All Quizzes/ROM/Post Midterm Material + Goni
1/443
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
444 Terms
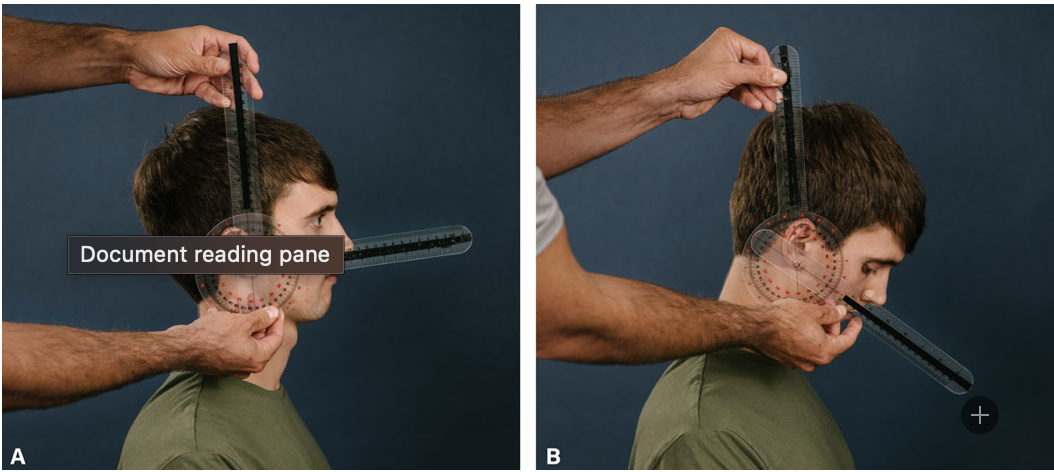
Neck Flexion
Goni: earlobe
Stationary Arm: perpendicular to ceiling
Moving Arm: base of nose
chin going to chest
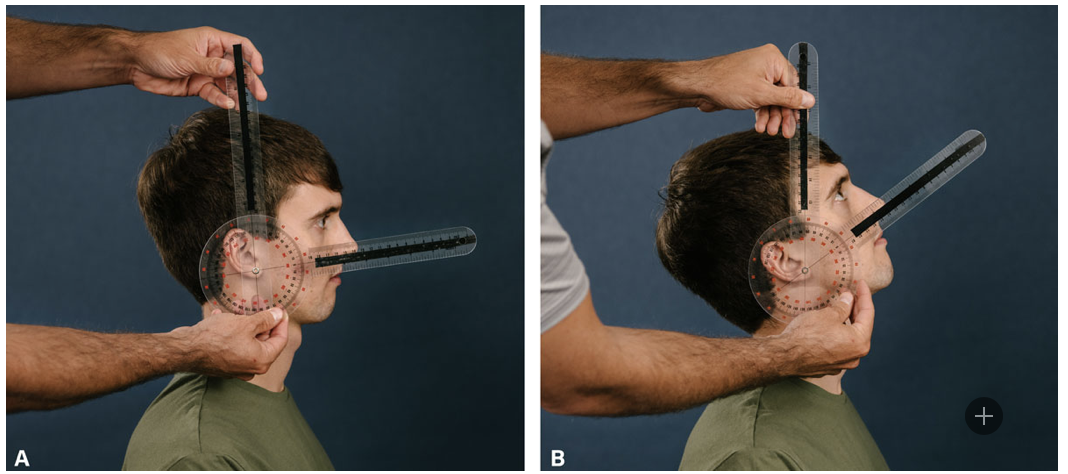
Neck Extension
Goni: earlobe
Stationary Arm: perpendicular to ceiling
Moving Arm: base of nose
chin going to sky
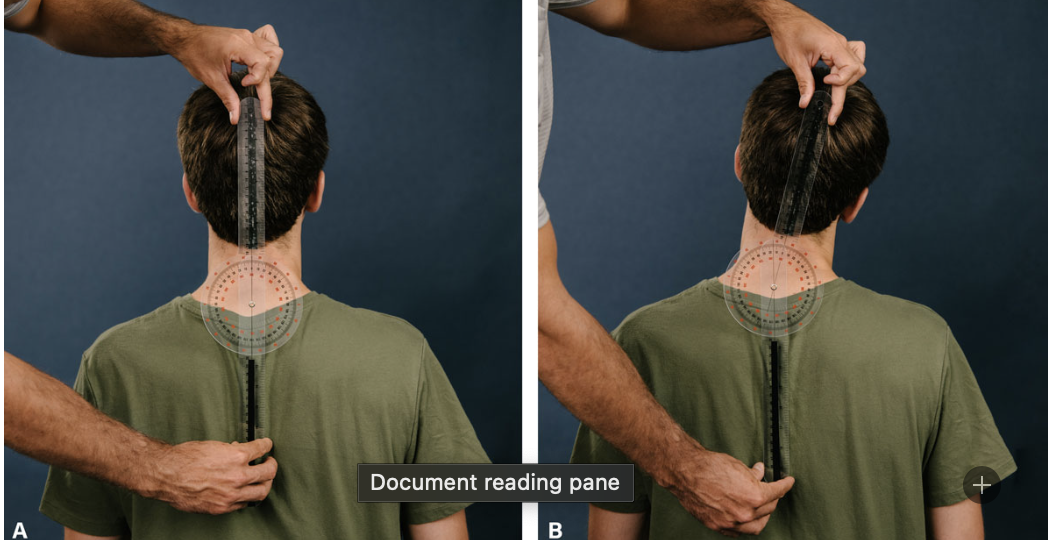
Neck Lateral Flexion
Goni: C7
Stationary Arm: perpendicular to floor
Moving Arm: midpoint of head
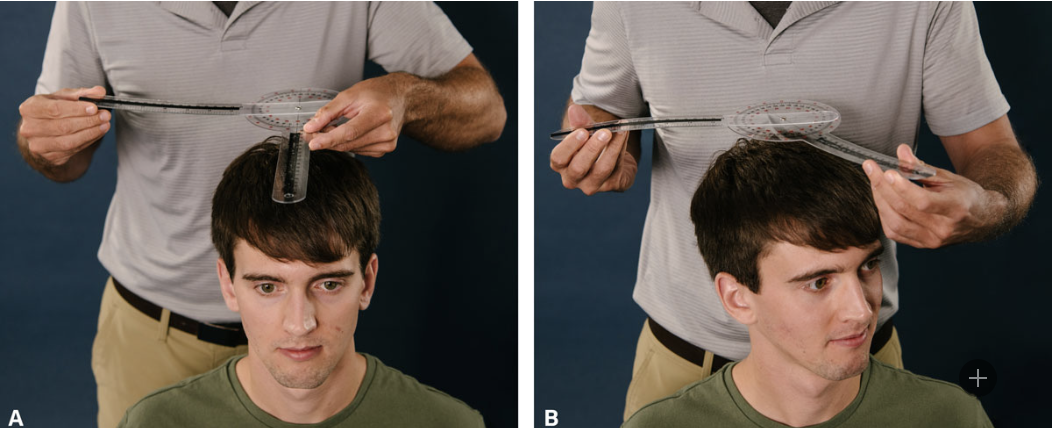
Neck Rotation
Goni: midpoint of the top of head
Stationary arm: acromion
Moving Arm: nose

CMC Flexion (Opposition) Typical Range of Motion
15

CMC Extension Typical Range of motion
20

Palmar Abduction/adduction Typical Range of Motion
0-70 (pa)

Radial Abduction/Adduction Typical Range of Motion
0-70 (ra)

Thumb MCP Flexion/Extension Typical Range of Motion
0-50

Thumb IP Flexion Typical Range of motion
0-80

IP Extension Typical Range of Motion
0-45
Goni Axis - Adjacent to CMC Joint
CMC Flexion, CMC Extension
Goni Axis adjacent to LATERAL CMC joint
Palmar Abduction/adduction
Goni Axis Adjacent to Dorsal IP joint
IP Extension/Flexion
Goni Axis Adjacent Dorsal CMC joint
Radial abduction/adduction
Goni Axis adjacent dorsal MCP joint
MCP flexion, extension
Stationary arm parallel to midline of radius
CMC Flexion, CMC Extension
Stationary Arm midline of lateral aspect of 2nd Metacarpal
Palmar abduction/adduction
Stationary Arm Midline of Posterior 2nd metacarpal
radial abduction/adduction
stationary arm dorsal aspect of 1st metacarpal
MCP Flexion/extension
