week 38 - uterine cancer and premalignant lesions
0.0(0)
Studied by 1 personCard Sorting
1/16
There's no tags or description
Looks like no tags are added yet.
Last updated 4:05 PM on 7/8/26
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
17 Terms
1
New cards
Endometrial cancer introduction
* It is the most common gynaecological tumour in developed countries
* it is not the only uterine corpus tumour but it is the most common
* 5th most common cancer in women
* Incidence is rising rising due to increase life expectancy and increase prevalence of obesity
* Occurs mainly in perimenopausal (transitional period, irregular menstruation, around 47 y/o) and postmenopausal (12 months of amenorrhoea and loss of ovarian follicular activity, around 51 y/o) women
90% are menopausal
Only a minority (< 5%) are diagnosed < 40 y/o, in these women, obesity as well as PCOS seem to play an important role in carcinogenesis
* Most commonly complain of abnormal uterine bleeding and are diagnosed at an early stage (unlike cervical cancer)
* Typically has a good prognosis if diagnosed early
* The main risk factors for the development of endometrial cancer are unopposed endogenous and exogenous oestrogen exposure (but dont postmenopausal women have less oestrogen==__???__==)
* 80% are adenocarcinomas (fact check\*\*\*)
* it is not the only uterine corpus tumour but it is the most common
* 5th most common cancer in women
* Incidence is rising rising due to increase life expectancy and increase prevalence of obesity
* Occurs mainly in perimenopausal (transitional period, irregular menstruation, around 47 y/o) and postmenopausal (12 months of amenorrhoea and loss of ovarian follicular activity, around 51 y/o) women
90% are menopausal
Only a minority (< 5%) are diagnosed < 40 y/o, in these women, obesity as well as PCOS seem to play an important role in carcinogenesis
* Most commonly complain of abnormal uterine bleeding and are diagnosed at an early stage (unlike cervical cancer)
* Typically has a good prognosis if diagnosed early
* The main risk factors for the development of endometrial cancer are unopposed endogenous and exogenous oestrogen exposure (but dont postmenopausal women have less oestrogen==__???__==)
* 80% are adenocarcinomas (fact check\*\*\*)
2
New cards
Most common stromal tumours
Endometrial stromal sarcomas and uterine leiomyosarcomes
But mesenchymal (stromal) tumours are rare and cover only 1% of uterine malignancies
Generally occur at a younger age
But mesenchymal (stromal) tumours are rare and cover only 1% of uterine malignancies
Generally occur at a younger age
3
New cards
Premalignancies of the endometrium
* Premalignancies of the endometrium can be divided into → low-grade endometrioid precursor lesions (eg. atypical hyperplasia (AH) or endometrial intraepithelial neoplasia (EN)) or into serous carcinoma in situ (= serous endometrial intraepithelial carcinoma (SEIC))
* AH/EIN:
* = architecturally and cytologically altered endometrial glands (complex, irregular crowded endometrial glands with minor cytological atypia, without confluent back-to-back or cribriform growth and without myometrial invasion)
* The nuclear atypia is distinct from the surrounding endometrium with rounding, enlargement and loss of polarity
* SEIC:
* = serous carcinoma colonising pre-existing endometrial glands without forming a tumour mass or without invasion of the endometrial stroma or the myometrium
* often occurs in polyps or in atrophic endometrium
* Associated with widespread extrauterine disease
