biomechanics final combined
1/591
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
592 Terms
[…]
Consists of three components.
Visual Observation.
Qualitative Assessment.
Biomechanical Analysis.
GAIT ANALYSIS
OBJECT OF GAIT ANALYSIS
Visually observe the […].
Start from [body area] and work your way down to […].
Attempt to observe motion in each of the three planes.
Sometimes easier said than done.
gait cycle
head
Feet
STEP ONE THE HEAD
Primarily observe in the [plane].
Should be […] (straight up and down)
Look for tilt to either side.
Tilt could indicate problem with extraocular muscles, scoliosis, neurologic deficit, degenerative joint disease, or neuromuscular disease.
Could also indicate a bony limb length discrepancy. The head will tilt toward the short side when compensated, toward the long side when uncompensated.
In a functional limb length discrepancy - where one foot is more pronated than the other the head will tilt toward the pronated side.
frontal plane
rectus
STEP ONE THE HEAD
Primarily observe in the frontal plane.
Should be rectus (straight up and down)
Look for tilt to either side.
Tilt could indicate problem with […], scoliosis, […], degenerative joint disease, or neuromuscular disease.
Could also indicate a bony […]. The head will tilt toward the short side when compensated, toward the long side when uncompensated.
In a functional limb length discrepancy - where one foot is more pronated than the other the head will tilt toward the pronated side.
extraocular muscles
neurologic deficit
limb length discrepancy

RECTUS HEAD

FRONTAL PLANE TILT
STEP ONE THE HEAD
Observations in the [plane] is difficult.
Observation in the [plane] plane made from the side.
Look for tilt either forward or backward.
May indicate […] problem such as kyphosis.
Also, look for abnormal motion or lack of neck control. Could indicate neurologic problems.
transverse
sagittal
postural

SAGITTAL PLANE HEAD TILT
STEP TWO THE SHOULDERS
Observation in the [plane].
Shoulders should be even, or parallel to the [plane].
Look for tilt in the frontal plane.
May indicate postural problem such as […] or possibly a bony or functional limb length discrepancy.
Again the shoulders will tilt toward the shorter side.
frontal
transverse
scoliosis

RECTUS SHOULDERS
STEP TWO THE SHOULDERS
Observation in the [plane].
Shoulders should be even. Not slumped forward.
Indicates poor posture or a possible […].
sagittal
kyphosis

SHOULDER TILT
STEP TWO THE SHOULDERS
Observation in the [plane].
Shoulders should be rotating the same as the [contralateral or ipsilateral] hip.
In english, if right hip is internally rotated leading to heel contact, left shoulder should be internally rotated.
The opposite would be true for left hip and right shoulder.
transverse
contralateral
STEP THREE ARM SWING
Observation in the [plane].
Arm swing should be [asymmetrical or symmetrical].
One arm should not swing differently than the other.
Such as one arm swinging out wider than the opposite arm or circumducting.
May indicate […], or possible […].
frontal
symmetrical
balance problem
neurologic manifestation
STEP THREE ARM SWING
Observation in the [plane].
Arm swing should be symmetrical.
One arm should not swing differently than the other.
Such as one arm swinging out farther forward than the opposite arm.
Normal arm swing is 2/3 anterior to a line representing the frontal plane passing through the body and 1/3 posterior to the frontal plane line.
sagittal
STEP THREE ARM SWING
Observation in the transverse plane. Arm swing should be symmetrical.
One arm should not swing differently than the other. Such as one arm swinging out farther forward than the opposite arm.
Again circumduction of one arm greater then the opposite arm should […].
not be observed
STEP THREE ARM SWING
Normal arm swing is the same as the fore mentioned […]
As right leg extends for heel contact, left arm should swing forward.
The opposite is true for left leg and right arm motion.
hip rotation, shoulder rotation.
STEP THREE ARM SWING
If excessive arm swing is seen in the sagittal plane then it is a […] for decreased motion in the trunk, hips, knee, lower leg, or the foot.
If decreased arm swing is seen in the sagittal plane then it is a compensation for […] motion in the trunk, hips, knee, lower leg, or the foot.
compensation
excessive
STEP FOUR PELVIS AND TRUNK ROTATION
They should exhibit [symmetrical or asymmetrical] rotation during the gait cycle in all planes.
[symmetrical or asymmetrical] rotation may indicate a variance in the normal weight transfer sequence.
eg.: abnormal propulsive subtalar joint pronation.
symmetrical
Asymmetrical

PELVIC AND SHOULD ROTATION
STEP FOUR PELVIS AND TRUNK ROTATION
The [bony prominance] should be equal and level with one another on the frontal plane.
A difference in the levels of the iliac crests could indicate a […]
iliac crests
limb length discrepancy.

