Microscopic Examination of Urine
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
43 Terms
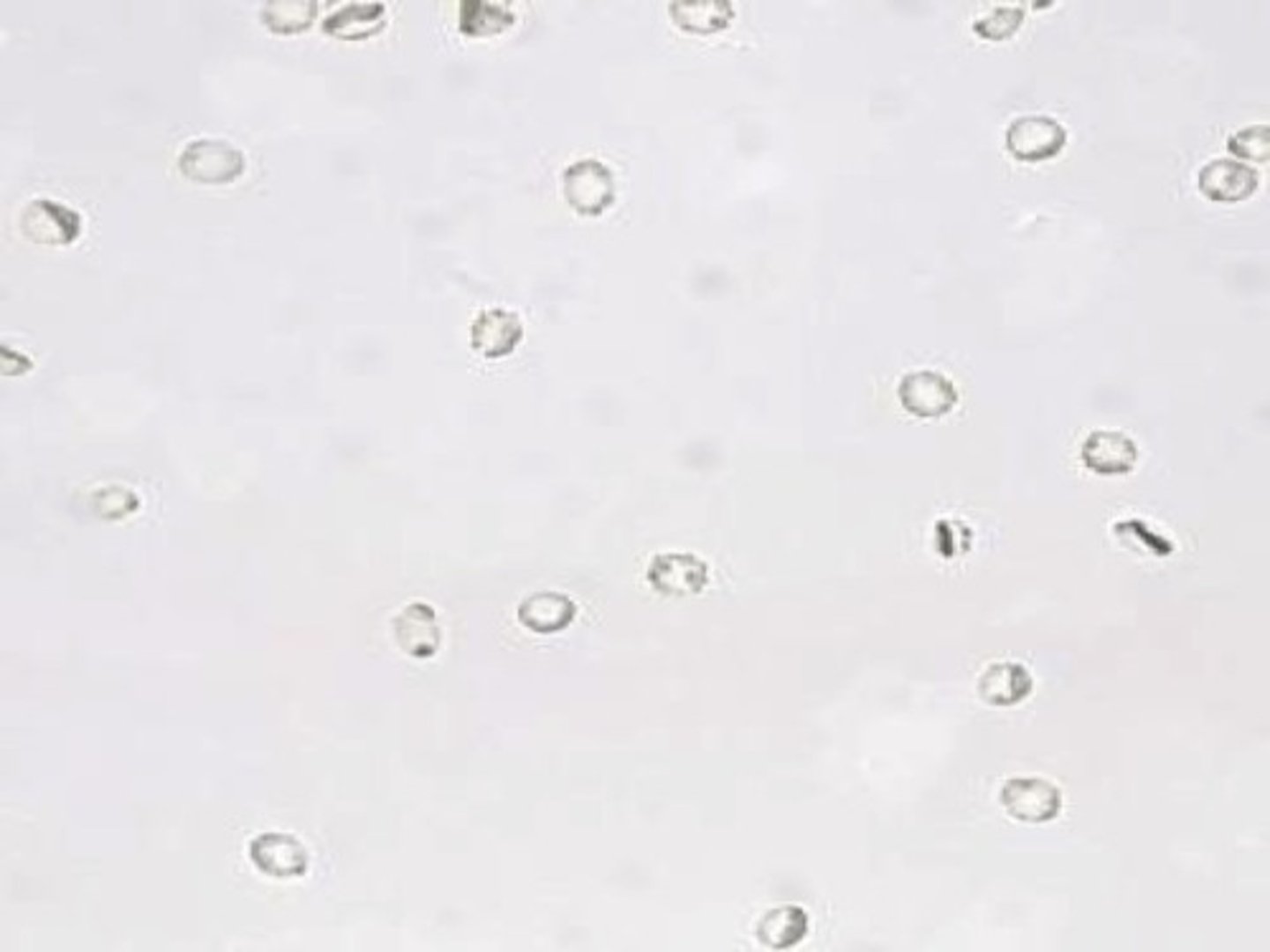
Red Blood Cells
Appear as smooth, non-nucleated, biconcave disks measuring approximately 7mm in diameter
- In concentrated urine they may appear CRENATED; or irregularly shaped
- In dilute urine, they may swell and burst leaving only the cell membrane behind, these are known as GHOST CELLS
- They also may just be dysmorphic in size, have cellular protrusions and are fragmented due to certain diseases
DO NOT: confuse with yeast cells (budding), oil droplets/air bubbles (which are refractile in the light)
Clinical Significance:
- Associated with damage to the glomerular membrane or vascular injury within the genitourinary tract
- Also can be seen following strenuous exercise and menstruation
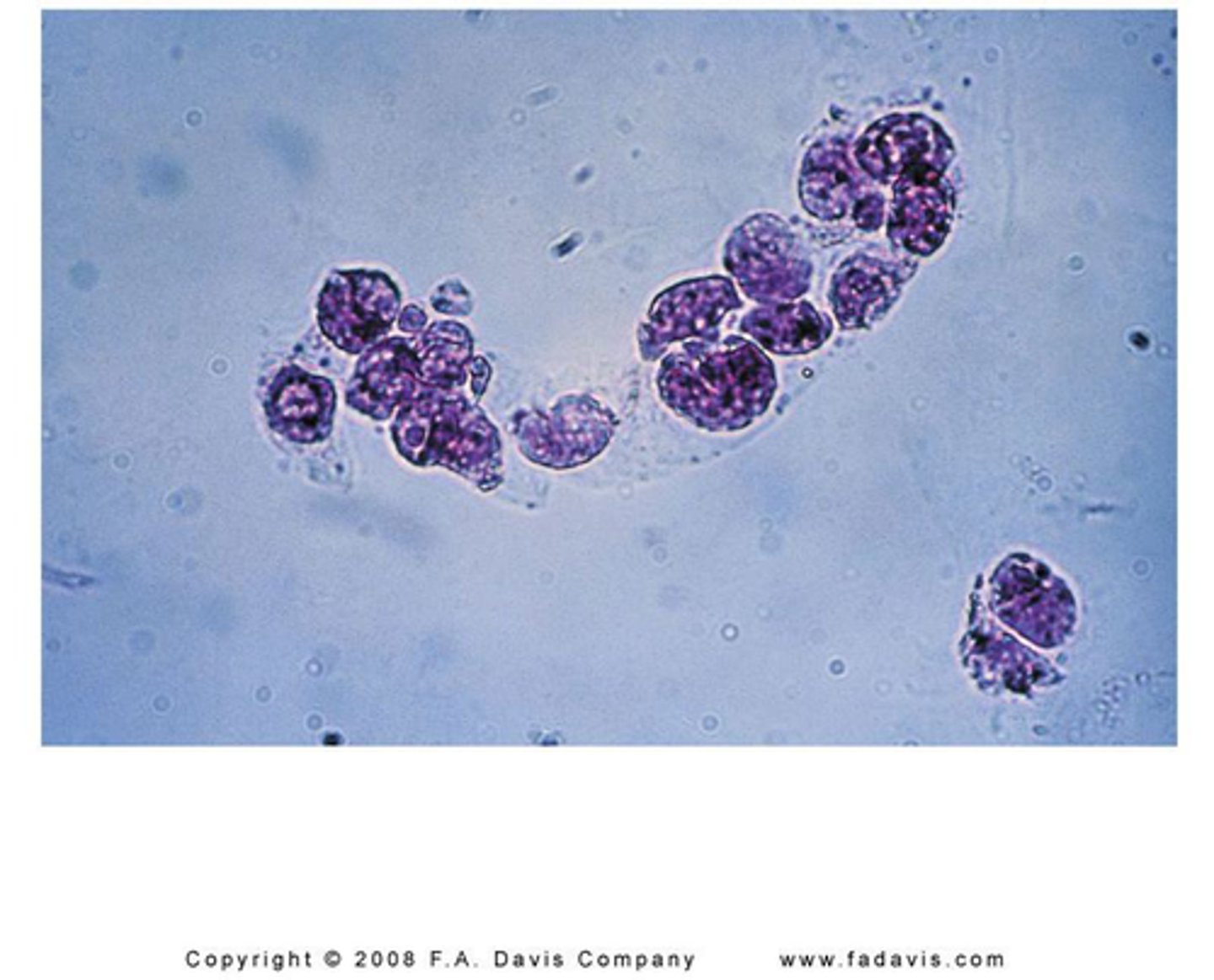
White Blood Cells
Appear as either neutrophils, eosinophils or mononuclear cells
- Neutrophils: contain granules and multi-lobed nuclei. If Brownian movement is observed due to swelled cells, then the granules appear to sparkle "glitter cells"
- Eosinophils: Is primarily associated with drug-induced interstitial nephritis. Small numbers may also be seen in UTIs and renal transplant rejection.
Since they are not normally seen, the finding of more than 1% Eos is considered clinically significant
- Mononuclear Cells: Lymphs, Monos, Macrophages. Lymphs are very small and can be confused with RBCs, Monos and Macrophages are usually large cells that may appear vacuolated or contain inclusions. They need to be differentiated from RTE cells, which are usually larger, with a eccentrically located nucleus
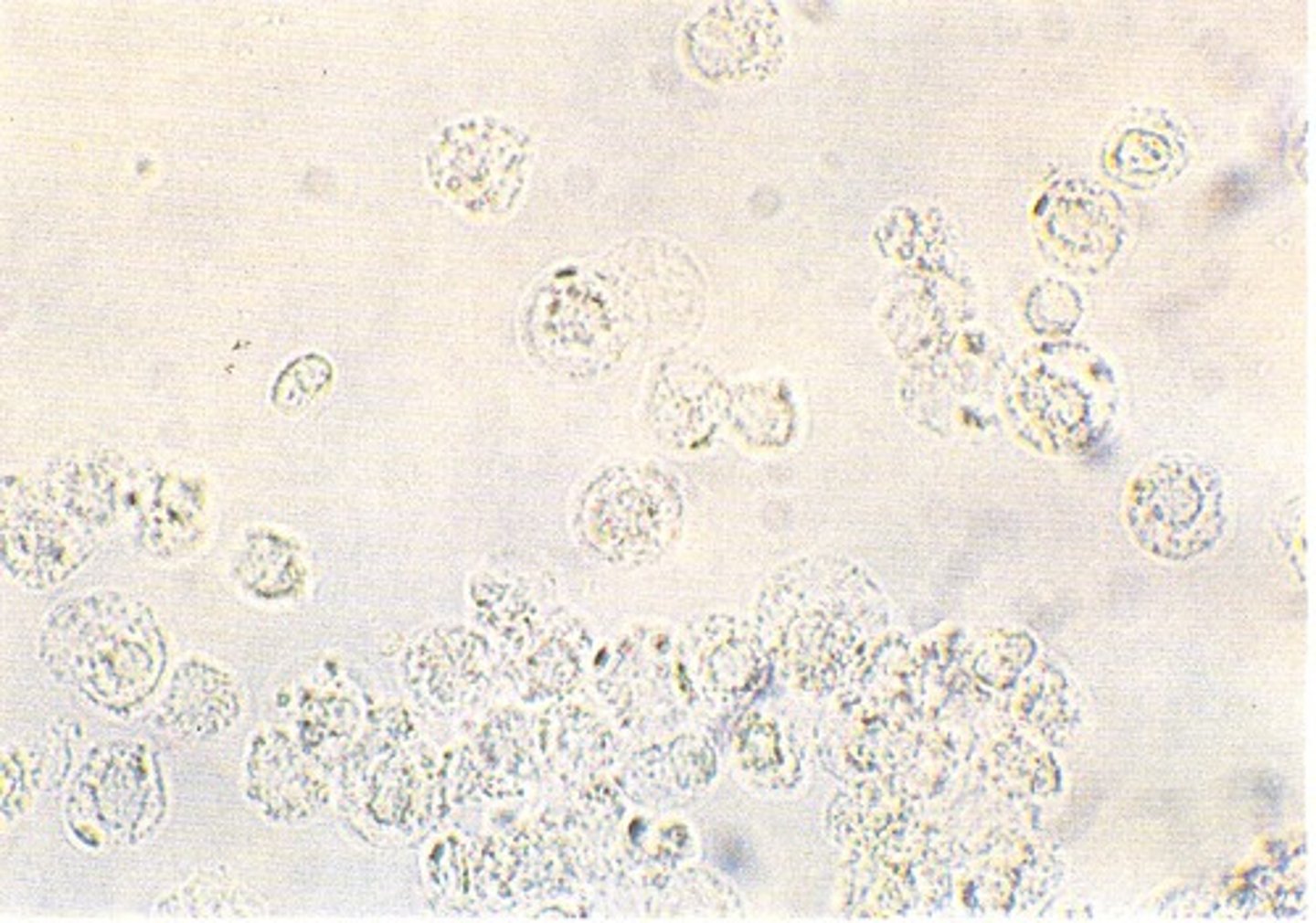
Pyuria
An increase in urinary WBCs and indicates the presence of an infection or inflammation in the genitourinary system.
