SBVAC Week 7 OB/GYN
1/91
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
92 Terms
What does Geriatrics refer to? How does it affect care?
Population over 65 years old, these are patients who need special precautions due to their age
Physiologic Changes of Aging
What is physiological reserve and how does it change?
Aging affects physiologic function of all body tissue, leading to decreased function in the body.
There is a decreased physiological reserve (body can’t respond to stressors as well) and immune system decline
What are the cellular changes of aging
Decreased cell replication and increased DNA damage and oxidative stress
Decreased cell replication causes decreased blood cell replication and regeneration, and bone thinning and skin thickening
What are respiratory changes with aging?
DECREASED size and strength of respiratory muscles, leading to higher risk of respiratory infection
Enlargement of alveoli in lung tissue leads to decreased chest expansion, reduced coughing/gag reflex, and lowered chemoreceptors to determine CO2 or O2 levels.
Cardiovascular changes with aging
Hypertrophy (thickening) of the heart with age, thicker wall takes up more space, and the ventricle holds less blood
There is decreased collagen and elastin, leading to less elastic vessel walls → higher/wider BP and poor circulation, aortic valve stenosis occurs that impairs blood flow
Increased risk of clots due to lack of movement, and electrical conduction system deteriorates as number of pacemaker cells decreases
What are some nervous system changes with aging?
DECREASED brain weight and volume, loss of 5-10% of neurons.
Changes in 5 physical senses, thinking speed, memory, and posture stability changes
How does vision change with aging, and what is the outcome? What is the inability to see up close called?
Depth perception, vision acuity, and adjustment to light are changed with age.
Outcome:
Decreased tear production
Can’t differentiate colors
Diminished night vision
Presbyopia (inability to see up close)
How does hearing change with aging, and what is the outcome? What is the gradual hearing loss called?
Hearing sounds become more difficult due to inner ear changes
Outcomes:
Problems with balance →likely to fall
Presbycusis → gradual hearing loss
How does taste change with aging? What is the outcome?
Lessened number of taste buds
Outcome:
Weight loss
Malnutrition
Fatigue
How does touch change with aging? What are the outcomes?
Loss of end nerve fibers causes decreased sense of touch and pain perception
Outcome:
Decreased sensation of hot and cold
Geriatric patient may not feel injury
What are some musculoskeletal changes with aging? What is reduced bone, muscle mass called? What is the inflammation of joints called?
Osteoporosis(reduced bone mass) and Sarcopenia(reduced muscle mass), reduces strength
Arthritis (painful inflammation of joints destroying cartilage) and wearing down of intervertebral discs lead to decreased height and posture issues.
All of these lead to difficulty with tasks requiring fine motor skills
What are some gastrointestinal changes with aging?
(Less liquid, less digestion, less excretion)
Gastric secretions are reduced, and there’s less saliva production.
Gastric motility is decreased, and there is a higher chance of bowel-related diseases.
Peristalsis(wave movement) leads to constipation, and decreased size and strength of rectal sphincter leads to incontinence.
What are some endocrine system changes with aging?
A decrease in thyroid hormones leads to:
Decreased heart rate
Fatigue
Dry skin and hair
Cold Intolerance
Weight gain
A fluid imbalance due to increased secretion of antidiuretic hormones, resulting in hyperglycemia
What are renal system changes associated with aging?
Kidneys shrink in size and weight, leading to less nephrons(filtering units). The decrease in kidney mass leads to electrolyte imbalance/dehydration
Causes a reduction in renal function and renal blood flow and lower bladder capacity.
What is Pneumonia? How does it change in geriatric patients and what are some S/Sx
An infection of the lungs from bacteria/viral causes, leading to fluid/pus accumulation in the alveoli
The risk of respiratory infection increases with age, partly due to increased exposure due to frequent hospitalization
S/Sx: Rhonchi lung sounds, Shortness of breath, productive cough, or asymptomatic due to weakened immune system
What is Pulmonary Embolism? How does it change in geriatric populations and what are some S/Sx?
The sudden blockage of an artery by a venous clot
There are increased risk factors such as living in a nursing home, recent surgery, history of heart failure or clots, and sedentary behavior
S/Sx: Sudden onset of Dyspnea, shoulder/back/chest pain, cough, hemoptysis (coughing of blood), syncope (temp. loss of consciousness)
What is Atherosclerosis? How does it change in geriatric populations and what are some S/Sx?