Stationary arm dorsal aspect of proximal phalanx
IP Flexion, IP Extension
Moving Arm Parallel to midline of 1st metacarpal
CMC Flexion, CMC extension
Moving Arm is in midline of lateral aspect of 1st metacarpal
Palmar Abduction/Adduction
Moving Arm is in midline of posterior aspect of 1st metacarpal
radial abduction/adduction
Moving Arm dorsal aspect of proximal phalanx
MCP Flexion/extension
MCP Abduction/Adduction
CMC Flexion/Extension
MCP Flexion/extension
Moving arm dorsal aspect of distal phalanx
IP Flexion, IP extension
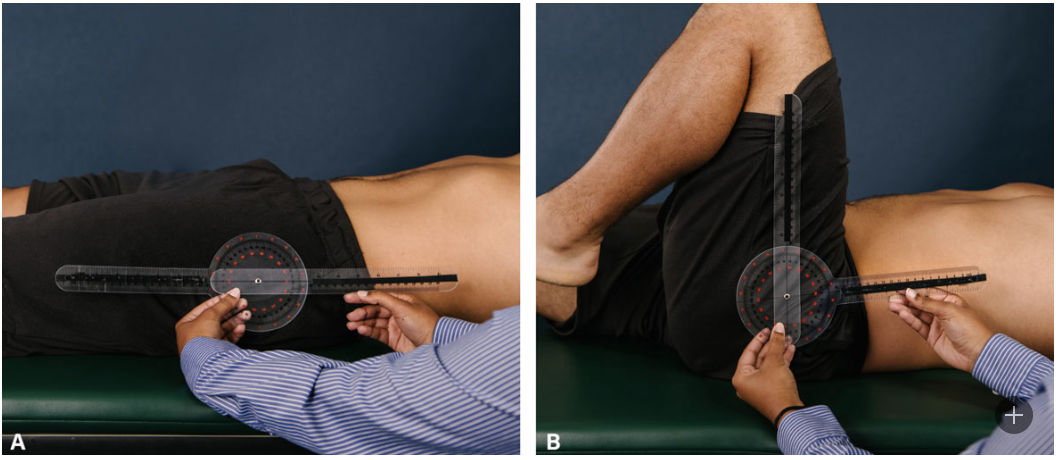
Hip Flexion
Goni: Greater Trochanter
Stationary arm: lateral midline of trunk
Moving Arm: lateral midline of femur
when patient is in supine
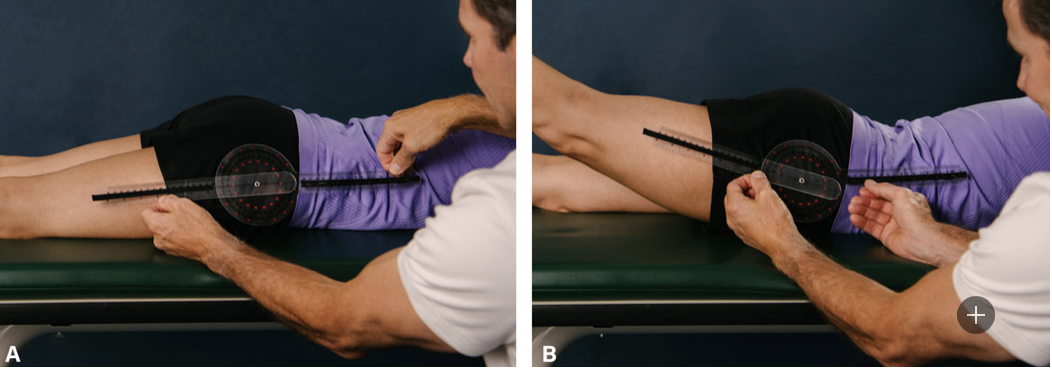
Hip Extension
Goni: Greater Trochanter
Stationary Arm: lateral midline of trunk
Moving Arm: midline of lateral femur
when patient is in prone
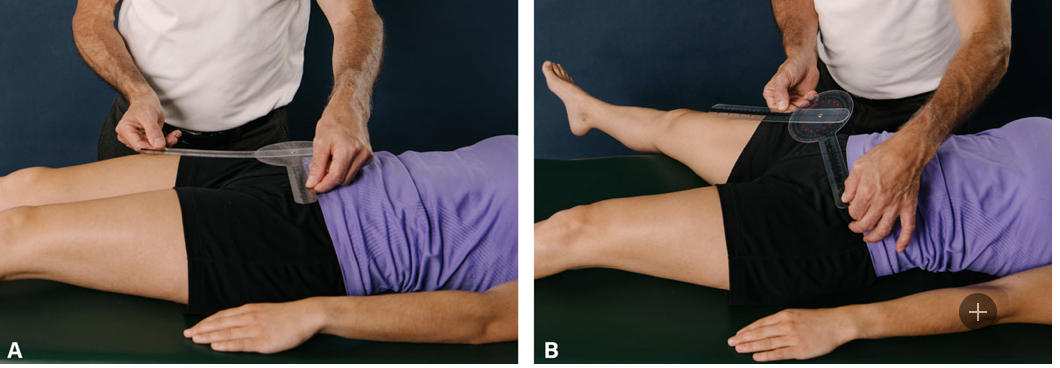
Hip Abduction
Goni: ASIS
Stationary Arm: across pelvis in line with ASIS on opposite side
Moving Arm: midline of anterior femur

Hip Adduction
Goni: ASIS
Stationary Arm: across pelvis in line with ASIS on opposite side of pelvis
Moving arm: midline of anterior femur
when opposite leg abducted off mat
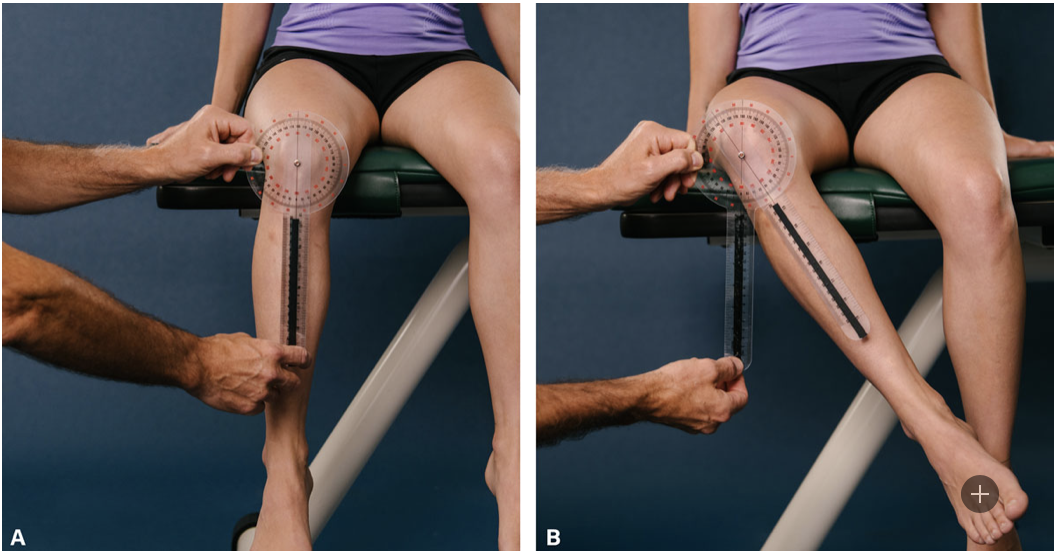
Hip External Rotation
Goni: patella
Stationary Arm: perpendicular to floor
Moving Arm: midline of anterior tibia
(ER)

Hip Internal Rotation
Goni: patella
Stationary arm: perpendicular to floor
Moving arm: midline of anterior tibia
(IR)
Stability depends on:
vision, vestibular system, proprioception, tactile sensation
vision and vestibular system only
proprioception and vestibular system