EX: pyelonephritis, cystitis, prostatitis and urethritis
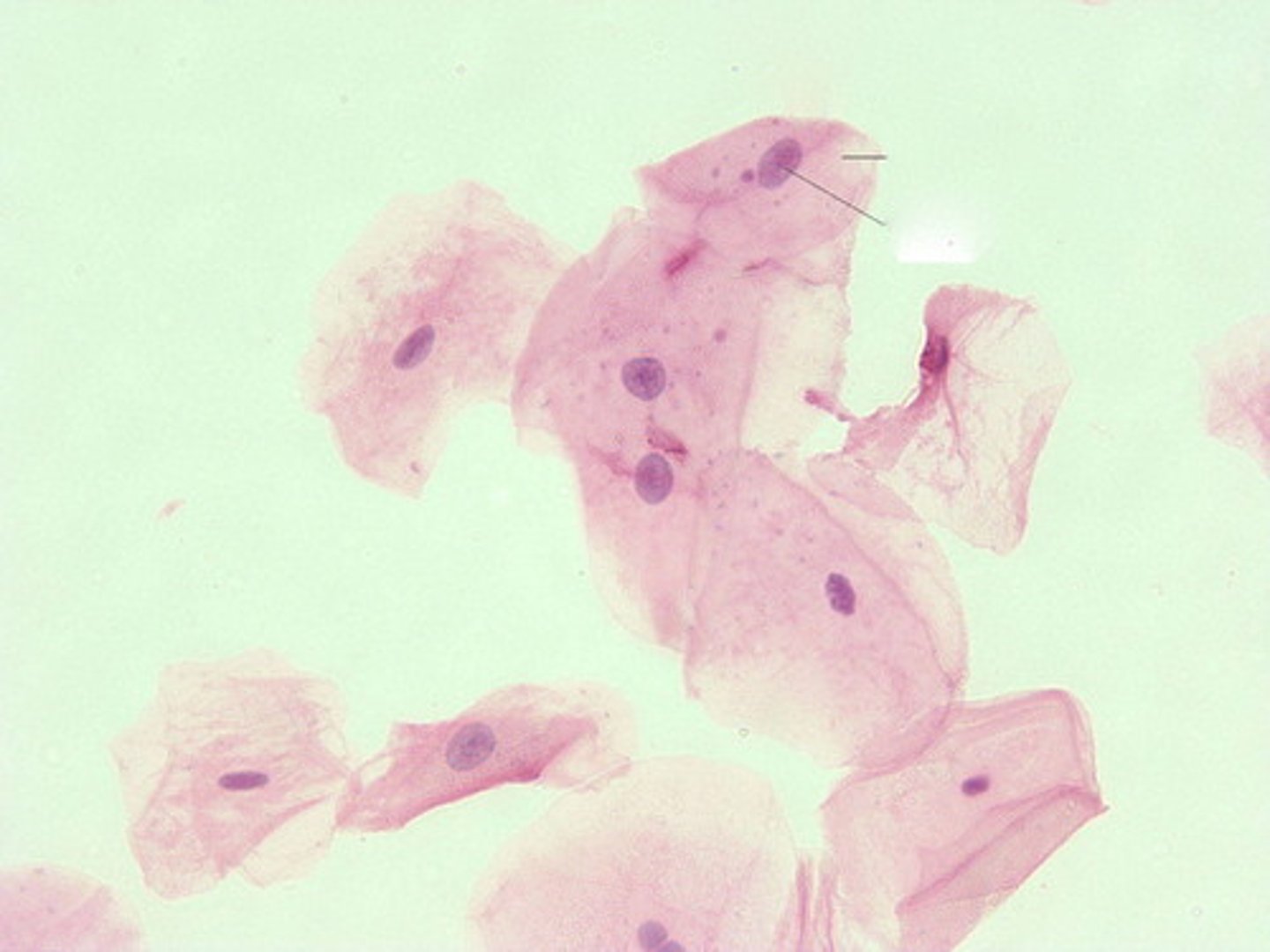
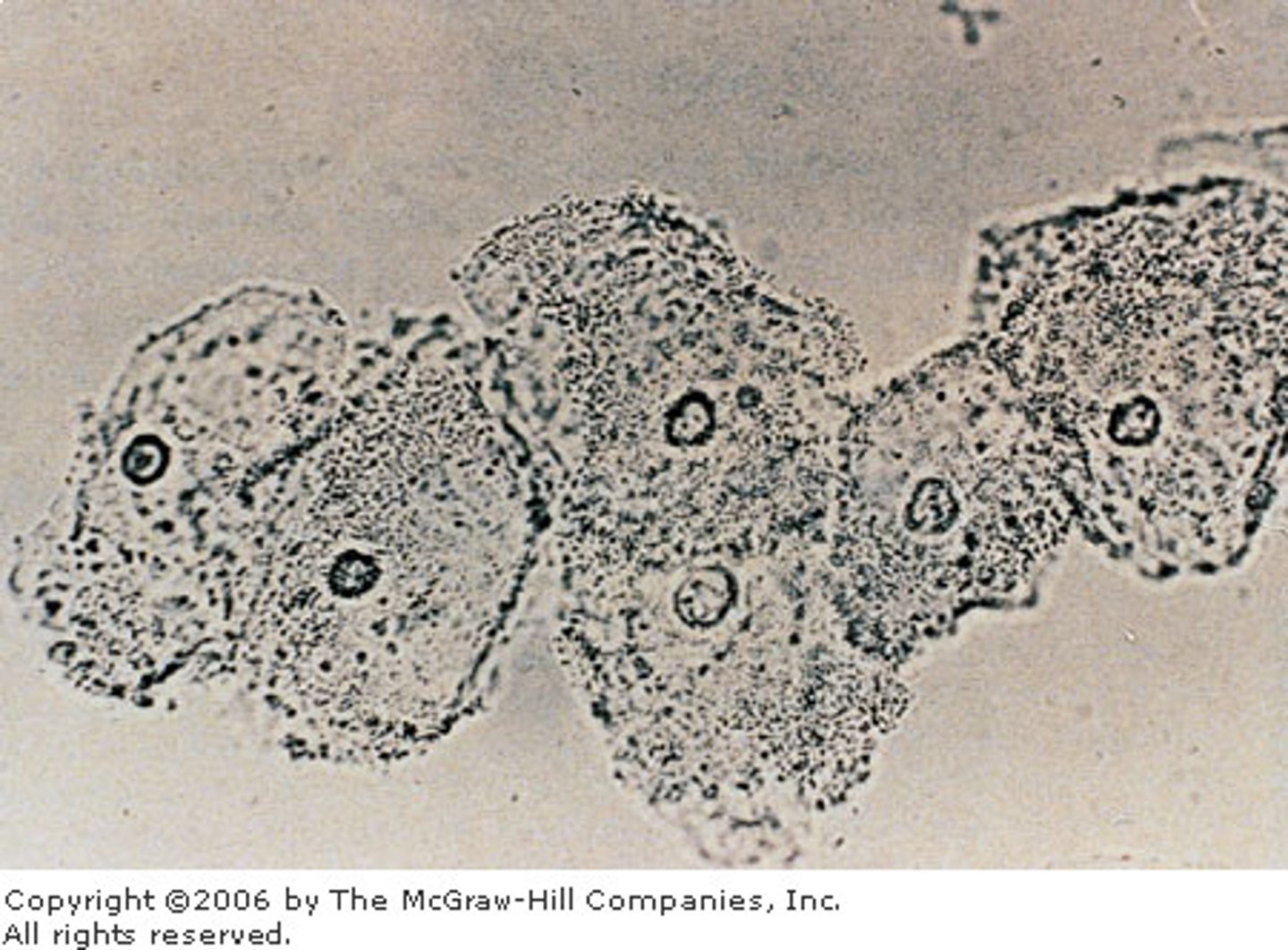
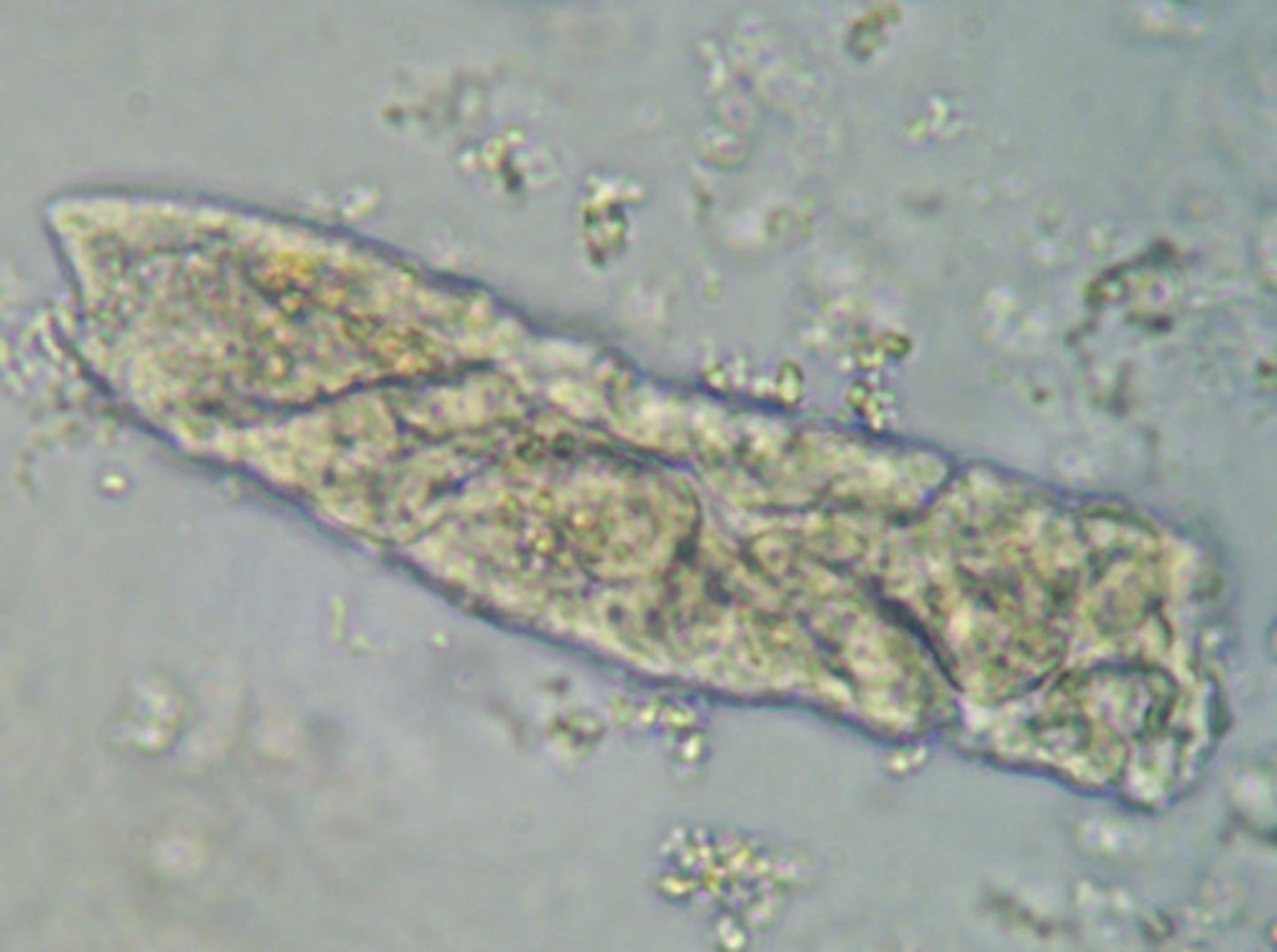
Squamous Epithelial Cells
They are the largest cells that appear in the sediment and contain abundant, irregular cytoplasm and a prominent nucleus about the size of an RBC. They could also be folded, resembling a cast, BUT a cast would NOT have a nucleus present
- They originate from the linings of the vagina and female urethra and the lower portion of the male urethra
Clinical Significance: They are normal cells that are seen in the urine and have NO significance.
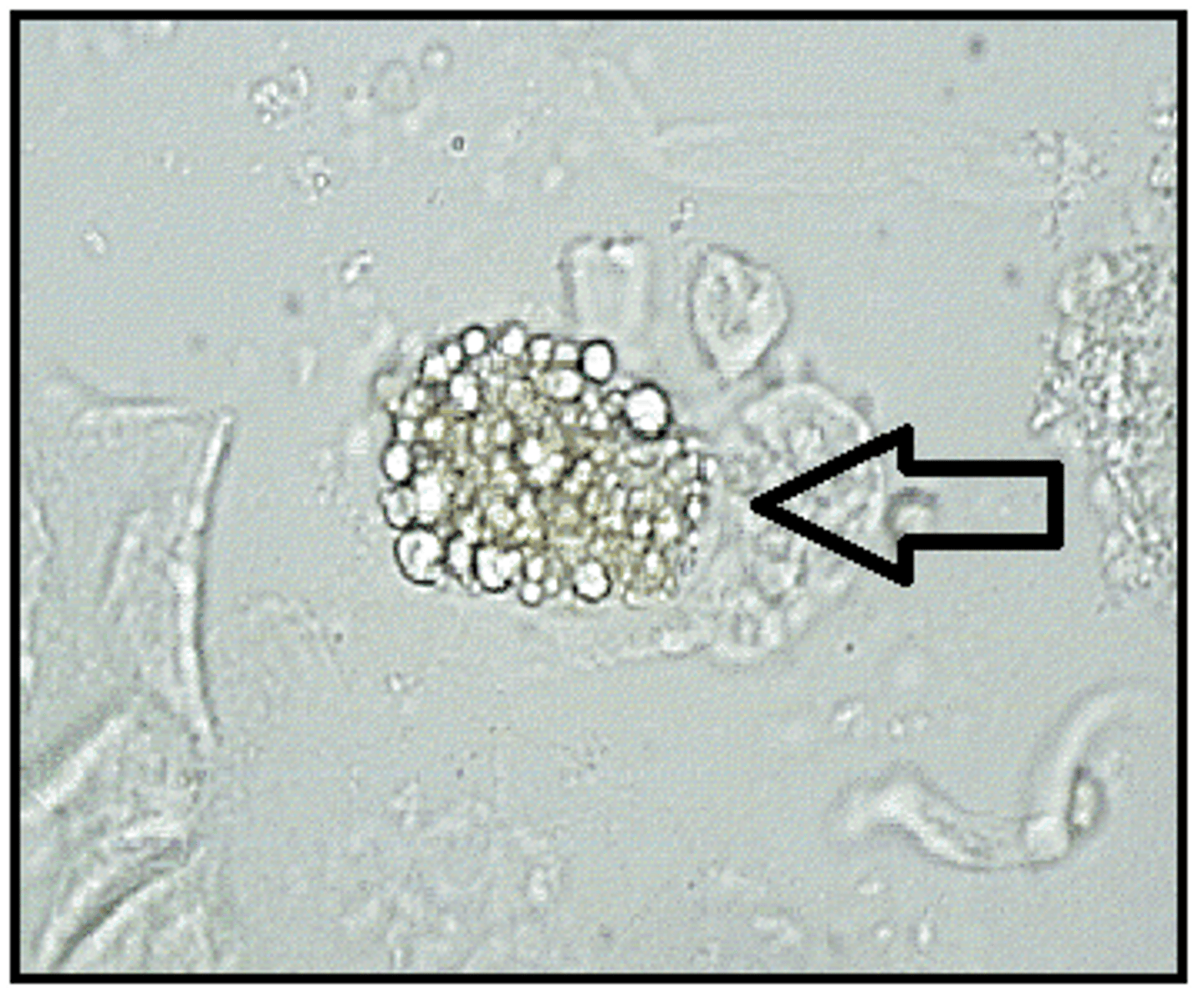
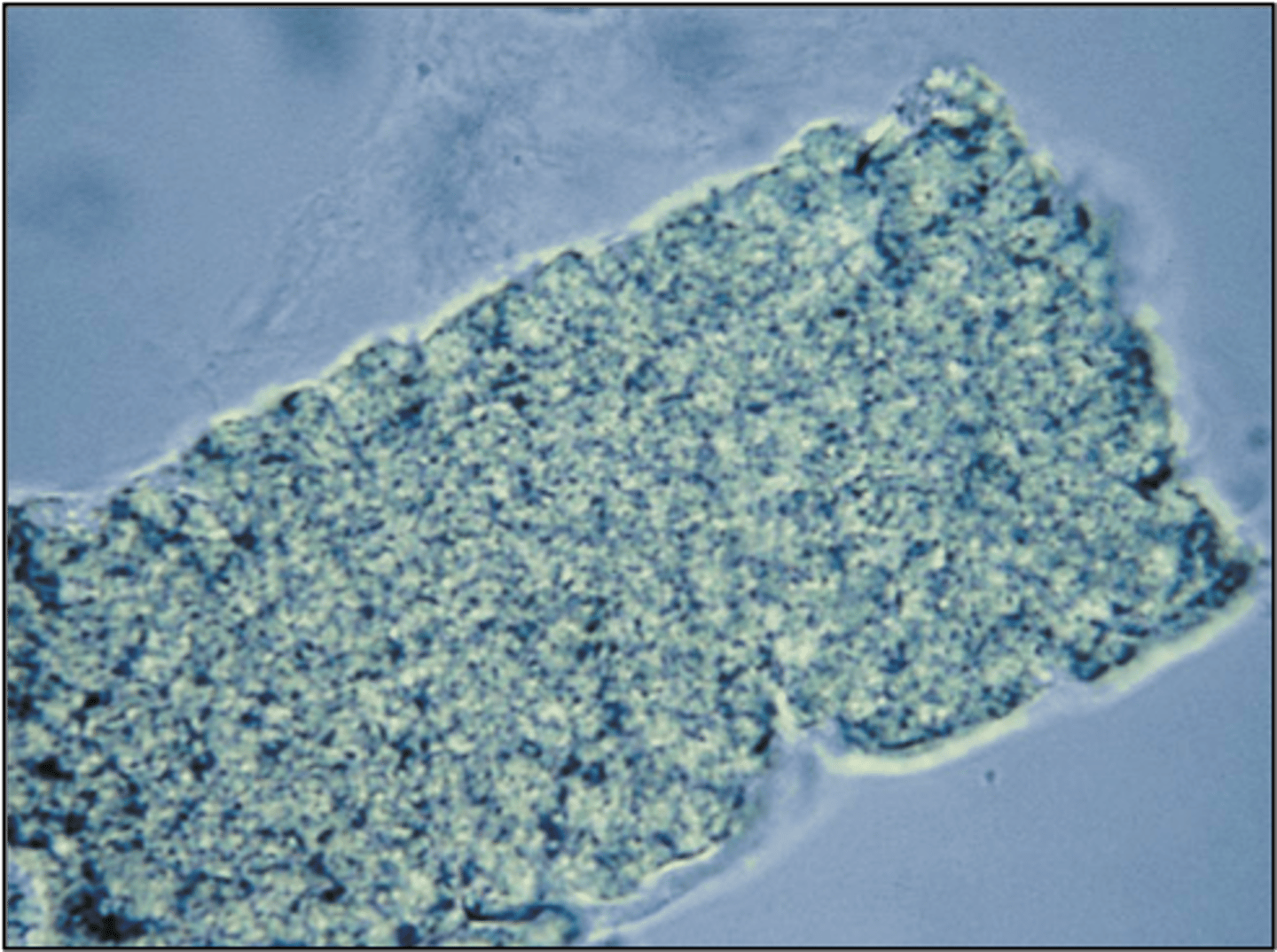
Clue Cells
Are a variation of squamous epithelial cells that ARE of clinical significance
- They are indicative of a vaginal infection from Gardnerella vaginalis
- They appear as squamous cells covered with the Gardnerella coccobacillus bacteria. This gives the cell a granular/irregular appearance
Transitional Epithelial (Urothelial) Cells
They are smaller than their squamous counterparts and can be either spherical, polyhedral and caudate
- The change in size is due to the amount of water that is absorbed by the cells. The more water the more spherical they look. They have a very large CENTRALLY located nuclei.