The buildup of fat and cholesterol (plaque) in and on artery walls
In geriatric populations, there is an increased risk of developing the condition due to stiffening of arteries
S/Sx: Chest pain, leg pain, shortness of breath, fatigue on exertion, or asymptomatic
What is Congestive Heart Failure? How does it change in geriatric populations and what are some S/Sx?
When the heart muscle can’t pump blood as effectively as it should
In geriatrics, there is an increased risk due to comorbidities such as hypertension, coronary artery disease,
S/Sx: Peripheral Edema, Pulmonary Edema, Shortness of breath, or asymptomatic
What is a heart attack? How does it change in geriatric populations and what are some S/Sx?
Occurs when blood flow to part of the heart muscle is blocked
Geriatric patients present atypically during a heart attack compared to younger patients (fatigure, shortness of breath, acute confusion)
S/Sx: “Silent” heart attacks (prevalent in women and diabetics), dyspnea, nausea/vomiting
What is delirium? How does it change in geriatric populations and what are some S/Sx?
What are the increased risk factors for this**
Temporarily disturbed state of mind, usually has rapid onset
Geriatric patients have an increased risk (DELIRIUM):
Diabetes (increased risk)
Emotional
Low O2
Infection
Recent Surgery
Ictal (Seizures)
Undernutrition/dehydration
Meds/alcohol effects
S/Sx: Hallucinations, restlessness, incoherent thought/speech
What is Dementia? How does it change in geriatric populations and what are some S/Sx?
Progressive loss of cognitive function due to neuronal death
Geriatric patients have an increased risk for dementia and associated conditions?
S/Sx: Baseline AMS, rarely any hallucinations, irreversible, progress loss of cognitive, psychomotor, and social skills
What is Alzheimer’s and what is it caused by? How does it change in geriatric populations and what are some S/Sx?
Most common form of dementia, thought to be caused by abnormal buildup of proteins in and around brain cells
Geriatric patients have an increased risk for Alzheimer’s, with the risk doubling every 5 years after turning 65
S/Sx: Misplaced objects and trouble recalling names (early stage), difficulty with moving, eating, swallowing, and speech (late stage)
What is Parkinson’s Disease? How does it change in geriatric populations and what are some S/Sx?
Age-related neurological disease thought to be caused by gradual loss of dopamine-producing cells
Geriatrics are at higher risk of developing the disease, as these neurons automatically decline by age. Older patients have more pronounced symptoms
S/Sx: Resting tremors, rigid extremities, mask-like face, depression, bradykinesia (slow movement)
What is a stroke? How does it change in geriatric populations and what are some S/Sx?
When blood flow to the brain is interrupted, causing a lack of oxygen and nutrients to the brain. Can be ischemic or hemorrhagic
Blood clots and brain bleeds are more common in geriatrics, ask for blood thinners and baseline presentation
S/Sx: AMS, numbness, weakness, or paralysis on one side, slurred speech, visual disturbance, headache/dizziness, incontinence, seizure.
What are some musculoskeletal related conditions in geriatrics? What is the loss of joint flexibility
Falls:
More prevalent in geriatrics due to vision, gait, balance, and orthostatic hypotension
Ask about blood thinners
Higher chance of injury due to sarcopenia
Osteoarthritis:
Joints lose their flexibility
Affects joints in the hands, knees, hips, and spine
Decreased muscle mass leading to less strength
What is Chronic Kidney Disease? What are the two types of incontinence? How does urinary retention get affected?
Kidney Disease:
Geriatrics can experience Chronic Kidney Disease (CKD), leading to kidney failure
Could be on hemodialysis 3x a week (machine filtering blood), missing dialysis causes lethal toxin buildup
Incontinence
Stress incontinence: Incontinence during activities like coughing, laughing, sneezing, lifting, and exercise
Urge incontinence: Incontinence triggered by hot or cold fluids, running water, or thinking about going to bathroom
Urinary Retention
Difficulty urinating
Enlargement of the prostate in geriatric men makes urination difficult
Severe cases of urinary retention can cause renal failure
What are some hospital-related conditions for geriatrics?
