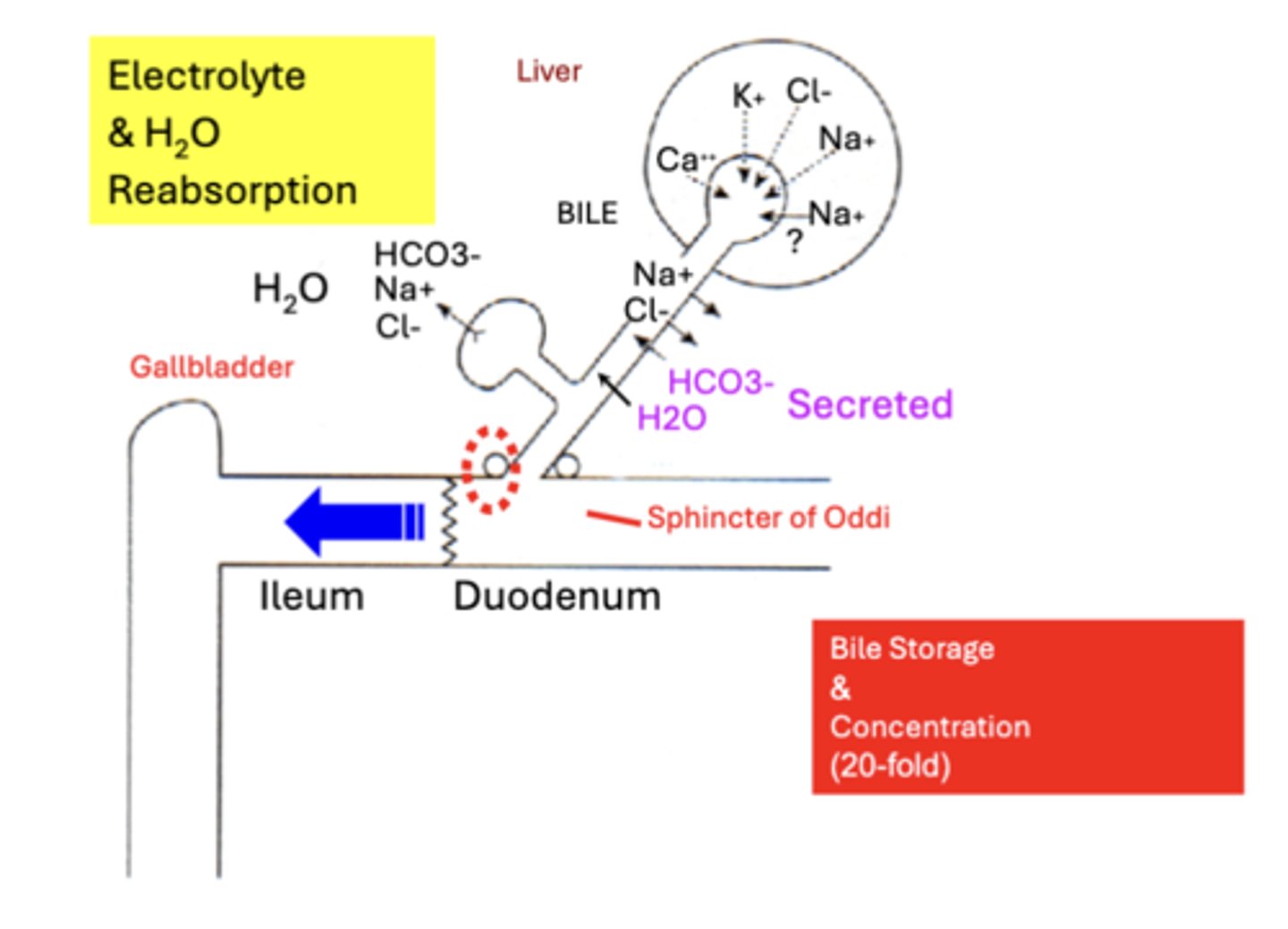
major effects of bile concentration by the gallbladder are
1. a large decrease in fluid Volume (H2O loss)
2. a large increase in the concentration of organic constituents
- Bile Salts, Cholesterol, Bilirubin
- Effects on [Electrolyte] vary
physiological importance of B.A. concentration
1. Micelle formation only occurs when Bile Acids reach a certain concentration, called the Critical Micellar Concentration
• Only at these High [B.A.] concentrations will bile salts aggregate to form micelles.