- Increased number of transitional cells (singly or in pairs/clumps) is called SYNCYTIA and is present following invasive urologic procedures such as catheterization and are of NO clinical significance
- Abnormal morphology (vacuoles and irregular nuclei) indicate malignancy or viral infection

Renal Tubular Epithelial Cells (RTE)
These cells differ in size depending on the area that they originated from. They can also absorb things like bilirubin and turn yellow or contain hemosiderin granules from iron breakdown.
- Most have coarsely granular cytoplasm and often resemble casts (but casts would NOT contain a nucleus)
- PCT: are larger and tend to have a rectangular shape (columnar or convoluted cells)
- DCT: are smaller and are round/oval in shape and can be confused with transitional epithelial cells. BUT transitional cells have a centrally located nuclei where as RTE cells have an eccentrically located nuclei
Clinical Significance: Increased presence is indicative of necrosis of the renal tubules, with the possibility of affecting overall renal functions.
- Due to: exposure to heavy metals, drug-induced toxicity, hemoglobin/myoglobin toxicity, viral infections, pyelonephritis, malignant infiltrations or transplant rejections
Oval Fat Bodies
RTE cells that have absorbed lipids that were present in the glomerular filtrate. They appear as highly refractile and the nucleus may be more difficult to observe. Usually seen in the conjunction of free-floating fat bodies.
- Lipiduria: is most often associated with damage to the glomerulus caused by the nephrotic syndrome that is present. Also seen in diabetes mellitus, severe tubular necrosis, and in trauma cases that cause release of BM fat from the long bones.
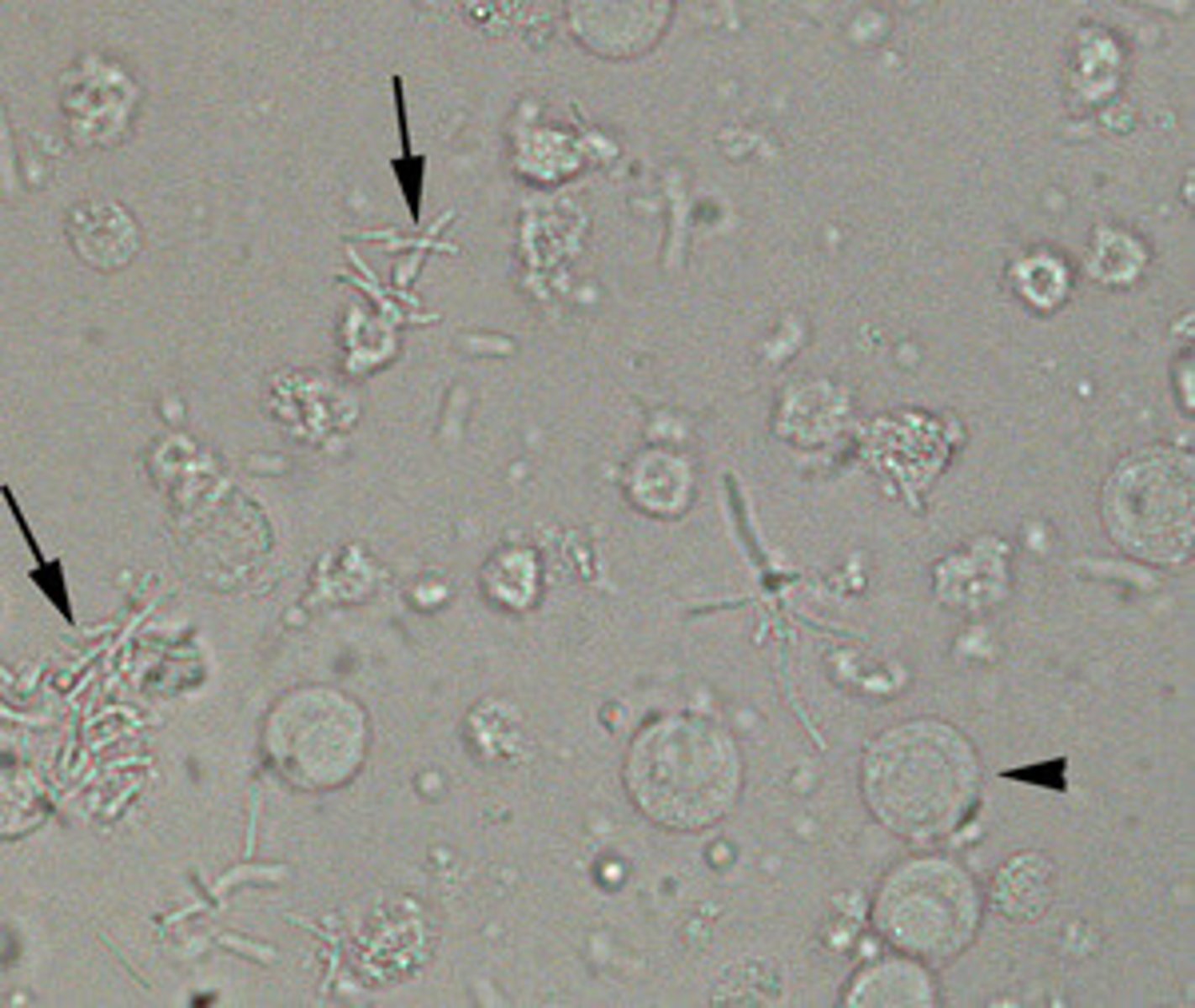
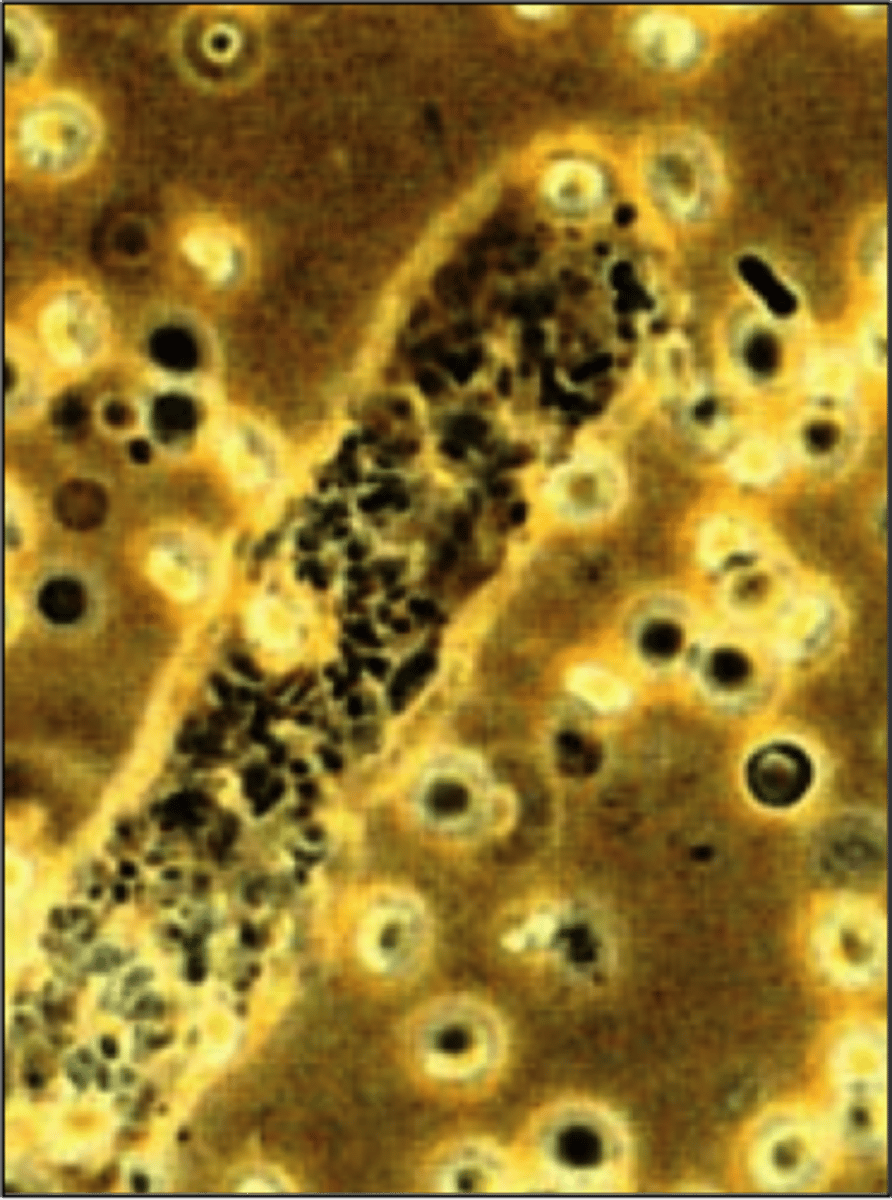
Bacteria
Bacteria are normally not present in the urine, but a few can occur as result of vaginal, urethral or external genitalia contamination of the collection container.
- To be clinically significant for a UTI the bacteria MUST be accompanied by WBCs.
- Observing them for motility is also a good way to distinguish them from other amorphous phosphates and urates.
UTIs: Most frequent culprits
- Enterobacteriaceae (gram-negative rods)
- Staphylococcus and Enterococcus are also possible but less likely
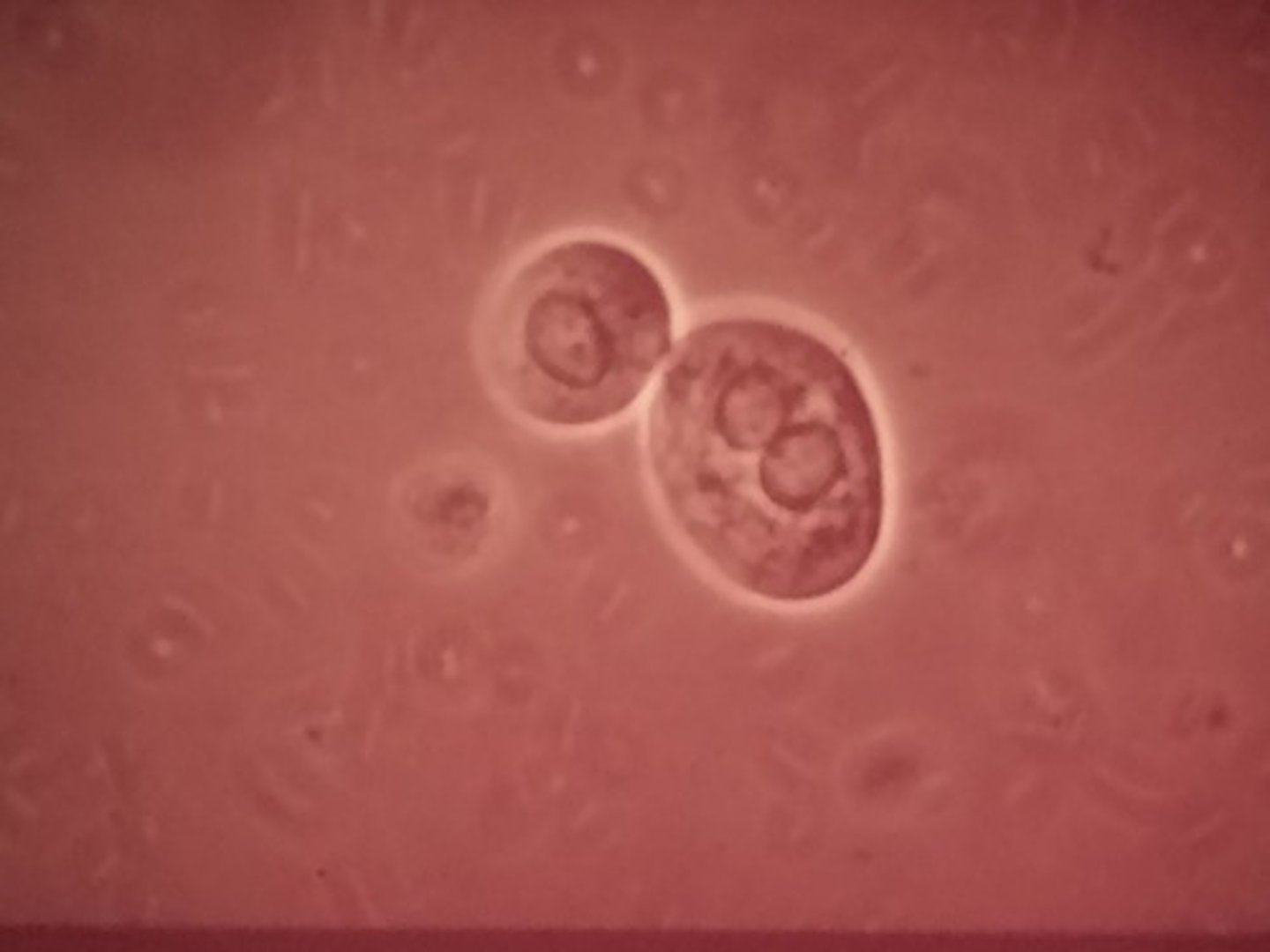
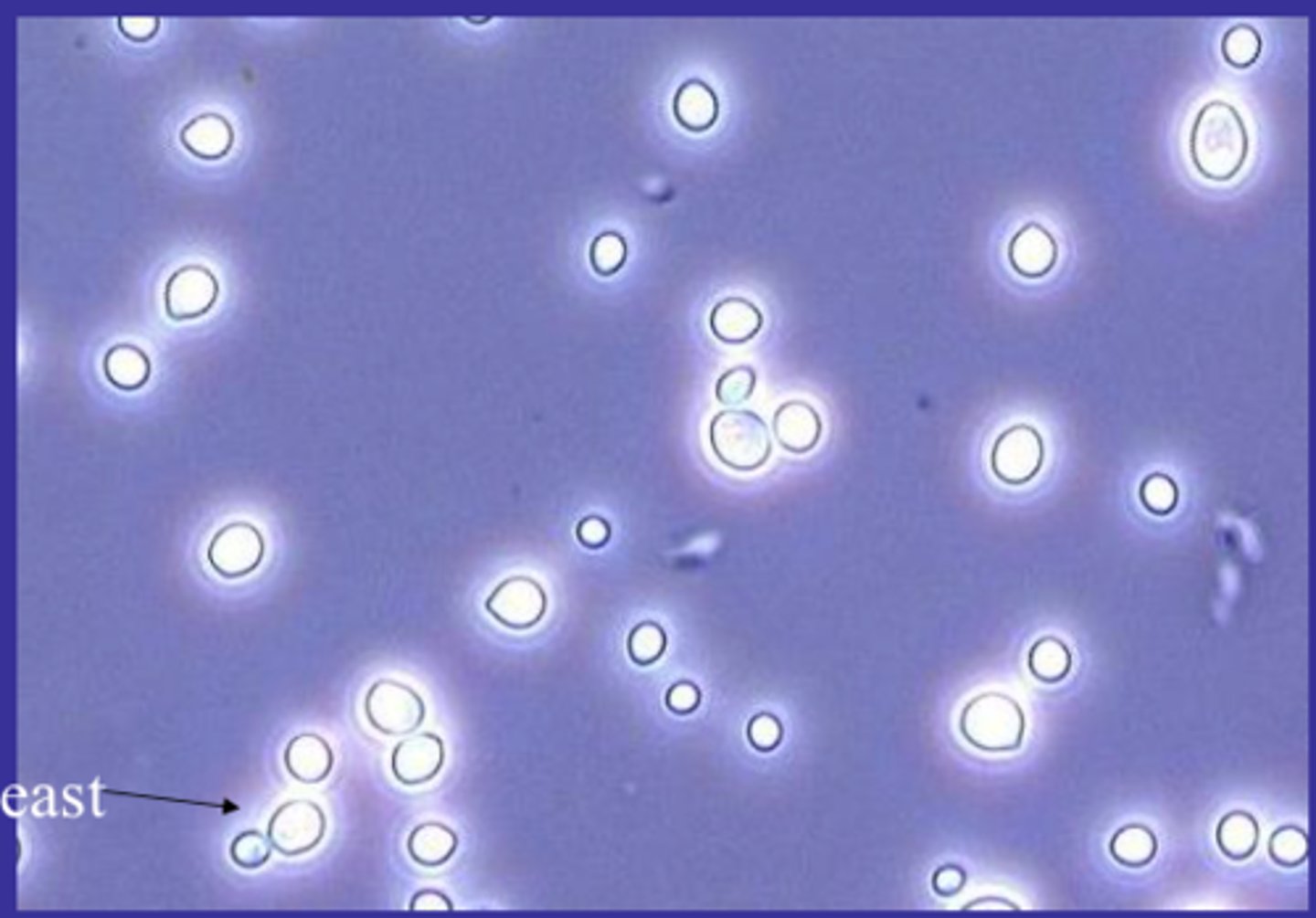
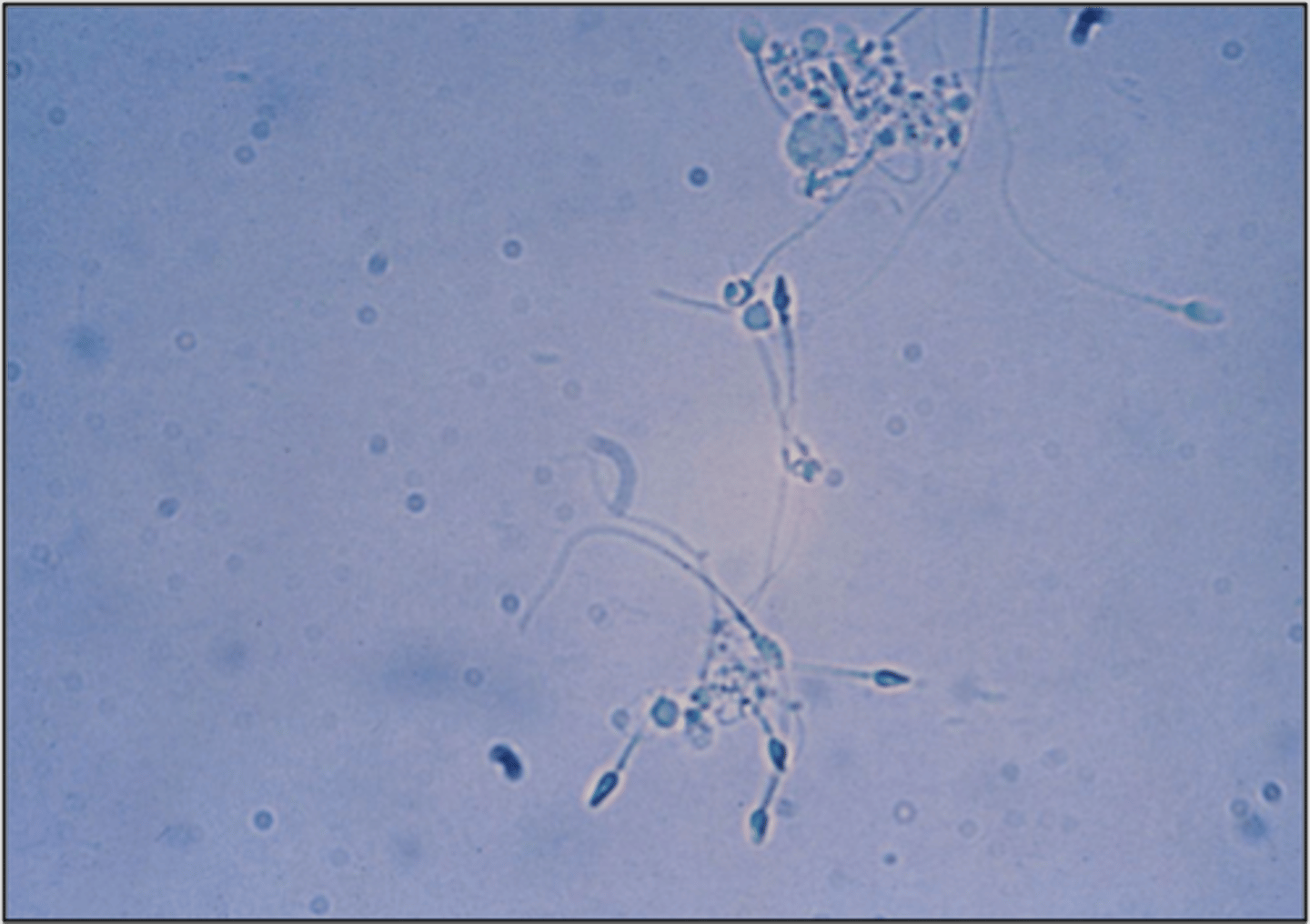
Yeast
They appear as small, refractile oval structures that may or may not contain a bud. (Budding is the best way to confirm in a specimen though). In severe infections they may as appear as branched mycelial forms
- Primarily Candida albicans, seen in the urine of diabetic patients, immunocompromised or women with vaginal moniliasis
- A true yeast infection SHOULD be accompanied by WBCs
Parasites