* AH/EIN:
* = architecturally and cytologically altered endometrial glands (complex, irregular crowded endometrial glands with minor cytological atypia, without confluent back-to-back or cribriform growth and without myometrial invasion)
* The nuclear atypia is distinct from the surrounding endometrium with rounding, enlargement and loss of polarity
* SEIC:
* = serous carcinoma colonising pre-existing endometrial glands without forming a tumour mass or without invasion of the endometrial stroma or the myometrium
* often occurs in polyps or in atrophic endometrium
* Associated with widespread extrauterine disease
4
New cards
Endometrial malignancies
* subdivided into 6 histological categories → endometrioid, mucinous, serous, clear cell, undifferentiated/dedifferentiated carcinoma, and carcinosarcoma
* The tumour differentiation is expressed in grades
* Most endometrioid and mucinous tumours are low grade, and classified as well differentiated and moderately differentiated endometrial cancer (grade 1 and 2)
* 10-20% of endometrioid endometrial cancers are high grade and classified as poorly differentiated (grade 3)
* All serous, clear cell, un/dedifferentiated carcinoma and carcinosarcoma are poorly differentiated (grade 3)
* Also divided into type I and type II but its not used very much
* The tumour differentiation is expressed in grades
* Most endometrioid and mucinous tumours are low grade, and classified as well differentiated and moderately differentiated endometrial cancer (grade 1 and 2)
* 10-20% of endometrioid endometrial cancers are high grade and classified as poorly differentiated (grade 3)
* All serous, clear cell, un/dedifferentiated carcinoma and carcinosarcoma are poorly differentiated (grade 3)
* Also divided into type I and type II but its not used very much
5
New cards
Stromal malignancies
I’m not sure if i understood this right
\
* currently classified as metaplastic carcinomas and the sarcoma is considered to be derived from the carcinomatous component through epithelial-to-mesenchymal transition (transdifferentiation) resulting in a more aggressive biological behaviour and a worse disease specific survival compared with poorly differentiated endometrial cancers
* Leiomyosarcomas (LMS), Endometrial stroma sarcomas (ESS), undifferentiated uterine sarcoma and adenosarcoma are the most common stromal or mesenchymal malignancies in the uterine corpus
* LMS, accounting for 60 % of all uterine sarcomas, are malignant smooth muscle tumours
* Most arise de novo
* A history of pelvic irradiation may be a risk factor for LMS
* *ESS are divided into endometrial stromal nodule, low-grade endometrial stromal sarcoma (ESS) and high-grade ESS. Endometrial stromal nodules have identical histological features to low-grade ESS, but are limited to the endometrium without invasion and have an excellent outcome. High-grade ESSs are clinically more aggressive than low-grade ESSs, and typically harbour a different genetic profile*
* *Undifferentiated uterine sarcoma, previously called undifferentiated endometrial sarcoma, is a highly malignant neoplasm without any resemblance to endometrial stroma or smooth muscle*
\
* currently classified as metaplastic carcinomas and the sarcoma is considered to be derived from the carcinomatous component through epithelial-to-mesenchymal transition (transdifferentiation) resulting in a more aggressive biological behaviour and a worse disease specific survival compared with poorly differentiated endometrial cancers
