Normal Fetal Chest, Abdomen, and Pelvis
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
Fetal Thorax
assess size, shape, and symmetry of the thorax
echogenicity and symmetry of the lungs
size, location, and axis of the heart
presence of complete diaphragm
presence/absence of fluid collections
Thorax
always scan through the thorax in transverse an longitudinal planes
assess the bony elements of thorax:
clavicles
ribs
scapula
vertebral bodies
sternum
Clavicles
not a routinely imaged part of the body
imaged in the presence of skeletal dysplasias and other rare suspected syndromes
can be measured and used as a tool to determine GA
Ossify as early as 8-9 weeks

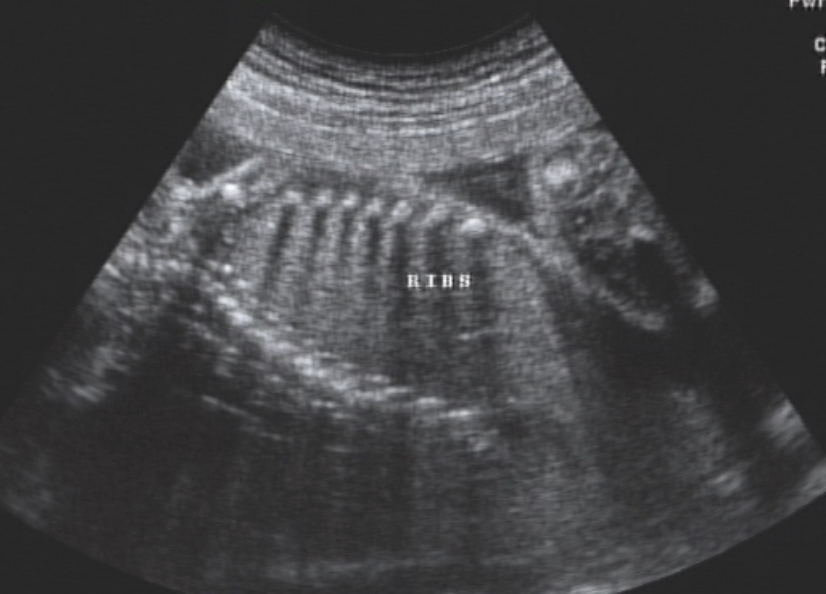
Ribs
Seen in transverse and longitudinal planes
ossify around 10-12 weeks
assess rib thickness, check for fractures, & symmetry
not routinely imaged
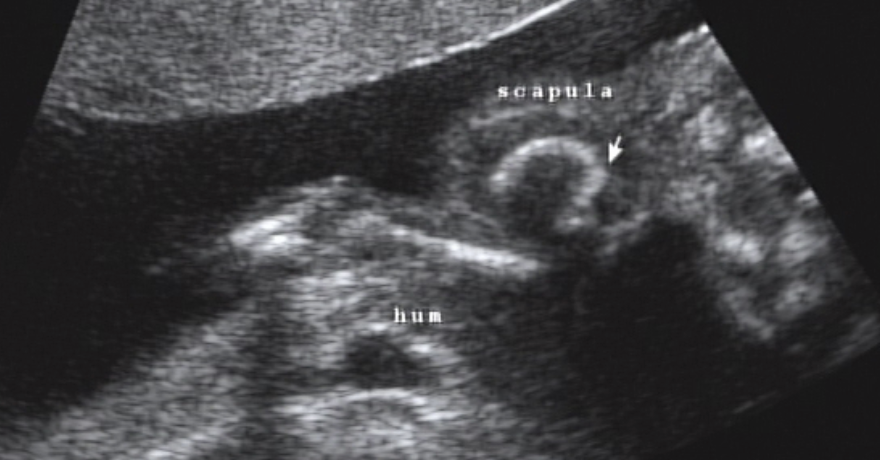
Scapula
not routinely imaged
ossification around 21-27 weeks
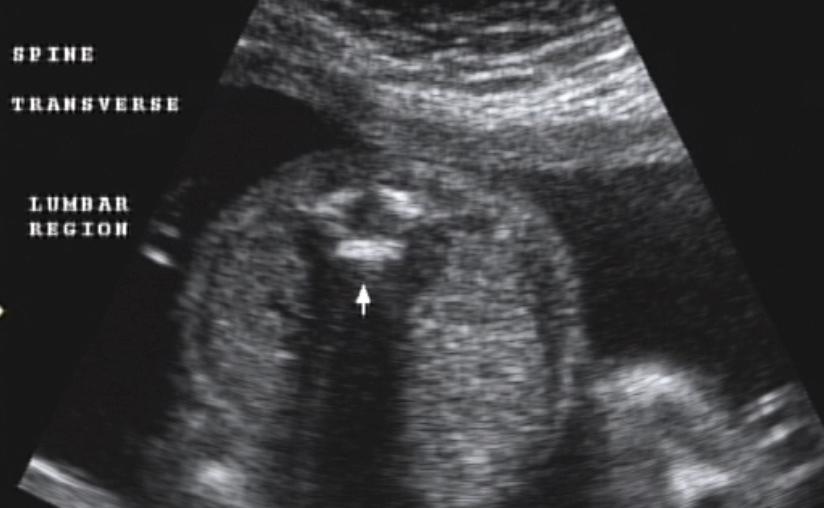
Spine
imaged in transverse and longitudinal planes
identify skin line - looks for breaks in skin (spina bifida)