• This is why clinically, Gallbladder Removal sometimes results in Impaired Dietary Fat Digestion
2. high bile acid concentration is important to solubilize the high concentrations of cholesterol & phospholipids in the gallbladder to Prevent Gallstones
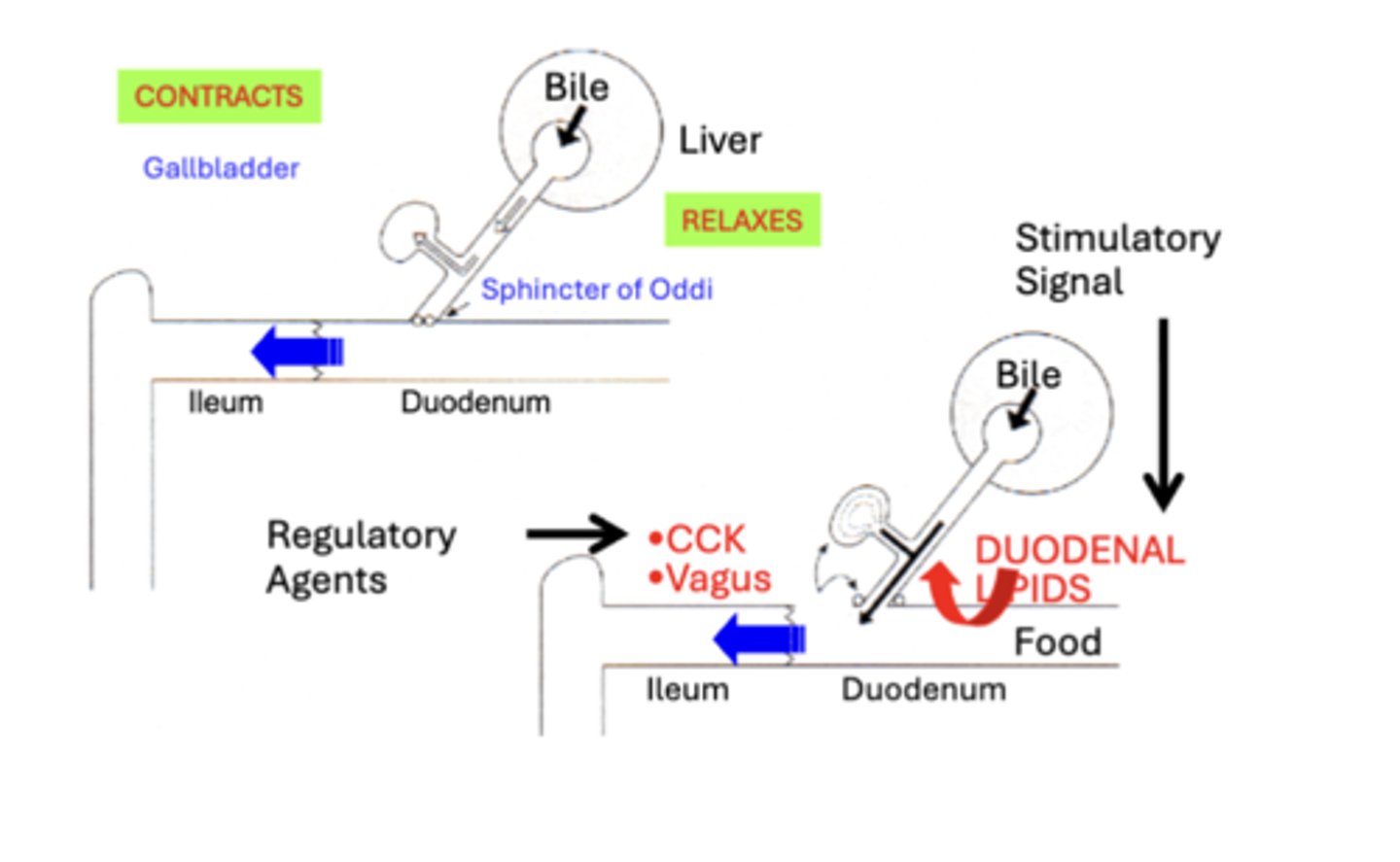
Regulation of gall bladder secretion
Stimulatory Signals
• Bile expulsion is typically initiated within 30 minutes after eating a meal
• Bile is primarily expelled from the gallbladder into the duodenum in response to the presence of Fat Digestion Products (Duodenal Lipids) in the GI tract
Regulatory Agents
• Cholecystokinin (CCK)
• Neural Stimulation (Vagus)
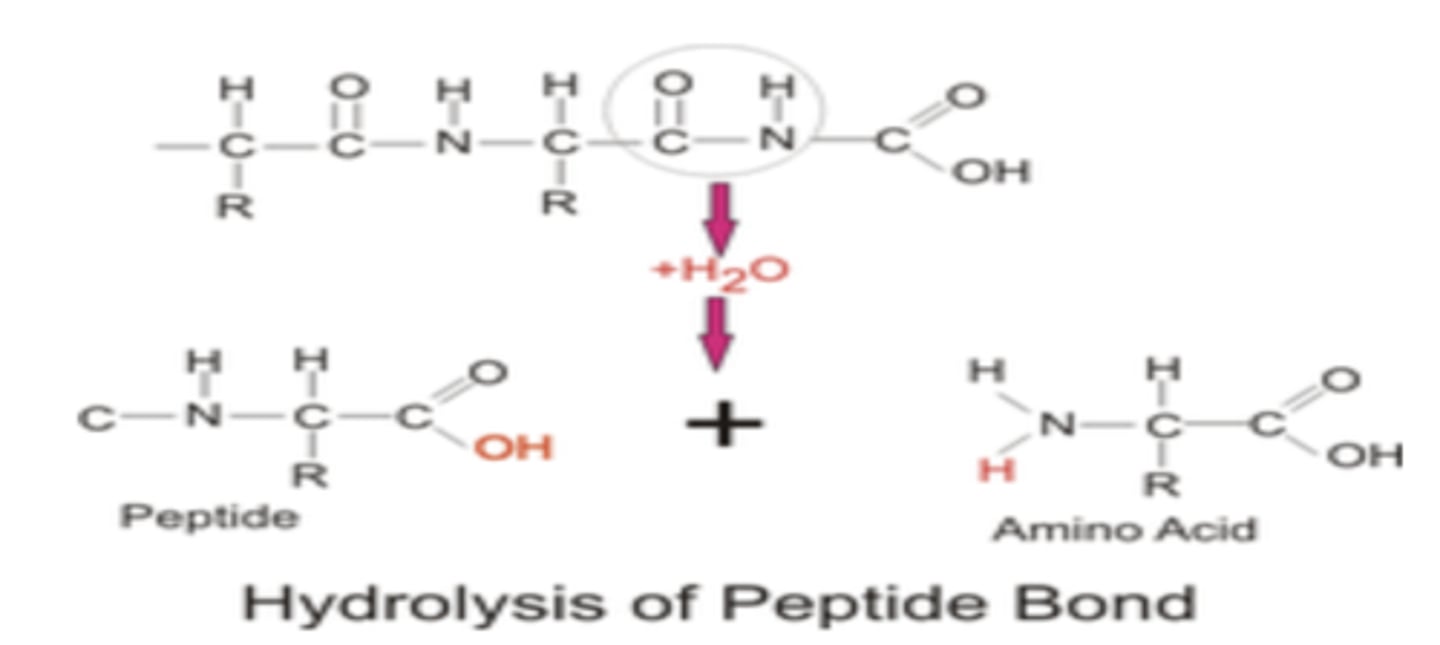
Digestion of proteins
Protein is ingested as large polypeptides and peptides that must be hydrolyzed to
absorbable
- proteolytic enzymes return a water molecule to the protein molecule to split them into amino acids
forms: Amino acids, dipeptides, & tripeptides
Protein Digestion: Stomach
enzyme: Pepsin
substrate: Only initiates
- Collagen and proteins
product: Proteose, peptones and polypeptides
Protein Digestion: Upper Small Intestine
enzyme: Pancreatic enzymes:
• trypsin,
• chymotrypsin,
• carboxypeptidase
• proelastase
substrate: Act on Protease, peptones and polypeptides
product: polypeptides and amino acids
Protein Digestion: Brush Border Enterocytes
enzyme: Peptidases
substrate: polypeptides and amino acids
product: amino acids
GI tract of an individual consuming a typical American diet must process how much protein?
