Pain Exam 1: Harrold Opioid Analgesics and Antagonists
1/99
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
100 Terms
mu, kappa, delta
3 major subtypes of opioid receptors
1. ___ (OP3)
2. ___ (OP2)
3. ____ (OP1)
mu, kappa
Current drugs target __ and ___ receptors
Gi, G0
Both μ (mu) and κ (kappa) receptors are coupled with ___ and __ proteins
inhibitory, ion channel
remember
Gi= think ____
G0= think ___ ___
ceiling effect
There is no ___ ___ of analgesia for opiates (means increasing the dose → always increases analgesia)
close, open
Opioids
-____ N-type voltage-operated Ca2+ channels
-____ calcium-dependent K+ channels
no
Do opioids alter the pain threshold of afferent nerve endings?
no
Do opioids affect the conductance of impulses across peripheral nerves?
tolerance
Adverse effects of μ agonists
1. sedation/dizziness
2. constipation (patients will NOT develop ___ to this)
respiratory
Adverse effects of μ agonists
3. ___ depression (this is what causes death in overdose)
4. nausea/vomiting
miosis, tolerance
Adverse effects of μ agonists
5. ___ or "pinpoint pupils" (patients will NOT develop ___ to this)
euphoria, tolerance
Adverse effects of μ agonists
6. ____ (bc increased dopamine release), addictive behavior, and dependence liability (patients will NOT develop ___ to this)
dysphoria, withdrawal
Adverse effects of κ agonists
