Palmer- Spinal Exam 4- Learning Objectives/TQs
1/226
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
227 Terms
In the thoracic curvature, ______________ body height is greater than _______________ body height.
The pelvic curvature has greater dimensions of sacral segments from ________________ to _____________ .
posterior; anterior
superior; inferior
The pelvic curve extends from ______ to ________. 100% TQ
The thoracic curve extends from ________ to _______.
Tricky, be careful!
L5-S1
T2-T12
Curvatures of the spine are names based according to what?
the direction of the convexity of the curve\
(ex: kyphotic convex part points posterior)
In primary curvatures, the earliest curves face _____________.
posteriorly
What are the other names for the kyphotic curvatures?
Which regions are kyphotic?
-posterior, primary
-Thoracic and pelvic (sacrococcygeal)
What are the other names for the lordotic curvatures?
Which regions are lordotic?
-anterior, secondary
-Cervical, compensatory and lumbar
Secondary curvatures are not apparent until the __________ period and allow for ___________ ________ in humans.
postnatal; erect posture
When is cervical lordosis first apparent in development?
When is it most accentuated? (when does the curve develop the most)
-3-4 months
-9 months (baby is looking around and sitting up)
The cervical spine is maintained by ____________ anterior dimensioned of the _____.
increased; IVD
Which curvature is the least distinct of the spinal curves and increases significantly with age?
Cervical lordotic curvature
What do some authors say the cervical curvature is composed of? (dumb tq)
Upper cervical curve and a lower cervical curve
when does the lumbar lordotic curvature develop? TQ
What is this time frame associated with?
-9-18 months after birth
- baby learning how to walk
The lumbar curvature extends from ________ to ______________ _________.
It is most prominent from ____-________ to ______. TQ
t12; lumbosacral articulation
L3-L5/ S1
T/F: Lumbar lordotic curvature is more pronounced in females.
TRUE
What maintains the lordotic curvature? (2 things, but one contributes more)
- IVD and VB taller anteriorly than posteriorly
The Z joints in infants are positioned __________, whereas the z joints in adults are positioned______________.
This is critical for what?
coronally; sagittal
transfer of weight
Facet movement begins at ___ months and continues until ___ months and aids in posture, ability to walk and formation of lumbar lordotic curvature.
6; 18
Which unique progression in the lumbar curve development only occurs at the L4 level? TQ
posterior shift of nucleus pulposus in annulus fibrosus at L4
When do we expect to see lateral curvatures appear in the spine?
What is this thought to be associated with?
-6 years old
- genetic component, environmental factors, handedness, asymmetrical muscle use
Lateral curvature deviations results from what? TQ
asymmetrical muscle use/tone
What condition is caused by a deviation of kyphotic curve toward the posterior aspect? (posterior bending condition) TQ
What causes this?
-Hyperkyphosis
-poor posture, DDD, arthritis, osteroporosis, trauma, developmental
What are the three most common kyphosis abnormalities seen in children and adolescence? TQ (all hyperkyphosis)
What is an example of hypokyphosis?
1. Postural kyphosis
2. Scheuermann's kyphosis
3. Congenital kyphosis
Straight back syndrome
Postural kyphosis is more commonly seen in ___________ between the ages of ______ to ________. TQ
Females; 12-17
T/F: Postural kyphosis is associated with severe structural abnormalities.
FALSE: due to poor posture, NOT structural abnormalities. Easily fixed with posture change.
Which kyphotic abnormality is due to a structural abnormality of the epiphyseal rims and cartilaginous end plates causing a decrease in IVD space anteriorly, leading to an exaggerated curve? 100% TQ/NBQ
Scheuermann's Kyphosis
T/F: Scheuermann's Kyphosis is idiopathic, meaning the cause is unknown. Patients typically outgrow this. NBQ
TRUE
When do we see Scheuermann's Kyphosis present itself typically?
Why is this?
TQ
-10-15 years old
-condition affects epiphyseal rims and cartilaginous end plates which are SECONDARY centers of ossification, so this happens during puberty.
A structural abnormality that results in disrupted cartilaginous end plates and epiphyseal rims causing wedge shaped vertebral bodies is known as what condition? TQ!
Scheuermann's Kyphosis
What are common terms that describe hyperkyphosis?
Humpback, Hunchback, Roundback
Hyperkyphotic results when the kyphotic curvature is greater than _______ degrees.
the natural thoracic kyphotic curve is ____ to ________ degrees
50
20-45
which kyphotic abnormality is present at birth? What is the cause of this?