- MOST FREQUENTLY encountered would be that of Trichomonas vaginalis, which is a pear shaped flagellate with an undulating membrane. It has rapid movement under a wet-prep and is easy to identify
- Causes: vaginal inflammation in women and is asymptomatic in males
- Another possible parasite is the Ova of the Schistosoma haematobium will appear in the urine as part of its naturally life-cycle within the host.
- If there is fecal contamination then you can also have parasites that are in the intestinal tract. Biggest one is the Ova from the pinworm Enterobius vermicularis
Spermatozoa
Oval, slightly tapered heads and long, flagella-like tails.
- Rarely exhibit motility because urine is toxic to sperm and kill it almost instantly
-Rarely of clinical significance, except in the cases of male infertility or retrograde ejaculation in which the sperm expel into the bladder instead of the urethra
Mucus
Is a protein material produced by the glands and epithelial cells of the lower genitourinary tract and RTE cells. It is made up of Uromodulin (Tamm-Horsefall protein).
- It has an irregular and string-like appearance in the sample
- It has no clinical significance ever in either males or females
- It is just an irritant to have in the sample

Casts
Are the only elements found in the urinary sediment that are unique to the kidneys. They are formed within the lumens of the DCT and collecting ducts, providing a microscopic view of conditions within the nephron.
Hyaline Casts
Are the most frequently seen casts and are made up almost entirely of uromodulin. The presence of 0-2/lpf is considered a normal finding.
Increased numbers can be from
- Strenuous exercise
- Dehydration
- Heat exposure
- Emotional Stress
- Acute Glomerulonephritis
- Pyelonephritis
- Chronic renal disease
- Congestive Heart Failure
They appear color-less and have the same refractile as the urine itself making them very easy to overlook in the sediment. They consist of parallel sides with rounded edges, as it degrades though it does become wrinkled. They also can contain some granules as well.

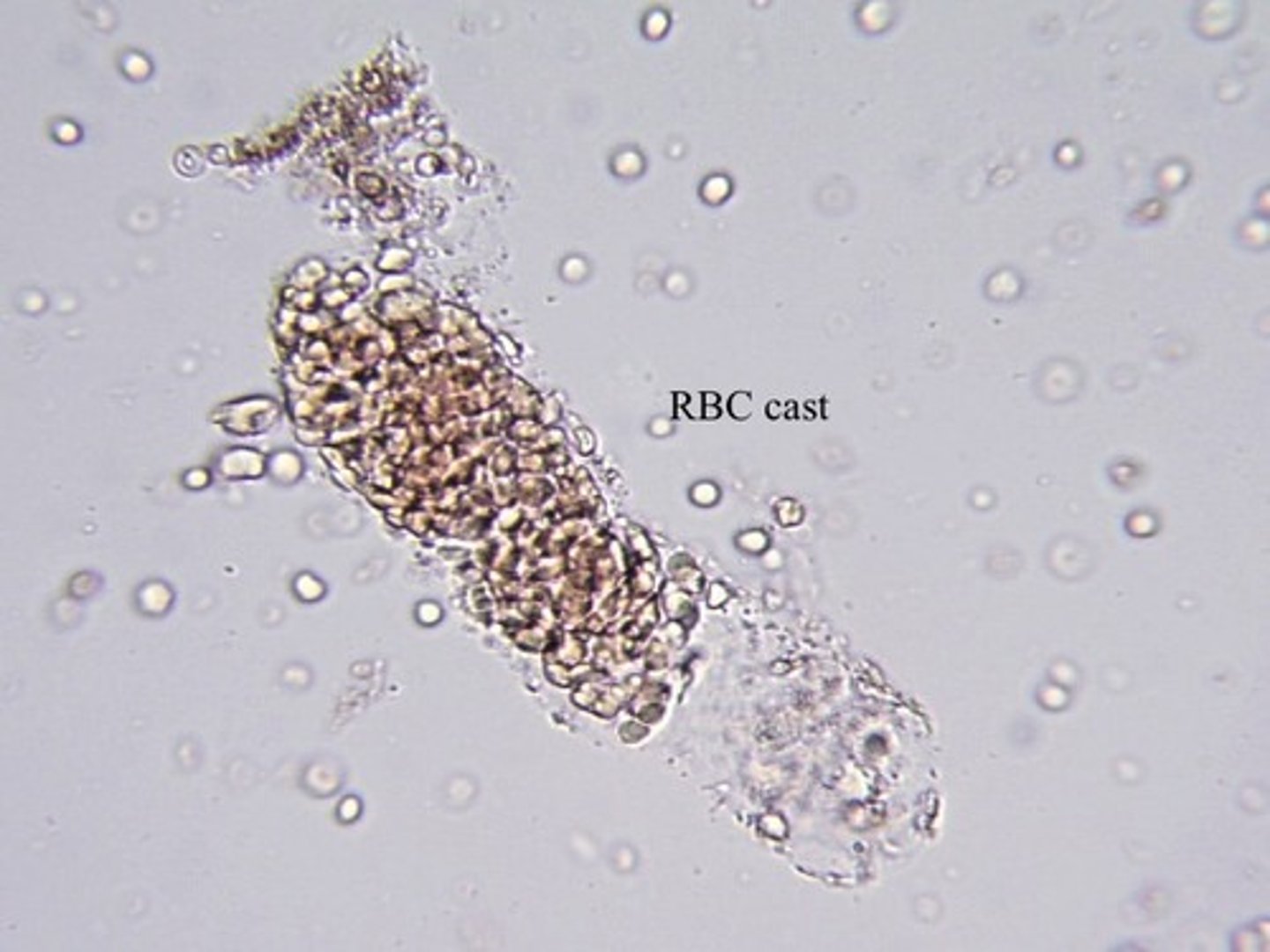
RBC Casts
The presence of RBC casts shows that there is bleeding within the nephron. Primarily associated with damage to the glomerulus or to the nephron capillary structure
- It will be accompanied by proteinuria and dysmorphic erythrocytes
- Usually under low power they have a red-orange color and they may also exist as fragments as a result of tightly packing to the protein membrane
- As it ages the RBCs begin to lyse and they develop a more homogenous appearance
- Massive hemoglobinuria or myoglobinuria can cause dirty, brown, granular casts to occur as it converts to methemoglobin in its breakdown.
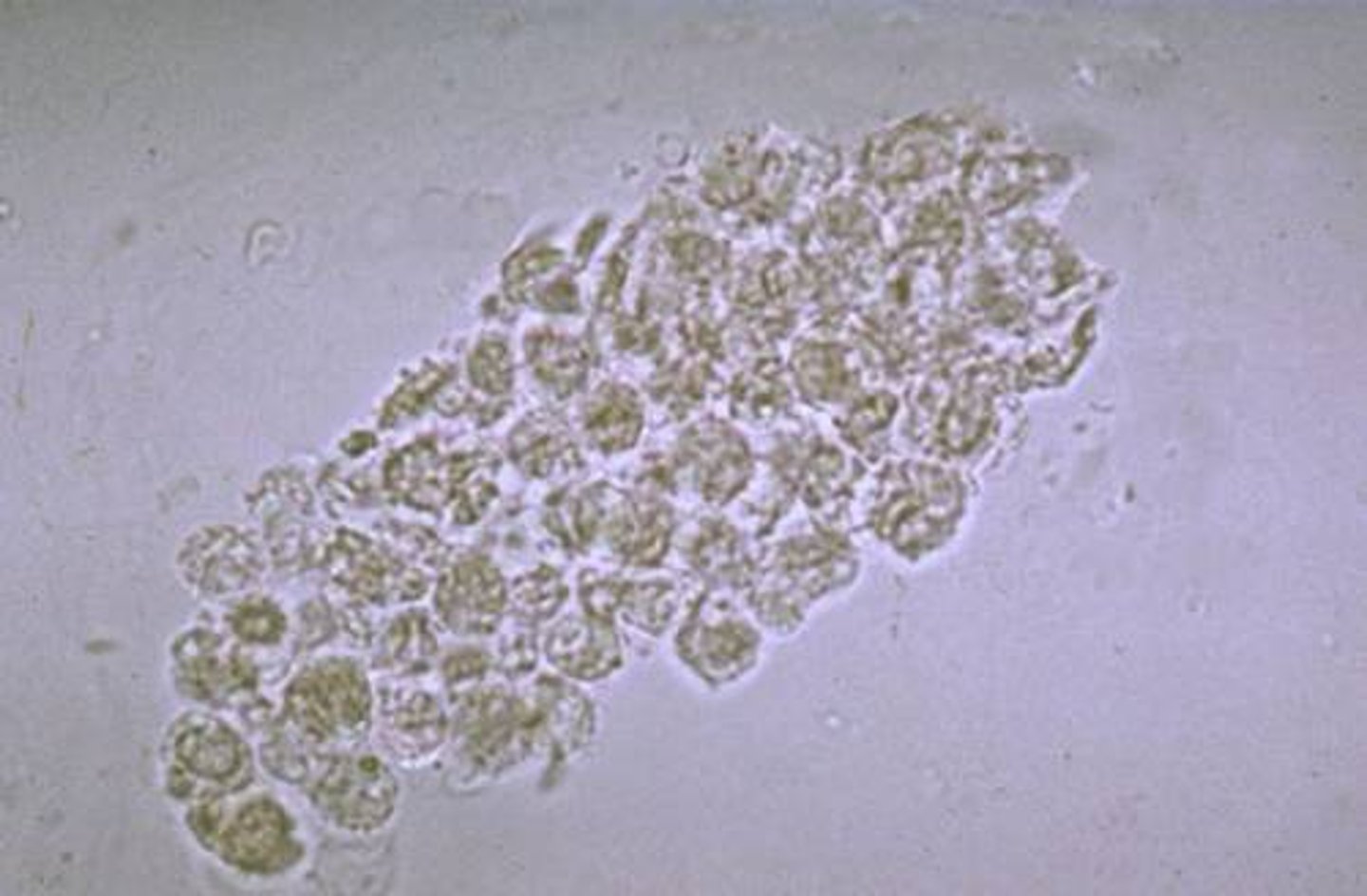
WBC Casts
Signifies infection or inflammation within the nephron. Most frequently seen with pyelonephritis and are primary markers for distinguishing pyelonephritis from cystitis.