proprioception, vision, vestibular system, planted limb, tactile sensation
vision, vestibular system, proprioception, tactile sensation
“parts of the body or mobility devices that come into
contact with the ground and the distance between those points” best describes what component of stability:
Center of gravity (CoG)
base of support (BoS)
base of support (BoS)
How can an occupational therapist modify an activity to better support the base of support and stability of a patient?
increase more points of contact and decrease the distance between them
decrease points of contact and increase the distance between them
decrease points of contact and the distance between them
increase more points of contact and the distance between them
increase more points of contact and the distance between them
“focal point at which gravity acts; where
the weight of an object is evenly distributed” describes which component of stability?
Center of gravity (CoG)
base of support (BoS)
Center of Gravity (CoG)
At what level is CoG at in anatomical position:
1st sacral level
2nd sacral level
3rd sacral level
2nd sacral level
As Your BoS widens, stability _____:
as your BoS widens, stability decreases
as your BoS widens, stability increases
as your BoS widens, stability stays the same
as your BoS widens, stability increases
As your CoG lowers toward the ground, stability ______
As your CoG lowers toward the ground stability increases
As your CoG lowers toward the ground stability decreases
As your CoG lowers toward the ground stability stays the same
As your CoG lowers toward the ground stability increases
“relative position of body
segments in response to demands of