1. sedation/dizziness, nausea/vomiting
2. ___ (bad mood)
3. precipitation of __ symptoms in μ agonist dependent patients
euphoria, dysphoria
μ receptor → increases dopamine release → causes ___
κ receptor → decreases dopamine release → causes ___
pure agonists
Opioid receptor-mediated actions
1. __ ___ (ie full agonist): produce an analgesic acitivity
pure antagonists
Opioid receptor-mediated actions
2. ___ ___: blocks the actions of opioids at all receptor subtypes
antagonist/agonist
Opioid receptor-mediated actions
3. ____/____
agonists, antagonists
Most opioids with antagonist/agonist activity are ___ at the κ receptor and ___ at the μ receptor
antagonism, dose
Exception to usual antagonist/agonist activity is buprenorphine, which produces:
-weak ___ at κ receptor
-____-dependent agonist or antagonist activity at the μ receptor
tolerance
________: a decrease in the apparent effectiveness of a drug with continuous or repeated agonist administration. This effect will disappear over time whenever the agonist is discontinued
dependence
________: refers to a state of adaptation manifested by receptor/drug withdrawal syndrome produced by cessation of drug exposure (either by abstinence or administration of antagonist)
addiction
________: refers to a behavior pattern characterized by compulsive use of the drug
pure agonist
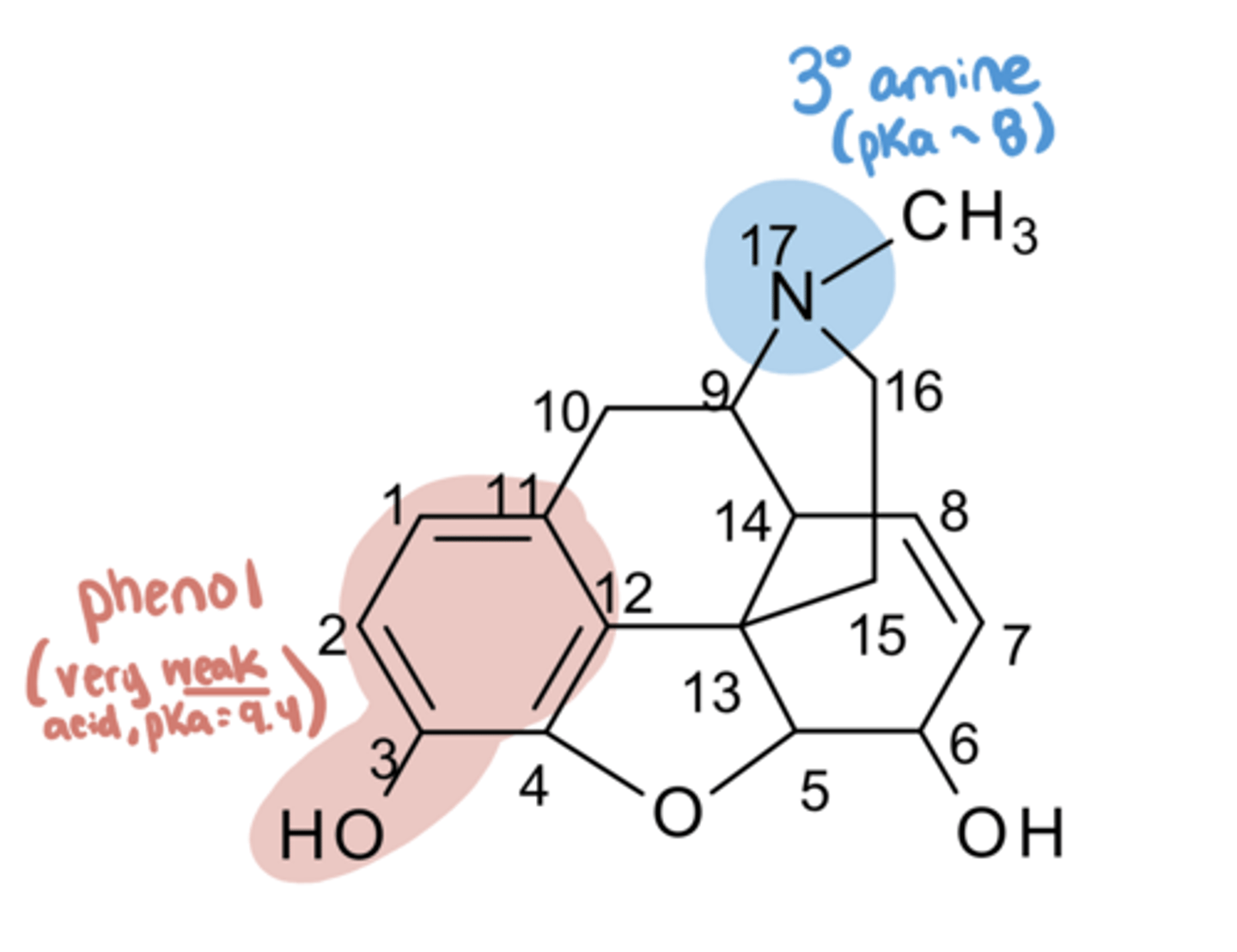