PELVIC TILT IN FRONTAL AND SAGITTAL PLANES
STEP FIVE THE KNEE
The [bone] should be internally rotated during the first […] of the stance phase of gait.
It should then externally rotate until it is straight ahead during midstance.
The patella will then continue to externally rotate throughout the propulsive period.
The patella follows the lower limb in rotating.
patella
25%
STEP FIVE THE KNEE
The patella should be internally rotated during the first 25% of the stance phase of gait.
It should then [externally or internally] rotate until it is straight ahead during midstance.
The patella will then continue to externally rotate throughout the [gait period].
The patella follows the lower limb in rotating.
externally
propulsive period
STEP FIVE THE KNEE
On the transverse plane if the knee is [internally or externally] rotated may indicate tight medial musculature or internal femoral position.
Likewise, if the knee is externally rotated this may indicate tight lateral musculature or external femoral position.
eg.: if the medial hamstrings are tight the knee will deviate medially just prior to heel contact.
internally
STEP FIVE THE KNEE
On the frontal plane if the knees are adducted relative to the thighs or "knock kneed", this is known as […].
This is frequently associated with […], a more horizontal attitude of the femoral head and neck.
Or, the femurs are in a varus attitude causing the knees to be positioned closer together.
genu valgum
coxa vara
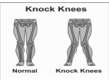
GENU VALGUM
STEP FIVE THE KNEE
On the frontal plane if the knees are abducted relative to the thighs or […]", this is known as […].
This is frequently associated with coxa valga, a more vertical orientation of the femoral head and neck.
Or, the femurs are in a valgus attitude causing the knees to be positioned farther apart.
"bow legged’’
genu varum
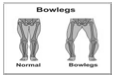
GENU VARUM
STEP FIVE THE KNEE
On the sagittal plane if the knees are […] we refer to this as genu […].
In this sagittal plane deformity the leg forms a [forward or backward] facing concavity.
This deformity may be observed in static stance as well as gait.
Very frequently seen when equinas (tight gastrocnemius group).
hyperextended
recurvatum
forward

GENU RECURVATUM
STEP SIX
ANGLE AND BASE OF GAIT
Normal angle of gait is between […°] and […°]abducted from the line of progression.
8-15°

ANGLE OF GAIT
STEP SIX ANGLE AND BASE OF GAIT
Normal base of gait is around […] and […] inches between the medial malleoli.
An excessively wide base of gait may be associated with diminished […] or […] function.
1-1.5
proprioceptive or vestibular

BASE OF GAIT
STEP SEVEN THE FOOT DURING GAIT
The position and motion of the [joint] should be observed during contact, midstance, and the propulsive periods of the stance phase of gait.
The motion of the [bone] in the frontal plane is used as a gauge of subtalar joint motion.
A vertical bisection of the calcaneus is the best reference when attempting to observe this.
subtalar
calcaneus
STEP SEVEN THE FOOT DURING GAIT
At the start of contact period the calcaneus should be slightly [inverted or everted], indicating a slightly supinated subtalar joint position.
inverted
STEP SEVEN THE FOOT DURING GAIT
During the […] period the subtalar joint should be pronating to absorb shock of heel contact.
contact
STEP SEVEN THE FOOT DURING GAIT
During the […] period the subtalar joint should be supinating to and continue supinating through propulsion.
The subtalar joint should reach its neutral position just before the end of the […] period.
However, before reaching the end of midstance the subtalar joint is still in a […] position.
midstance
midstance
pronated
STEP SEVEN THE FOOT DURING GAIT
Once the foot has passed through its neutral position at the end of midstance the subtalar joint enters into a [supinated or pronated] position, which is reflected by the calcaneus being [inverted or everted].
The subtalar joint continues to supinate until just before toe off.
supinated
inverted
STEP SEVEN THE FOOT DURING GAIT
On the transverse plane the patient should be observed at toe off for an [abduction or adduction] twist of the foot.
The calcaneus swings in on the transverse plane.
This is not normal and may be seen in […].
This also may be seen in patients with […] if there is sudden pronation just prior to toe off.
abductory
equinas
forefoot valgus
STEP SEVEN THE FOOT DURING GAIT
On the transverse plane the [joint] should be observed.
The lateral border of the forefoot will appear abducted on the [forefoot or rearfoot] if the midtarsal joint is in a pronated position.
Conversely, the lateral aspect of the forefoot will appear adducted on the rearfoot giving a C shape to the foot if the midtarsal joint is in a supinated position.
midtarsal joint
rearfoot