curvature and normal alignment of vertebral bodies
Lungs
Embryologic development of the lungs occurs around week 5
at 16-24 weeks the normal number of bronchi are formed
after 24 weeks the air spaces, blood vessels and capillaries change and increase in number to prepare for life outside the womb
In order for lung development to occur:
Adequate space in the thorax
↓ constriction = lung volume
Fetal breathing motion
without ability to “practice” breathing → pulmonary hypoplasia
Fluid within the lungs → distends airways
Amniotic fluid
How does amnionic fluid aid in lung development?
Amniotic fluid is vital
Without fluid = pulmonary hypoplasia = usually lethal
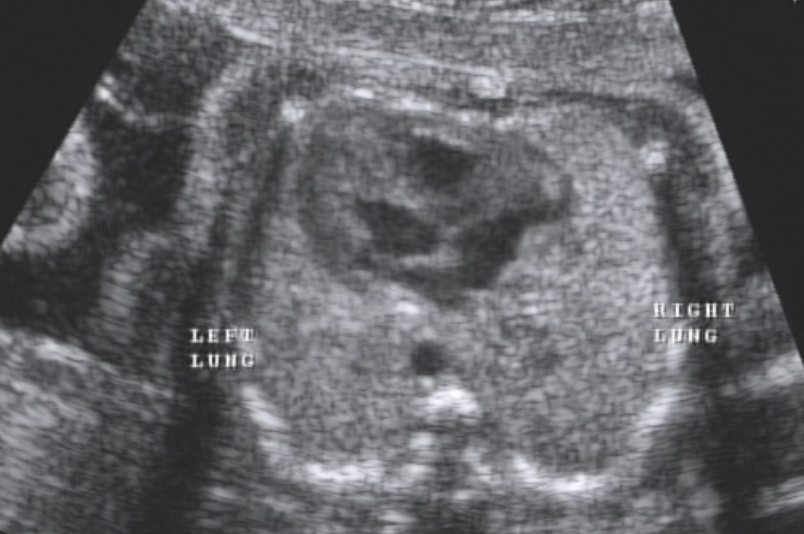
Lungs U/S appearance:
Symmetric & homogenous
Early in fetal life lungs echogenicity ≤ to the liver
Later in pregnancy lungs echogenicity ≥ to the liver
by volume : right lung is slightly larger than the left
Ultrasound cannot determine lung maturity
Fetal breathing does not indicate lung maturity
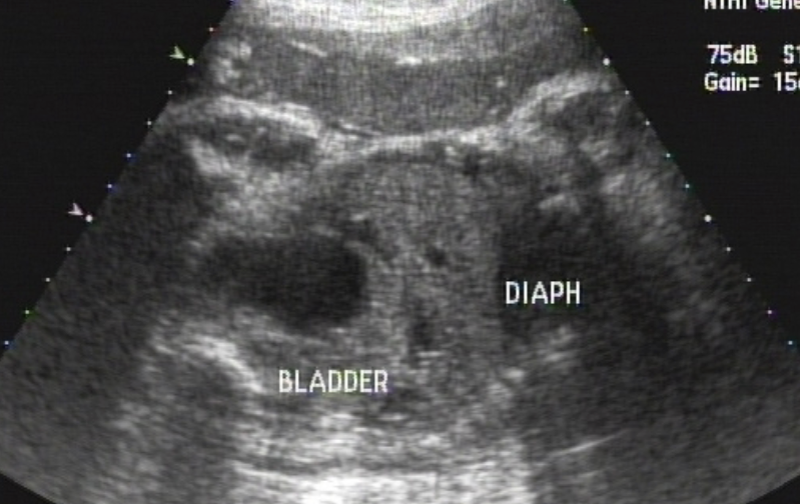
Diaphragm