Most casts consist of neutrophils, therefore they appear granular and unless disintegration has occurred, multi-lobed nuclei will be present
Will have irregular boarders and need to be observed for the cast matrix
Bacterial Casts
They contain both bacilli within and bound to the outside of the cast. This is sen in pyelonephritis.
There presence should be considered when WBC casts and may free WBCs and bacteria are seen in the sediment.
Epithelial Cell Casts
Casts that contain RTE cells represent the presence of advanced tubular destruction, producing urinary stasis along with disruption of the tubular linings.
- Associated with heavy metal and chemical or drug-induced toxicity along with viral infections and allograft rejection.
Fatty Casts
Are seen in conjunction with oval fat bodies and free fat droplets in disorders causing lipiduria.
- Examples: nephrotic syndrome, toxic tubular necrosis, diabetes mellitus or crush injuries
- They are highly refractile under bright-field microscopy.
- The matrix may contain attached fat droplets or oval fat cells on the outside

Mixed Cellular Casts
Where there is more than one element making up the cast. This can make it extremely hard to differentiate which is causing the issue
MOST CLINICALLY SIGNIFICANT:
1. RBC/WBC in glomerulonephritis
2. WBC/RTE or WBC/Bacteria in pyelonephritis
Granular Casts
Come in two forms, coarse and fine granules
- Non-pathogenic occurrences, the granules are formed from lysosomes excreted by the RTE cells during normal metabolism. This could be due to strenuous exercise.
- Pathogenic occurrences, are a result of cellular disintegration. So you may be able to see a recognizable cell.

Waxy Casts
Are representative of extreme urine stasis indicating chronic renal failure
- They have a brittle and highly refractile cast matrix
- They often appear fragmented with jagged ends and have notches on their sides
Broad Casts
Can occur to any cell type and mean that the cast broadens width wise to be larger than normally expected.
- Usually indicates renal failure and extreme urinary stasis
- Indicates the widening of the tubular walls
- Most commonly seen are granular and waxy
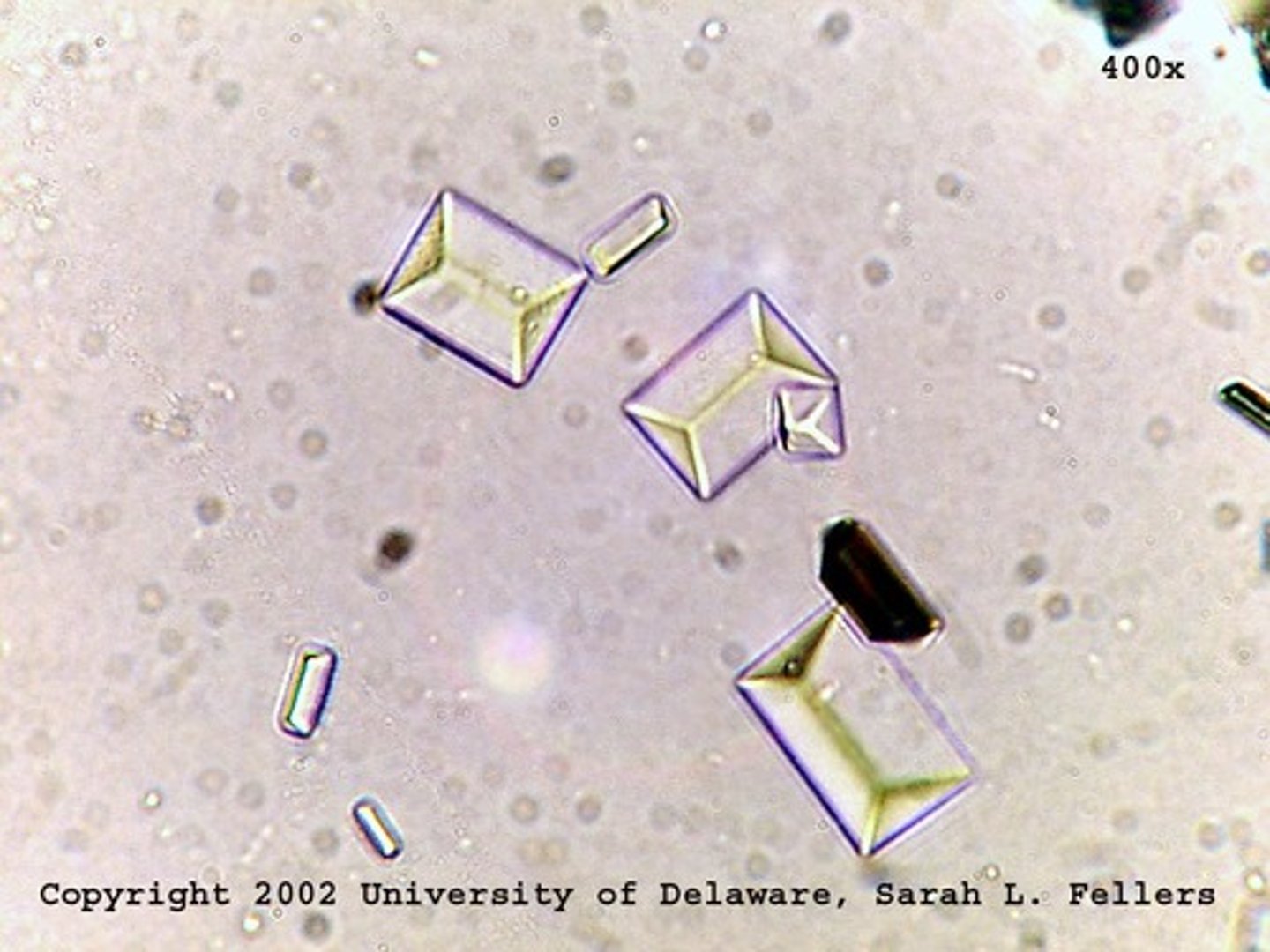
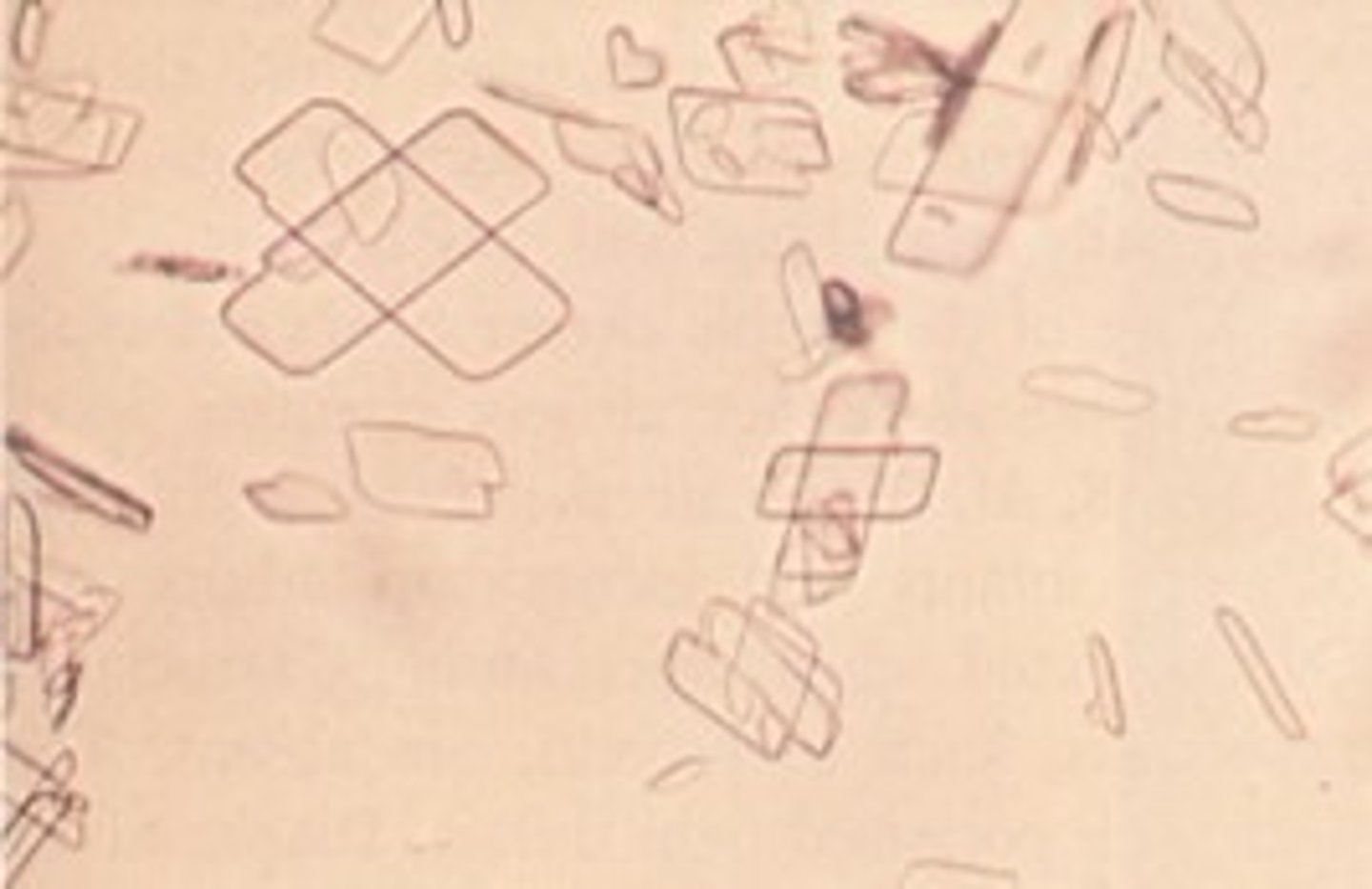
Uric Acid Crystals
- Acid pH urine <5.5
- Yellow-brown color
- Shapes: rhombic, four-sided plates, wedges and rosettes
- Associated with increased levels of purines an nucleic acids
- Seen in patients with leukemia receiving chemotherapy and those with Lesch-Nyhan Syndrome
- Highly birefringent in polarized light allowing them to turn brilliant colors
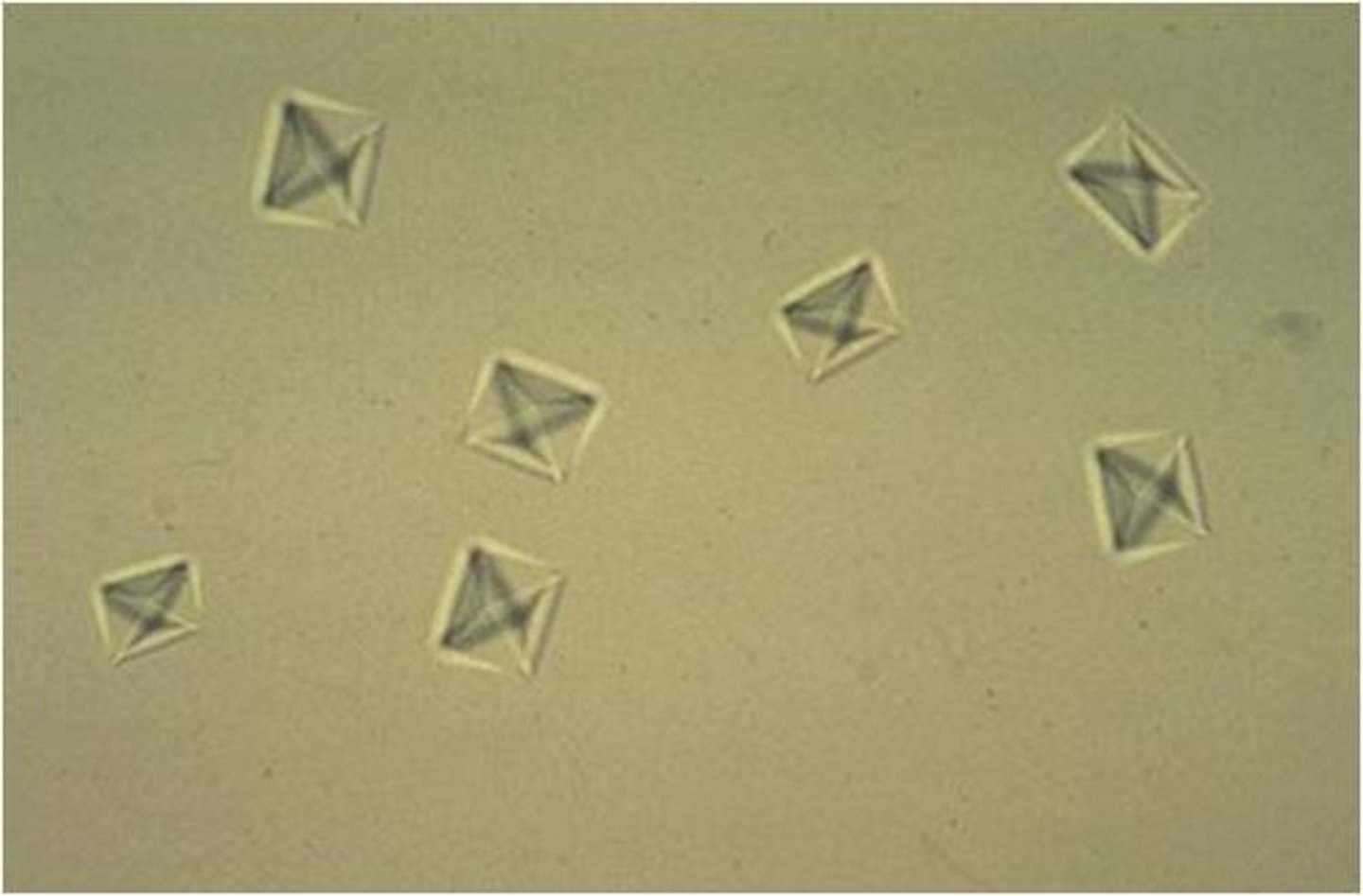
Calcium Oxalate Crystals
- Acid pH urine <5.5
- Colorless
- Dihydrate: octahedral envelope or two pyramids joined at the bases
- Monohydate: are shaped like ovals or dumbbells
- Related to the formation of renal calculi
- Also can be seen after eating tomatoes, asparagus and ascorbic acid (high levels of oxalic acid)
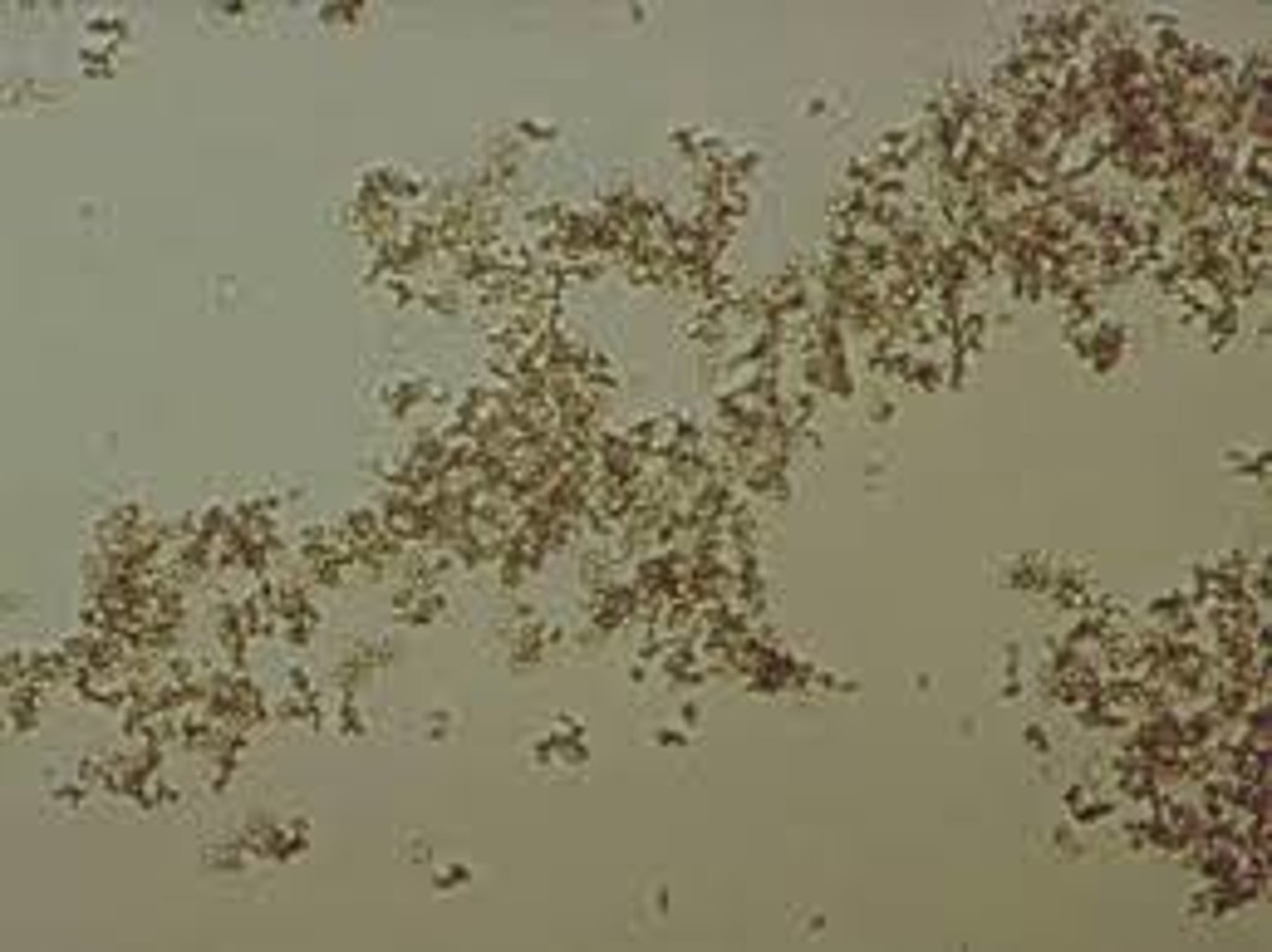
Amorphous Urates
- Acid pH urine <5.5
- Brick dust or yellow brown color
- Can occur in clumps or resemble that of debris or granular casts attached to other sediment structures.