ADDUCTED FOREFOOT ON REARFOOT
ABDUCTED FOREFOOT ON THE REARFOOT
STEP SEVEN THE FOOT DURING GAIT
On the sagittal plane the midtarsal joint should be observed.
With abnormal subtalar joint [Pronation or supination] a sagittal plane subluxation can occur at the midtarsal joint at the end of midstance and during the propulsive phase of gait.
This is caused by the rearfoot flexing over the forefoot due to the loss of the rigid lever.
This is known as a "[…]".
pronation
midtarsal joint break

midtarsal joint break
STEP SEVEN
THE FOOT DURING GAIT
Lastly, the examiner will want to assess if the patients gait is
[…] or […].
In a propulsive gait the patient will have a flexing of the metatarsophalangeal joints during propulsion.
This can also be demonstrated by a blanching of the digits.
propulsive
apropulsive
STEP SEVEN THE FOOT DURING GAIT
If the gait is [propulsive or apropulsive], the patient will have no flexing of the metatarsophalangeal joints during propulsion.
This can also be demonstrated by a lack of […] of the digits during propulsion.
apropulsive
blanching
CONCLUSION IDEAL CONDITIONS
Well lit area long enough for patient to ambulate normally.
Unobstructed view of patients head, shoulders, torso, hips, knees, and feet.
Patient in bathing suit.
Reality: you will have difficulty doing this in your office. Have patient in […] and do the best you can.
At the minimum you need an unobstructed view of the patients […]
shorts
feet and ankles.
ARTHROMETRIC EXAMINATION Instruments for Orthopedic Evaluation
…
…
…
…
Gravity Goniometer.
Forefoot Measuring Device.
Orthopedic Evaluation Device.
Tractograph
ARTHROMETRIC EXAMINATION
Gravity Goniometer
Best for measuring […] leg deviation and malleolar position.
Consists of arms like tongs which are adjustable.
A 360 degree compass with a free swinging needle at the center.
Can be attached to a stationary base.
frontal plane

ARTHROMETRIC EXAMINATION Gravity Goniometer
Best for measuring frontal plane leg deviation and malleolar position.
Consists of arms like tongs which are adjustable.
A […] with a free swinging needle at the center.
Can be attached to a stationary base.
360 degree compass

Forefoot Measuring Device
Best for measuring […] relationship.
Consists of half a compass with attachment to a handle.
A 180 degree compass with an area at the posterior to bisect the calcaneus.
Not commonly used.
forefoot to rearfoot

ARTHROMETRIC EXAMINATION Forefoot Measuring Device
Best for measuring forefoot to rearfoot relationship.
Consists of half a compass with attachment to a handle.
A […] with an area at the posterior to bisect the calcaneus.
Not commonly used.
180 degree compass

Orthopedic Evaluation Device (O.E.D)
Best for measuring […]. Can be used for all measurements.
Consists of a clear rectangle of plexiglass with a half compass attached.
Plexiglass has a line etched along the long border.
Center of compass is centered along this etched line.
Compass should rotate freely.
everything

Orthopedic Evaluation Device (O.E.D)
Best for measuring everything. Can be used for all measurements.
Consists of a clear rectangle of plexiglass with a half compass attached.
Plexiglass has a line etched along the long border.
Center of compass is centered along this etched line.
Compass should […].
rotate freely
Tractograph
Can be used for […]
Can be used for […]
Can be used for […]
Joint ROM
Rearfoot ROM
Forefoot to rearfoot relationship