Decubitus Ulcers
Bedsores/pressure ulcers that form due to immobility
Usually found on lower legs, sacrum, and glutes
Occurs most in nursing homes or prolonged hospital stay
Patients must be turned every 2 hours in nursing homes
UTIs:
Urinary tract infection, occurs when a foley catheter is left too long in geriatric patients, check the catheter for color and opacity of urine, as well as blood
Common hospital-associated infection, more prevalent in women (shorter urinary tract)
S/Sx: Shortness of breath, painful urination, polyuria, can lead to septic shock
What is Polypharmacy? What are some common drug (endings)?
Simultaneous use of multiple drugs at a time by a single patient (geriatrics are on a lot of medication), causing multiple side effects
Ask about ALL medications they’re taking and medical history, some common ones include:
Metformin (Diabettes)
Drugs ending in “statin” (high cholesterol)
Drugs ending in “pril” or “olol” (hypertension)
Drugs ending in “cillin” or “mycin” (antibiotics)
How is suicide and depression affected by geriatrics?
More prevalent due to loneliness, loss of function, lack of independence, extremely common in older patients
Older men most at risk for suicidal ideation, substance and prescription abuse along with chronic medical conditions lead to depression
What are some increased risk factors for falls in geriatrics?
Increased age
Gender (women more prone)
Drugs (Greatly increases if more than four medications are taken)
Benzodiazepine use increases falls by 44%, used to treat anxiety by depressing the CNS
Living alone
Poor nutrition
Cognitive disorders
What are the main problems with geriatric falls?
Environmental Factors increase fall risk
Poor lighting
Uneven surfaces
Slippery Floors
Missed steps/slips/trips
Hip Fractures
90% of hip fractures caused by falls in geriatrics
What are EMS considerations or what may you see on geriatric calls?
Indwelling catheter
Lung Drains (chest tubes)
Feeding Tube
Colostomy Bag
What should you look out for on geriatric calls? (Report)
Elder abuse and neglect, most common in women older than 75 years old
How can you move a geriatric patient?
Sheet transfer, have the patient “hug themselves,” and have all crew members hold the sheet taut as close to the body as possible. (move them to another place)
What are some important questions for geriatrics?
All medications they’re taking (especially blood thinners)
Advanced Directives (DNR, MOLST)
Baseline Presentation (Geriatric patients can suffer from more than one condition normally)
What is palliative care?
Comfort care provided to people with serious illnesses to improve quality of life (treating for comfort, not the disease)
What is hospice care?
Form of palliative care in which the prognosis of the patient is 6 months or less, focusing on symptom management, spiritual, and psychosocial support for end of life care
What defines a child?
Pediatric Protocols are used for children under 15 years old
How does consent work with children?
Consent considered as the ability of the patient to understand and make an informed decision about their health care.
Minors (under 18) are generally not able to provide consent, guardians/parents must provide informed consent
If parents are not present and care is needed, implied consent is applied even if minors refuse care
How are airways different in children?
Their airways are smaller! They have narrow nostrils, looser teeth, and a larger tongue relative to the oropharynx
The epiglottis and trachea are smaller and collapse easier
What is the pediatric airway positioning? Why is it used?
Children have larger heads, which flexes the neck and compresses the soft airway
Use the classic sniffing position, don’t overextend the head/neck, and apply head rests or shoulder rolls if needed
How is blood volume affected in children?
Newborns only have 300 mL of blood!
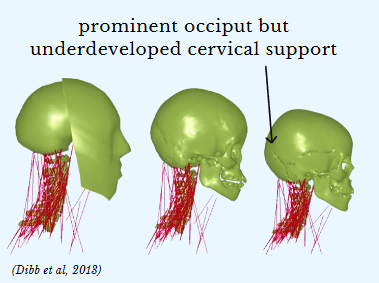
How do massive heads in children affect their skull structures? What about chance for injury?
Children have a prominent occiput but underdeveloped cervical support. Their big heads can cause injury with little injury or obvious signs!
Infants have fontanelles, a “soft spot” caused by any of the soft membranous gaps between the incompletely formed cranial bones of an infant.
How are organs affected in children?
Organs of children are vulnerable, as bone development starts as cartilage, hardening gradually by ossification.
What is pediatric shock like? What are some early signs and late signs of shock?
Children maintain blood pressure by increasing heart rate and vasoconstriction, while losing up to 1/8 of blood volume.
They decompensate extremely fast! Hypotensive pediatrics approach cardiac arrest!