between 90-170 gm protein per day
- well in excess of minimal needs (0.5-0.7 gm/kg body wt./day or 35-50 gm/day for a 70 kg non-lactating adult)
Protein digestion substrate
1. Most comes from Dietary Protein
• typically constitutes 10-20% of daily adult Caloric Intake
2. in addition, GI tract must digest an additional 10-30 gm protein from:
- Gastrointestinal Secretions (Pancreatic, Biliary & Intestinal)
- Exfoliated Intestinal Cells generated from the constant and rapid mucosal cell turnover of the GI tract
In humans, essentially ALL protein is digested and absorbed by?
intestinal mucosa (typically before it has traversed jejunum)
Fecal protein
mainly from bacteria and exfoliated epithelial cells from the distal tract
Source of Protein
Dietary Protein:
• Minimum = 35-50 gm/day
• Avg. American = 70-110 gm/day
GI Secreted Protein: (10-30 gm), Enzymes & Mucin
• Gastric
• Pancreatic
• Biliary
• Intestinal
Exfoliated Epithelium: (10-30 gm)
•Constant & Rapid Mucosa Turnover
Protein Ingestion
ingested as large Polypeptides & Peptides
that must be hydrolyzed to absorbable:
• Amino Acids, Dipeptides & Tripeptides
• by Proteolytic Enzyme action
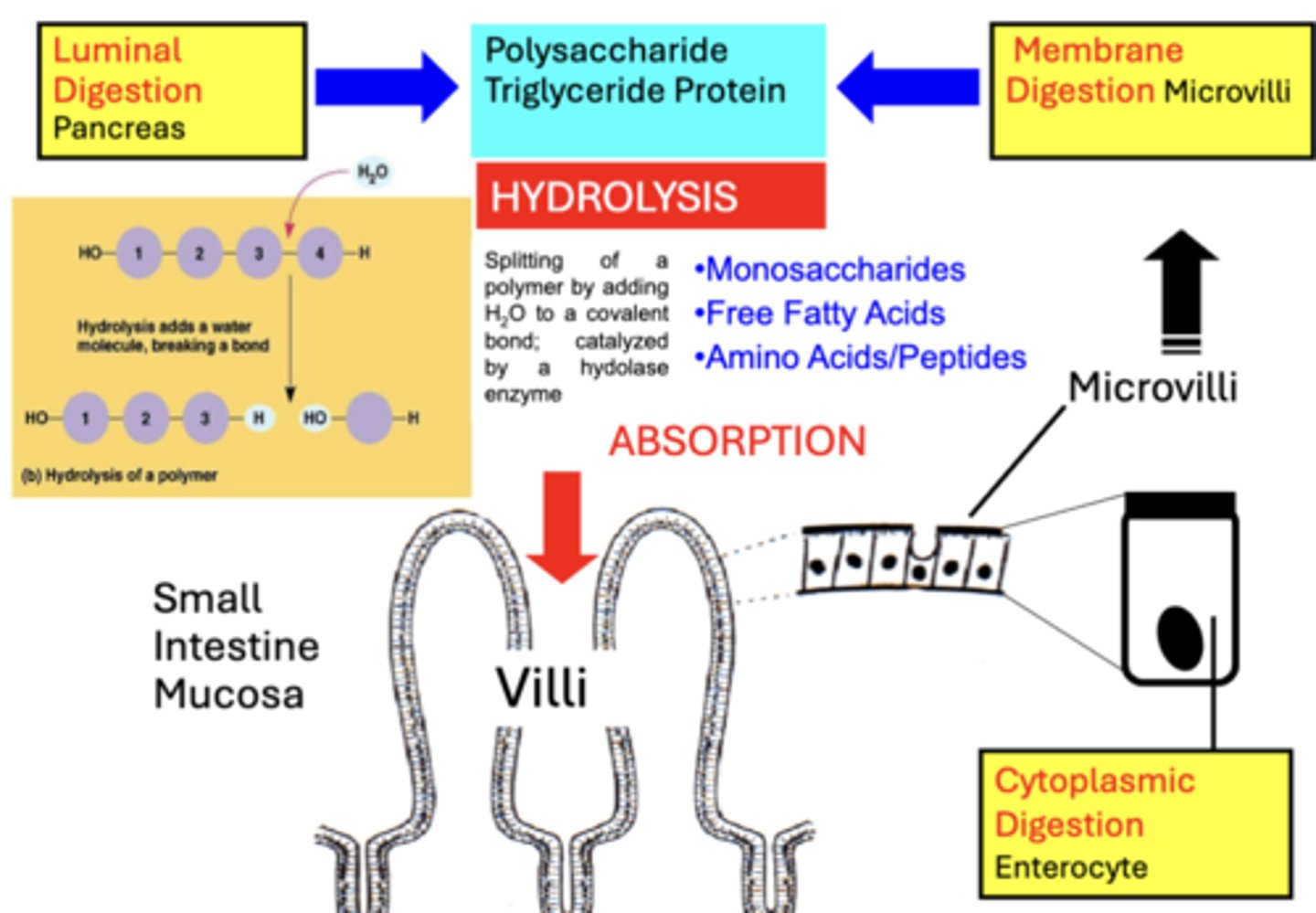
Phases of Protein digestion