Ranges of Motion - Interphalangeal Joint
Motion available is […] and […].
Normal motion is plantarflexion from a fully extended position.
Any dorsilfexion from a fully extended position is abnormal but not pathological.
The minimum amount of plantarflexion required is not known.
When examining [joint] assess that plantarflexion from a fully
extended position is occurring.
dorsiflexion and plantarflexion
IPJ
Ranges of Motion - Interphalangeal Joint
Motion available is dorsiflexion and plantarflexion.
Normal motion is […] from a fully extended position.
Any […] from a fully extended position is abnormal but not pathological.
The minimum amount of plantarflexion required is […].
When examining IPJ assess that plantarflexion from a fully extended position is occurring.
plantarflexion
dorsilfexion
not known
Ranges of Motion - Metatarsalphalangeal Joint
Provide motion in the [what plane] and [what plane] planes.
Motion needed in the 1st MPJ is 65 degrees or greater, for propulsion.
Motion needed in the lesser MPJ's is slightly less than the 65 degrees required at the first MPJ.
Motion is assessed by dorsiflexing the digit on the corresponding metatarsal. Bisect the metatarsal shaft and the shaft of the digit being assessed.
The first MPJ is the easiest to assess and the one commonly assessed.
MPJ is the center for motion.
transverse
sagittal
Ranges of Motion - Metatarsalphalangeal Joint
Provide motion in the transverse and sagittal planes.
Motion needed in the 1st MPJ is […] degrees or greater, for propulsion.
Motion needed in the lesser MPJ's is slightly [more or less] than the 65 degrees required at the first MPJ.
Motion is assessed by dorsiflexing the digit on the corresponding metatarsal. Bisect the metatarsal shaft and the shaft of the digit being assessed.
The first MPJ is the easiest to assess and the one commonly assessed.
MPJ is the center for motion.
65
less
Ranges of Motion - Metatarsalphalangeal Joint
Provide motion in the transverse and sagittal planes.
Motion needed in the 1st MPJ is 65 degrees or greater, for propulsion.
Motion needed in the lesser MPJ's is slightly less than the 65 degrees required at the first MPJ.
Motion is assessed by […] the digit on the corresponding metatarsal. Bisect the metatarsal shaft and the shaft of the digit being assessed.
The first MPJ is the easiest to assess and the one commonly assessed.
MPJ is the […].
dorsiflexing
center for motion
Ranges of Motion - 1st Ray
Consists of the […] and […].
Axis angulates approximately 45 degrees from the frontal and sagittal planes and only slightly from the transverse plane.
Motion occurs in three planes simultaneously with dorsiflexion and plantarflexion being the primary motions.
Dorsiflexion is accompanied by inversion and plantarflexion is accompanied by eversion.
Motion will either dorsiflex or plantarflex the first metatarsal head above or below the second metatarsal head. Normally there is equal dorsiflexion and plantarflexion.
first cuneiform
first metatarsal
Ranges of Motion - 1st Ray
Consists of the first cuneiform and first metatarsal.
Axis angulates approximately […] degrees from the frontal and sagittal planes and only slightly from the transverse plane.
Motion occurs in three planes simultaneously with […] and […] being the primary motions.
Dorsiflexion is accompanied by inversion and plantarflexion is accompanied by eversion.
Motion will either dorsiflex or plantarflex the first metatarsal head above or below the second metatarsal head. Normally there is equal dorsiflexion and plantarflexion.
45
dorsiflexion
plantarflexion
Ranges of Motion - 1st Ray
Consists of the first cuneiform and first metatarsal.
Axis angulates approximately 45 degrees from the frontal and sagittal planes and only slightly from the transverse plane.
Motion occurs in three planes simultaneously with dorsiflexion and plantarflexion being the primary motions.
Dorsiflexion is accompanied by [inversion or eversion] and plantarflexion is accompanied by [inversion or eversion].
Motion will either dorsiflex or plantarflex the first metatarsal head above or below the second metatarsal head. Normally there is […]dorsiflexion and plantarflexion.
inversion
eversion
equal
Ranges of Motion - 1st Ray
[pronation or supination] of the STJ will [increase or decrease] first ray ROM. Supination will decrease first ray ROM.
Best way to assess is to place the STJ in […] with the midtarsal joint [pronated or supinated]. This will allow for consistant measurements for both feet.
To examine, hold the second through fifth metatarsal heads between the thumb and forefinger of one hand. Thumb plantar. With the thumb and forefinger of the opposite hand hold the first metatarsal head. In the neutral position the fingers on the first metatarsal head will be slightly higher and lower due to the first metatarsal heads increased thickness to the second metatarsal head.
Pronation
increase
neutral
pronated
Ranges of Motion - 1st Ray
Compare position of the fingernails of either the thumbs or the forefingers. If they are at [equal or unequal] levels the 1st ray is neutral.
Dorsiflex the first metatarsal head maximally without causing motion of the subtalar or midtarsal joints. Then plantarflex the first metatarsal head [maximally or minamally].
If the amount of motion is equal the first ray ROM is [normal or abnormal].
If plantarflexion exceeds dorsiflexion the it indicates […].
If dorsiflexion exceeds plantarflexion it indicates […].
equal
maximally
normal
plantarflexed first ray deformity
dorsiflexed first ray deformity
First Ray ROM exam technique