Early Signs:
Sustained Tachycardia
Capillary refill > 2 seconds
Cold, clammy extremities
Late Signs:
Weak peripheral pulses
Decreased consciousness
Hypotension
How do you recognize if a patient is sick or not? What are some indicators for adult and pediatrics***?
Literally just look at them.
Adult Indicators:
MOI/NOI, obvious trauma
Pulse, respirations, skin
Level of Consciousness
Pediatric Indicators:
Appearance
Work of breathing
Circulation to skin
What is the Pediatric Assessment triangle? What does it do?
Appearance, work of breathing, and circulation to skin.
Informs oxygenation, brain perfusion, and overall CNS function
What is the Appearance section of Pediatrics?
(TICLSC)
Tone: Good muscle tone?
Interactiveness: Responds to people or environmental changes?
Consolability: Able to be comforted by caregiver or responder?
Look/Gaze: Maintains eye contact with objects/people? Fixes gaze on faces?
Speech/Cry: Strong and spontaneous crying?
Color: Skin color? Visible differences between trunk and extremities?
What is the Work of breathing section of Pediatrics?
Does the child require extra effort to move air in and out?
(PAR)
Positioning: Sniffing position, tripoding, head bobbing, nasal flaring?
Adventitious lung sounds: Stridor, wheezing, rales, or rhonchi?
Retractions: Visible sinking-in of soft tissues, especially in the chest or neck?
What is the Circulation to skin section of Pediatrics?
Skin signs reflect overall circulation status
(CCP)
Color, temperature, condition: Examine the child’s calf or forearm
Capillary Refill: Blanch a distal extremity, such as the nail bed or foot
Pulse: Rate and strength of the brachial or radial pulse. Are the vitals normal?
What are the divided age ranges?
Neonates: Birth - 28 days
Infant: 1 - 12 months
Toddler: 1 - 2 years
Preschool: 3 - 5 years
School Age: 6 - 11 years
Adolescence: 12 - 18 years
How do the vital signs of extremely young children compare to that of older children?
Heart Rate: Much higher in younger patients (Small heart)
Respiratory Rate: Much higher in younger patients (Small Lungs)
Systolic/Diastolic BP: Much lower in younger patients
MAP (Mean Arterial Pressure: Much lower in younger patients
What are some developmental conditions for infants?
May have separation anxiety
Provide sensory comforts
Be careful of nasal obstructions
What are some developmental conditions for toddlers?
May have stranger anxiety
Approach slowly, limit physical contact, use a quieter
Use play or distraction objects
Have parent hold ask history
Not very good at describing pain
What are some developmental conditions for preschool age?
Explain procedures simply
Praise and set limits on behavior
What are some developmental conditions for school age?
Explain all procedures beforehand
Speak directly, don’t negotiate
What are some developmental conditions for adolescents?
Explain procedures and why
Show and respect independence
Ask some questions privately
What are common pediatric emergencies?
Fevers, Seizures, Sirs (sepsis), and respiratory infections
How do fevers present in children? How to take history and a physical assessment, and what are some considerations?
38 C or higher
History:
OPQRSTI, SAMPLE
Recent or household illness
Up-to-date immunisation status
Maximum temperature, method
Food and consumption, urination, and bowel movements
Physical Assessments:
Bulging or sunken fontanelles
Rash, especially if NON blanching
Palpable abdominal mass
Considerations:
Fevers most commonly caused by some form of infection
For patients less than 3 months old, note and be careful of tylenol, aspirin, or other fever reducers
How do seizures present in children? How to take history and a physical assessment, and what are some considerations? What is a common seizure type in children
History:
OPQRSTI, SAMPLE
Infection, head trauma, epilepsy, electrolyte imbalance, toxins, hypoglycemia, birth injury
Diastat is commonly prescribed gel form of valium (diazepam)
Febrile Seizures:
Accounts for most seizures in patients 6 months - 6 years
< 15 minutes, generalized tonic-clonic and short postictal period
How do sirs/sepsis present in children? How to take history and a physical assessment, and what are some considerations?
Systemic inflammatory response
Syndrome + known infection → sepsis
Systemic organ damage and failure
Physical Assessment:
Hypo/hyperthermia
Heart rate and respirations above normal age range by 2 Standard Deviations
Additionally: signs of shock
What are the types of respiratory infections in children? How to treat?