-Congenital kyphosis
-vertebrae do not form properly or may fuse together (ex: hemivertebrae)
T/F: Congenital kyphosis corrects itself with time as the child develops. TQ
FALSE: this condition WORSENS with age
T/F: Straight (flat) back syndrome is a structural abnormality.
true
Which kyphotic abnormality is due to the curve being almost completely absent?
Why might this cause a problem with the heart? TQ
-Straight (flat) back syndrome
-narrows thoracic cage, decreasing room for heart, heart shifts positions kinking great vessels
Which lordotic abnormality has a decreased anterior curve in the cervical region ? (hypolordotic)? TQ
Military (straight) neck
Which lordotic abnormality is due to an increased curve in the lumbar region? (hyperlordotic) TQ
Who is this most commonly seen in?
Swayback
females
What is the typical cervical lordotic curve (in degrees)?
What would be considered hyperlordotic or hypolordotic?
100% TQ
typical: 20-40 degrees
Hyperlordotic= greater than 40 degrees
Hypolordotic= less than 20 degrees
what is the typical lumbar lordotic curve? (in degrees)
What would be considered hyperlordotic and hypolordotic? TQ
typical: 40-60 degrees
Hyper= greater than 60
Hypo= less than 40
Putting it all together...
swayback is specific to the lumbar spine and is _______________.
straight (military) neck is only in the cervical spine and is ___________.
Hunchback is specific to the thoracic and sacral spine and is an ___________ posterior curve.
Straight (flat back) is specific to the thoracic spine and is a _______________ in the posterior curve.
-hyperlordotic
-hypolordotic
-increase
-decrease
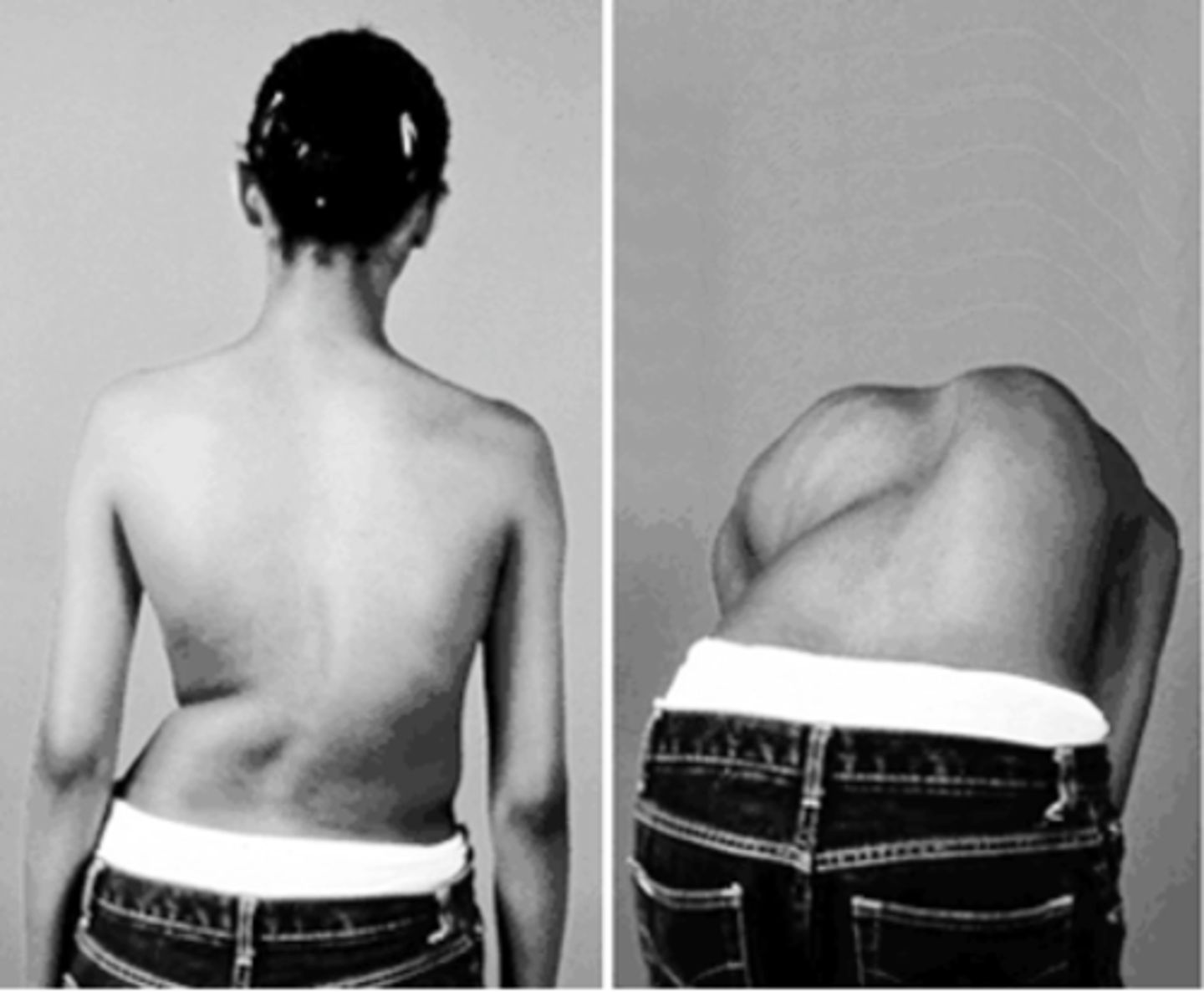
which spinal region is most prominently affected to scoliosis ?