distinguished into 3 types based on the Site of Digestion:
1. Luminal (cavital) Digestion
2. Membrane (contact) Digestion
3. Cytoplasmic digestion
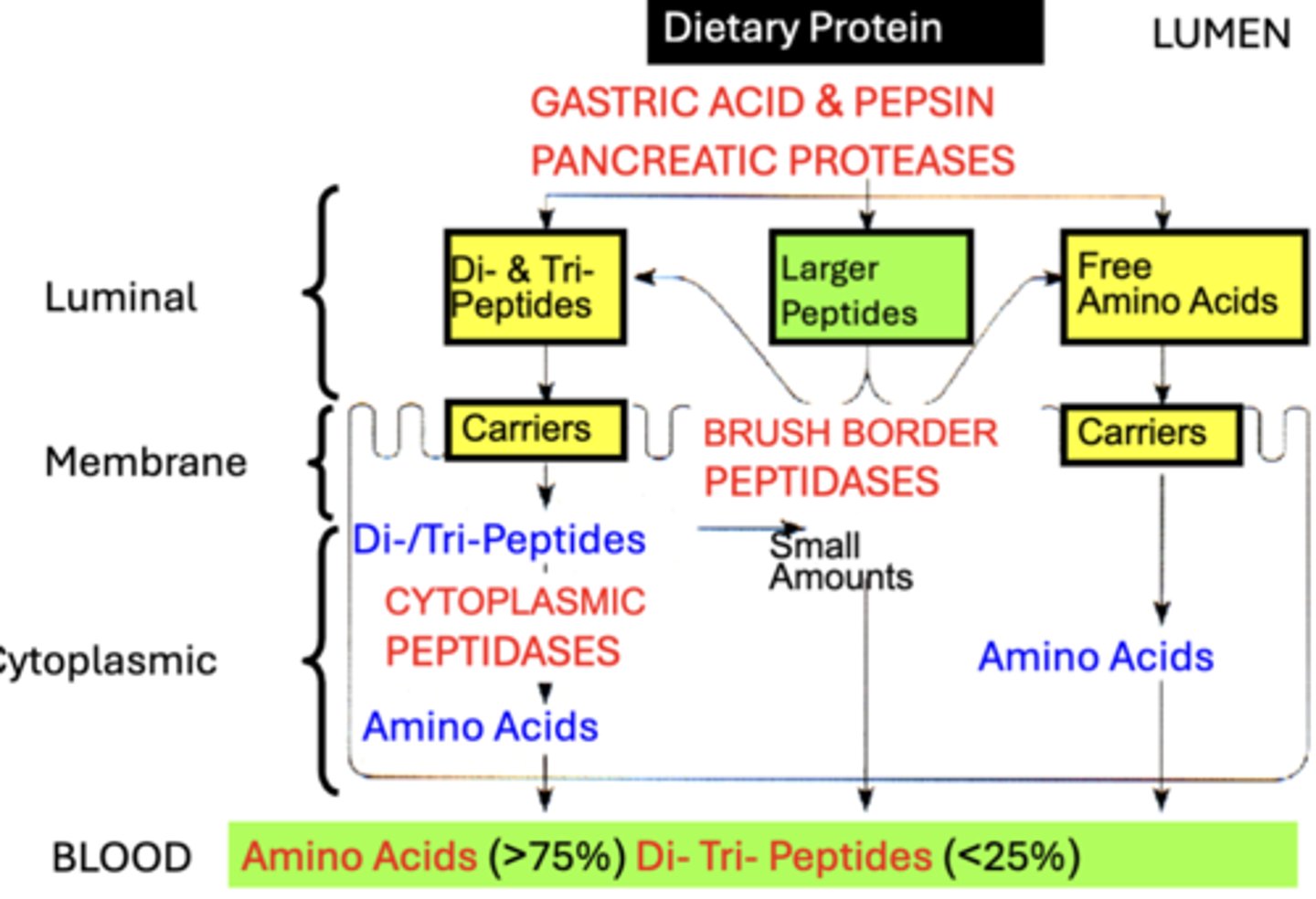
Luminal Digestion
1. Dietary Protein digestion begins in the stomach
- through the actions of Gastric Acid and Pepsin
- Gastric actions account for 15% of protein digestion, but is NOT considered physiologically essential
2. Luminal Digestion occurs mainly through actions of Pancreatic Peptidases secreted into the small intestine:
• End-products are predominantly:
- absorbable Free Amino Acids & small Di- & Tri-Peptides
- which are transported across the brush border
Membrane Digestion
Small amounts of Larger Peptides (4-8 amino acids) remain after luminal digestion
- Non-Absorbable
- must be further digested via Membrane Digestion
Brush Border Peptidases
- located at apical membrane of enterocytes
- serve to further digest Larger Peptides into Free Amino Acids & Di-/Tri-Peptides
Cytoplasmic digestion
- Very minor amounts of unabsorbable larger peptides remain after membrane digestion
- Products are rapidly absorbed across membrane into enterocyte for Cytoplasmic Digestion:
• Intracellular Cytoplasmic Peptidases complete the protein digestion process by further hydrolyzing absorbed Di-/Tri-Peptides into Amino Acids