First Ray ROM exam

First Ray ROM

Dorsiflexed First Ray

Plantarflexed First Ray

Ranges of Motion - [joint]
Oblique axis produces dorsiflexion and abduction (with pronation) and plantarflexion and adduction (with supination). This is forefoot in relation to rearfoot motion.
The Longitudenal axis produces inversion and eversion of the forefoot on the rearfoot.
Subtalar joint supination decreases the total range of motion at the midtarsal joint in both supination and pronation.
Subtalar joint pronation increases the total range of motion at the midtarsal joint in both supination and pronation.
Total range of motion of the midtarsal joint depends on subtalar joint position. 4 to 6 degrees of motion is needed about the longitudenal axis to compensate for calcaneal eversion.
Remember: minimum amount of eversion of the calcaneus with STJ pronation for normal function is 4-6 degrees!
Midtarsal Joint
Ranges of Motion - Midtarsal Joint
Oblique axis produces dorsiflexion and abduction (with pronation) and plantarflexion and adduction (with supination). This is forefoot in relation to rearfoot motion.
The Longitudenal axis produces inversion and eversion of the forefoot on the rearfoot.
Subtalar joint supination decreases the total range of motion at the midtarsal joint in both supination and pronation.
Subtalar joint pronation [increase or decrease] the total range of motion at the [joint] in both supination and pronation.
Total range of motion of the midtarsal joint depends on subtalar joint position. […] to […] degrees of motion is needed about the [what axis] to compensate for calcaneal eversion.
Remember: minimum amount of eversion of the calcaneus with STJ pronation for normal function is 4-6 degrees!
increases
midtarsal joint
4 to 6
longitudenal axis
Ranges of Motion - Midtarsal Joint
[what axis] produces dorsiflexion and abduction (with pronation) and plantarflexion and adduction (with supination). This is forefoot in relation to rearfoot motion.
The [what axis] produces inversion and eversion of the forefoot on the rearfoot.
Subtalar joint supination [increases or decreases] the total range of motion at the midtarsal joint in both supination and pronation.
Subtalar joint pronation increases the total range of motion at the midtarsal joint in both supination and pronation.
Total range of motion of the midtarsal joint depends on subtalar joint position. 4 to 6 degrees of motion is needed about the longitudenal axis to compensate for calcaneal eversion.
Remember: minimum amount of eversion of the calcaneus with STJ pronation for normal function is 4-6 degrees!
Oblique axis
Longitudenal axis
decreases
Midtarsal Joint Range of Motion (ROM)