Why ?
-Thoracic
-attachment to thoracic cage
What is the primary indicator that someone has scoliosis? TQ
they have a posterior elevation on one side of the thorax 6mm or greater
T/F: scoliosis is a condition that can be caused by structural or non-structural parts.
TRUE- can be developmental, anatomical or idiopathic
Which test is used to determine bone maturity in scoliosis to determine ossification of iliac crest? 100% TQ
(this allows docs to know how much of an impact they can make on scoliosis treatment)
Risser sign
What does the Risser sign measure and how does this corelate with scoliosis? TQ
-measures the growth life of the spine by looking at the iliac apophysis (crests)
-if child hasn't reached skeletal maturity yet, there is a better chance to correct scoliosis!
Which 5 measurements classify scoliosis deformity according to the Scoliosis Research Society?
1. Magnitude
2. Location
3. Direction
4. Etiology
5. Structural/ Non-structural
How do you determine the magnitude of a scoliotic curve? TQ
Cobb method
(measured using length and angle of curve on X ray)
How is scoliosis location determined? TQ
location of vertebra at apex of curvature
(example, an apex at T12 means it's the most lateral and the most horizontal vertebrae in the curve)
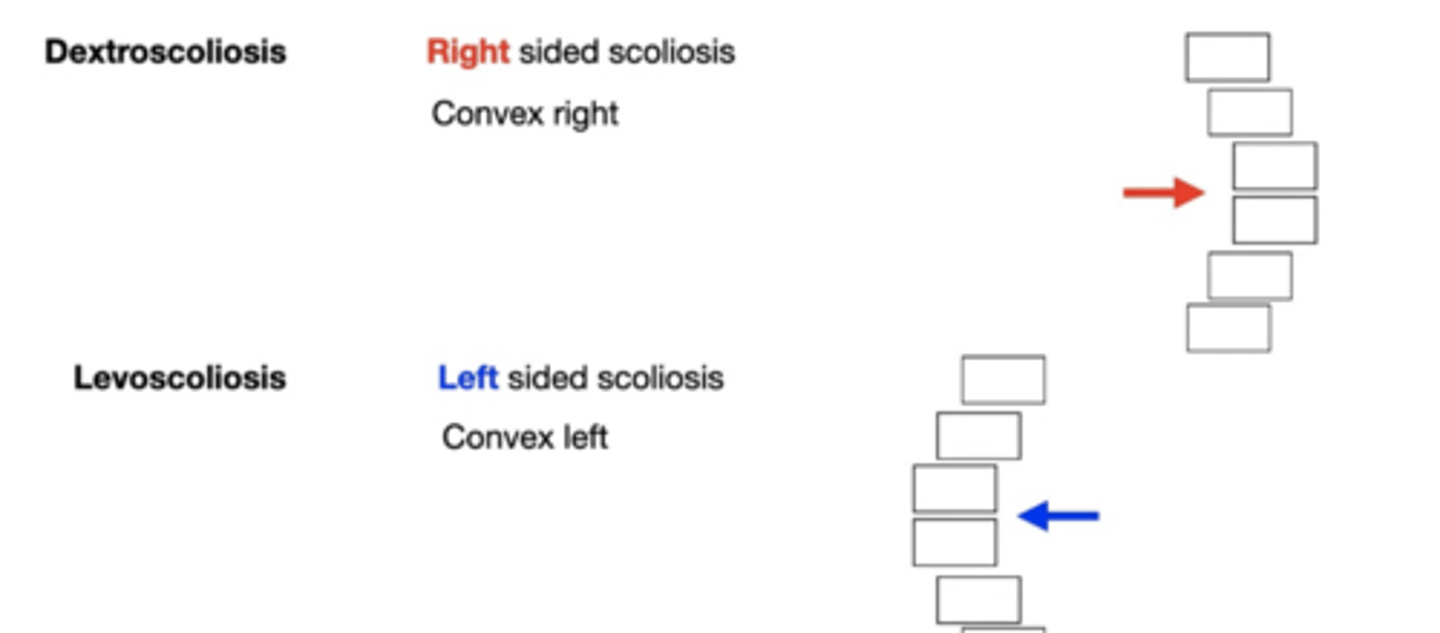
How is scoliosis direction determined? TQ
the side where the convex part of the curve lies.