Primary Infections:
Common Cold (viral): cough, runny nose, sore throat, body aches
Croup (viral): stridor, seal-like barking cough, fever, running cough
Secondary Infections
Sinusitis (viral, bacterial): sinus pressure, congestion, cough, runny nose
Bronchitis (viral): wheezing, congestion, fever, runny nose, sore throat
Pneumonia (viral, bacterial): chest pain, tachy/dyspnea, cough, fever
Many of these are similar and can’t be distinguished prehospitally. Treat with humidified O2, albuterol, rapid transport, and ALS as necessary, using APPROPRIATE PPE as necessary!
How should oxygen therapy be used on children?
Any child with a respiratory emergency or significant trauma should receive oxygen
Blow by oxygen: For children who can’t tolerate an NRB or NC, hold mask 2 inches from the face, making sure NOT to over-ventilate
What are some other interventions for children?
Consider giving humidified O2 via a nasal cannula to reduce nasal discomfort and irritation to moisten airways
Provide parental reassurance and guidance!
BGL can be taken at the heel!
What are concerns of poisoning in children? What are some common sources?
Oral seeking is a common developmental characteristic (children like putting things in mouth)
S/Sx depend on poison
Common poison sources:
Alcohol, pills, vitamins
Houseplants
Cleaning Products
What are concerns of trauma in children? What are some pediatric trauma centers?
Trauma kills more children than all other causes combined
Causes:
Submersion injuries, burns, abuse, neglect and trauma from firearms, MVAs, pedestrian and bicycle injuries
Consider mechanism in deciding in stable or critical
Centers:
Stony Brook University (lvl 1), Good Samaritan Hospital (lvl 2)
How to do SMR on children?
Roll towels and place on the sides of the head, or an upside down KED can be used as a full-body splint, just tape the forehead.
What are some sudden events that can occur in children? What must you do if these occur?
Sudden Infant Death Syndrome:
Unexplained death of a child < 1 year old, often while sleeping
Typically presents as cardiac or respiratory arrest
In cases of SIDS, law enforcement MUST be called, an investigation needed to rule out other causes of death
Brief resolved unexplained event:
Transient, self-resolving <1 minute event involving cyanosis/pallor, respiratory changes, and unresponsiveness
Must take a BGL!
How to deal with child abuse and neglect as an EMT? What are some signs/symptoms?
Abuse includes physical or emotional injury, negligent treatment, maltreatment, and sexual exploitation: 90% by primary caregiver
Signs/Symptoms:
Passive, withdrawn behavior
Injuries at various stages of healing or in unusual locations
Poor hygiene or nutrition
Drug or Alcohol Abuse
Required to report within 48 hours!
What is gynecology and obstetrics?
Gynecology: Field with medicinal and surgical aspects involving healthcare of female reproductive health
Obstetrics: Focuses on pre-conception, pregancy, and delivery
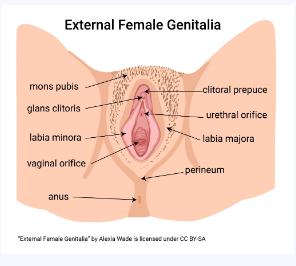
What are some external anatomy of female reproductive organs?
Vulva: Term describing all aspects of female external genitalia
Labia Majora & Minora: Tissue folds surrounding/protecting the vaginal opening
Clitoris: Erectile Organ of female genitalia
Vaginal Opening: Opening to the internal reproductive organs
Urethra: Exit for liquid waste (urinary system exit)
Anus: Exit for solid waste (digestive system exit)
Perineum: Skin between vagina and anus
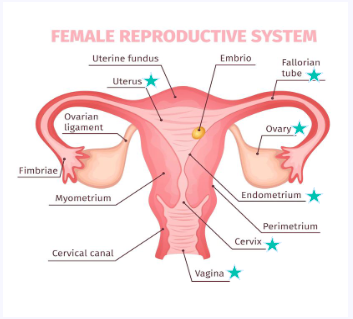
What are some internal anatomy of female reproductive organs?