Morphine
-an alkaloid obtained from the opium poppy plant
-___ ___ at all opioid receptors
basic
Morphine
-a ___ drug
-
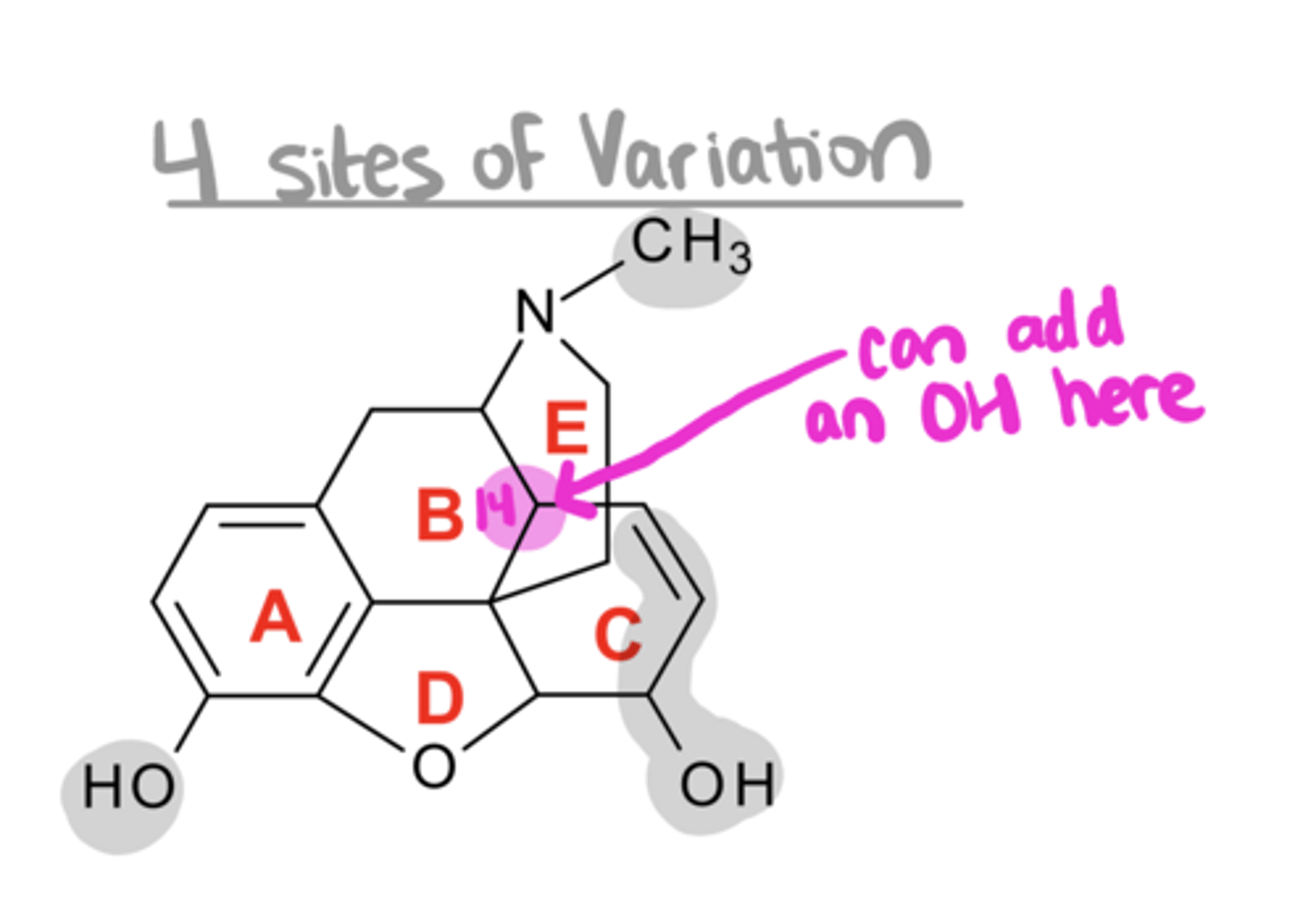
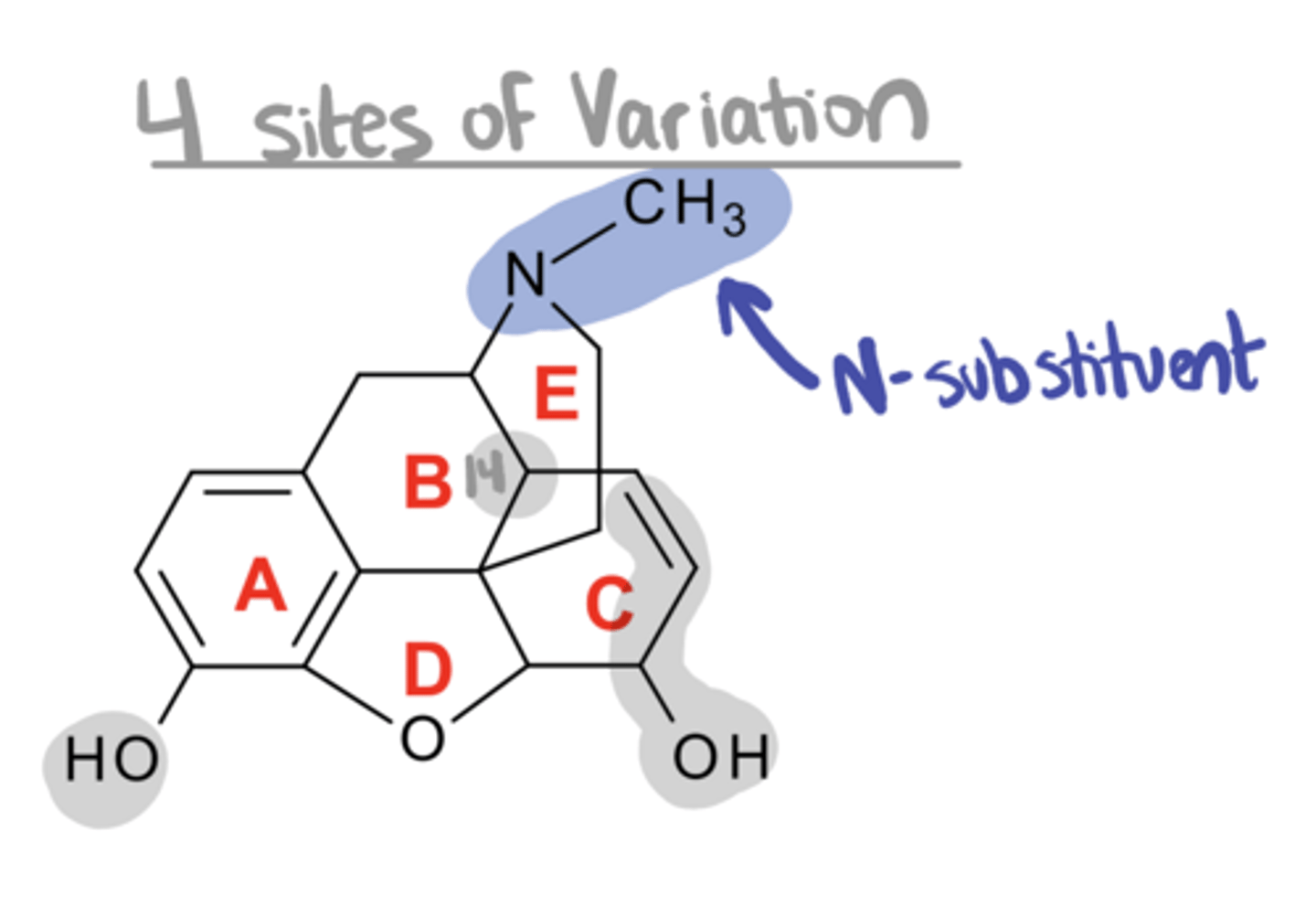
Morphine
-contains 5 asymmetric centers, the activity resides only in the (___) enantiomer
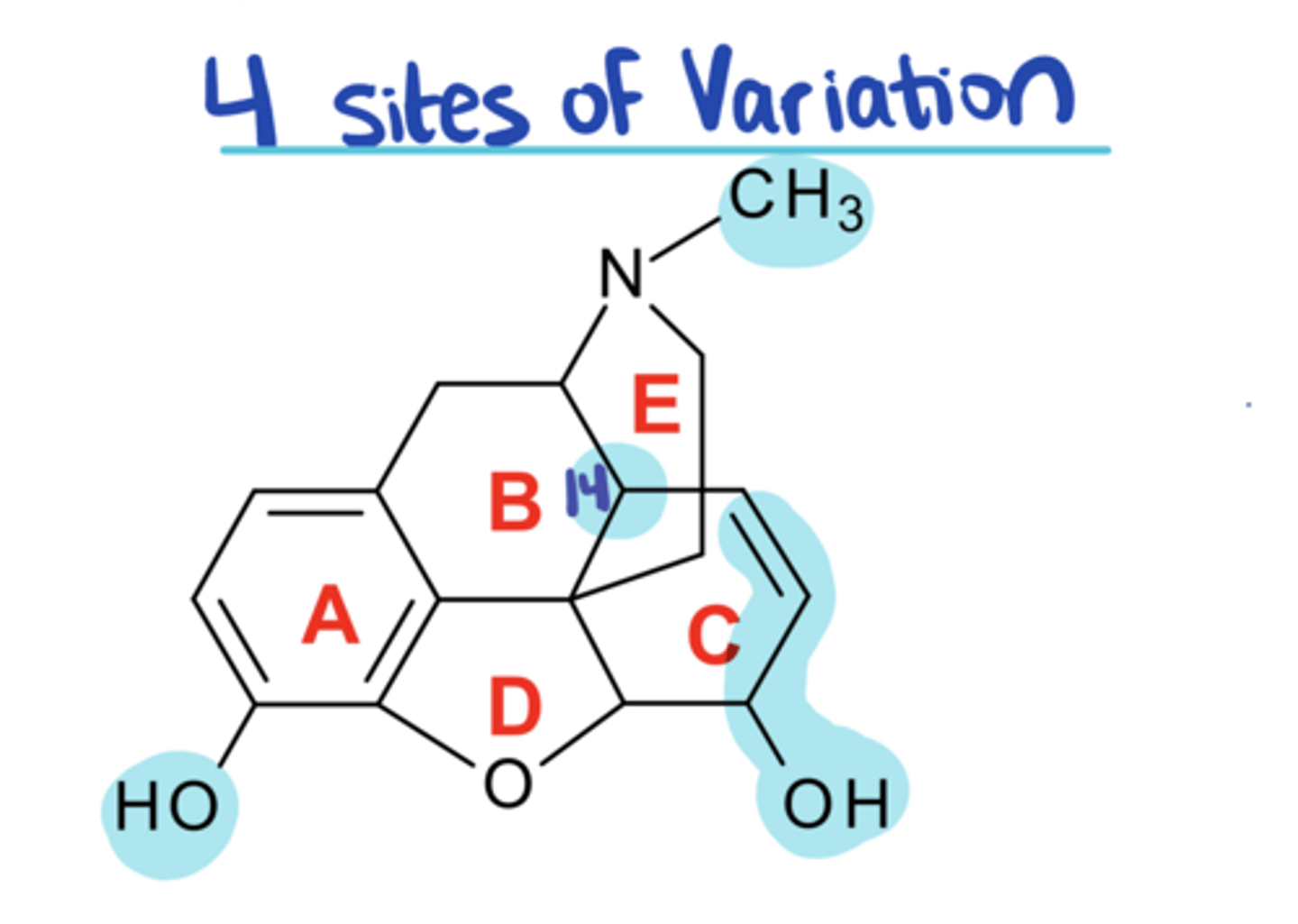
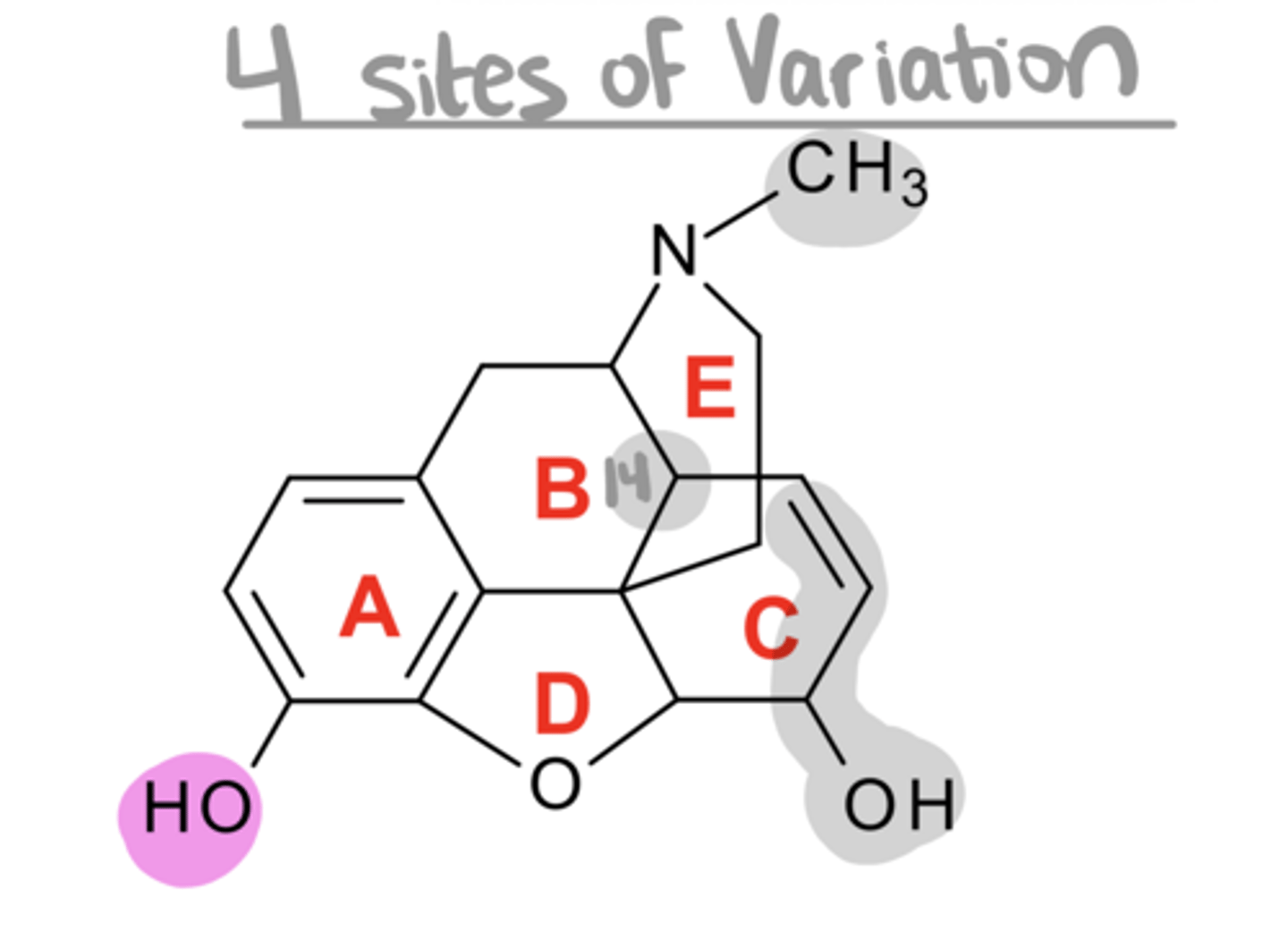
4
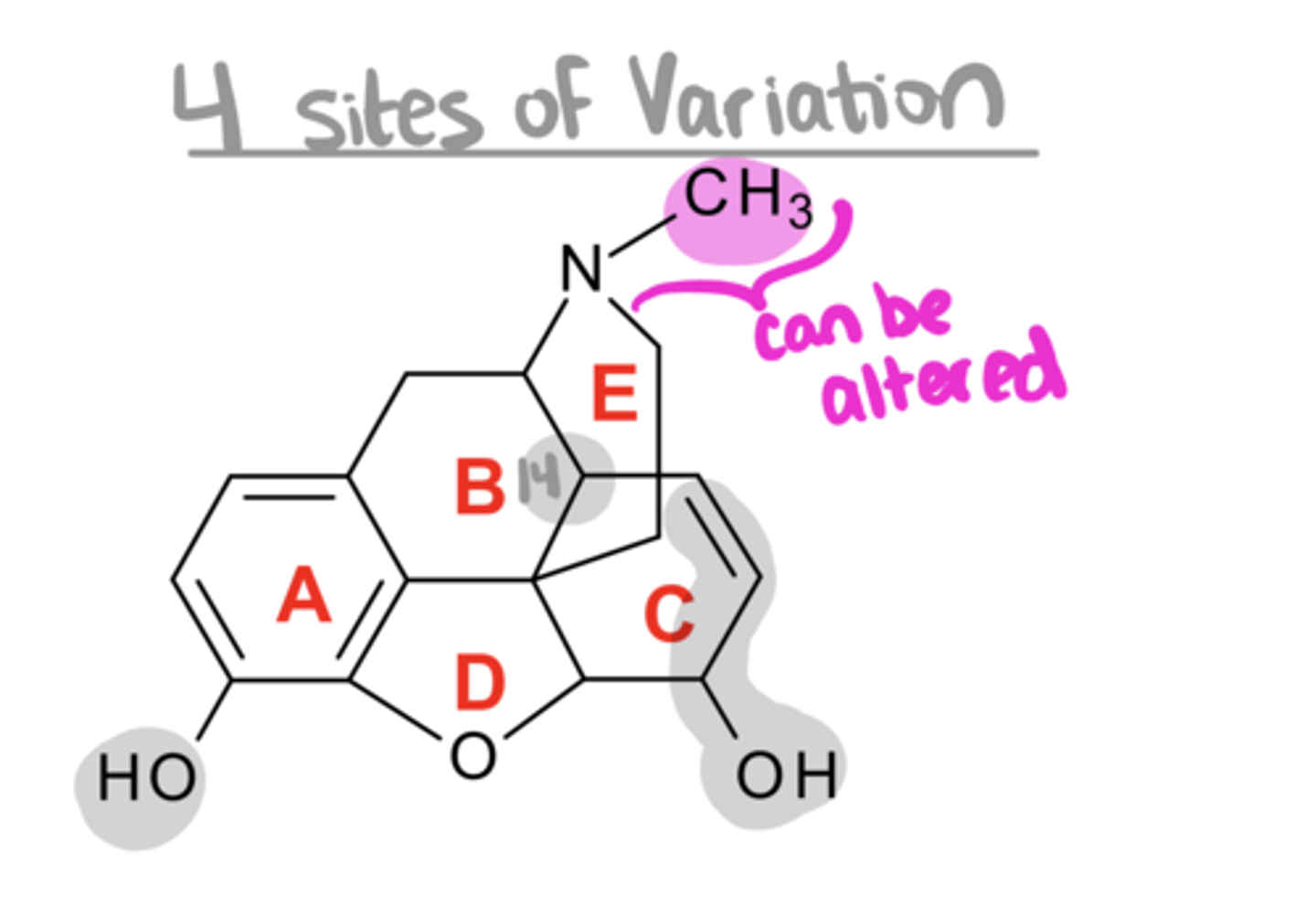
There are ____ sites of variation on morphine that are modified to create other opioid drugs
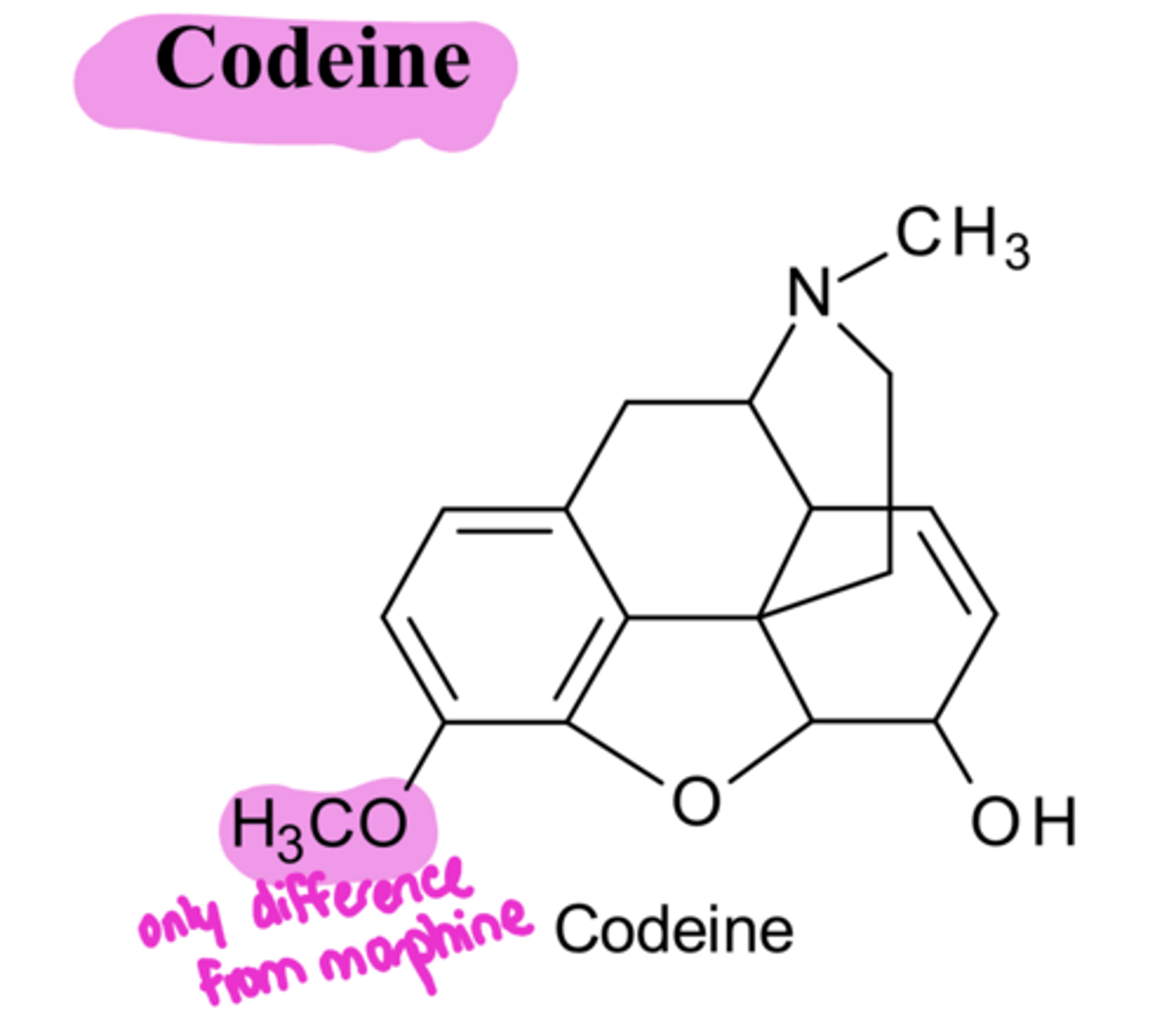
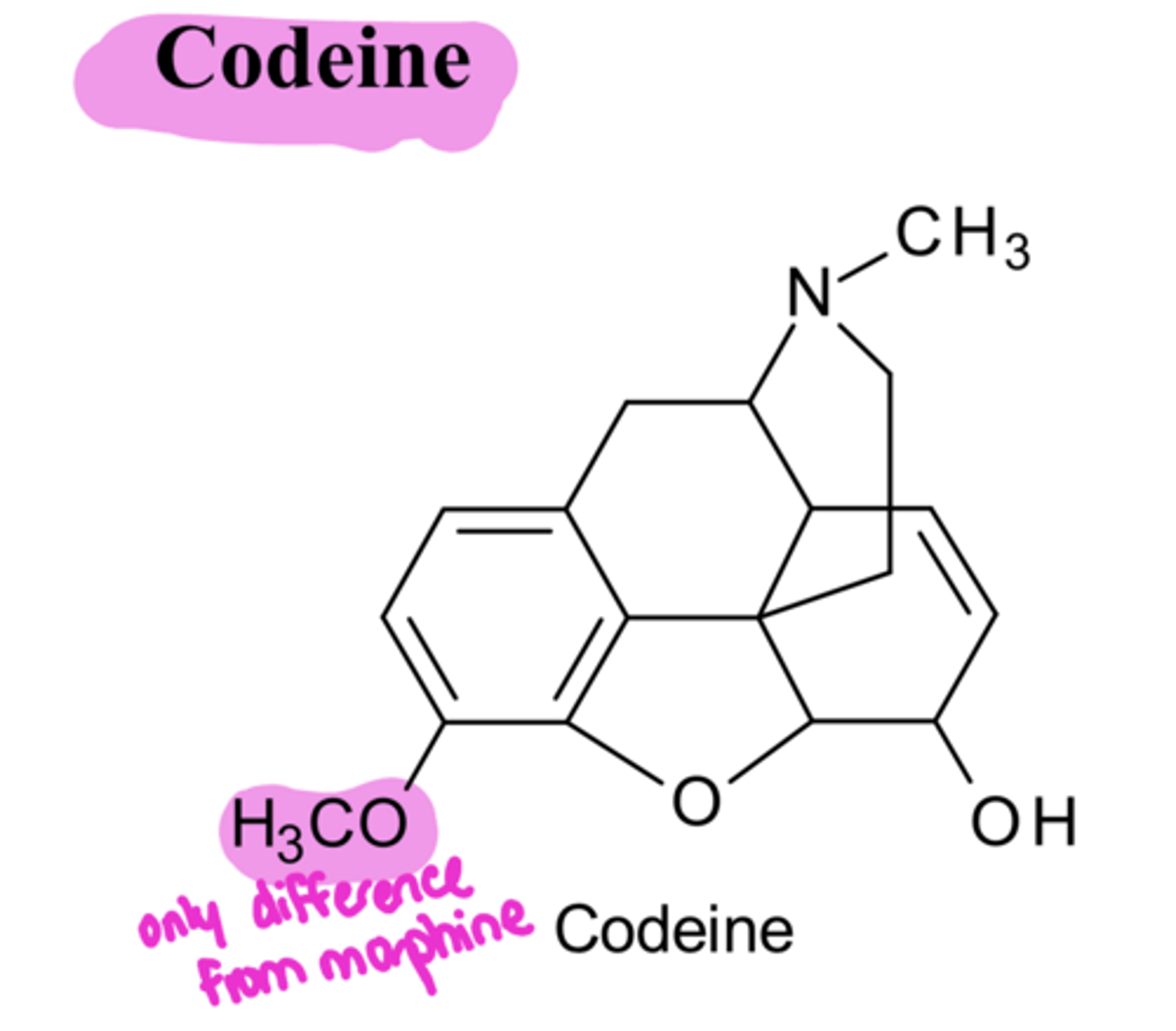
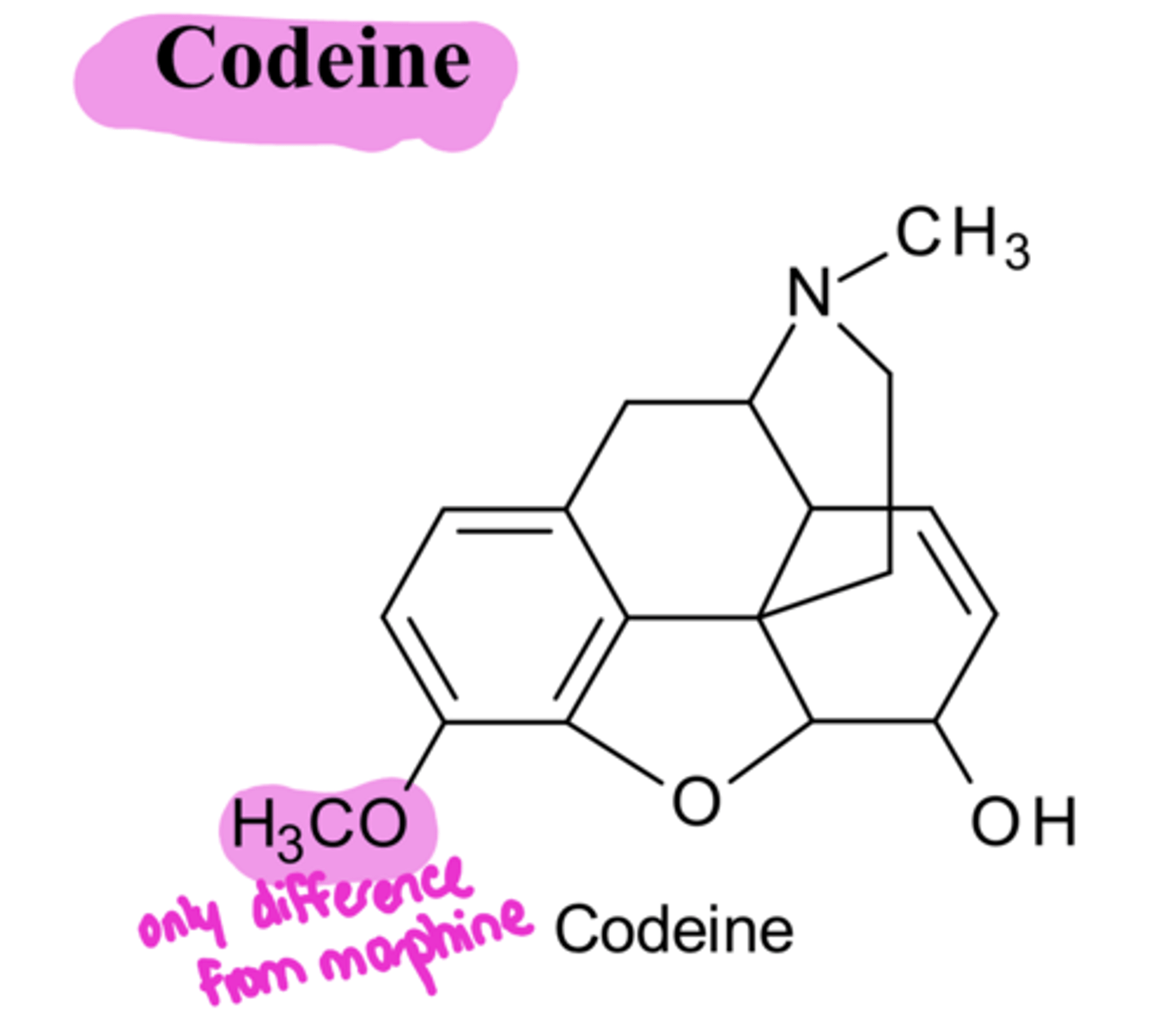
masking
The only modification from morphine in codeine is the ___ of the C3-OH
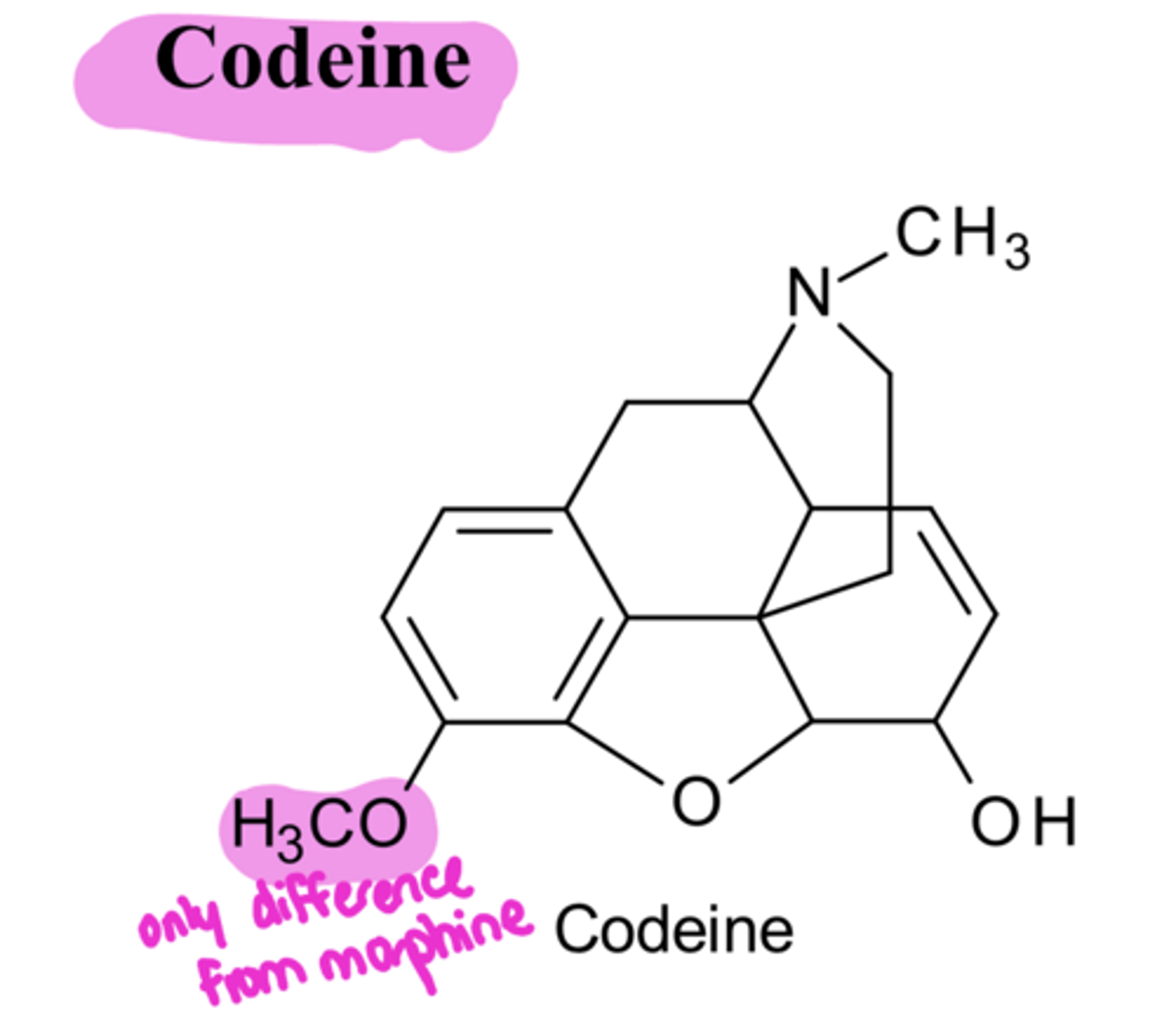
decreased, decreased
Because codeine replaced the C3-OH with C3-OCH3, it has ____ analgesic activity and ___ potency compared to morphine
less
Codeine
-causes ___ respiratory depression than morphine (none at normal doses)
better
Codeine
-has a ___ oral/parenteral ratio than morphine
-(morphine only 16% orally active, codeine is 60% orally active)
-phosphate and sulfate salts of codeine are used for solutions, elixers, etc
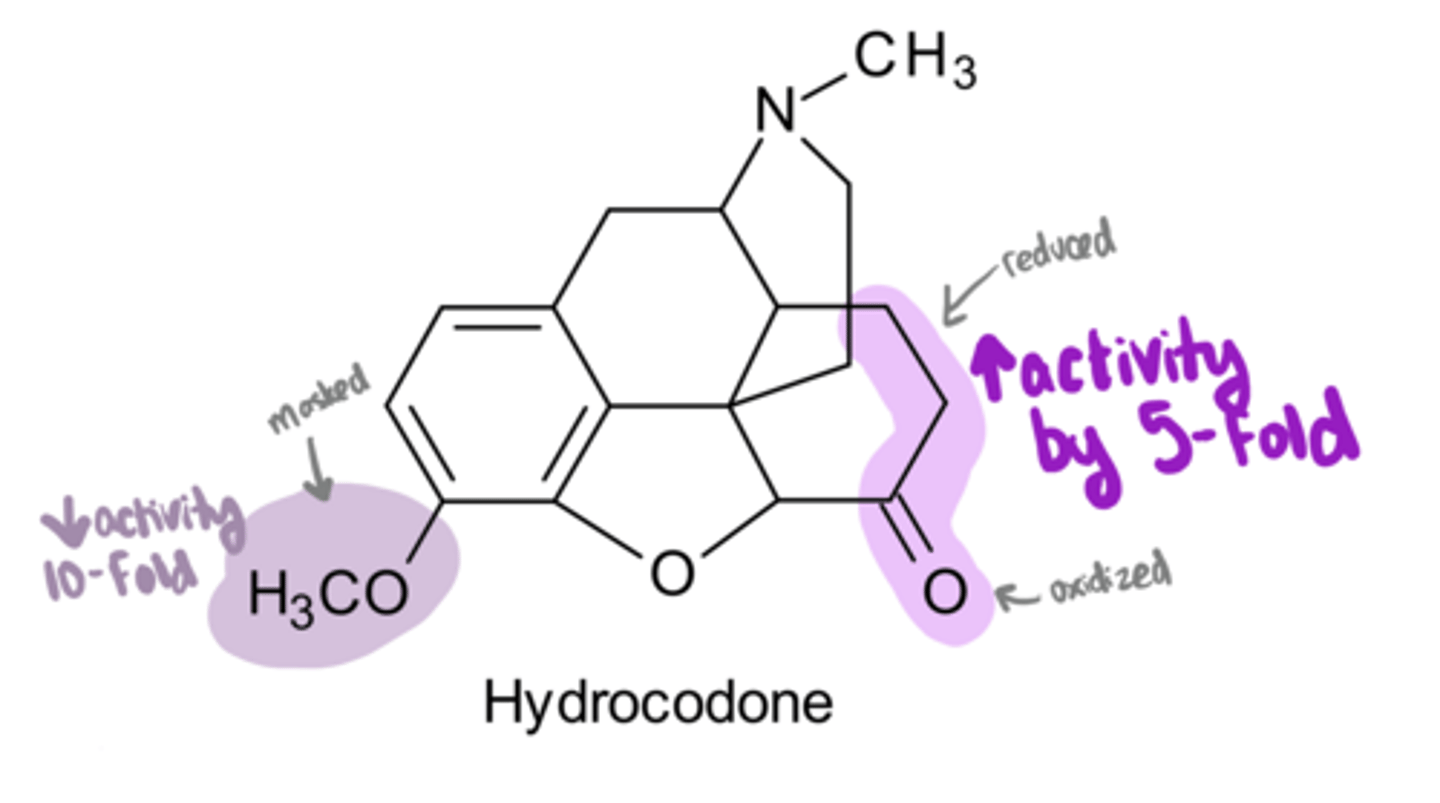
decrease
Key SAR for Morphine Analogs:
1. if you mask the C3-OH with a C3-OCH3 → ___ activity by 1/10th
increase