- Refrigeration causes a very characteristic pink sediment color in the samples
Amorphous Phosphates
- Alkaline/Neutral pH <8.0
- White to colorless
- They appear as granules and when they are in large quantities, after refrigeration they form a white precipitate that does not dissolve upon warming.

Calcium Phosphate Crystals
- Alkaline/Neutral pH <8.0
- Colorless
- Flat rectangular plates or thin prisms often in rosette formation like the picture presented
- Dissolve in dilute acetic acid
- Constituents of renal calculi

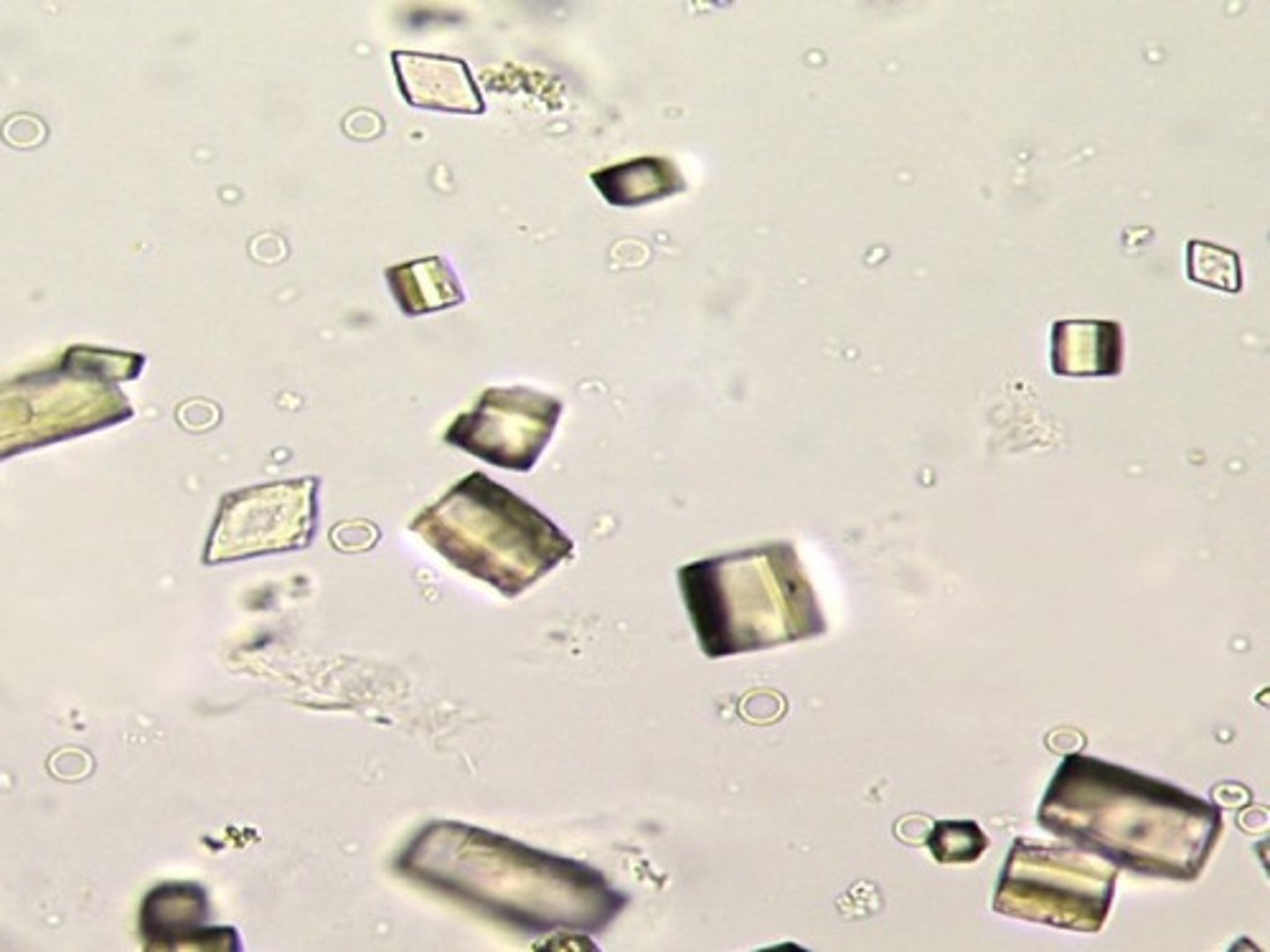
Triple Phosphate Crystals
- Alkaline pH <8.0
- Colorless
- Easily identified as "coffin lid" appearance of the prism shape
- No clinical significance but they are seen in the presence of urea-splitting bacteria
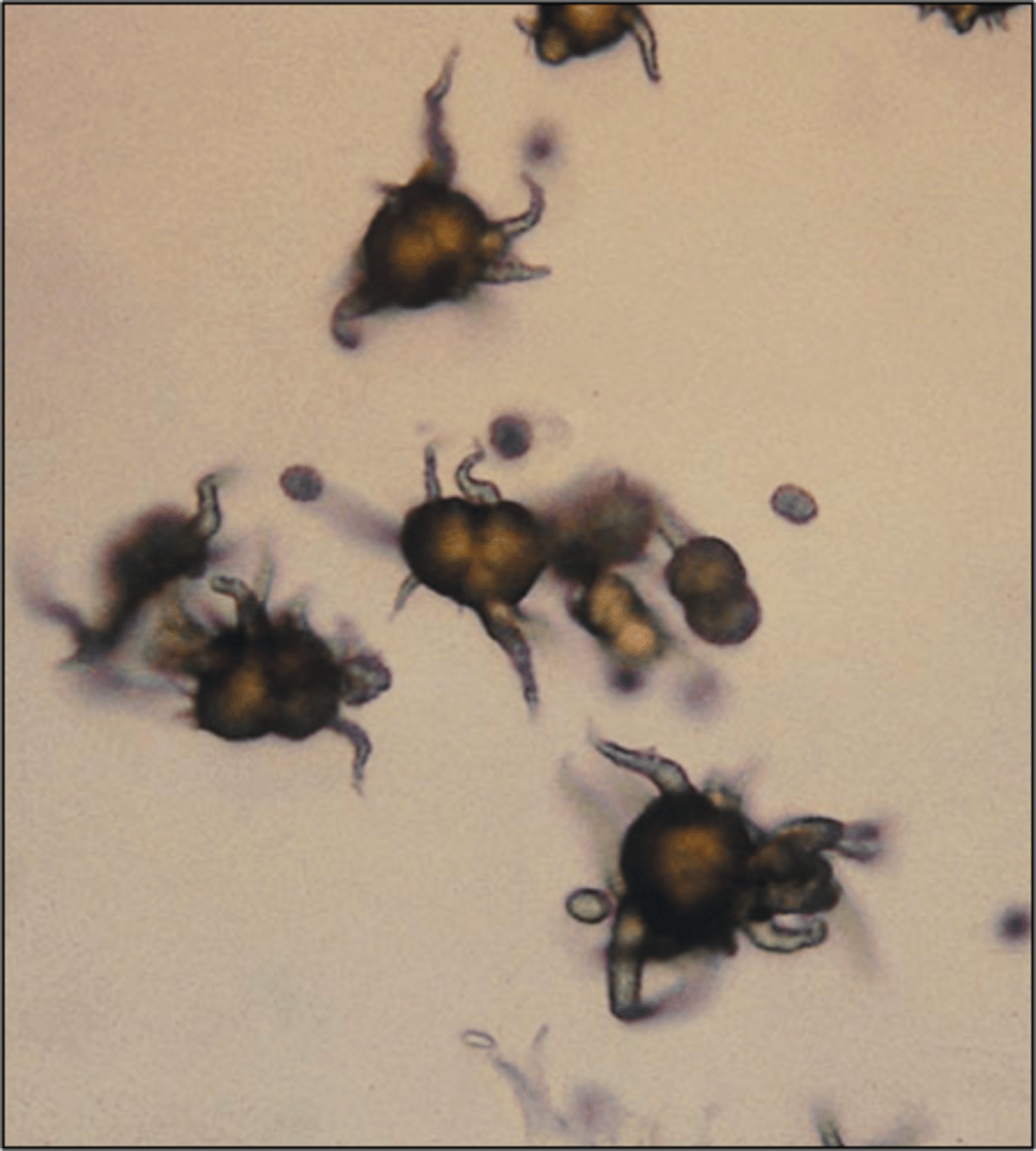
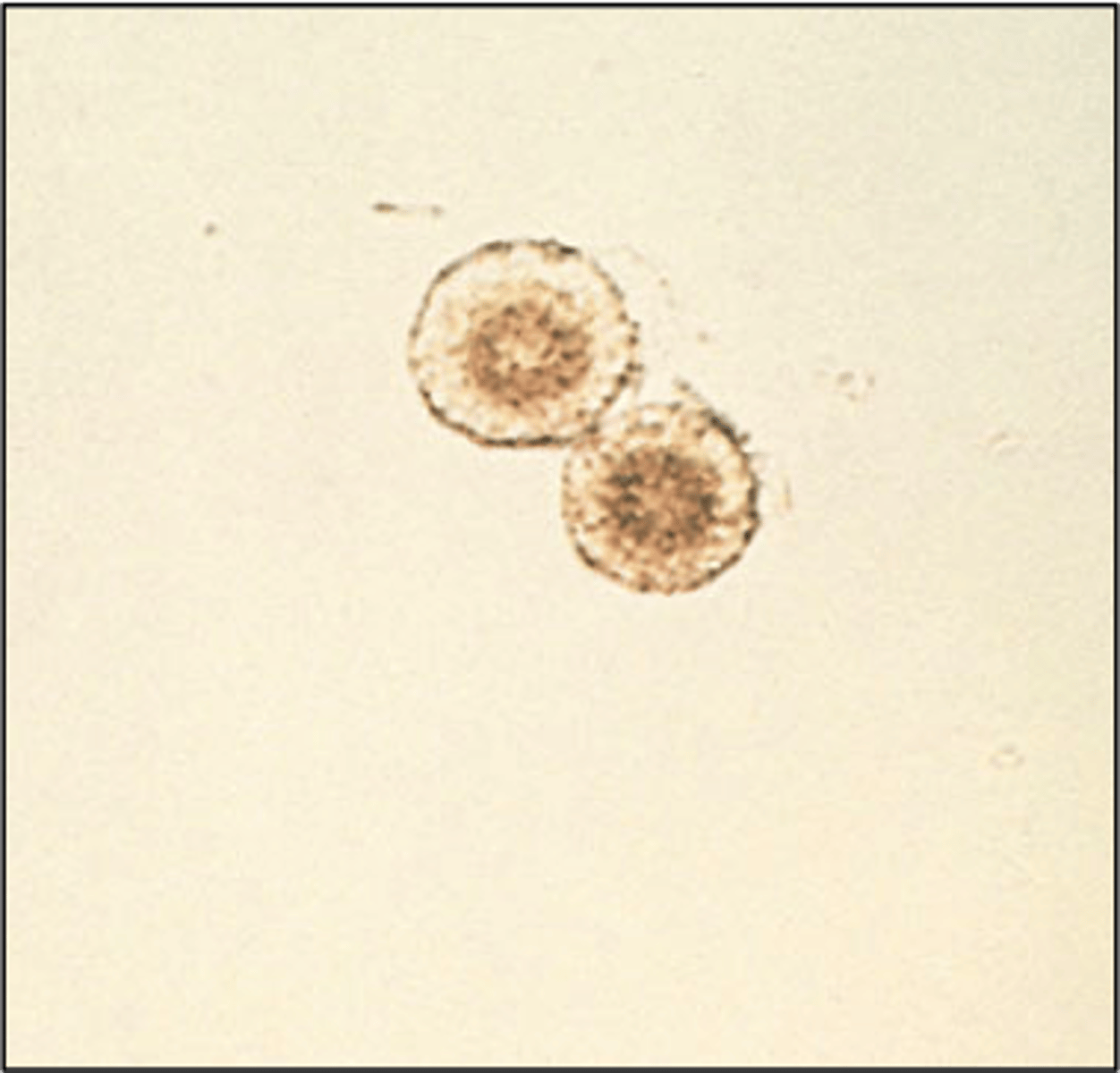
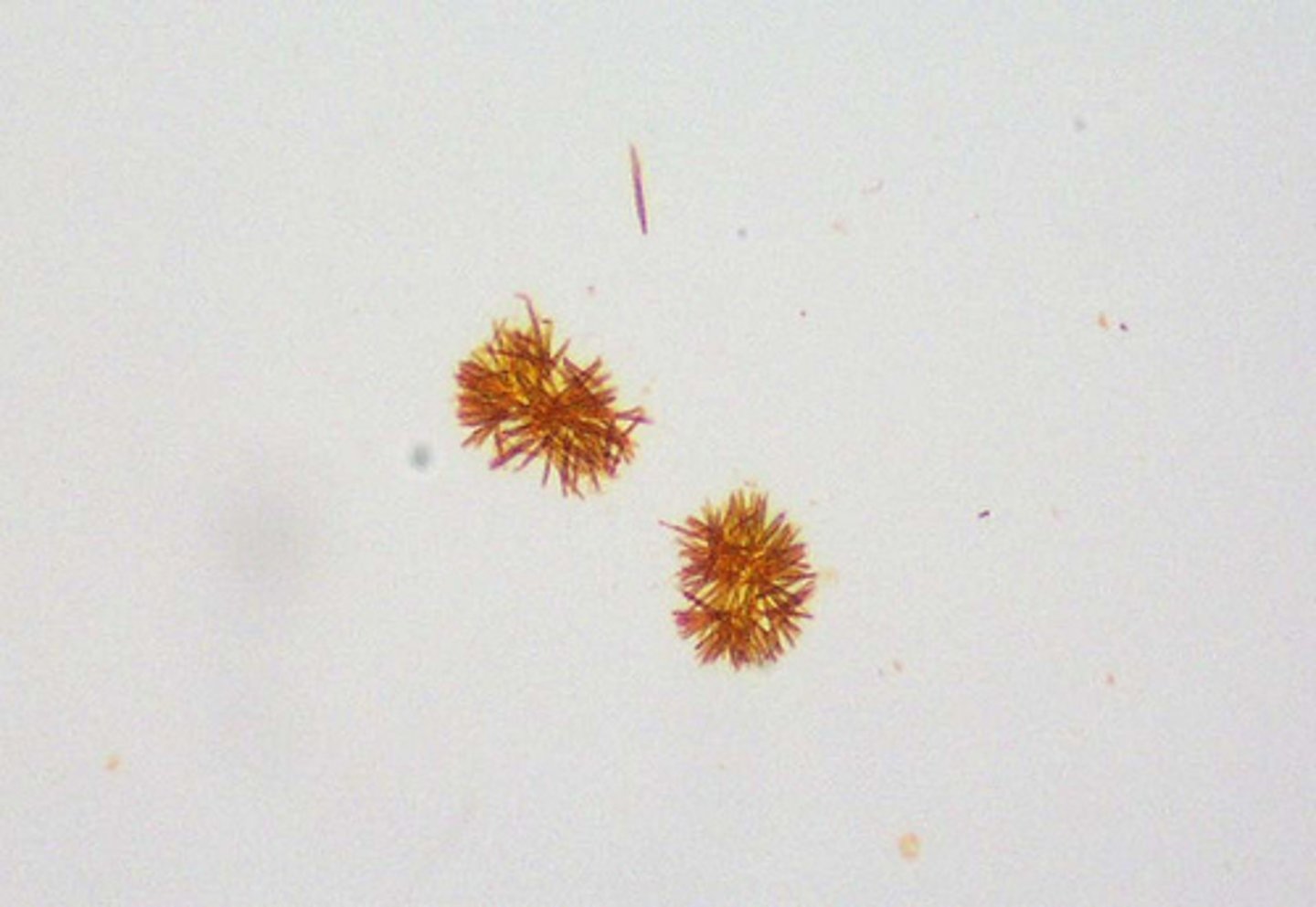