end products: mostly Free Amino Acids (75%)
- leave the cell and the enter Blood across the basolateral membrane
Enzymes for Luminal digestion
Proteolytic enzymes produced by Pancreatic Acinar Cells (Enzymatic Component)
1. Endopeptidases
2. Exopeptidases
Endopeptidases
hydrolyze only Interior peptide bonds
- end-products of endopeptidase digestion are Mostly Small Peptides
include:
• Gastric Pepsin
- aromatic amino acids
• Pancreatic proteases:
1. Trypsin(s)
- Basic Amino Acids
2. Chymotrypsin
- aromatic Amino Acids
3. Elastase(s)
- neutral Amino Acids
exopeptidases
remove one amino acid at a time from Exterior C-terminals
- End-products: Mainly Amino Acids and some incompletely digested peptides
include:
• Carboxypeptidase A
- Aromatic & Neutral Amino Acids
• Carboxypeptidase B
- Basic Amino Acids
Luminal digestion: Pancreatic proteases
• initially secreted (Pancreatic Precursors) as inactive peptidases
• must be enzymatically cleaved to form active peptidases within the small Intestinal Lumen
• activation cascade is initiated by the brush border enzyme ENTEROKINASE (also called Enteropeptidase-)
→ cleaves a hexapeptide from the pancreatic precursor Trypsinogen, forming proteolytically active Trypsin