Key SAR for Morphine Analogs:
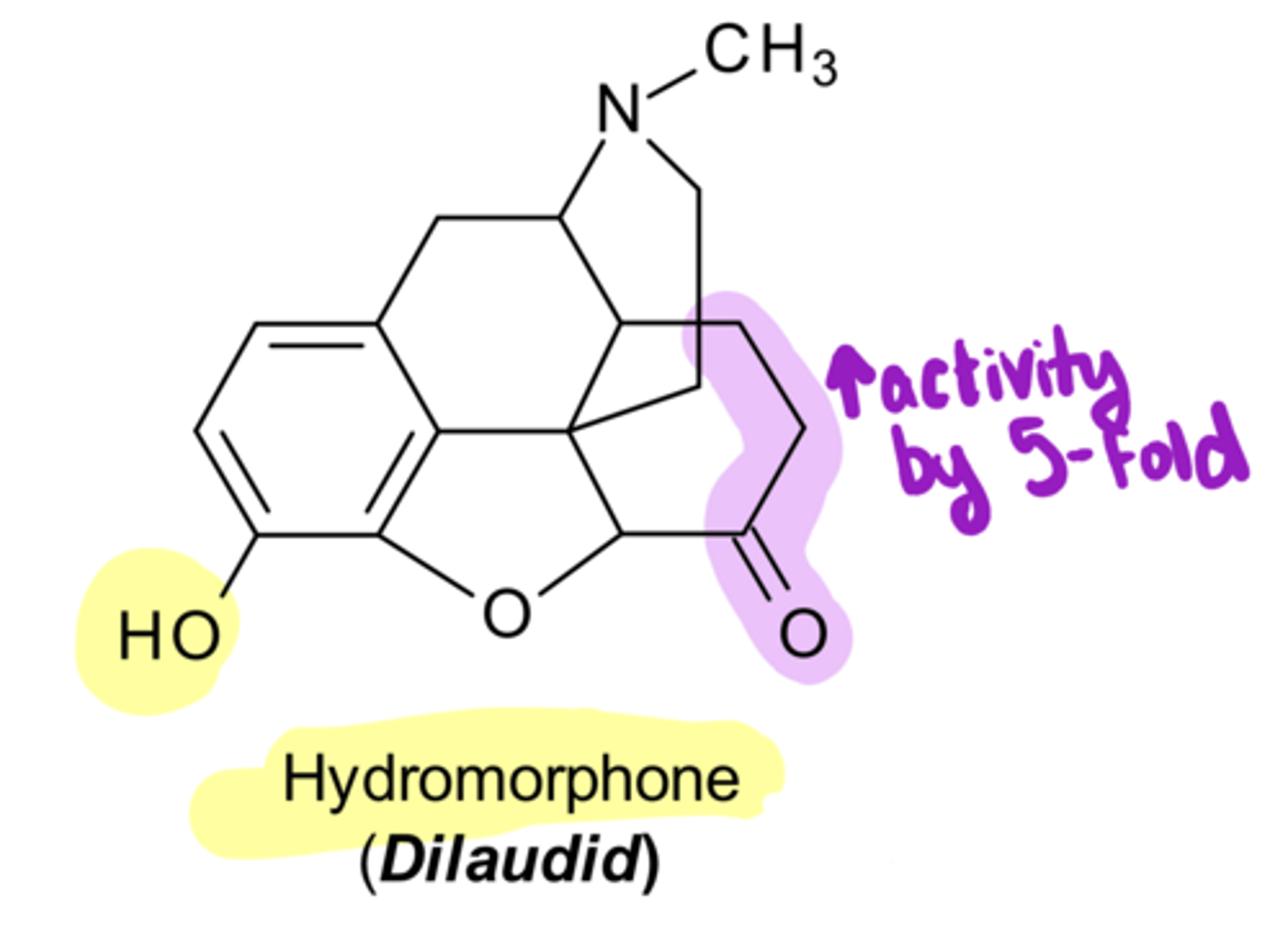
2. if you reduce the Δ⁷ (ie double bond between C7 and C8) and oxidize the C6-OH to a ketone → ___ activity by 5-fold
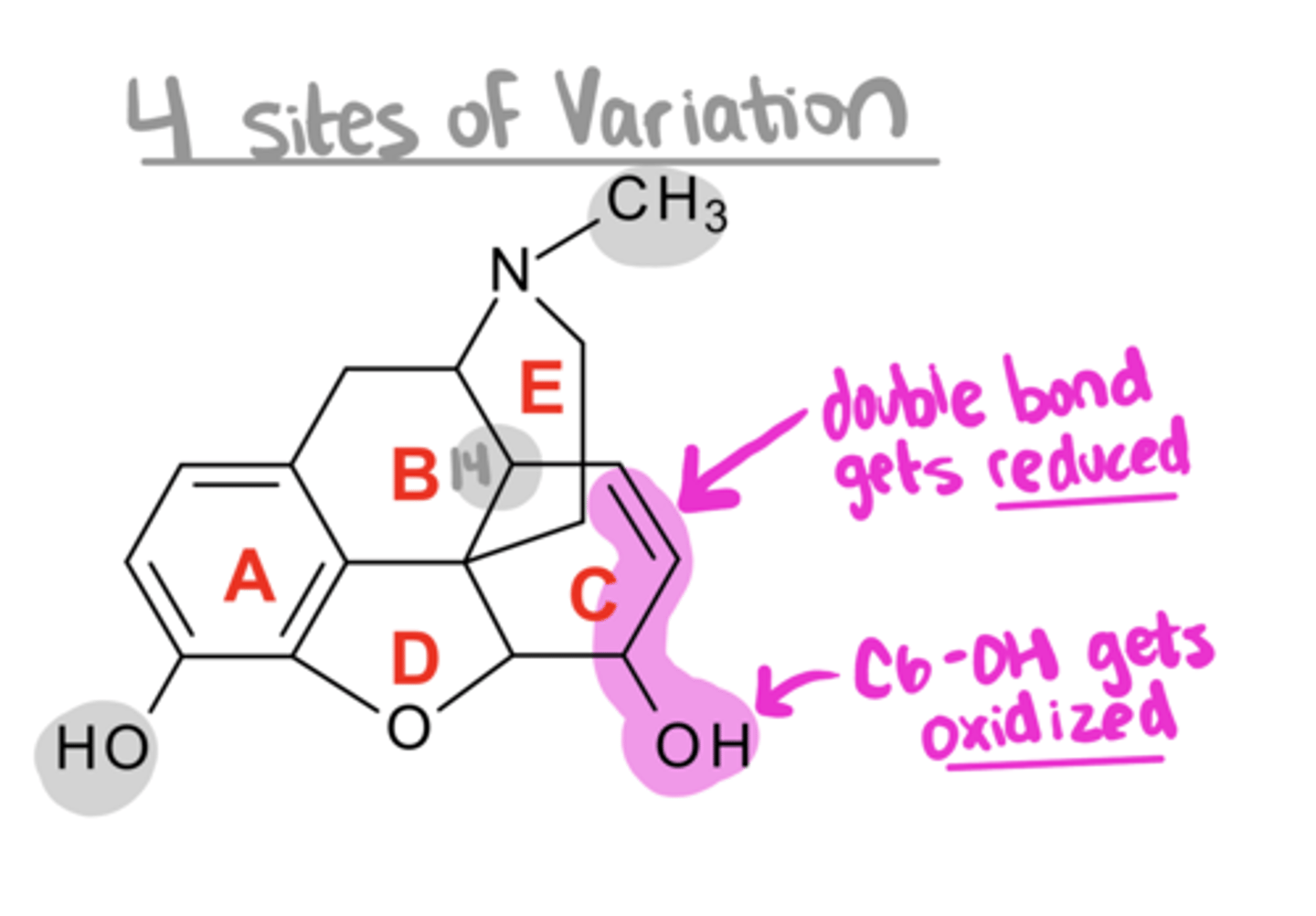
increase
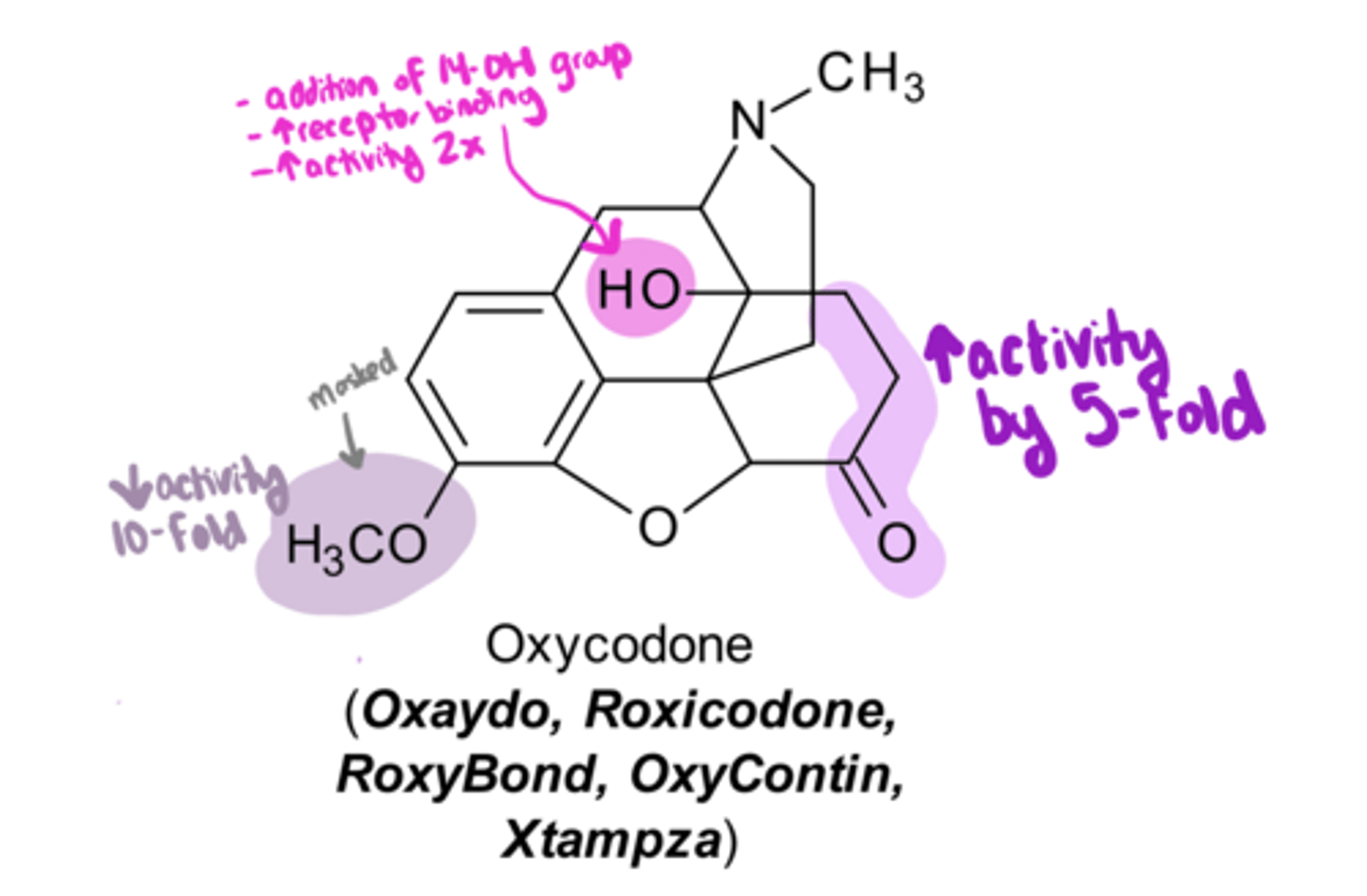
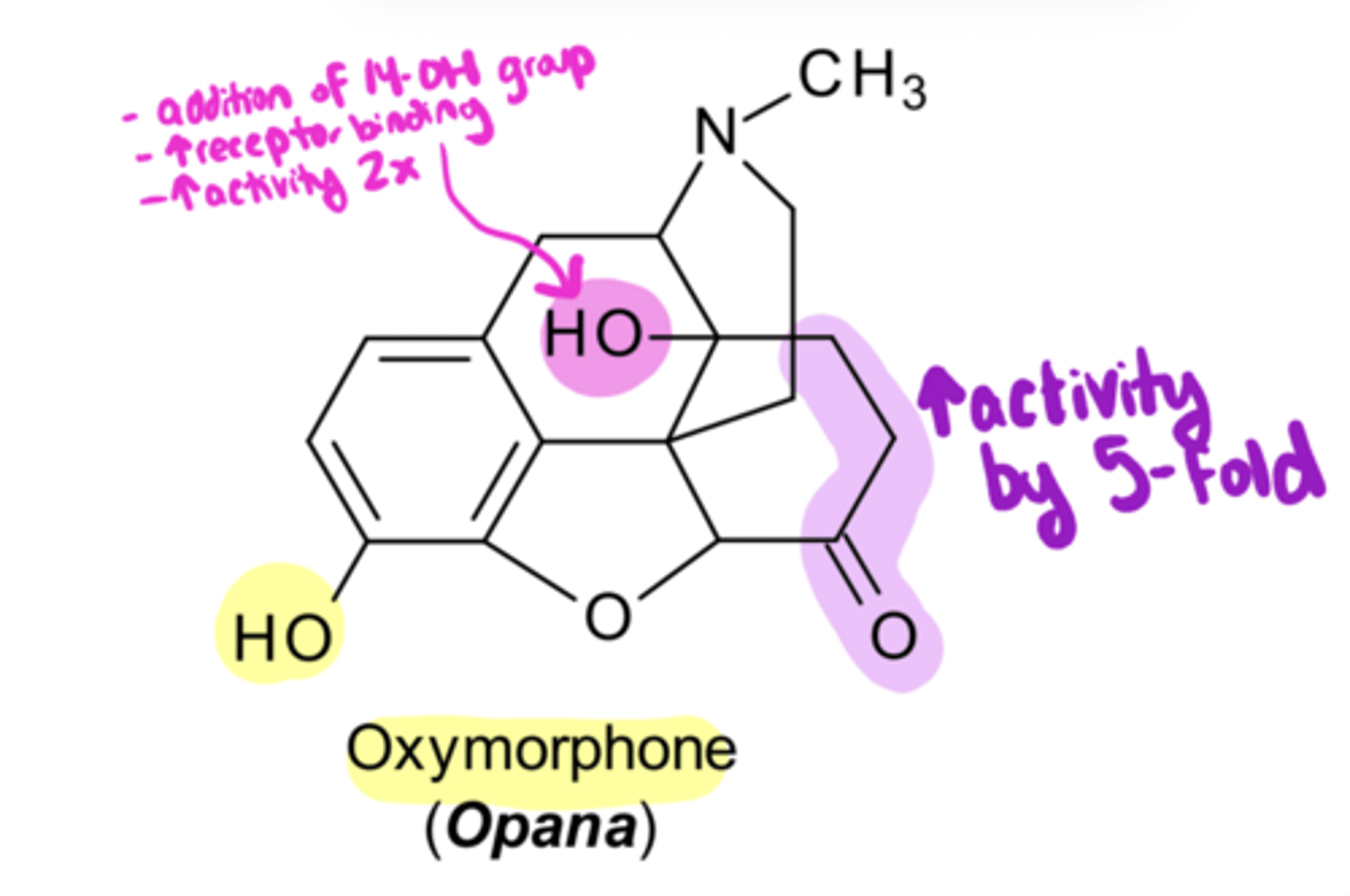
Key SAR for Morphine Analogs:
3. if you introduce a 14-OH group → ___ activity by 2-fold
antagonists, mixed
Key SAR for Morphine Analogs:
4. if you alter N-CH3 → produce ___ and ___ agonists/antagonists
hydromorphone, oxymorphone
Hydrocodone undergoes minor pathway → ____
Oxycodone undergoes minor pathway → ____
OCH3, OH
hydrocodone and oxycodone→ has C3-____
hydromorphone and oxymorphone→ has C3-____
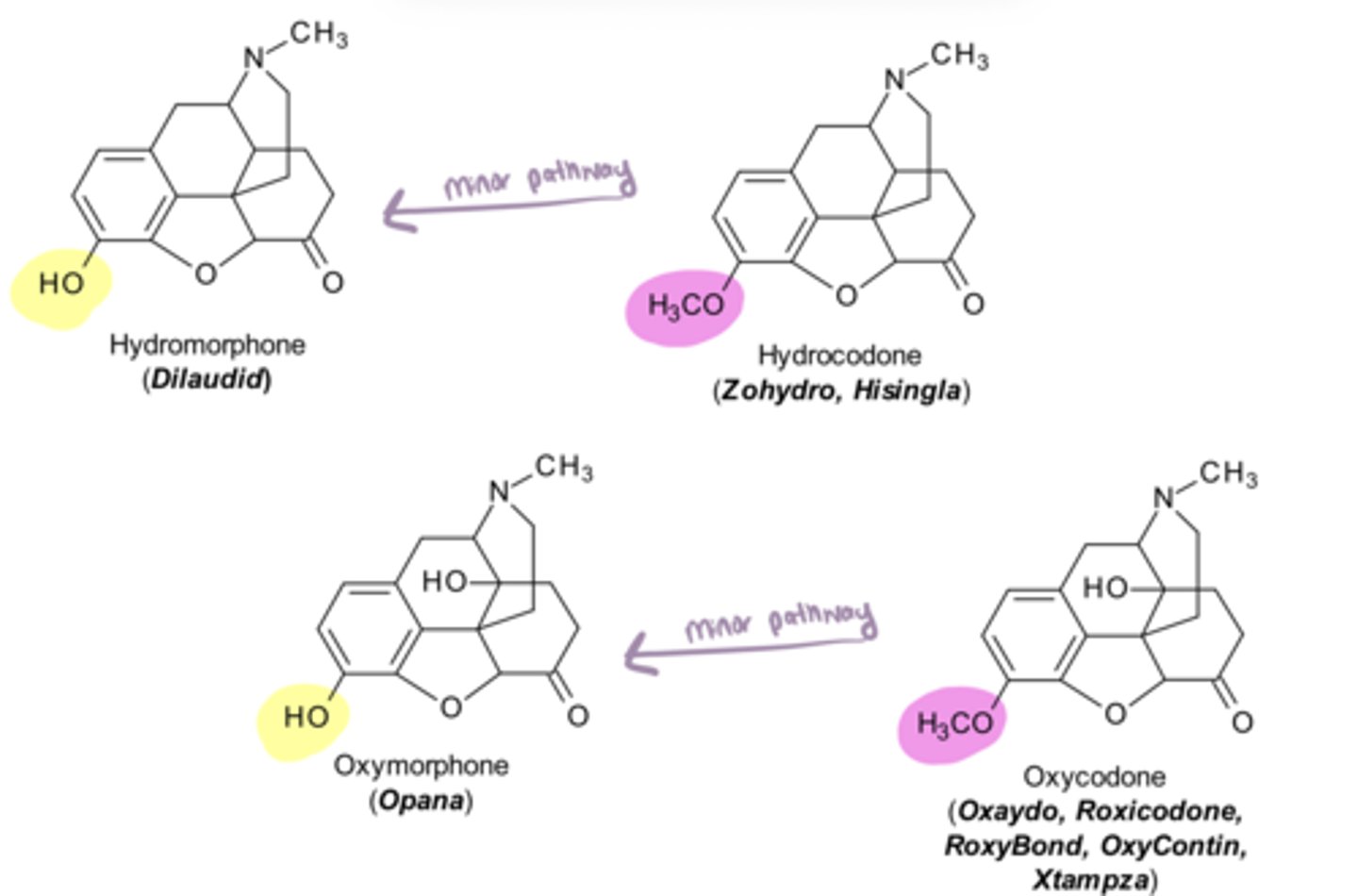
potent
Since hydromorphone and oxymorphone have a C3-OH (not masked with a methyl group), they will always be more __ than their parent compounds
midway
Hydrocodone
-pharmacological effects ___ between morphine and codeine
increases, decreases
Hydrocodone
-pharmacological effects midway between morphine and codeine because of these 2 variations from morphine:
1) reduction of the Δ⁷ (ie double bond between C7 and C8) and oxidization the C6-OH to a ketone → ___ activity 5-fold
2) masking of the C3-OH → ___ activity 10-fold
greater
Hydromorphone