activity” best describes:
body stance
posture
anatomical adjustment
placement
posture
Posture depends on:
sensory output and motor input
motor output and sensory input
motor output and sensory input
Which is an example of an ergonomic adjustment:
Hip, knees, elbows at 90 with wrist neutral and monitor 18-24 inches away from face at eye level
Hip, knees, elbows at 80 with wrist neutral and monitor 18-24 inches away from face at eye level
Hip, knees, elbows at 90 with wrist supine and monitor 18-24 inches away from face at eye level
Hip, knees, elbows at 90 with wrist neutral and monitor 20-24 inches away from face at eye level
Hip, knees, elbows at 90 with wrist neutral and monitor 18-24 inches away from face at eye level
How does the OTPF define functional mobility:
moving from one position/place to
another such as in bed mobility, w/c
mobility, and transfers
moving from one position/place to
another like driving
moving from one position/place to
another such as in bed mobility, w/c
mobility, and transfers
Lack of bed mobility can contribute to:
scar tissue build up
bedside incontinence
skin break down
skin break down
What are examples of OT interventions for bed mobility:
use of logrolling, bridging, and a trapeze bar
use or rolling pad, benching, and a trapeze bar
use of logrolling, bridging, and a quad bar
use of logrolling, bridging, and a trapeze bar
What can promote wheelchair mobility:
supportive seated surface to promote postural alignment only
supportive seated surface to promote postural alignment and stability
supportive seated surface to stability only
supportive seated surface to promote postural alignment and stability
Typical gait features:
reciprocal pattern of lower extremity movement
symmetrical pattern of lower extremity movement
asymmetrical pattern of lower extremity movement
reciprocal pattern of lower extremity movement
Gait includes what types of muscle movement
concentric and eccentric contractions
eccentric and isometric contractions
concentric, eccentric and isometric contractions
concentric, eccentric and isometric contractions
“Distance that one foot advances in relation to the
other” describes what part of Gait:
step
step width
cadence
step
“width between heels” describes which part of gait:
step
step width
cadence
step width
“steps per minute” describes what part of gait:
step
step width
cadence
cadence
What are the components of the stance phase:
heel strike, foot flat, mid stance, heel off
heel strike, foot flat, mid stance, heel off, toes off
heel tip, foot up, high stance, heel on, toe on
heel strike, foot flat, mid stance, heel off, toes off
What are the components of the swing phase:
midswing, deceleration, pivot
turn, step, lunge
acceleration, midswing , deceleration
acceleration, midswing, deceleration
What is NOT true about mobility devices:
they enhance safe functional mobility
they are can be prescribed by OT/PT team or individually
they can only be described by PT team
they add points of contact to ground and increase BoS
they can only be described by PT team
A patient comes with minor weakness and balance concerns. The best mobility device for suggested use is:
cane
walker
crutch
cane
A patient comes in with severe instability. Which mobility device is of best suggested use?
cane
walker
crutch
walker
At what level should a walker be adjusted to:
Tip of fingers
wrist crease
greater trochanter
wrist crease
How many inches from the armpit should a crutch be adjusted to:
1 inch
1.5 inch
2 inch
2.5 inch
2 inch
What determines the type of transfer used:
patient functional level and diagnoses only
patient functional level and medical status only
patient functional level, diagnoses, medical status
patient functional level, prescriptions, and medical status
patient functional level, diagnoses, medical status
Which type of transfer does the following description best describe, “requirement of upper body strength and consideration of friction”
sliding board transfer
squat pivot
stand pivot
dependent transfer
sliding board transfer
A dependent transfer includes:
at least two people
mechanical assist
at least two people or mechanical assist
at least 3 people or mechanical assist
at least two people or mechanical assist
Postural abnormality of leg length discrepancy is associated with which type of force:
ascending force
descending force
ascending force
Scoliosis is associated with what type of force:
ascending force
descending force
descending force
In a posterior tilt, what is the relationship of the positioning between the ASIS and PSIS:
PSIS is higher than the ASIS
ASIS is higher than the PSIS
ASIS is higher than the PSIS
Prolonged sitting can lead to:
rounded back, Lordosis
rounded back, Kyphosis
inverted back, lordosis
inverted back, kyphosis
rounded back, kyphosis
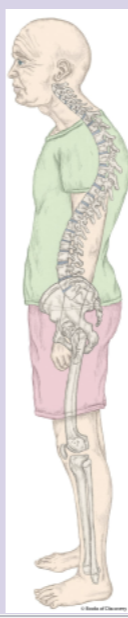
this image best implicates which postural abnormality?
dowagers hump
Sway back
Kordosis
dowagers hump
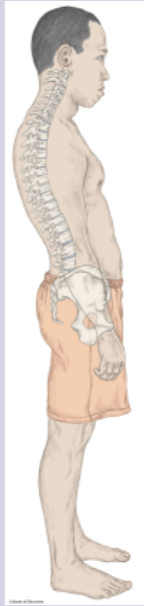
this image best implicates which postural abnormality?