* Leiomyosarcomas (LMS), Endometrial stroma sarcomas (ESS), undifferentiated uterine sarcoma and adenosarcoma are the most common stromal or mesenchymal malignancies in the uterine corpus
* LMS, accounting for 60 % of all uterine sarcomas, are malignant smooth muscle tumours
* Most arise de novo
* A history of pelvic irradiation may be a risk factor for LMS
* *ESS are divided into endometrial stromal nodule, low-grade endometrial stromal sarcoma (ESS) and high-grade ESS. Endometrial stromal nodules have identical histological features to low-grade ESS, but are limited to the endometrium without invasion and have an excellent outcome. High-grade ESSs are clinically more aggressive than low-grade ESSs, and typically harbour a different genetic profile*
* *Undifferentiated uterine sarcoma, previously called undifferentiated endometrial sarcoma, is a highly malignant neoplasm without any resemblance to endometrial stroma or smooth muscle*
6
New cards
Social determinants of uterine cancer
Genetics:
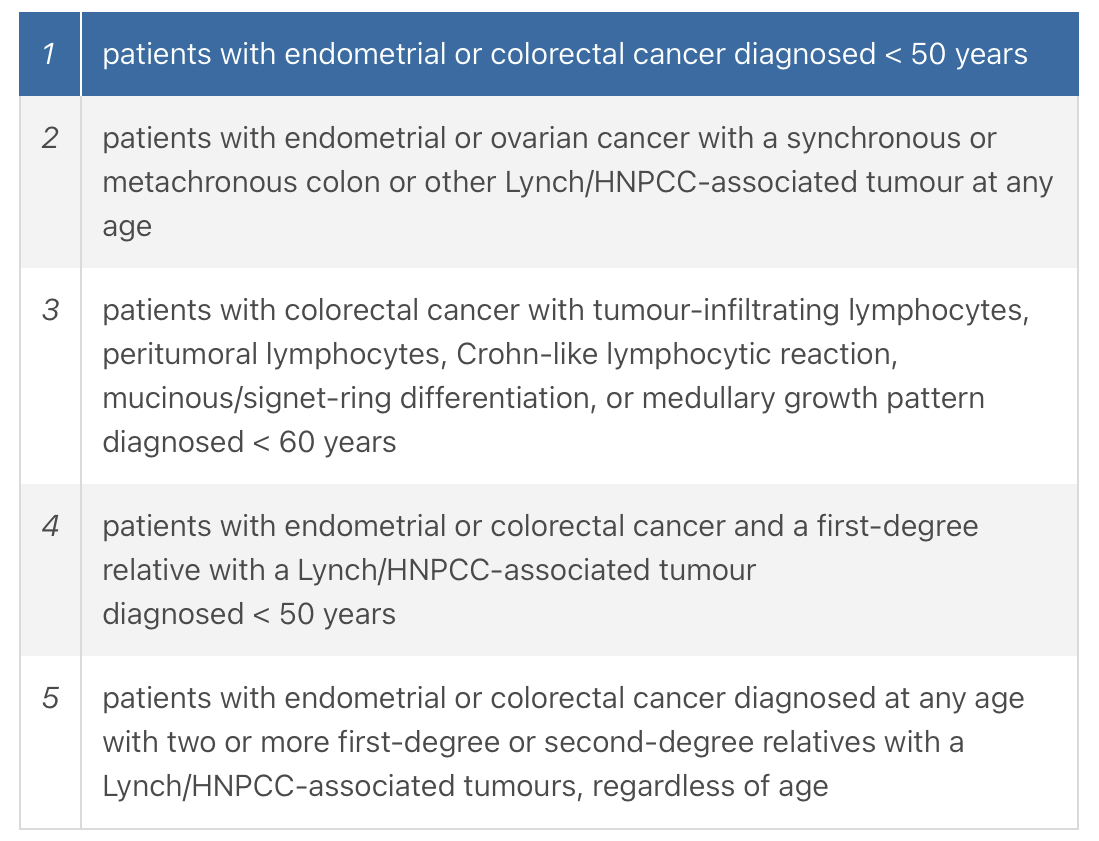
* 3 to 5% of uterine cancers are caused by genetic germ line mutations, mainly due to Lynch syndrome/hereditary nonpolyposis colorectal cancer (HNPCC)
* Lynch syndrome:
* autosomal dominant, mutations in the mismatch repair (MMR) genes (MLH1/2/6 and PMS2), risk of endometrial cancer is dependent on the affected gene (most common with MLH 1 or 6 mutations)
* Main risk is colorectal cancer but endometrial cancer is the 2nd most common malignancy with a lifetime risk of 25-70%
* Women with Lynch syndrome also have a lifetime risk of 4–24 % for ovarian cancer
* *Although the risk of Lynch syndrome in endometrial cancer patients is only about 3%, this is significantly higher in endometrial cancer diagnosed under the age of 50 (5-9%)*
* MMR testing is recommended for all women diagnosed with endometrial cancer under the age of 70 or with a history of other lynch associated malignancies (mainly colorectal)
* Cowden syndrome is rare but it is associated with an increased lifetime risk of endometrial cancer of 19-28% (also an increased risk for breast and thyroid cancer of 50% and 3-10% respectively)
\
Hormonal exposure:
* Endogenous oestrogen (produced in the follicles) exposure can be physiological (early menarche, nulliparity and late menopause) or due to endocrine abnormalities (eg. PCOS, obesity and diabetes)
* The main source of exogenous oestrogen exposure is hormonal replacement therapy, and tamoxifen
* Oestradiol (a type of oestrogen) has the most powerful oestrogenic activity (80x stronger than oestriol)
* The counter action of progesterone (produced in the corpus luteum) on endometrial proliferation is very important in healthy premenopausal women as it inhibits endometrial proliferation and alters the endometrium into a secretory phase
* Hormonal disturbances of this natural balance may influence endometrial proliferation and subsequently result in endometrial hyperplasia and/or endometrial cancer
\
Obesity:
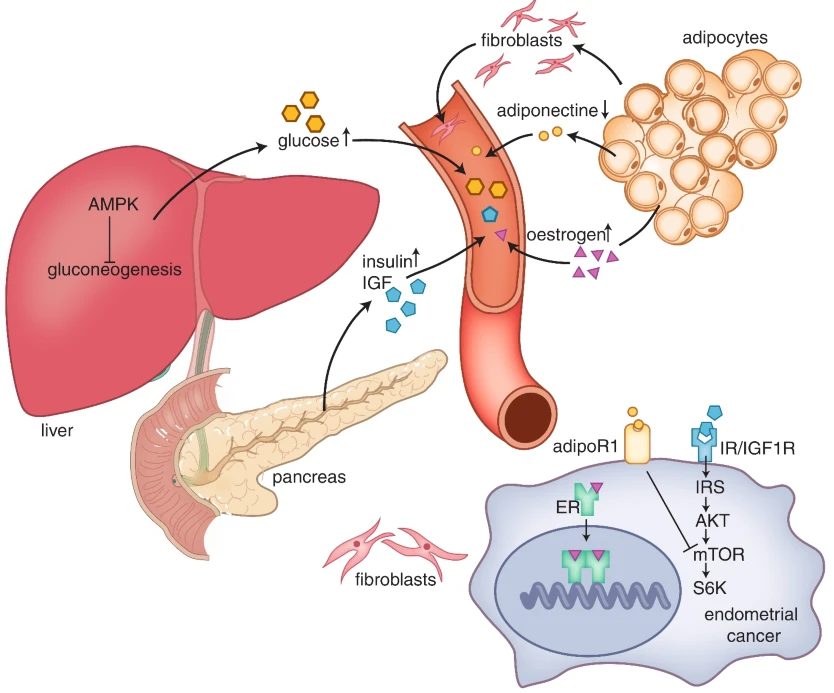
* strongly related to endometrial cancer, 57% of all endometrial cancers are attributed to overweight or obesity in the US
* The strong correlation of obesity and endometrial cancer is supported by the ‘dose-response’ relationship. With increasing body mass index (BMI), the risk of endometrial cancer is higher
* Prevalence of endometrial cancer is expected to rise due to the increase in obesity
* Several mechanisms:
1. production of adipokines in the adipocytes of the visceral fat tissue stimulates endometrial proliferation and tumorigenesis
\+ adipose tissue is a source of mesenchymal stem cells that support tumour growth and progression
2. Interaction of obesity with steroid production →
* premenopausal women → oestrogen is mainly produces in the endometrium which is counteracted by progesterone
* Postmenopausal women → adipose tissue is the main site of oestrogen (and im guessing also since progesterone isn’t produced it makes it worse?)
3. bioavailability of oestrogen is increased due to decreased levels of sex-hormone binding globulin as a consequence of the adiposity
* 3 to 5% of uterine cancers are caused by genetic germ line mutations, mainly due to Lynch syndrome/hereditary nonpolyposis colorectal cancer (HNPCC)
* Lynch syndrome:
* autosomal dominant, mutations in the mismatch repair (MMR) genes (MLH1/2/6 and PMS2), risk of endometrial cancer is dependent on the affected gene (most common with MLH 1 or 6 mutations)
* Main risk is colorectal cancer but endometrial cancer is the 2nd most common malignancy with a lifetime risk of 25-70%
* Women with Lynch syndrome also have a lifetime risk of 4–24 % for ovarian cancer
* *Although the risk of Lynch syndrome in endometrial cancer patients is only about 3%, this is significantly higher in endometrial cancer diagnosed under the age of 50 (5-9%)*
* MMR testing is recommended for all women diagnosed with endometrial cancer under the age of 70 or with a history of other lynch associated malignancies (mainly colorectal)
* Cowden syndrome is rare but it is associated with an increased lifetime risk of endometrial cancer of 19-28% (also an increased risk for breast and thyroid cancer of 50% and 3-10% respectively)
\
Hormonal exposure:
* Endogenous oestrogen (produced in the follicles) exposure can be physiological (early menarche, nulliparity and late menopause) or due to endocrine abnormalities (eg. PCOS, obesity and diabetes)
* The main source of exogenous oestrogen exposure is hormonal replacement therapy, and tamoxifen
* Oestradiol (a type of oestrogen) has the most powerful oestrogenic activity (80x stronger than oestriol)
* The counter action of progesterone (produced in the corpus luteum) on endometrial proliferation is very important in healthy premenopausal women as it inhibits endometrial proliferation and alters the endometrium into a secretory phase
* Hormonal disturbances of this natural balance may influence endometrial proliferation and subsequently result in endometrial hyperplasia and/or endometrial cancer
\
Obesity:
* strongly related to endometrial cancer, 57% of all endometrial cancers are attributed to overweight or obesity in the US
* The strong correlation of obesity and endometrial cancer is supported by the ‘dose-response’ relationship. With increasing body mass index (BMI), the risk of endometrial cancer is higher
* Prevalence of endometrial cancer is expected to rise due to the increase in obesity
* Several mechanisms:
1. production of adipokines in the adipocytes of the visceral fat tissue stimulates endometrial proliferation and tumorigenesis
\+ adipose tissue is a source of mesenchymal stem cells that support tumour growth and progression
2. Interaction of obesity with steroid production →
* premenopausal women → oestrogen is mainly produces in the endometrium which is counteracted by progesterone
* Postmenopausal women → adipose tissue is the main site of oestrogen (and im guessing also since progesterone isn’t produced it makes it worse?)
