6. SOAP Notes
1/17
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
18 Terms
why do we document?
Client care management
Treatment team communication
What's the PT working on?
Way to communicate in one place about the client
Evaluations
Progress notes
What's occurring?
Discharge summaries
Daily notes
Physician orders
If it wasn't documented, it didn’t happen!
supervisors/insurance may look at notes to say is it:
Appropriate
Medical necessity
Law abiding
Utilization Review
After services provided
Utilization Management
Takes place while patient is active such as D/C planning and physician monitoring.
inpatient care in hospitals and critical access hospitals, skilled nursing facilities (SNFs), home health care, and hospice
medicare part A
Covers physicians’ services and outpatient care, including OT, also services in SNF when the client does not qualify for skilled coverage under Part A
medicare part B
Private insurance companies contract with Medicare to provide individuals with Part A and Part B benefits through Medicare Advantage Plan
medicare part C
prescription drug coverage
medicare part D
why do we need to know the payment sources when documenting?
ex: If client was injured at work and workers comp is paying, we have to document on how they are doing their job, not parenting their child
general guidelines for documentation
Include:
Date and time
What services were provided and when they were provided.
What was said and what happened
Why the skill of an occupational therapist was required rather than the services of an aide, a family member, or another professional.
why is good documentation important?
Someone else will read this and will have to understand what you wrote.
people cover you for vacation and sick time
This entry will be scrutinized by insurances
Can be read by a Medicare reviewer
Is what we documented reimbursable
My client or patient can ask to read what I wrote.
how do you correct errors on documentation?
strikethrough
what are special situations?
client refuses therapy
absences
incidents/accidents
client sick
SOAP Note
S-Subjective
O-Objective
A-Assessment
P-Plan
Patient report of problems, limitations, and needs
Brief, couple sentences
Relate subjective to what you're doing
Initial evaluation should be longer
Initial Interview
subjective (S)
Health professionals observation
Measurable
Quantifiable
Observable data
No speculation on your part, just what you see
objective (O)
The occupational therapist’s interpretation or assessment of what happened
Analysis of the subjective and objective sections
Put our feedback
assessment (A)
What to do next
Frequency
Duration
Goals
plan (P)
what is included in a discharge summary note?
Goals met
Client no longer making functional gains requiring skilled OT
Client moves to another location
Setting does not match the individual’s needs
client and caregiver education
home exercise program
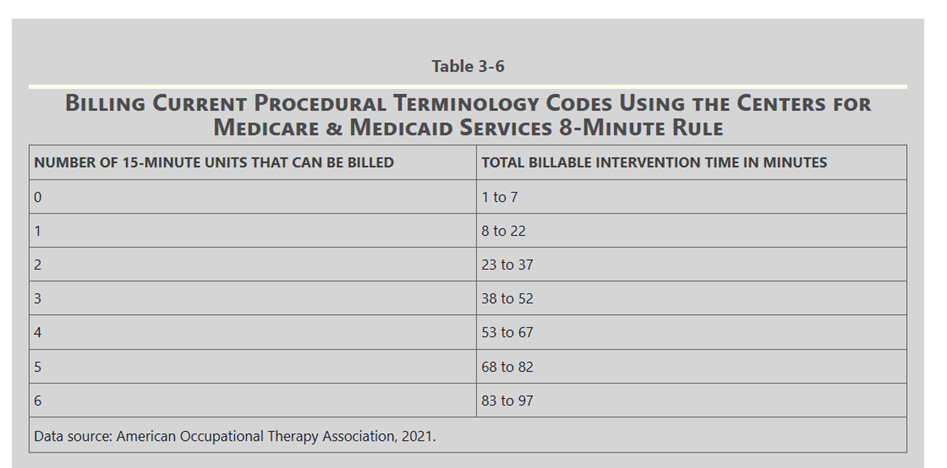
A service must have been provided for at least 8 minutes to bill one 15-minute CPT code. A second billable unit cannot be billed “until you have at least 8 minutes past the 15-minute mark
8 minute rule