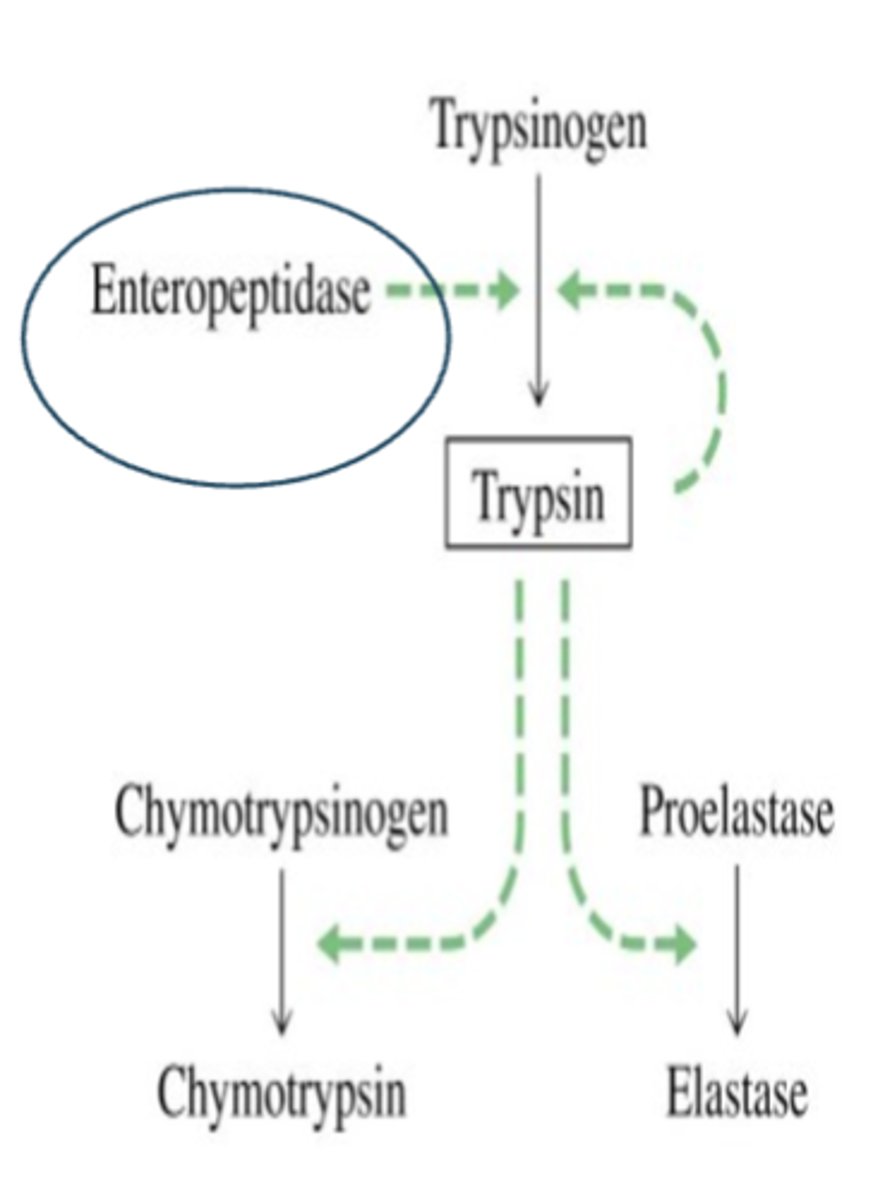
Trypsin
Autocatalytic
• once a small amount of trypsin becomes activated it cleaves its own precursor,
which accelerates its own activation
Trypsin then cleaves all other pancreatic protease precursors
• Chymotrypsinogen, Proelastase, Procarboxypeptidase A & B
• to their active form
- Chymotrypsin, Elastase, Carboxypeptidase A & B
end products of pancreatic protease digestion
mostly Free Amino Acids and Di- & Tri-Peptides
• absorbed across the brush border
• Pancreatic protease Inactivation occurs through Autodigestion or Cross Digestion
Big picture of Enzymatic digestion
A. Luminal (Cavital) Digestion is performed by digestive enzymes secreted into the GI Lumen
- mainly by pancreas but also stomach & salivary glands
B. Membrane (Contact) Digestion is performed by digestive enzymes bound to apical Microvilli that comprise the "brush border" of small intestine enterocytes
C. Cytoplasmic digestion is performed by digestive enzymes located within the Cytoplasm of small intestine enterocytes
- Mainly relevant to protein digestion
result is the formation of smaller molecules that can be absorbed by small intestine
- Monosaccharides, Fatty Acids, & Amino Acids