Vagina: Muscular opening between external genitalia and uterus
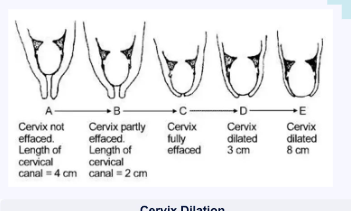
Cervix: Opening of the uterus to the vagina which dilates during labor and menstration
Uterus: Muscular organ that sheds endometrium during menstrual cycle, houses a developing fetus
Endometrium: Inner uterus lining
Ovaries: 2 almond-shaped organs that develop and release ova during ovulation
Ova: Egg, mature female reproductive cell that can give rise to an embryo if fertilized
Fallopian tubes: pair of hollow, muscular ducts serving as passageways for ova between the ovaries and the uterus
What is the menstrual cycle? What are the phases? What hormones control it?
A female hormone cycle that begins on the first day of the period and ends on the day before the next period
Can last between 23-35 days
Consists of four phases:
Menstruation
Follicular phase
Ovulation
Luteal phase
Controlled by estrogen and progesterone hormones
What is menstruation? What are some terms for when women start/stop having periods? What are some S/Sx?
A period that typically lasts 2-7 days (varies per person and cycle).
Occurs when an egg from the previous cycle isn’t fertilized, and the endometrium that had been thickening to prepare for a potential pregnancy is no longer needed
Menarche: When one begins having periods (~12 years)
Menopause: When one stops having periods (~51 years)
S/Sx: Abdominal cramps (from shedding), backaches, headaches, bloating
What are some period products?
Pads: Strips of absorbent material to soak up blood
Liners: Slimmer, neater, and discreet pads, better for lighter flow days or discharge
Tampons: Small, cotton-wool tubes inserted in the vagina to soak up blood, with a string at the bottom to remove them
Menstrual Cups: Insert menstrual cup into the vagina for collection instead of absorption
Menstrual disc: Disc-shaped menstrual cups
Period pants/underwear: Act like pads but are worn and washed like normal pants
What is Toxic-Shock Syndrome? What are some S/Sx?
A rare but life-threatening condition caused by infection, can be caused if a tampon or menstrual cup is left in for too long.
Tampons should only be left in for 4-8 hours
S/sx: Sudden high fever, low bp (vasodilation), vomiting or diarrhea, confusion, muscle aches, seizures
What are the common types of birth control?
Birth Control Pill: Daily pill taken
IUD (Intrauterine device): A copper, T-shaped object placed inside uterus (lethal to sperm)
Contraceptive injection: Injection every three months, suppressing ovulation and thickens cervical mucus
Implant: A tiny, thin rod around size of matchstick, inserted under skin of upper arm, releasing progestin
Reasons for birth control?
Preventing preganncy
Regulating menstrual cycle
Lightening periods and reducing menstrual cramps
What are some female reproductive disorders? (part 1)
Amenorrhea: Absence of period (not by pregnancy)
Menorrhagia: Heavy/prolonged bleeding during period
Urinary Tract Infection: Infection of urinary tract from bacteria entering urethra, common in women
S/Sx: painful urination, cloudy urine with foul smell, lower back pain
STIs/STDs: Sexually transmitted disease (chlamydia, gonorrhea, herpes)
S/Sx: Itching, burning, Painful urination, painful intercourse, foul-smelling discharge
Yeast Infection: Fungal infection of vulva and vagina caused by environmental changes
Sx: itching, burning, thick white “cottage cheese” discharge
Endometriosis: Disease in which tissue similar to the lining of uterus grows outside uterus, causing severe pelvic pain and difficulty getting pregnant
What are some female reproductive disorders? (part 2)
Polycystic ovary syndrome: Hormone imbalance causing one to have many eggs that don’t or rarely mature
S/Sx: irregular period, hirsutism, weight gain
Pelvic Inflammatory Disease: When untreated sexually transmitted bacteria spread from vagina to womb, fallopian tubes, or ovaries
S/Sx: lower abdominal pain, foul-smelling discharge, painful intercourse, shuffling gait
Ovarian Cyst: Fluid-filled sac in ovary, caused by unregulated hormones or as a symptom of something more serious. Often asymptomatic or pain on one side, can go away, but bursting can cause sepsis
Assault: Can happen to anyone, have a female crew member take lead if possible, preserve evidence and crime scene, request SAFE/SANE nurse
General Vaginal Bleeding: Multiple causes, assess circulation and treat for shock, active bleeding can be treated with a pad, let the patient do it themselves if they can
Vocabulary for pregnancy
Placenta: Source of nutrients for growing baby
Umbilical cord: Connects mom to baby through placenta
Amniotic sac: Insulates and protects baby
Full Term: 38-40 weeks gestation
Premature: <38 weeks gestation
Postmature: >42 weeks gestation
Trimester: Classifying pregnancy stages
Neonate: Infant <28 days old
Gravida: Number of times patient has been pregnant (ASK)
Para: Number of patient’s live births (ASK)
Abortus: Number of miscarriages, abortions, and stillbirths (ASK)
What are some body changes during pregnancy?