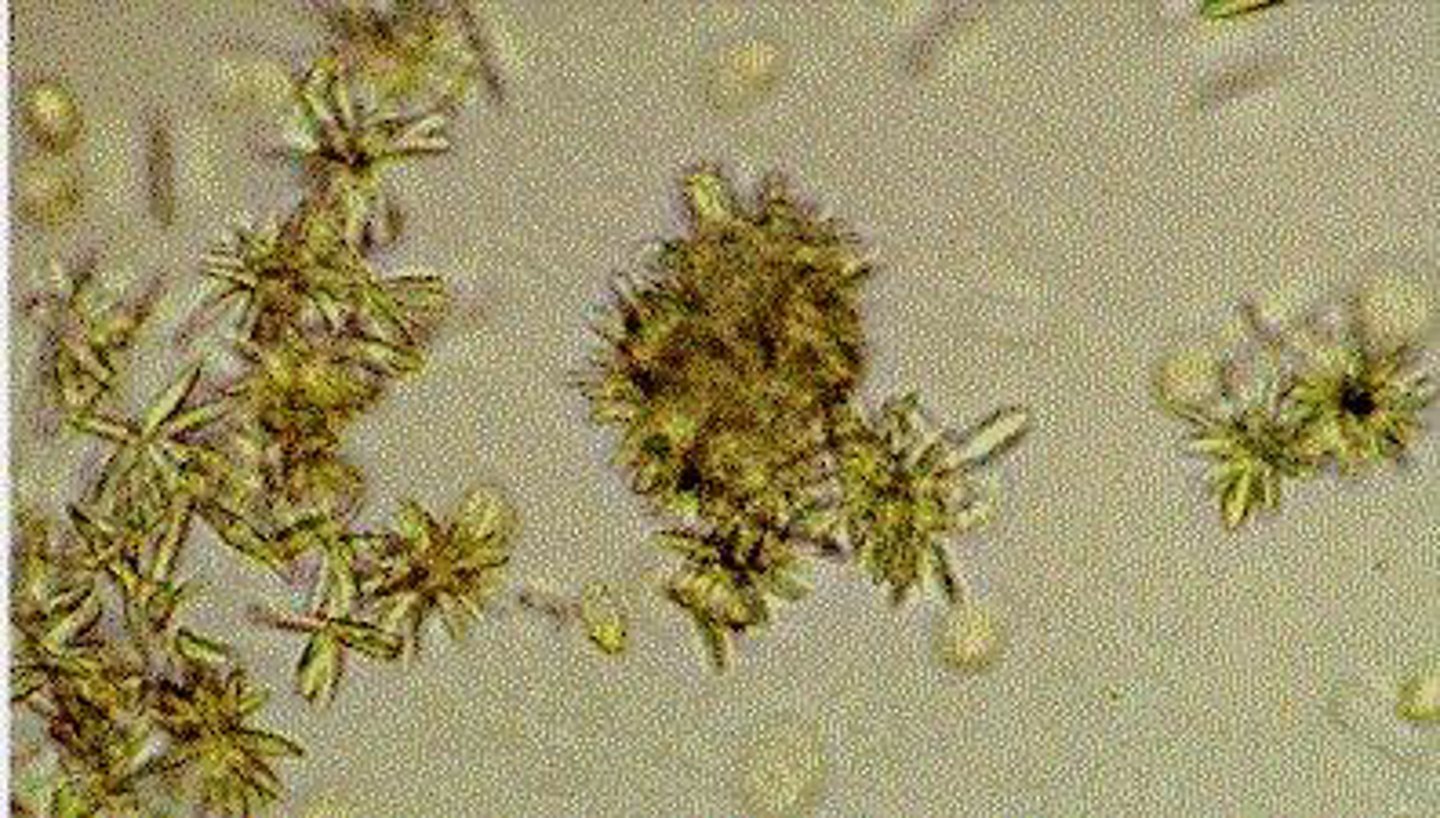
Ammonium Biurate Crystals
- Alkaline pH <8.0
- Yellow-brown "thorny-apples"
- Always encountered in old specimens and may be associated with the presence of ammonia produced by urea-splitting bacteria
Calcium Carbonate Crystals
- Alkaline pH <8.0
- Colorless (dumbbells)
- Resemble amorphous material, but can be distinguished by producing gas after the addition of acetic acid.
- No clinical significance
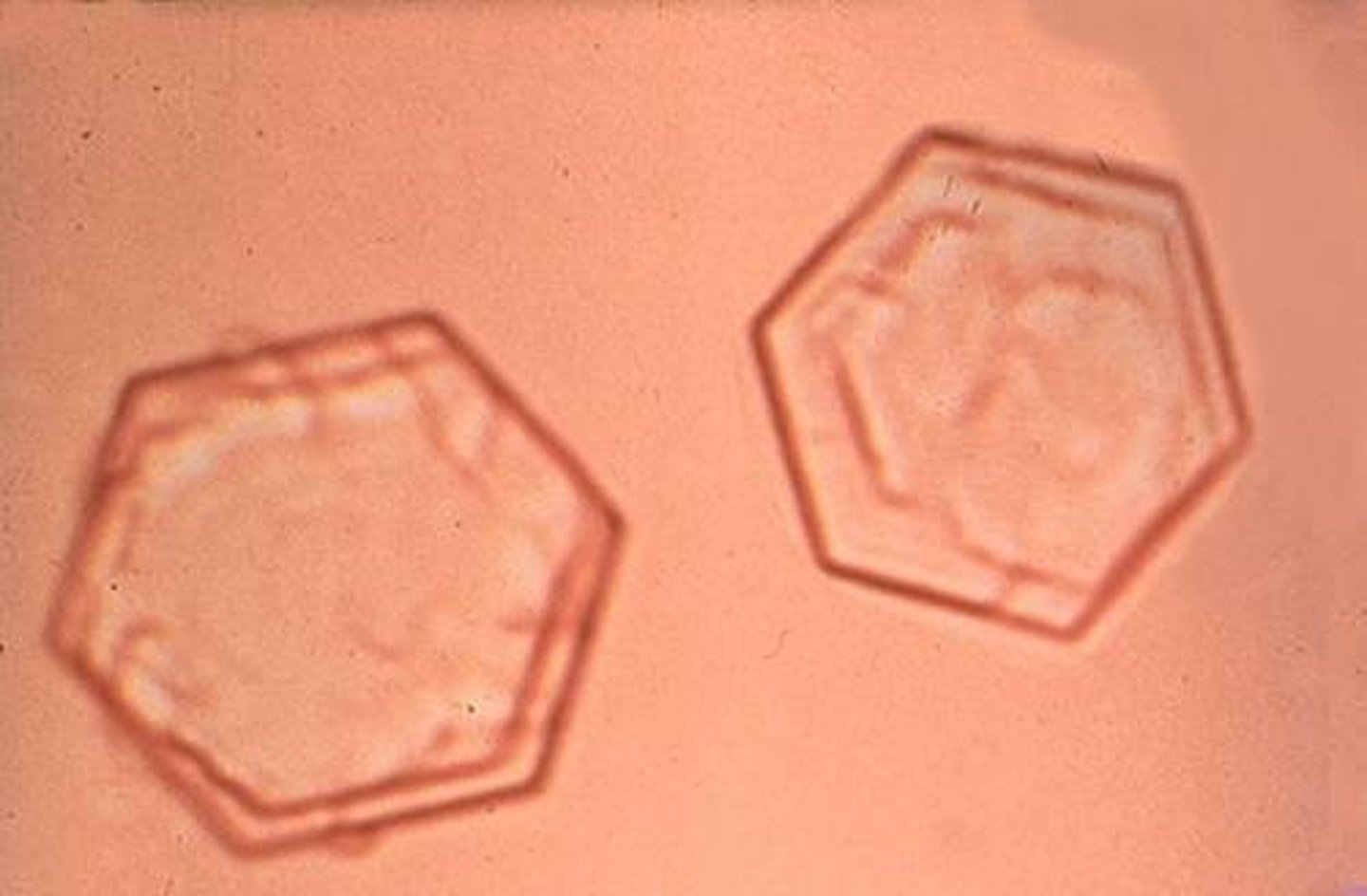
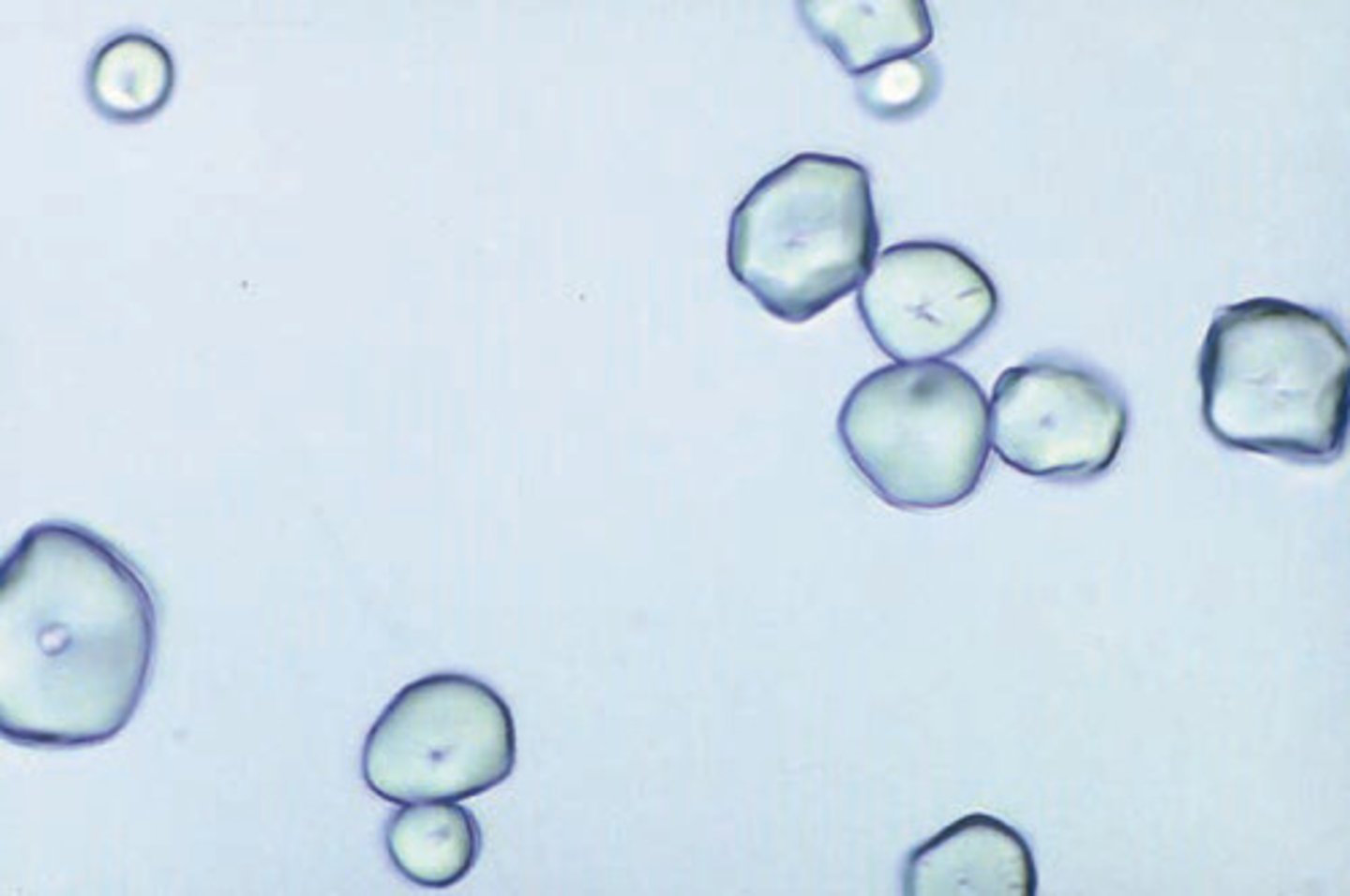
Cystine Crystals
- Acid pH
- Colorless, hexagonal plates
- Inherited cystinuria, means that they don't reabsorb cystine in the tubules so they are more prevalent to forming renal calculi
Cholesterol Crystals
- Acid pH
- Colorless, notched plates
- Nephrotic Syndrome
- Seen in refrigerated specimens
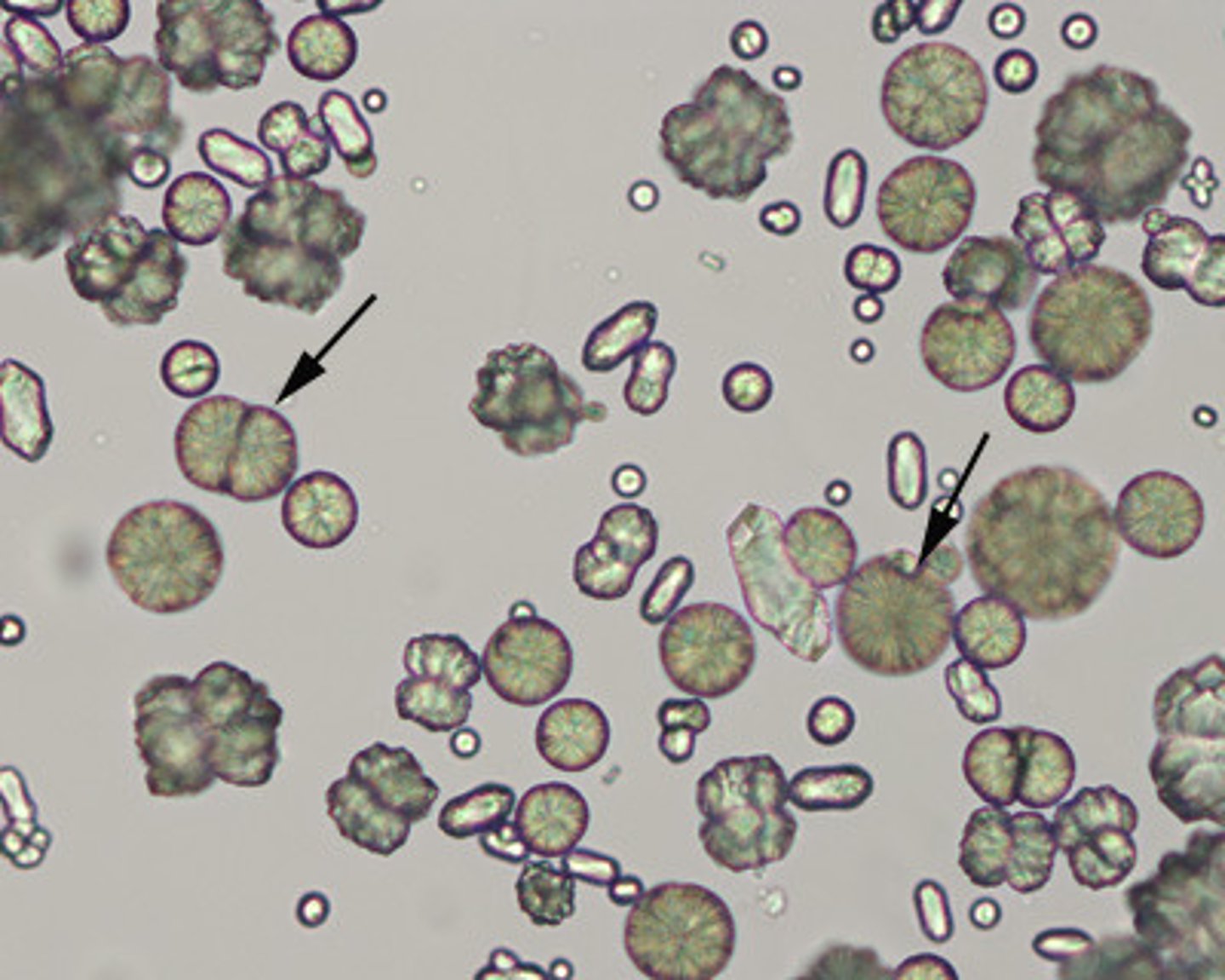
Leucine Crystals
- Acid/Neutral pH
- Yellow, concentric circles