3. bioavailability of oestrogen is increased due to decreased levels of sex-hormone binding globulin as a consequence of the adiposity
7
New cards
Bethesda criteria for endometrial cancer criteria for genetic referral
8
New cards
Obesity and endometrial cancer
9
New cards
Prevention of endometrial cancer
Like telling people not to become obese?
Several population-based studies have demonstrated a protective effect of hormonal contraception on the development of endometrial cancer with an estimated reduction of 50 %. This preventive action is observed for oral, systemic and local (intrauterine device) contraception, and may be considered in women at increased risk for endometrial cancer such as obese women, and women with Lynch syndrome. Patients with Lynch syndrome are recommended to have annual screening for endometrial pathology by transvaginal sonography and subsequent endometrial biopsy from the age of 30–35 years. In addition, patients are encouraged to contact the gynaecologist in case of abnormal uterine bleeding. Risk reducing hysterectomy and bilateral salpingo-oophorectomy should be discussed with the patient as alternative to screening when they are in their mid-40s
\
They mean progesterone only contraception right???
Several population-based studies have demonstrated a protective effect of hormonal contraception on the development of endometrial cancer with an estimated reduction of 50 %. This preventive action is observed for oral, systemic and local (intrauterine device) contraception, and may be considered in women at increased risk for endometrial cancer such as obese women, and women with Lynch syndrome. Patients with Lynch syndrome are recommended to have annual screening for endometrial pathology by transvaginal sonography and subsequent endometrial biopsy from the age of 30–35 years. In addition, patients are encouraged to contact the gynaecologist in case of abnormal uterine bleeding. Risk reducing hysterectomy and bilateral salpingo-oophorectomy should be discussed with the patient as alternative to screening when they are in their mid-40s
\
They mean progesterone only contraception right???
10
New cards
Diagnosis of endometrial cancer
11
New cards
Diagnosis of endometrial cancer
1. Clinical examination:
* most present with early stage disease so clinical examination may be normal
* Examination of the abdomen → palpation of the inguinal and supraclavicular regions to detect palpable masses and enlarged and suspicious nodes
* Gynaecological examination → macroscopic inspection of the cervix and cervical cytology (how exactly???)
* Bimanual examination contributes to the estimation of the size and mobility of the uterus, as well as notification of any palpable mass along the uterus (what is that???)
* Transvaginal sonography → to measure the size of the uterus and the endometrial thickness
* adnexal masses can be detected as well as the presence of ascites in the pouch of Douglas
* Endometrial cancer can be diagnosed in the outpatient clinic in the majority of patients
* Once a patient presents with abnormal uterine bleeding and thickened endometrium (≥ 4 mm) on US, an endometrial aspiration biopsy can be obtained from the uterine cavity
Other options or if biopsy is inconclusive → hysteroscopic guided biopsy, or dilation and curettage
* Any patient with recurrent postmenopausal bleeding should have histology checked out regardless of endometrial thickness
* In patients suspected of stromal malignancies, endometrial sampling is frequently inconclusive, and fine needle aspiration is discouraged as it is associated with a risk of tumour spillage in the abdominal cavity
2. Histological diagnosis:
* based on an endometrial biopsy, curettage or resection specimen
* Endometrioid endometrial cancer → glands with tall columnar cells resembling proliferative type endometrium
* grading is based on the % of solid growth with decreasing glandular differentiation (grade 1 → < 5% solid growth and grade 3 → > 50%)
* grade 3 nuclear atypia involving ≥ 50 % of tumour cells is associated with more aggressive behaviour and increases the overall differentiation grade by one (what so it becomes grade 4?)