dowagers hump
Sway back
Kordosis
sway back
In an anterior tilt, what is the relationship of the position of the PSIS to ASIS
PSIS is higher than ASIS
ASIS is higher than PSIS
PSIS and ASIS are in alignment
PSIS is higher than ASIS
Anterior Tilts are associated with:
kyphosis
lordosis
lumbar kyphosis
lumbar lordosis
lumbar lordosis
What is implicated in Pelvic obliquity:
kinematic chain, asymmetry, skin integrity
open chain movements, asymmetry, skin integrity
close chain movements, asymmetry, skin integrity
kinematic chain, asymmetry, skin integrity
A forward head posture is caused by:
cervical vertebrae losing natural kyphosis
cervical vertebrae losing natural lordosis
cervical vertebrae losing natural lordosis
“Weakness in gluteus medius causing a lateral lean to weak side” describes which abnormal gait pattern:
trendelenberg
circumduction
foot drop
hemiplegic
trendelenberg
“muscle weakness in legs causes
trunk and pelvis to compensate by
laterally swinging leg to the side
of the body to propel it forward” describes which abnormal gait pattern:
trendelenberg
circumduction
foot drop
hemiplegic
circumduction
“weakness or paralysis of ankle dorsiflexors causing the toes to come into contact with group before the heel, typical after stroke” describes which abnormal gait pattern?
trendelenberg
circumduction
foot drop
hemiplegic
foot drop
Hemiplegic Gaits can include which gait abnormalities:
circumduction and foot drop
circumflexion and foot drop
circumduction and foot tilt
circumflexion and foot tilt
circumduction and foot drop
“Hip adducted and knee locked in extension” describes which abnormal gait:
hemiplegic
parkinsonian
trendelenberg
hemiplegic
Where is weight placed in a Parkinsonian Gait:
tips of toes with flexion of trunk
balls of heels with flexion of trunk
balls of heels with extension of trunk
tips of toes with extension of trunk
balls of heels with flexion of trunk
“Affected by impaired perception
and modulation of motor
movements looking like shuffling of feet” best describes which abnormal gait pattern?
hemiplegic
parkinsonian
trendelenberg
parkinsonian
“Narrowing or crossing
over of the legs during
ambulation and is associated with CP and
other neurological
diagnoses” best describes which gait:
ataxic gait
parkinsonian gait
scissor gait
scissor gait
Manny was in a car accident where his cerebellum was injured but everything else was okay. Even so, he is walking funny. Which abnormal gait pattern does this best describe?
scissor gait
ataxic gait
TVA gait
ataxic gait
Which of the following is NOT a contraindication to MMT
Acute Fracture
Hypermobility
Post-Op orders limiting all ROM
Subluxation
Hypermobility
Your patients elbow flexion and extension is measured at 15-120. Which of the following is true?
There is limitation at both flexion and extension
TRUE OR FALSE: the resistive hand in MMT is place proximal to the joint you are testing
FALSE
What are two environmental considerations for measuring ROM
time of day, temperature
What is the axis to perform ROM of GH horizontal abduction
Superior Aspect of humeral head
what is the most commonly dislocated joint
GHJ
Which of the following joints the MOST mobile joint
ball and socket
TRUE OF FALSE: then considering scapulohumeral rhythm, the scapula accounts for 60 out of the 180 degrees of motion in shoulder flexion
TRUE
What is the typical ROM for shoulder horizontal adduction
135
During MMT if a patient has a full ROM in an AG plane and breaks at MOD resistance, what is the score?
3+
When performing MMT of forearm supination, the patient performs full ROM against gravity. What do you do next?
apply resistance
what is the norm for forearm pronation
80
the humeradial joint is classified as which of the following
modified hinge
where is the resistance applied for elbow flexion
distal forearm
While performing MMT where do you apply resistance during wrist extension?
proximal metacarpals
dorsal metacarpals
medial metacarpals
none of the above
dorsal metacarpals
TRU EOR FALSE: the hamate is the axis of movement for radial deviation
FALSE
When performing MMT your patient is only able to complete ½ the range of motion for wrist extension while her forearm is supported on the table in neutral (thumb up). What is her MMT score?
2-
Where do you stabilize when performing MMT of wrist flexion
Distal forearm
What is the AROM of wrist extension
70
what is the norm ROM of PIP flexion
0-100