Muscle that separates the chest from the abdomen
Fetal heart and lungs should be visualized superior to the diaphragm
Fetal stomach, liver, and bowel should be below the diaphragm
Appears as hypoechoic band between heart and stomach in the longitudinal and coronal planes

Abdomen
Superior border is the diaphragm
Identify stomach, liver, kidneys, adrenal glands, gallbladder, bowel, cord insertion, bladder, and genitalia
Spleen and pancreas are not routinely imaged and can be difficult to identify
Stomach
Anechoic stomach “bubble” should be positioned on the left side of the abdomen
Check for single “bubble”
Non-visualization of the stomach, especially in the presence of polyhydramnios may indicate abnormality
If the stomach is still not visualized at the end of the scan, the exam should be repeated in 30 minutes
Echogenicities or debris may be visualized within the stomach and are normal - usually vernix

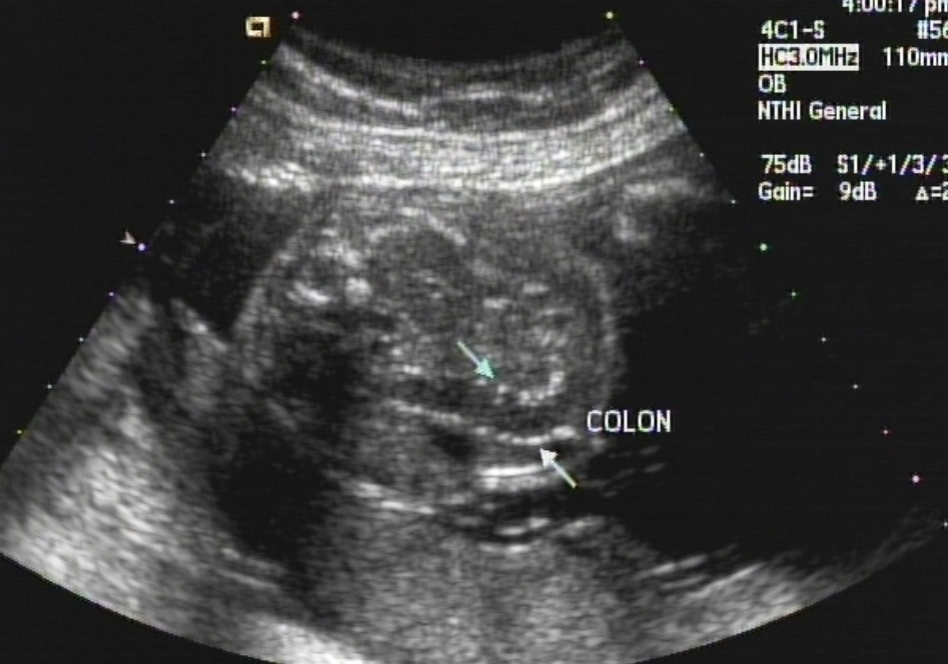
Bowel
Bowel appears somewhat echogenic
After 20 weeks the large and small intestines may be distinguished