What does the scoliosis etiology refer to? (dumb TQ)
How the scoliosis was derived. There are multiple classifications for this (we don't need to know them)
Non-structural scoliosis has a _________ deviation and is ____________ to worsen.
It is _______ associated with deformities of the vertebral body or IVD.
TQ
mild; unlikely; not
What is non-structural scoliosis often linked to? TQ!! (3)
1. poor posture
2. unequal leg length
3. muscle spasm
Which is more common, structural or non-structural scoliosis?
structural scoliosis
Structural scoliosis will __________ in time and involves deformities of the _________ and/or the ____________. TQ!
worsen; vertebra; IVD
What are the possible causes of structural scoliosis? (5)
1. disease state (ex: rheumatoid dz)
2. Birth defects (hemivertebrae)
3. Injury
4. Infection
5. Abnormal growth
What three types of idiopathic scoliosis were discussed inlecture?
1. Infantile idiopathic scoliosis
2. Juvenile idiopathic scoliosis
3. Adolescent idiopathic scoliosis
T/F: the majority of scoliosis patients have idiopathic scoliosis.
TRUE
Infantile idiopathic scoliosis is from _______ to _______ years old. NBQ/TQ
________% of the patients are ________. TQ
birth; 3
56%, males
T/F: Infantile idiopathic scoliosis is typically treated with surgery since it will worsen with development. TQ
FALSE- typically patients will outgrow this and it will resolve spontaneously. Only once in a while do patients need surgery.
Juvenile idiopathic scoliosis is seen from ages ______ to _______ years old.
There is ________ gender difference until age ______. After this we see that __________ are affected more often. NBQ/TQ
3-10
no; 6; females
In juvenile idiopathic scoliosis, what is the typical curve pattern?
Does this worsen with age?
right thoracic deviation
yes
In infantile idiopathic scoliosis, which curve pattern predominates? TQ
does this worsen with age?
left thoracic deviation
no, patients typically "outgrow" this
What is the most common type of idiopathic scoliosis?
What is second most common?
1st- adolescent idiopathic scoliosis (80%)
2nd -juvenile idiopathic scoliosis (12-21%)
What age do we see adolescent idiopathic scoliosis? NBQ/TQ
which group do we see this in most commonly? Why? 100% TQ
over 10 years old
females, it's related to growth spurts
In adolescent idiopathic scoliosis, which curve pattern predominates?
right thoracic curves (seen in 90% of cases)
T/F: adolescent idiopathic scoliosis is linked to autosomal dominant inheritance, meaning this typically occurs in family members.
TRUE
Lack of lordosis is commonly seen in those under what age? TQ
17 years old
What are the three distinct zones of the intervertebral disc? (TQ)
1. Central zone (nucleus pulposus)
2. Peripheral zone (annulus fibrosus)
3. Horizontal zone (superior and inferior margins, cartilaginous end plates)
The intervertebral disc is filled with water and what two other substances?
How is water restored to the IVD after being diminished throughout the day?
-proteoglycan gel and collagen fibers
-8 hour period in supine position
IVD height ____________ with age. TQ
diminishes
T/F: the nucleus pulposus becomes more fibrous as water and proteoglycans decrease.
TRUE
What are the cartilaginous end plate (attached to VB and IVD) composed of? 100% TQ
Where do each of these parts articulate with? TQ
-Fibrocartilage (articulates with IVD)
-Hyaline cartilage (articulates with VB)
** unique, composed of TWO types of cartilage.
which aspect of the IVD allows for diffusion of gases, nutrients and waste materials? TQ
Cartilaginous end plates
What is the innervation to the anterior outer 1/3 of the annulus fibrosus (of IVD)?
What about the lateral 1/3?
Posterior 1/3?