* Serous carcinoma of the endometrium → resembles high grade serous carcinoma of the ovary and Fallopian tube → a complex papillary, solid and/or glandular growth with serrated luminal borders and lined by discohesive cells with diffuse, severe nuclear atypia, pleomorphism, numerous mitoses and bizarre forms
* Clear cell carcinoma → papillary, solid or tubulocystic growth patterns, cells are irregular polygonal, flattened or hobnail-shaped with clear, eosinophilic or granular cytoplasm + marked nuclear atypia
!! Prominent stromal hyalinization of the fibrovascular papillary structures is a diagnostic clue
* Undifferentiated carcinoma → poorly differentiated
If it is associated with a low grade endometrioid component, it is called dedifferentiated carcinoma
* *Carcinosarcoma the epithelial component often predominates and can be endometrioid (most common) or non-endometrioid (serous, clear cell or mixed). The mesenchymal component can be minimal or extensive and can be subdivided into homologous and heterologous, the latter including skeletal muscle, cartilage, fat or osteoid as reported in up to 60 % of tumours*
==So what differentiates it from any of the above???==
* !! Serous carcinoma, clear cell carcinoma, undifferentiated/dedifferentiated carcinoma and carcinosarcoma are always considered to be grade 3 tumours
* ==__The presence of a TP53 mutation almost always indicates a high-grade tumour__==
* LMS presents as dominant solitary mass, poorly circumscribed and often with areas of necrosis and haemorrhage, large fascicles of atypical spindle cells, multineucleated cells and marked nuclear pleomorphism
Some tumours do not show all morphological features of malignancy and are designated smooth muscle tumour of uncertain malignant potential (STUMP)
* Endometrial stromal nodule and low-grade ESS → composed of small round monomorphic cells resembling proliferative-phase endometrial stroma, CD10 and ER positive
*High-grade ESS contains a high-grade component with more destructive myometrial invasion. High grade ESS might be associated with a low-grade component. The high-grade component lacks CD10 and ER positivity and is defined by the genetic alterations*
* *Undifferentiated uterine sarcoma is a high-grade sarcoma showing a combination of severe nuclear atypia and high mitotic rate, frequently with tumour necrosis. Occasionally, transition from a classic low-grade ESS is found*