Colon can be seen most commonly in the 3rd trimester
Small bowel should not exceed 6-7 mm
Colon should not exceed 23 mm
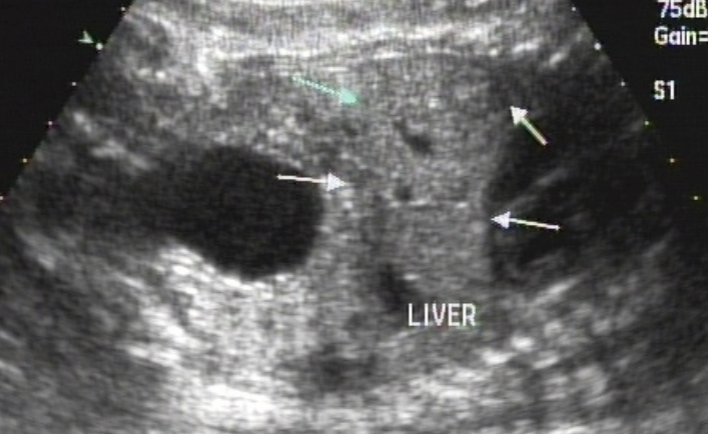
Liver
Large compared to other abdominal organs
10% of fetal weight at 11 weeks
5% at term
Located in the RUQ
Homogeneous echotexture
Gallbladder
Should be visualized after 20 weeks
Tear-drop shaped
Anechoic
Located in the RUQ
Passive in fetal life but can develop stones

Pancreas
Difficult to visualize due to lack of fatty tissue therefore it is not routinely imaged
Echogenicity slightly more than the liver
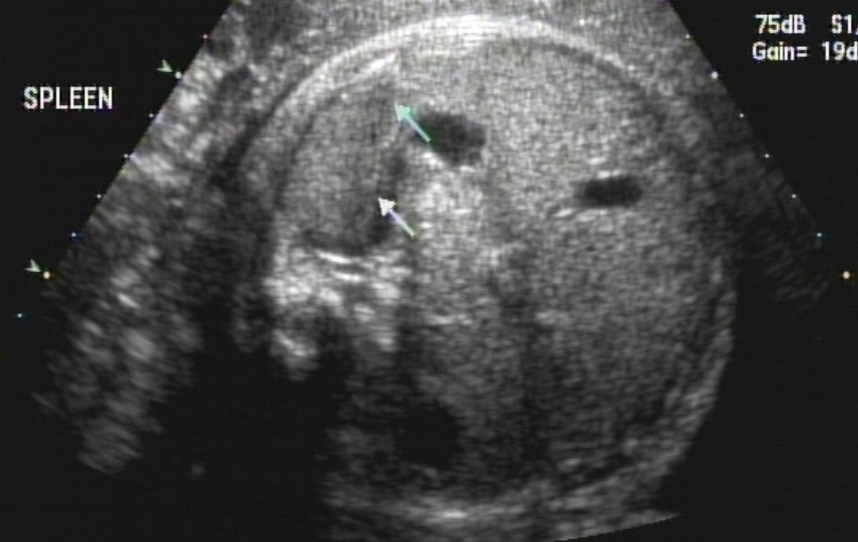
Spleen
DIfficult to image - Not routinely imaged, but can be visualized after 18 weeks
Homogeneous texture similar to the kidneys, less echogenic than the liver
best imaged in the transverse plane
posterior and to the left of the fetal stomach
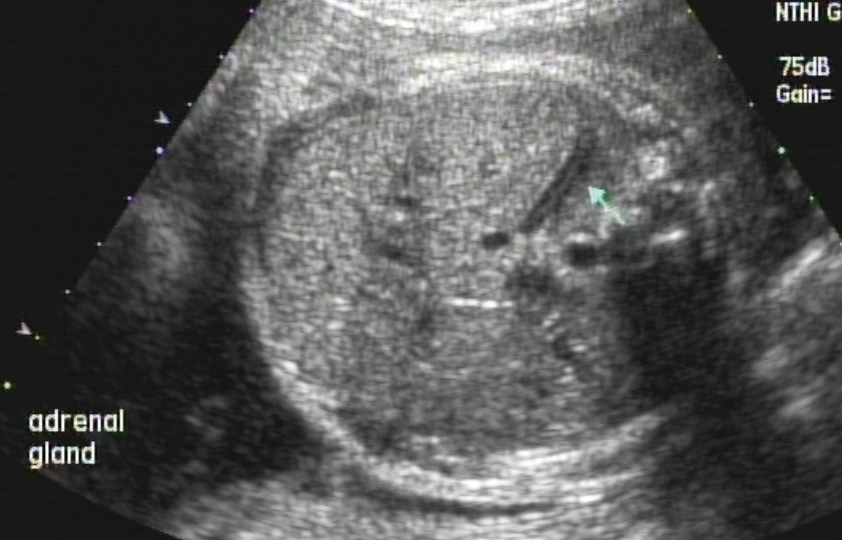
Adrenal Glands
Elongated oval to triangle shaped structures superior to the kidneys
Hypoechoic rim with echogenic center “stripe”
Seen as a “cap” of the superior pole of the kidney