Ranges of Motion - [joint]
Motion occurs in three planes simultaneously.
Supination consists of inversion, adduction and plantarflexion.
Pronation consists of eversion, abduction and dorsiflexion.
Remember we visualize subtalar joint motion by viewing motion
of the calcaneus. Inversion of the calcaneus = supination,
eversion of the calcaneus = pronation.
A minimum of 4 to 6 degrees of calcaneal inversion with supination
and a minimum of 4 to 6 degrees of calcaneal eversion with
pronation are considered normal for locomotion. Total Minimum Range = 8 to 12 degrees of frontal plane motion at the subtalar joint.Normal STJ range of motion is cited to be twice as much inversion of the calcaneus with STJ supination than eversion of the calcaneus with STJ pronation.
A 2:1 ratio of inversion to eversion of the calcaneus.
Subtalar Joint
Ranges of Motion - Subtalar Joint
Motion occurs in […] planes simultaneously.
Supination consists of […], […] and […].
Pronation consists of […], […] and […].
Remember we visualize subtalar joint motion by viewing motion of the […]. Inversion of the calcaneus = supination, eversion of the calcaneus = pronation.
A minimum of 4 to 6 degrees of calcaneal inversion with supination
and a minimum of 4 to 6 degrees of calcaneal eversion with
pronation are considered normal for locomotion. Total Minimum Range = 8 to 12 degrees of frontal plane motion at the subtalar joint.Normal STJ range of motion is cited to be twice as much inversion of the calcaneus with STJ supination than eversion of the calcaneus with STJ pronation.
A 2:1 ratio of inversion to eversion of the calcaneus.
three
inversion, adduction and plantarflexion.
eversion, abduction and dorsiflexion.
calcaneus
Ranges of Motion - Subtalar Joint
Motion occurs in three planes simultaneously.
Supination consists of inversion, adduction and plantarflexion.
Pronation consists of eversion, abduction and dorsiflexion.
Remember we visualize subtalar joint motion by viewing motion of the calcaneus. Inversion of the calcaneus = supination, eversion of the calcaneus = pronation.
A minimum of […] degrees of calcaneal inversion with supination and a minimum of […] degrees of calcaneal eversion with pronation are considered normal for locomotion. Total Minimum Range = 8 to 12 degrees of frontal plane motion at the subtalar joint.
Normal STJ range of motion is cited to be [twice or half] as much inversion of the calcaneus with STJ supination than eversion of the calcaneus with STJ pronation.
A […] ratio of inversion to eversion of the calcaneus.
4 to 6
4 to 6
twice
2:1
Ranges of Motion - Subtalar Joint
Place patient [prone or supine]. This allows calcaneus to be viewed on the [ what plane].
Raise opposite hip either through a pillow or by having patient flex knee and rest their ankle on the knee of the leg you are examining.
Bisect the calcaneus and the lower 1/3 of the leg. By placing and abductory or adductory force on the forefoot you will invert and evert the calcaneus in relation to the leg.
Invert the calcaneus and measure how many degrees the calcaneus inverts to the leg. This is your inversion component.
Evert the calcaneus and measure how many degrees the calcaneus everts to the leg. This is your eversion component.
prone
frontal plane
Ranges of Motion - Subtalar Joint
Place patient prone. This allows calcaneus to be viewed on the frontal plane.
Raise opposite hip either through a pillow or by having patient flex knee and rest their ankle on the knee of the leg you are examining.
Bisect the […] and the lower […]. By placing and abductory or adductory force on the […] you will invert and evert the calcaneus in relation to the leg.
Invert the calcaneus and measure how many degrees the calcaneus inverts to the leg. This is your inversion component.
Evert the calcaneus and measure how many degrees the calcaneus everts to the leg. This is your eversion component.
calcaneus
1/3 of the leg
forefoot
STJ ROM Positioning

Heel Bisection

STJ Range of Motion (ROM)