Increased blood volume (up to 50%) in mother by end of term, increases anemic risk and higher HR
Uterus grows with fetus, exposing fetus to injury and displaces the organs and balance disruption
Displaced organs place diaphragm pressure, increased respiratory rate and shallow respirations
Higher chance of vomiting due to trauma and aspiration
Increased hormone levels
Looser ligaments to prepare for birth
What are some pregnancy complications? (Pt 1)
Ectopic Pregnancy: Pregnancy that develops outside the uterus, will eventually rupture, causing internal bleeding
Must be treated by termination of pregnancy
S/Sx: Sudden, sharp, one-sided abdominal pain, vaginal bleeding, signs of shock, proteinuria
Preeclampsia: High BP during pregnancy
S/Sx: headache, hypertension, peripheral edema
Eclampsia: Preeclampsia + seizure activity
Treatment: Lay patient on left side, provide O2, maintain ABCs, rapid transport, ALS
Miscarriage: Spontaneous abortion occurring within the first 20 weeks
Stillbirth: Fetal death after 20 weeks of pregnancy, very rare
Abruptio placenta: Placenta separates from uterus prematurely
S/Sx: Port win vaginal bleeding, shock, abdominal pain, contractions
What are some pregnancy complications? (Pt 2)
Placenta previa: Placenta develops over cervix
S/Sx: Bright red vaginal bleeding, shock, painless
Gestational Diabetes: New diabetes developing pregannt person
Raises risk of Type II developing in mother and child
Extra glucose from mom passes in placenta, causing fetus to make extra insulin → fat baby, need C section
Treatment: Treat patients the same as non-pregnant
Supine Hypotension Syndrome: If patient is lying supine, their descending aorta and inferior vena cava become compressed
S/Sx: Hypotension and dizziness
PROM: Premature rupture of membrane:
Occurs before 37 weeks of gestation
Increased infection risk
Trauma: Have high index of shock suspicion in all cases of trauma involving pregnant woman, treat for shock
What are the stages of labor?
Onset to dilation
rupturing of amniotic sac and onset of contractions until full dilation achieved
Dilation to baby delivery
From the time of full dilation to delivery of baby
Baby to placenta delivery
From time baby was delivered until placenta was delivered
What is the APGAR Scoring System? What is the range of a heathy baby and when should it be taken?
Activity (muscle Tone):
Absent: 0 points
Flexed Limbs: 1 point
Active: 2 points
Pulse:
Absent: 0 points
<100 BPM: 1 point
>100 BPM: 2 points
Grimace (reflex irritability)
Floppy: 0 points
Minimal stimulation response: 1 point
Prompt response to stimulation: 2 points
Appearance:
Pale/blue: 0 points
Pink body, blue extremities: 1 point
Pink: 2 points
Respiration:
Absent: 0 points
Slow and irregular: 1 point
Vigorous cry: 2 points
Should be taken after birth and 5 minutes after
Healthy range: 7-10
What are some neonatal reflexes?
Rooting: Stroke baby cheek, should turn to finger
Moro: If baby feels like it’s falling, it will spread out its arms
Walking: Baby will try to “walk” when feet touch flat surface
Sucking: Baby begins to suck when roof of mouth is touched
Palmar: Baby will grab anything touching the palm.
Delivery Complications
Breech: Baby hips come out before head
Footling Breech: Feet come out first
Prolapsed Umbilical Cord: UC coming out first
Shoulder Dystocia: Shoulders get stuck behind pelvis
Nuchal Cord: Umbilical cord wrapped around the baby’s neck
What is a tracheostomy? What is it also known as?
A surgical opening in the neck to secure ventilation and airway, also known as a stoma
What is a colostomy bag?
Medical device used to collect stool from a hole made in an abdomen
What is a gastrostomy tube?
Tube inserted directly in abdomen to directly deliver food, nutrients, medications, or fluids.
What is an indwelling catheter? What is it also known as?
A flexible tube inserted in the urethra to drain urine. Also known as a foley catheter.