Can be included in the abdominal circumference or APD / AD measurements
Kidneys
Paired hypoechoic structures located on either side of the spine
Can be imaged in sagittal plane as well - appear bean shaped
Can be imaged as early as 12 weeks
Renal pelvis can be visualized - anechoic
Ureters not usually visualized unless abnormality is present

Renal to Abdominal Circumference ratio should be:
0.30 throughout pregnancy
Renal Pelvis
Up to 20 weeks = 5mm or less
20-30 weeks =8 mm or less
30 weeks to term = 10 mm or less
Abdominal Cord Insertion
Vessels can be visualized as they enter fetal abdomen
assess w/ color and 2D
2 arteries and 1 vein (Mickey Mouse Sign)
Be sure both arteries can be visualized coursing around fetal bladder (confirms 3vc)
Be sure abdominal wall is intact at the area of the cord insertion

Bladder
Visualized in lower pelvis
Anechoic
Fetus urinates approx. 1-2 times per hour
If bladder is not visualized throughout exam, repeat in 20-30 min
if bladder cannot be visualized and there is oligo/anhydramnios → most likely kidney anomaly
Male Anatomy
“Turtle” sign
Penis and scrotum can be visualized
Testes descend by 32 weeks
Hydroceles are common

Female Anatomy
“Hamburger” sign
3 lines → labia majora with central labia minora

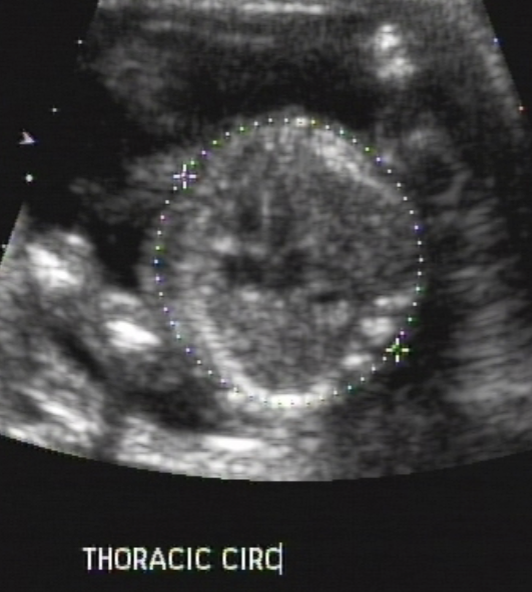
Thoracic Circumference
Measured at the level of the 4 chamber heart
Compared to Abdominal Circumference to evaluate fetus for pulmonary hypoplasia
TC/AC ratio should = 0.89 throughout pregnancy
Not a routine measurement
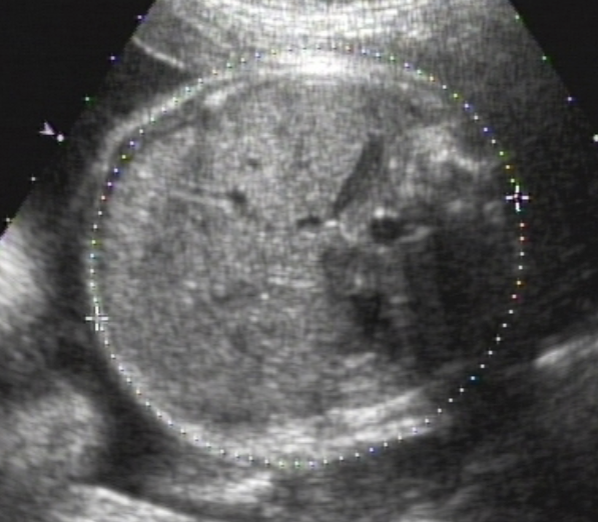
Abdominal Circumference (AC)
Routine measurement to calculate EGA / EFW
Transverse plane
Landmarks:
Umbilical Vein
Stomach
Adrenal glands (may/may not be in image)
DO NOT include lungs or kidneys in image
Be on axis → round abdomen without “off axis” ribs
Anterior to Posterior Diameter (APD)
Measured from outer edge of skin to outer edge of skin from transverse spine to anterior abdominal wall through J-hook
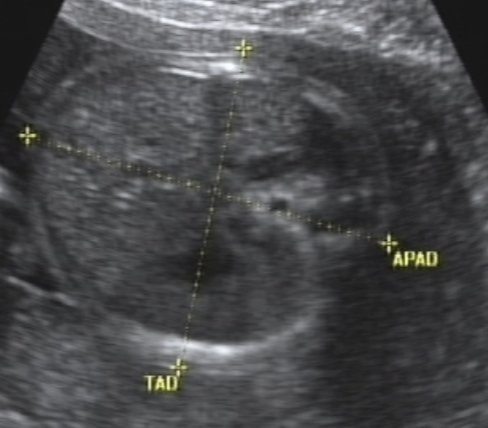
Transverse Abdominal Distance (TAD)
Measured from outer edge of abdominal skin at 90° angle to APD line
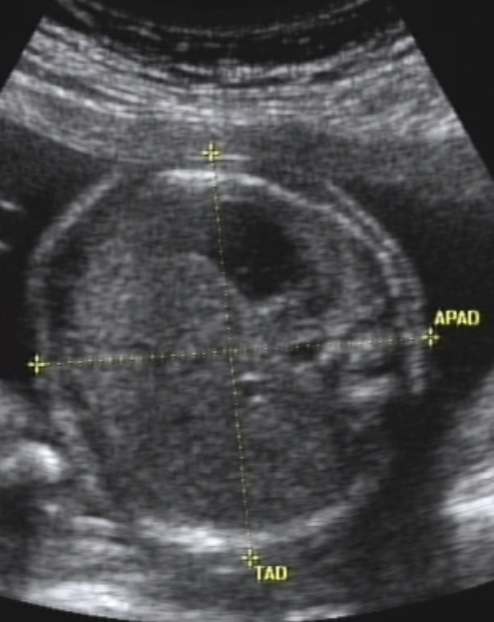
AC can be calculated by:
AC = APD + TAD x 1.57