Ranges of Motion - Ankle Joint
Primary motion occurring at the ankle joint is […] and […].
At least […] degrees of dorsiflexion is required in the normal ankle joint when the knee is extended and the subtalar joint is in neutral position. The midtarsal joint also is completely pronated. This according to Root.
Place patient prone. Put knee on the frontal plane as you did with the subtalar joint.
Passively dorsiflex the foot on the leg while keeping the subtalar joint neutral. It is very important that the subtalar joint is kept in neutral.
dorsiflexion
plantarflexion
10
Ranges of Motion - Ankle Joint
Primary motion occurring at the ankle joint is dorsiflexion and plantarflexion.
At least 10 degrees of dorsiflexion is required in the normal ankle joint when the knee is extended and the subtalar joint is in […] position. The [joint] also is completely pronated. This according to Root.
Place patient [prone or supine]. Put knee on the frontal plane as you did with the subtalar joint.
[passive or active] dorsiflex the foot on the leg while keeping the subtalar joint neutral. It is very important that the subtalar joint is kept in neutral.
neutral
midtarsal joint
prone
Passively
Ranges of Motion - Ankle Joint
Next ask the patient to [active or passive] dorsiflex the [medial or lateral] side of the foot. The subtalar joint must still be maintained in its […] position. Patient can do this by contracting their [what muscle] muscle.
You now measure the angle formed by the plantar aspect of the foot and the distal lateral1/3 of the leg.
The plantar aspect of the foot extend from the plantar aspect of the calcaneus to the skin beneath the fifth metatarsal head.
The lower 1/3 of the leg extends from the musculotendinous junction of the triceps surae to just proximal to the lateral malleolus.
actively
medial
neutral
anterior tibialis
Ranges of Motion - Ankle Joint
Next ask the patient to actively dorsiflex the medial side of the foot. The subtalar joint must still be maintained in its neutral position. Patient can do this by contracting their anterior tibialis muscle.
You now measure the angle formed by the plantar aspect of the foot and the [what part of the leg] of the leg.
The [dorsal or plantar] aspect of the foot extend from the plantar aspect of the calcaneus to the skin beneath the fifth metatarsal head.
The lower 1/3 of the leg extends from the musculotendinous junction of the triceps surae to just proximal to the [bony prominence].
distal lateral1/3
plantar
lateral malleolus

How to grasp foot for Ankle Joint ROM

Ankle Joint Dorsiflexion and Plantarflexion

Measuring Ankle Joint Dorsiflexion

SilverskÖld Test
Ranges of Motion - Knee Joint
Knee joint under normal conditions should only move in […] and […].
Knee should have no [plane] or [plane] plane motion on examination.
Range of motion in the sagittal plane should be up to […] to […] degrees of flexion.
The knee should extend so that lower leg is in line with the upper leg or femur. Any further extension is abnormal.
As in genu recurvatum.
flexion
extension
frontal
transverse
120 to 130

Knee Joint Flexion
Ranges of Motion - Hip Joint
Hip joint motion occurs in the [plane] or […] and […] rotation.
Motion should be equal […] degrees internal and 45 degrees external rotation
Motion can be assessed with patient [supine or prone] and legs extended. Patient may also be supine with knees flexed with lower leg haning over the edge of the examining table.
Neutral position of the hip is calculated by taking both internal and external rotation measurements and subtracting 45 degrees from either internal or external component.
Example: 55 degrees external rotation, 35 degrees internal rotation. Neutral position 10 degrees external.
transverse plane
internal and external
45
supine

Hip Range of Motion Exam

Hip ROM – External Rotation

Hip ROM – Internal Rotation
Structural Positions - Locking of the Midtarsal Joint
Patient placed [supine or prone] on examining table.
Knee placed on the [plane].
Subtalar joint placed in neutral position.
A dorsiflexory force is applied to the […] of the fifth
metatarsal while the subtalar joint is maintained in neutral.
This loading maximally pronates the midtarsal joint thus locking it.The forefoot to rearfoot measurement can now be taken.
The bisection of the calcaneus being perpendicular to the
ground, place measuring device across the metatarsal heads and assess whether forefoot is inverted, everted or neutral to rearfoot.
prone
frontal plane
neck
Structural Positions - Locking of the Midtarsal Joint
Patient placed prone on examining table.
Knee placed on the frontal plane.
Subtalar joint placed in neutral position.
A dorsiflexory force is applied to the neck of the fifth
metatarsal while the subtalar joint is maintained in neutral.
This loading maximally pronates the midtarsal joint thus [locking or unlocking].The forefoot to rearfoot measurement can now be taken.
The bisection of the calcaneus being perpendicular to the ground, place measuring device across the metatarsal heads and assess whether forefoot is inverted, everted or neutral to rearfoot.
locking it