TQ!- need to know
-Anterior: Afferent branches from the sympathetic trunk
-Lateral: Gray ramus communicans
-posterior: Sinuvertebral (aka recurrent meningeal) nerve
T/F: Degeneration of the IVD can occur very early in life (between 20-30 years old) TQ
TRUE- this is something that makes disc degeneration unique compared to other tissues in the body
Which condition discussed in lecture promotes disc degeneration by depositing calcium in the posterior wall of the aorta, increasing risk of disc degeneration and is associated with back pain? TQ
Aortic Atherosclerosis
The expansion of disc material beyond its normal borders is a condition referred to as ?
(NO tearing, NO extrusion, NO protrusion...just displacement...watch wording on TQ)
disc bulge
What structure is associated with the herniation of intervertebral discal material? TQ
Cartilaginous end plate- if weak, it will not hold the IVD within anatomical borders as it should
what are the three subcategories of IVD herniation?
1. Protrusion
2. Extrusion
3. Sequestration
T/F: the annulus fibrosis bulges in both disc herniation and disc bulge
TRUE
Which subtype of disc herniation happens with a localized bulge of the NP through a few layers of the AF and discal matter is displaced?
(AF is still surrounding NP all the way around)
Protrusion ("true" herniated disc)
Which subtype of disc herniation occurs when the NP protrudes through ALL layers of the AF while remaining attached to the disc origin?
What are the three subtypes of this?
-extrusion
1. Pedunculated protrusion
2. Subligamentous extrusion
3. Transligamentous extrusion
Which type of extrusion is happening when the diameter of the peripheral herniated disc material has a greater diameter than attachment site (base) to the host disc? TQ
Pedunculated protrusion
Which type of extrusion does not penetrate the PLL?
Which type of extrusion penetrates the PLL?
TQ
- subligamentous extrusion
-Transligamentous extrusion
T/F: Herniated disc is another name for a disc bulge.
FALSE- a herniated disc involves protruded or extruded nucleus pulposus, while disc bulge can just be the disc extending beyond its anatomical borders.
which subtype of disc herniation happens when there is a free disc fragment with no attachment to the host IVD? (the fragment can migrate freely) TQ
What are the two subtypes of this?
-Sequestration
1. Subligamentous sequestration
2. Transligamentous Sequestration
Which type of sequestration doesn't penetrate the PLL?
Which type does penetrate the PLL and can protrude through both the PLL and dura matter?
TQ
- Subligamentous sequestration
-Transligamentous sequestration
What is the orientation and shape of the anterior longitudinal ligament (ALL)? TQ
-extends from the anterior aspect of vertebral bodies from occiput to sacrum
-hour glass shape
What is the function of the ALL? 100% TQ
limits extension
- especially important in lumbar region to help lordotic curve and weight bearing
What is the innervation of the ALL? TQ
anterior neural plexus (fibers from the ventral primary ramus)
the ALL is thicker from ________________ to _________________ at regions of bodies compared to regions of the IVD. TQ
anterior; posterior
The ALL is multilayered. The superficial fibers span ________________ vertebrae while the deep gibers span from _____________ vertebra to the next. TQ
(this helps fill in the concave spaces and creates a smooth anterior surface of VBs. )
several; one
Diffuse idiopathic skeletal hyperostosis is also called _____________ disease. This occurs with OALL causing the vertebral body to demonstrate hyperostosis, causing accessory bone growth. TQ
(OALL means ossification of ALL)
Forestier's Disease
What may happen to the cervical spine with Forestier's disease/DISH?
-Reduced cervical mobility
-may see fibrous masses behind odontoid process (retro-odontoid pseudotumor)
What is the only spinal ligament that limits extension?
ALL
above C2, what is the ALL continuous with?
medial portion of anterior atlanto-occipital membrane
What are the attachments of the ALL? TQ
-basilar part of occiput
-anterior tubercle of C1
- tight to anterior VB
-loose attachment to IVD
What is the function of the PLL? TQ
Limits flexion of the spine
What is the innervation of the PLL? TQ
What is significantly important about the innervation PLL? TQ 100%
-posterior neural plexus from recurrent meningeal nerves
-High nociceptive innervation, making this one of the most pain sensitive areas of the spine
T/F: The PLL does not receive a lot of sensory innervation, therefore isn't affected by pain. TQ
FALSE: receives a ton of nociceptive innervation, making it one of the most pain sensitive areas of the spine!!
what is the attachment sites of the PLL?
tightly attaches to epiphyseal rims and IVD from C2 to sacrum (to prevent disk herniation)