Mature T cell lymphoma\leukemia
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
Classic presentation of T-PLL?
Remember: “5 S’s”
Severe leukocytosis
Splenomegaly (hepatosplenomegaly)
Skin lesions
Swollen lymph nodes (lymphadenopathy)
Serous effusions
Most common extramedullary site of T-PLL?
✅ Skin
Dermal infiltrate
Predominantly perivascular
No epidermotropism
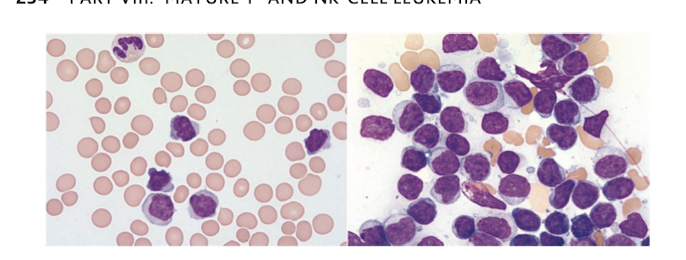
Peripheral blood morphology in T-PLL?
A:
Medium-sized prolymphocytes
Condensed chromatin
Single prominent nucleolus
Basophilic cytoplasm
Cytoplasmic blebs
Characteristic immunophenotype of T-PLL?
✅ CD2+
✅ CD3+
✅ CD5+
✅ CD7 (strong)
✅ CD52
✅ TCL1+
❌ TdT negative
Hallmark cytogenetic abnormality of T-PLL?
A:
✅ inv(14)(q11;q32)
Major diagnostic criteria for T-PLL?
A:
Need:
≥5 × 10⁹/L T-PLL cells
Clonal T-cell population
TCL1A/B or MTCP1 abnormality
What is the first-line treatment for T-PLL?
A:
✅ Alemtuzumab (anti-CD52) ( IV over SC)
Which infection prophylaxis is mandatory during alemtuzumab?
A:
PCP prophylaxis
Herpesvirus prophylaxis
Weekly CMV monitoring
Only curative treatment for T-PLL?
.
A:
✅ Allogeneic hematopoietic stem cell transplantation
Should be offered in first remission to eligible patients
vTreatment options for relapsed T-PLL?
A:
Repeat alemtuzumab (if remission >6 months)
Nelarabine
Bendamustine
Pentostatin
Alemtuzumab + pentostatin
FMC-A
Ibrutinib + venetocla
Most common mutation in T-LGLL?
STAT3 (28–75%)
Classic immunophenotype of T-LGLL?
Back
CD3+
CD8+
CD57+
CD16+
TIA-1+
Granzyme B+
Dim CD5/CD7
CD56−
CD28
Most common indication for treatment?
Severe neutropenia (ANC <0.5 ×10⁹/L) with recurrent infections
First-line drugs for T-LGLL?
Methotrexate
Cyclophosphamide
Cyclosporine
A 67-year-old woman with long-standing rheumatoid arthritis presents with recurrent bacterial sinus infections. CBC shows Hb 10.8 g/dL, ANC 0.3 ×10⁹/L, lymphocytes 5.5 ×10⁹/L. Flow cytometry reveals CD3+, CD8+, CD57+, CD16+, dim CD5 expression. Which molecular abnormality is most commonly associated with this disorder?
A. BRAF V600E
B. STAT3 mutation
C. JAK2 V617F
D. MYD88 mutation
E. TP53 deletion
Answer: B. STAT3 mutation
Explanation: STAT3 gain-of-function mutations are found in 28–75% of T-LGLL and drive constitutive JAK/STAT signaling. The other mutations are characteristic of different hematologic malignancie
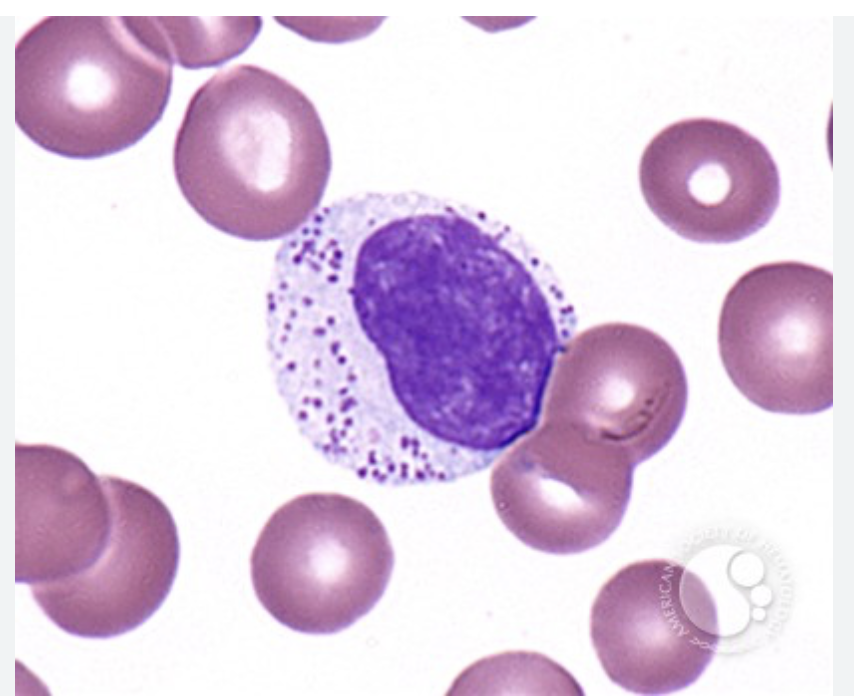
spot diagnosis?
T LGLL
Which virus is classically associated with ANKCL?
Epstein-Barr virus (EBV).
Which immunophenotype is characteristic of ANKCL
CD2+
CD56+
Cytoplasmic CD3ε+
Surface CD3−
Granzyme B+
Perforin+
TIA-1+
Q: What is the TCR configuration in ANKCL?
Germline (no TCR rearrangement).
Which mutation is most characteristic of ANKCL?
STAT3 mutation.
Which mutation favors ENKTL instead?
JAK3 mutation.
Preferred induction therapy ANKL?
L-asparaginase-based chemotherapy (Modified SMILE). followed by allo
Question 2
Which immunophenotype is most consistent with ANKCL?
A. Surface CD3+, CD5+, CD57+
B. CD19+, CD20+, CD79a+
C. CD2+, CD56+, cytoplasmic CD3ε+, surface CD3−
D. CD10+, BCL6+, CD20+
E. CD30+, ALK+
Answer: C