-pharmacological effects are 5-fold ____ than morphine because only 1 variation from morphine, which is reduction of the Δ⁷/ oxidization the C6-OH to a ketone
increases
-oxycodone/oxymorphone have an additional SAR change compared to hydrocodone/hydromorphone, which is addition of a C-14 OH (remember this increases receptor binding, and therefore ____ activity 2-fold)
equipotent
Oxycodone
-pharmacological effects are ____ with morphine because of these 3 variations from morphine:
1) reduction of the Δ⁷ and oxidization the C6-OH to a ketone → increases activity
2) masking of the C3-OH → decreases activity
3) introduction of 14-OH → increases activity
greater
Oxymorphone
-pharmacological effects are 10-fold ___ than oxycodone because of these 2 variations from morphine:
1) reduction of the Δ⁷ and oxidization the C6-OH to a ketone → increases activity
2) introduction of 14-OH → increases activity
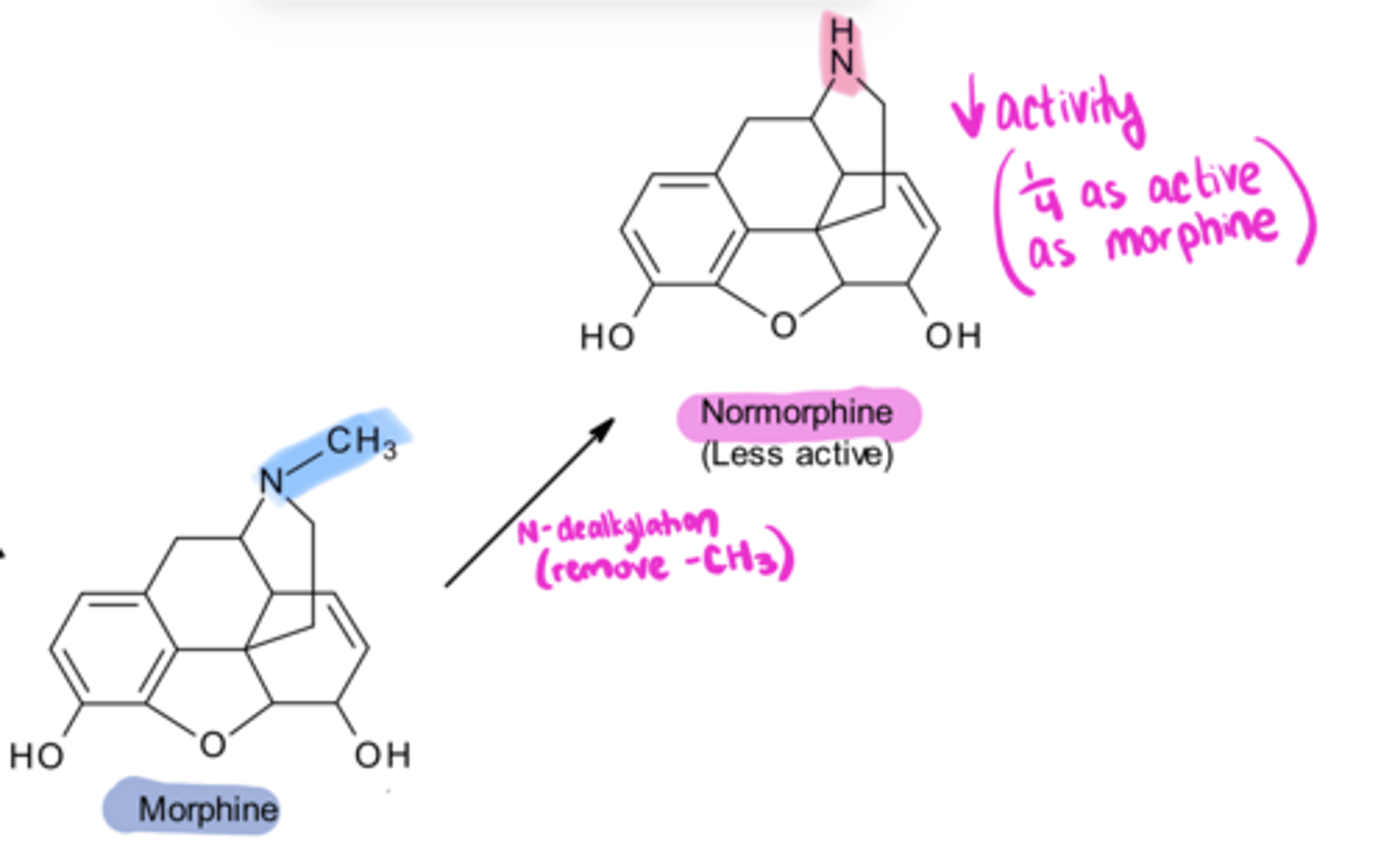
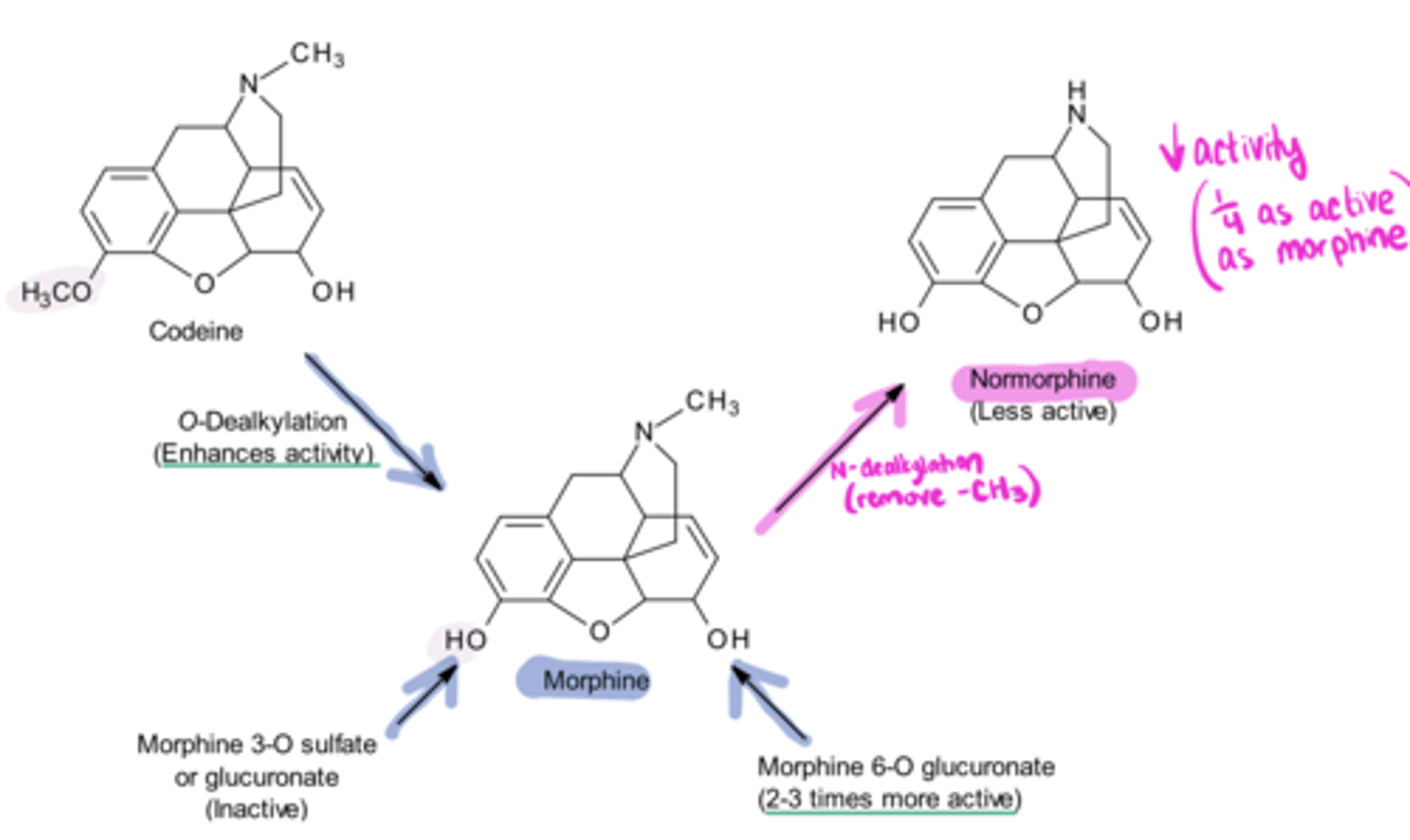
normorphine, decreased
Removal of -CH3 from morphine gives ____, which has ___ activity
agonist/antagonist, antagonist
If you lengthen the N-substituent on morphine, you will change the activity from an agonist to a mixed ___/___ or pure ___
nalbuphine
An example of a "normal" mixed agonist/antagonist is ____
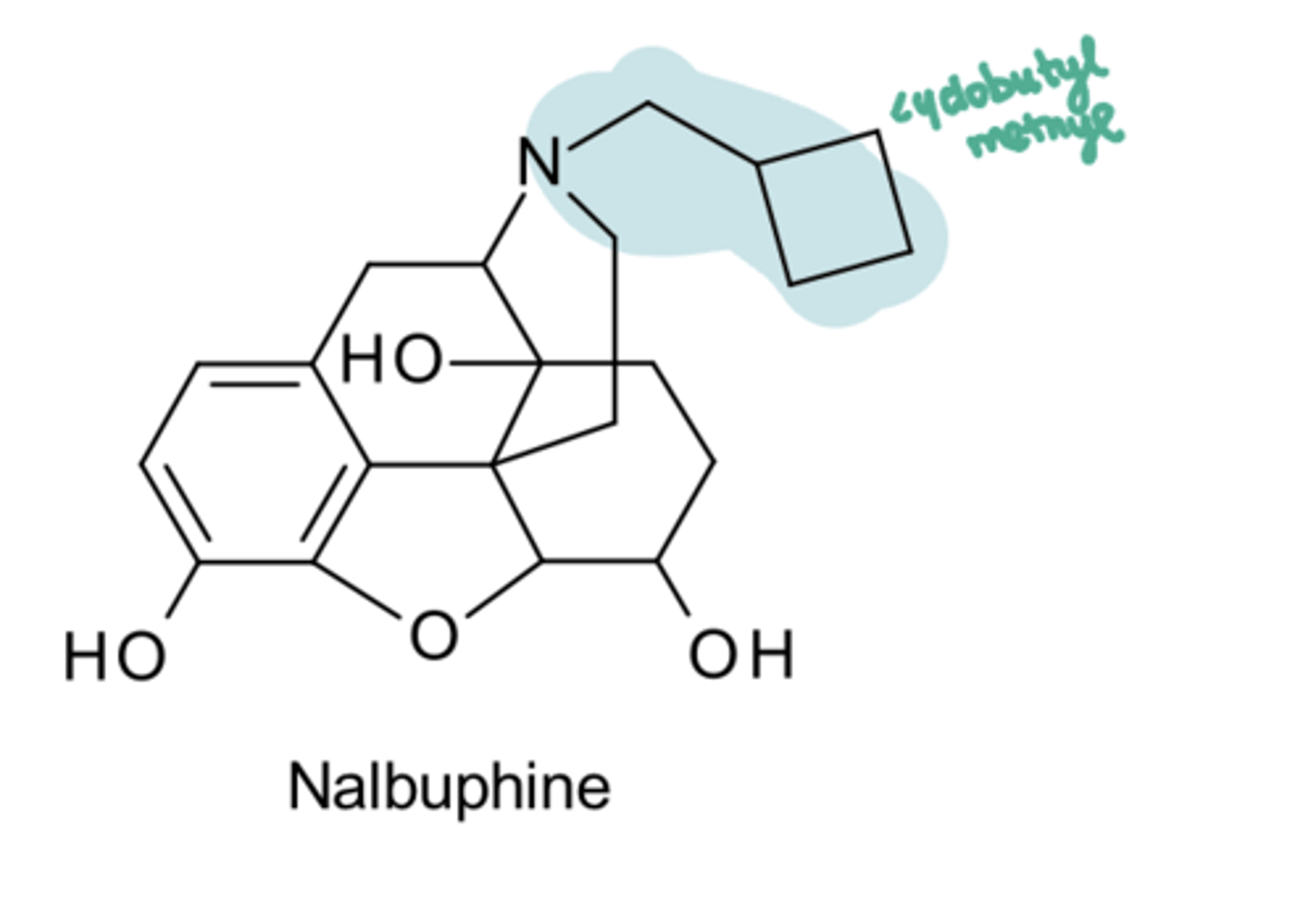
antagonist, agonist
Nalbuphine
-competitive μ ____
-κ _____ (resulting in analgesia)