- Liver disease
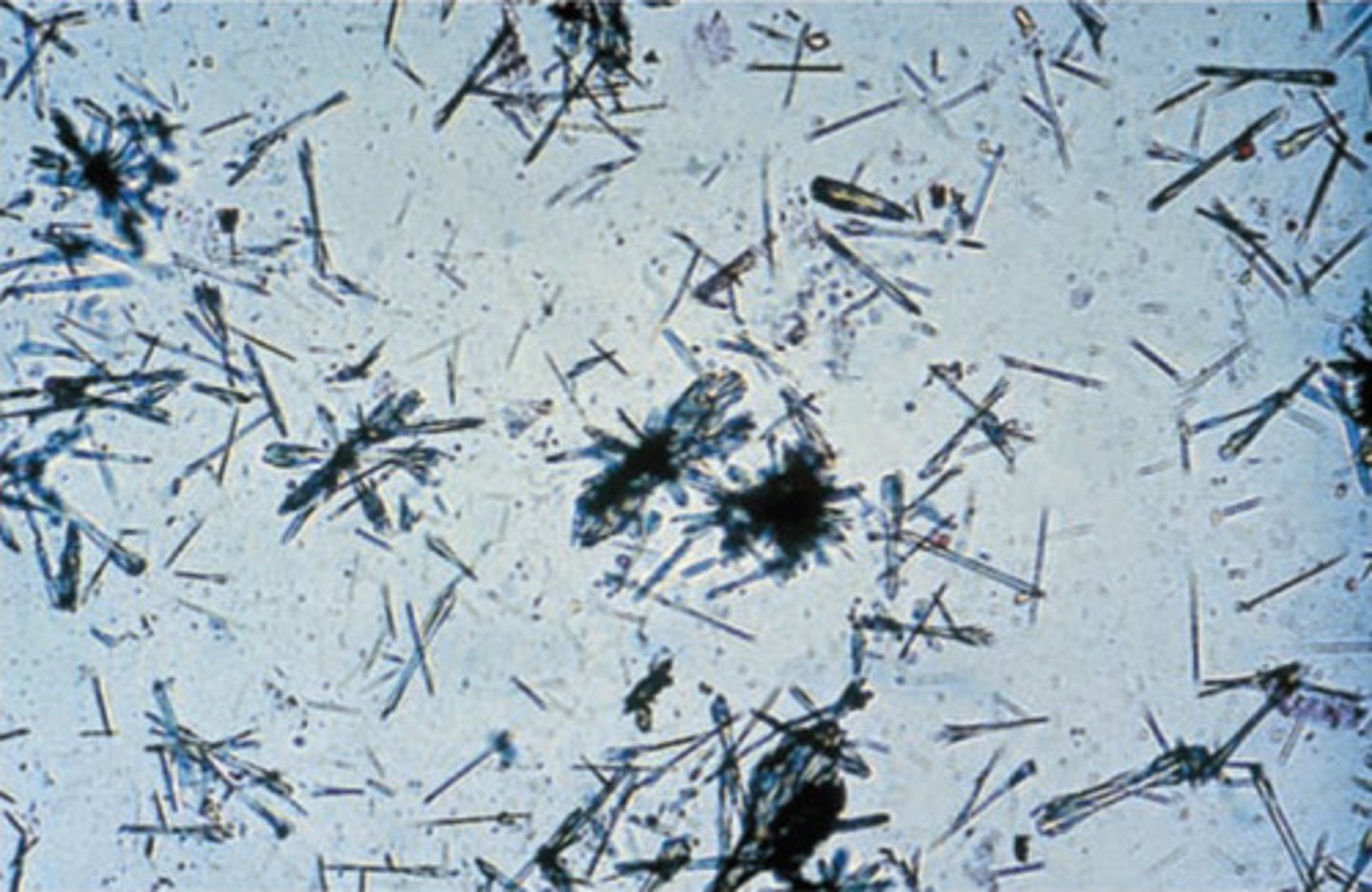
Tyrosine Crystals
- Acid/Neutral pH
- Colorless to yellow, needles
- Liver disease

Bilirubin Crystals
- Acid pH
- Yellow
- Liver disease
Sulfonamide Crystals
- Acid/Neutral pH
- Varied in color and shape
- Infection treatment (antibiotics)
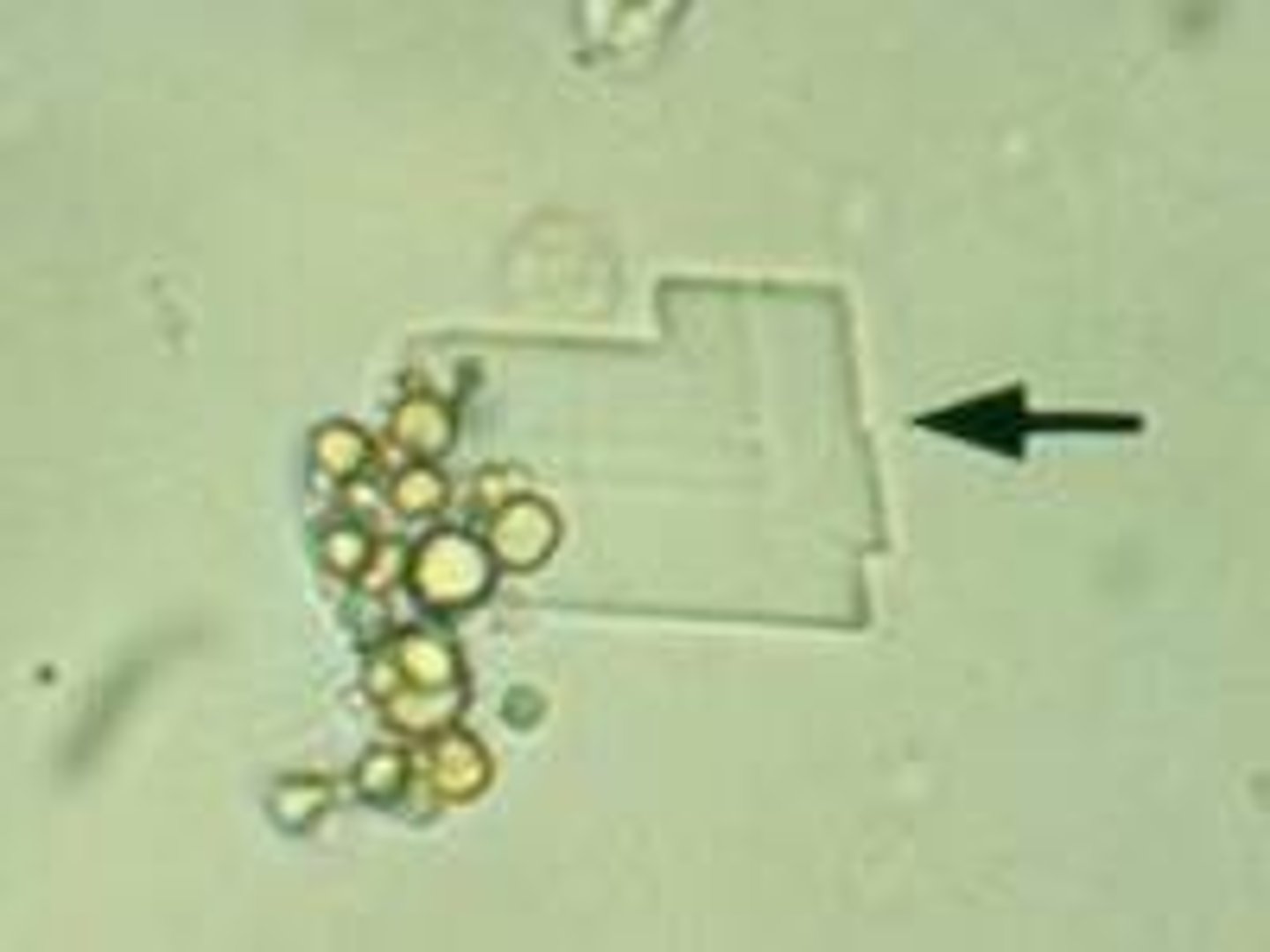
Radiographic Dye Crystals
- Acid pH
- Colorless, flat planes
- Radiographic procedure
Ampicillin Crystals
- Acid/Neutral pH
- Colorless, needles
- Infection treatment (antibiotics)
Starch Granules
- When cornstarch is the powder used in powdered gloves
Pollen Grain
Seasonal contaminants that appear as spheres with cell walls and occasional concentric circles.

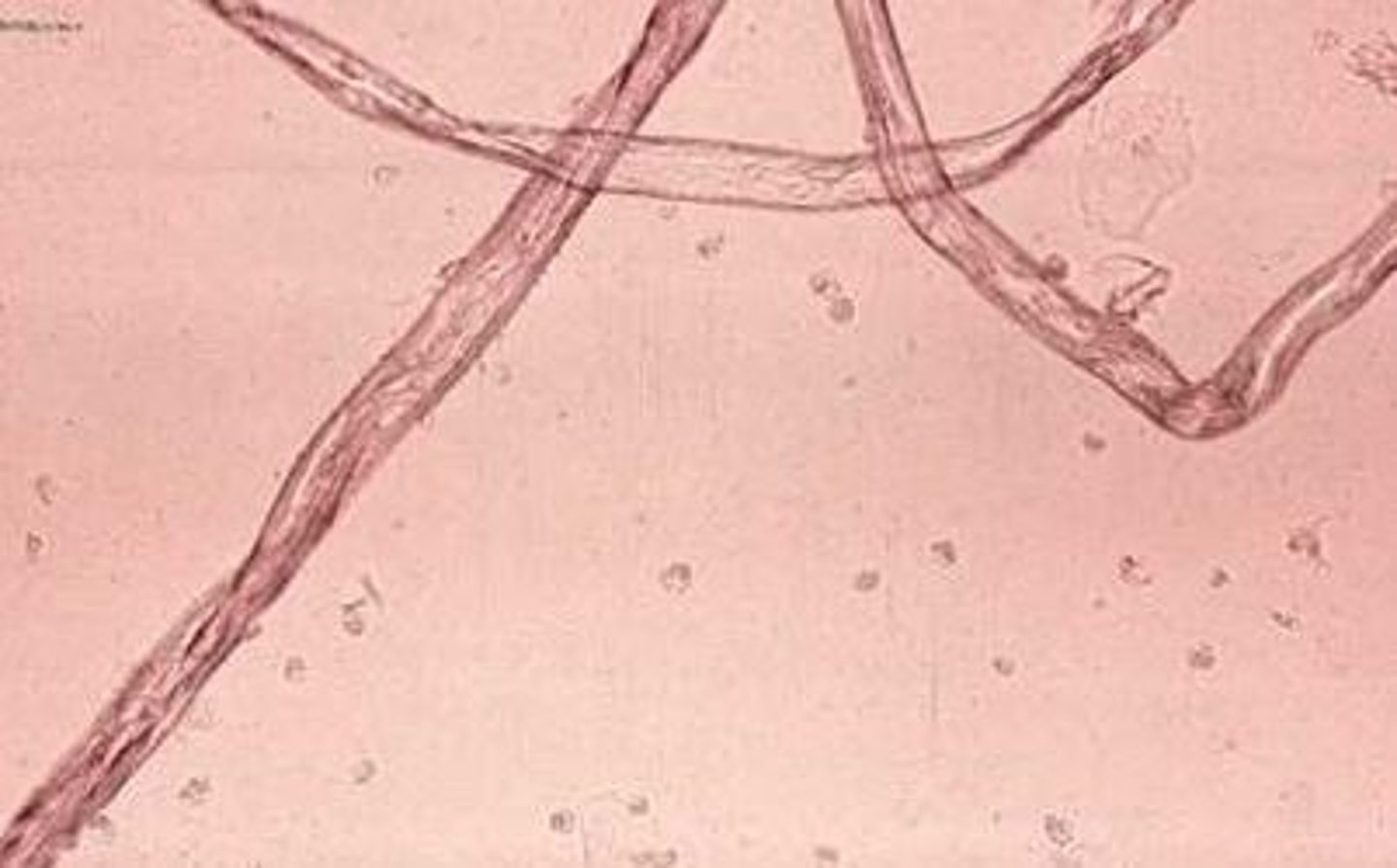
Fiber Urine
Much longer and more refractile than casts, from hairs or diaper fibers. They also usually polarize and can be distinguished under the microscope.