3. Imaging:
* type and extent of imaging is based on tumour histology and tumour grade, as well as the clinical examination
* preoperative early stage and low-grade endometrial cancers → small risk of metastasis → a chest X-ray is recommended as part of the work-up (but the chance of pulmonary metastasis is estimated to be < 1%)
* clinical early stage high risk and extended disease → CT and or PET (PET more accurate but more expensive)
* MRI? FDG PET CT
12
New cards
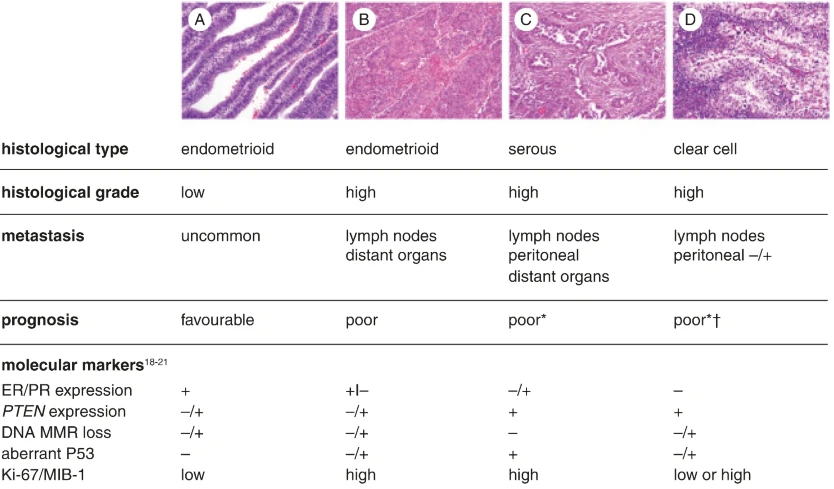
Clinicopathological and molecular characteristics of the common types of epithelial endometrial carcinoma
A is grade 1 and B is grade 3
13
New cards
golden standard for diagnosis of endometrial cancer
Histology
14
New cards
Therapy for endometrial cancer
1. Surgery:
* primary treatment of endometrial cancer
* early stage and low grade disease → hysterectomy and bilateral salpingo-oophorectomy (no need for lymph node removal)
* currently, hysterectomy is performed by a minimal invasive surgical approach in most patients if both uterus and ovaries can be removed completely through the vagina → faster recovery, less blood loss and reduced complications when compared to open surgery
* preooperative early stage and high grade tumour (eg. high grade endometrioid or serous and clear cell endometrial cancer) → surgical staging + hysterectomy + salpingo-oophorectomy to exclude microscopic metastasis
* surgical staging = pelvic and para aortic lymph node for grade 3 endometrioid endometrial cancer
* for all non-endometrioid endometrial cancer a careful assessment of the peritoneal cavity by sampling peritoneal biopsies, and omentectomy is also recommended
* radical hysterectomy can be done in patients with clinical involvement of the cervix
* uterine stromal or mesenchymal malignancies are treated by surgical resection of the uterus if feasible
retention of ovaries may cause a higher risk of recurrence but they may be kept in a selective group
2. radiotherapy:
* postoperative radiotherapy reduces the risk of a locoregional recurrence in patients with early stage, endometrioid endometrial cancer with deep myometrial invasion, and high tumour grade