withdrawal
In a patient who is dependent on pure agonists, switching to a mixed agonist/antagonist can produce ___ symptoms
equipotent, ceiling
Nalbuphine Advantages
-___ with morphine at the kappa receptor
-has a ___ effect for respiratory depression (meaning at a certain point, increasing dose will not increase respiratory depression)
addiction
Nalbuphine Advantages
-lower ___ potential
dysphoria
Nalbuphine Disadvantages
-____ due to kappa agonism
normorphine, codeine
Metabolism of Morphine
1. morphine → ___ (which is less active)
2. O-dealkylation of ____ → morphine
3. Morphine 3-O sulfate or glucuronate → morphine
4. Morphine 6-O glucuronate → morphine
reverses
Giving small doses of pure antagonist Naloxone IM or IV promptly ___ the effects of μ agonists (increases resp rate, reverses sedative effects, lowers BP if elevated)
1-4
Naloxone
-duration of effects is __-__ hours
dependence
We can use Naloxone to check for ___ (because will precipitate withdrawal syndrome)
not
Naloxone does ___ produce dependence
increase, exaggeration
Long-term Administration of Naloxone will:
-___ density of opioid receptors in brain and cause a temporary ___ of response to subsequent doses of agonists
metabolized
Naloxone
-is orally absorbed but completely ____ via glucuronide conjugation before reaching systemic circulation
spray, solution
Naloxone
-are orally absorbed but completely metabolized before reaching systemic circulation, so given in nasal ___ and ___ for injection
orally, longer
Naltrexone Advantages (over naloxone)
-___ active
-___ duration of action
agonist, antagonist
Buprenorphine is a UNIQUE mixed agonist/antagonist:
-partial ___ at μ receptor
-weak ____ at κ receptor
depression, dependence
Remember that stimulation of μ receptor produces:
-analgesia
-respiratory ___
-euphoria
-physical ___
antagonist
Buprenorphine is a partial μ agonist, at high doses, its analgesic effect plateaus and it behaves more like an ___
less
Due to the partial agonist activity, buprenorphine exhibits a ceiling to its pharmacological effects, thus, the danger of overdose, abuse liability, and toxicity may be ___ than with full opioid agonists
kappa
Patients with opioid or cocaine dependence have increased __ receptor sensitivity
euthymia
Patients with opioid or cocaine dependence have increased kappa receptor sensitivity, thus these patients are more likely to experience ____ (mental peace and tranquility) with buprenorphine vs patients receiving naltrexone
longer, lower
Buprenorphine
-dissociates very slowly from the μ receptor, providing a ___ duration of action than morphine, and a much ___ level of manifested physical dependence
abuse
Why do we add naloxone to buprenorphine (Suboxone)?