* but it doesnt affect survival? how does that make sense
3. chemotherapy:
* for stage III-IV, multimodality therapy is required → radical cytoreductive surgery if possible, followed by adjuvant CT
4. hormonal therapy:
* ==__most endometrial cancers express ER and PR (progesterone) receptors__==
* presence of these receptors is strongly related to the histological type and tumour grade (and to response to hormonal therapy)
* low grade endometrioid endometrial cancers have the highest expression levels of ER and PR, yet even in grade 3 tumours hormone expression is observed in about 35 % of the cases
* progesterone treatment has been used for recurrent endometrial cancer with a variable response
* may be considered in young women who wish to keep their fertility
* response rates are based on patients with grade 1 endometrioid endometrial cancer with limited (< 50%) myometrial invasion and without metastasis
→ response rate was 67-80% but recurrence rate was 40-50%
* requires at least 3 months
15
New cards
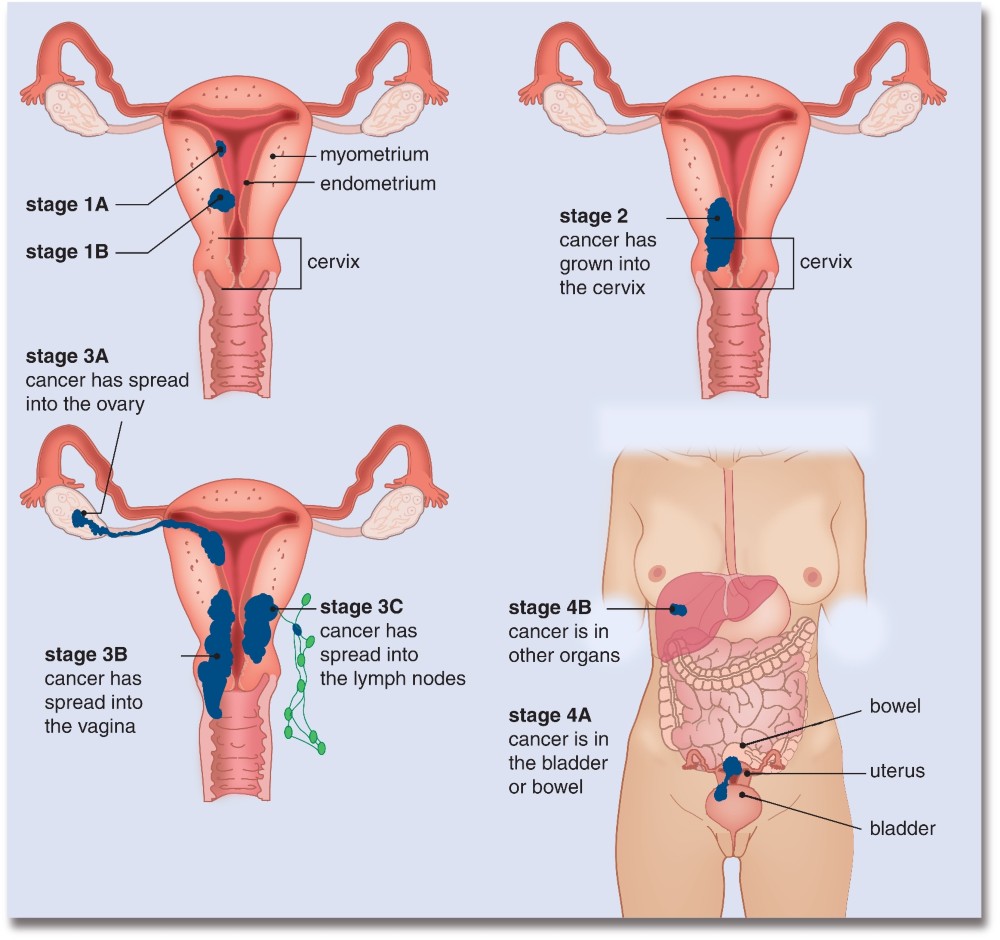
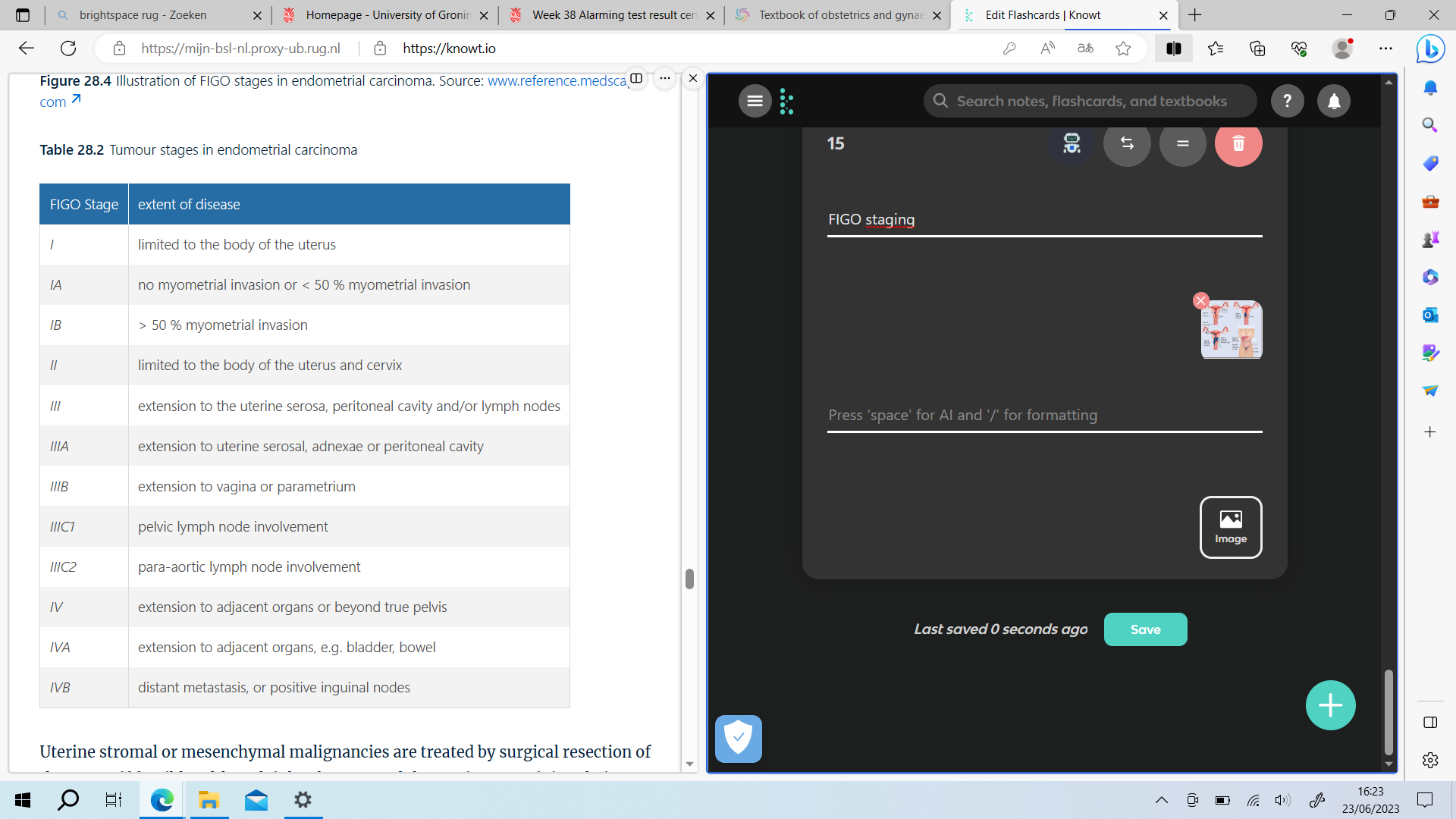
FIGO staging
16
New cards
follow up of endometrial cancer
* follow up is recommended for 5 years
* visits consist of a thorough history of symptoms with respect to vaginal blood loss, abdominal discomfort, and complaints of the urinary and GI tract
* there is no evidence that routine imaging or cytology of the vaginal vault is valuable to the early detection of recurrent disease
* most recurrences occur after 3 years of diagnosis
* visits consist of a thorough history of symptoms with respect to vaginal blood loss, abdominal discomfort, and complaints of the urinary and GI tract
* there is no evidence that routine imaging or cytology of the vaginal vault is valuable to the early detection of recurrent disease
* most recurrences occur after 3 years of diagnosis
17
New cards
social context
* increased sexual dysfunction
* QoL is in part related to treatment related morbidity
* endometrial cancer patients who have undergone lymphadenectomy have a risk of lymphedema with substantial impact on health-related quality of life
* QoL is in part related to treatment related morbidity
* endometrial cancer patients who have undergone lymphadenectomy have a risk of lymphedema with substantial impact on health-related quality of life