-because it acts as an ___-deterrent.
no
How is naloxone an abuse deterrent?
-Naloxone has very poor sublingual bioavailability. Therefore, in a SL formulation → naloxone produces ___ clinical effect.
counters
How is naloxone an abuse deterrent?
-When dissolved/injected → naloxone ___ the effects of buprenorphine (abuse deterrent!)
pure agonist
Levorphanol is a ___ ___
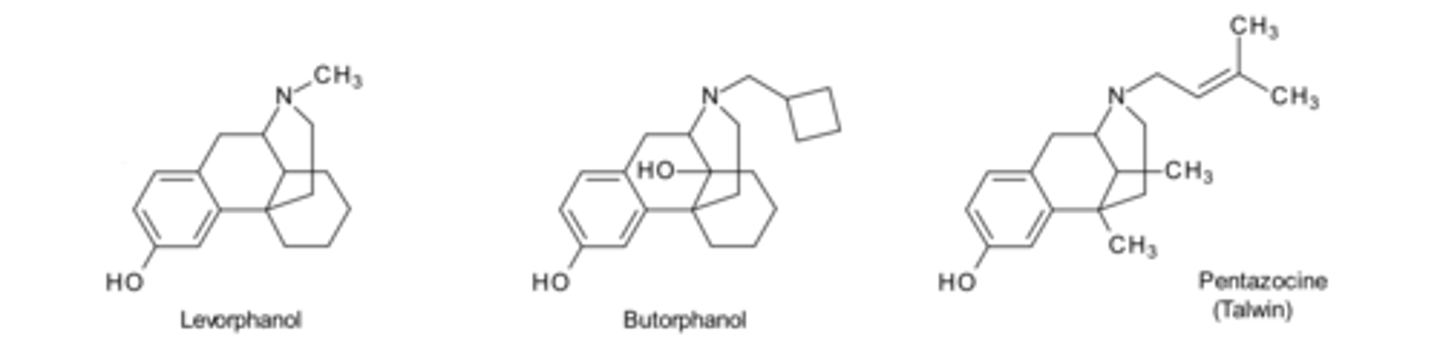
mixed, kappa
Butorphanol and Pentazocine are ___ agonist/antagonists. Activity comes from agonism at __ receptors. They also antagonize mu receptors
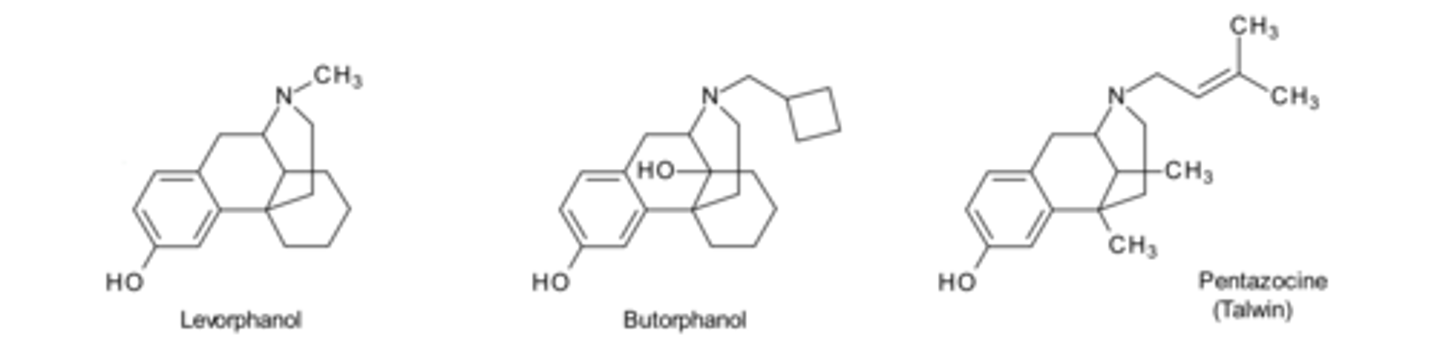
potent
Levorphanol and Butorphanol are more __ than morphine
abuse
Pentazocine
-is available as an oral tablet in combination with naloxone to prevent ___
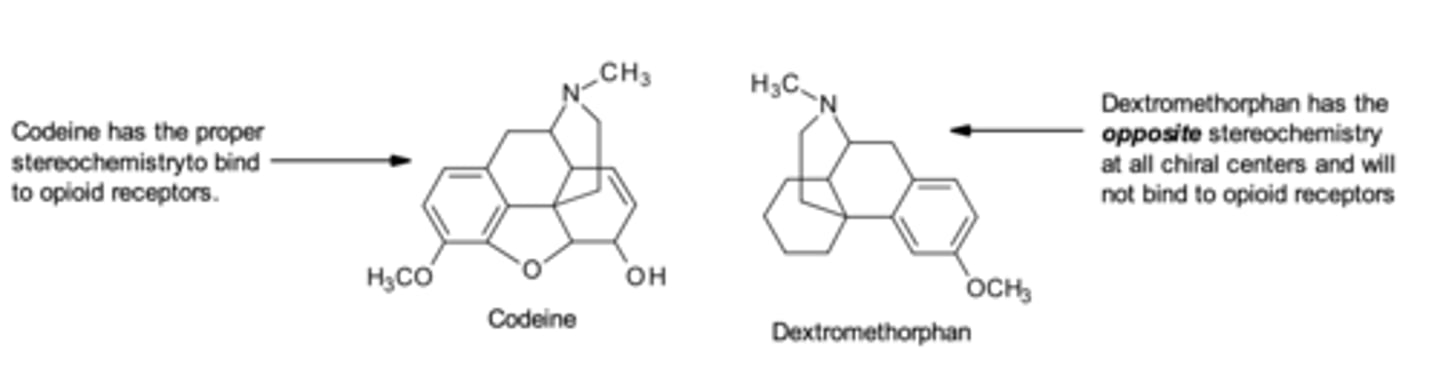
dextromethorphan
d isomer of Levorphanol = ____
coughing
Dextromethorphan
-no analgesia or addictive properties (because it is d-isomer, not l-isomer)
-does not act on opioid receptors, acts centrally to elevate the threshold for ___
4-phenylpiperidines
Meperidine, Fentanyl, and Sufentanil are __-___
mu, less
Meperidine
-predominantly a ___ agonist, exerts actions on CNS and GI tract
-___ potent than morphine
antidiarrheal
Meperidine
-the ___ agents (diphenoxylate and loperamide) are analogs of meperidine
slow
Diphenoxylate and loperamide
-act on peripheral μ-receptors in the GI tract and ____ GI transit. They may also inhibit fluid and electrolyte secretion.
atropine
Diphenoxylate is used with ____ to prevent abuse
euphoria, dependence
Why is Diphenoxylate used with atropine to prevent abuse?
-At higher doses, diphenoxylate (if given as a single drug) can cause ___ and ___. Atropine is added to prevent this
CNS
Why does Loperamide NOT need to be used with atropine to prevent abuse?
-Loperamide does not provide analgesia, euphoria, or dependence actions. This is because loperamide does not enter the ___ to any appreciable extent
more, rapid, short
Fentanyl
-a μ agonist that is 80-100x __ potent than morphine
-__ onset and __ duration of action
more
Sulfentanil
-10x ___ potent than fentanyl
racemic
Methadone
-marketed as its ___ mixture (but analgesic activity is primarily due to L-methadone)
-μ agonist
oral, extended, repeated
Methadone Advantages
-effective ___ analgesic
-___ duration of action
-demonstrates persistent effects with ___ administration
agonists, less
Tramadol and Tapentadol have 2 mechanisms of action:
mechanism 1: These two drugs are ___ at μ receptor; however, their affinity for the μ-receptor is __ than morphine
norepinephrine, serotonin, transmission
Tramadol and Tapentadol have 2 mechanisms of action:
mechanism 2: Inhibition of the reuptake of ___ and ___ in the CNS. This action inhibits pain ___ in the spinal cord
less
Tramadol
Advantage over morphine = ___ potential for abuse, dependence, or respiratory depression than other opioids
CYP3A4, CYP2D6
Tramadol requires ___ and ___ to be converted to its more active metabolite
decrease
Tramadol requires CYP3A4 and CYP2D6 to be converted to its more active metabolite. Inhibitors of either CYP3A4 or CYP2D6 would significantly ____ the analgesic action of tramadol but would not affect the actions of tapentadol.
no
If a patient overdosed on Tramadol or Tapentadol, could a pure opioid antagonist such as naloxone counter all of the actions of these agents?
reuptake
Why can't naloxone counter the effects of Tramadol/Tapentadol?
-Naloxone would only block the effects of these drugs at the μ-receptor. IT CANNOT block the actions that these two drugs have on the ___ of norepinephrine and serotonin in the CNS.
GPCRs
Opioid receptors are ____, traditional opioid agonists can bind to other targets and activate additional downstream pathways including those involving β-arrestin.
analgesia, side effects
Traditional Opiods activate 2 main pathways
G-protein pathway → ____
β-arrestin pathway → ___ ___
biased
Oliceridine is NOT a traditional opioid. It is a "____ agonist" at the μ-opioid receptor
selectivity
The term "biased" refers to the ligand-dependent ____ for certain signal transduction pathways relative to a reference ligand at the same receptor.
preferential, minimal
Oliceridine
-____ G-protein activation
-____ β-arrestin recruitment
fewer
Oliceridine
-preferential G-protein activation → analgesia
-minimal β-arrestin recruitment → so ___ side effects like constipation/respiratory depression :)