Applications of Psychology to Health
1/93
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
94 Terms
Who first defined stress + define it
Selye (1936) defined stress as the non-specific response of the body to any demand.
Characteristic of stress defined by Selye (1936)
—→ Demands can be psychological or physiological.
—→ To experience stress, a stressor must be present.
—→ Stress is experienced when a person recieves that the demands of the stressor exceed their ability to cope.
There are two types of stress:
Distress
Eustress
Distress vs Eustress Table:
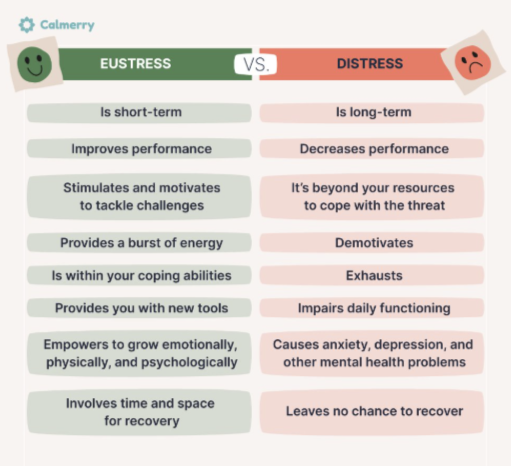
Distress
The negative psychological response to a stressor, as indicated by the presence of negative psychological states. (such as anger, fear or feelings of helplessness or hopelessness)
*considered a negative from of stress because it impedes ability to perform at an optimum level.
*Can lead to health risks.
E.g. Death of a loved one, financial difficulties, conflict, etc.
Eustress
The postive psychological response to a stressor as indicated by the presence of positive psychological states. (such as excitement, enthusiasm and optimism)
*Occurs when there is stress, yet a feeling of being capable to overcome.
*Increases alertness and energy levels, leading to optimum performance.
*Normally enjoyable and can motivate behaviour.
E.g. Exam, graduating, driving test, starting a new job, interviews, skydiving, rides, etc.
Adrenaline:
A hormone secreted from the adrenal glands that increases heart rate and supports the conversion of glycogen (stored form of energy) into glucose in the liver.
Noradrenaline:
A hormone secreted from the adrenal glands that causes blood vessels to constricts (becomes narrower) and blood pressure to increase.
Cortisol:
A steroid hormone secreted from the adrenal glands when the body experiences stress. (it increases pain tolerence)
Stressor
A stressor is any person, object or event that challenges or threatens an individual, thus causing feelings of stress.
*Stressors are sources of stress from internal or external factors
There are 4 types of stressors:
Environmental Stressor
Psychological Stressor
Social Stressor
Cultural Stressor
Environmental Stressor
Environmental stressors arise from the conditions and physical surroundings of an individual.
E.g. noise, temperature, smell, natural disasters, war, pollution.
Psychological Stressor
These stressors are caused by emotional and cognitive factors.
E.g. graduating, new job, buying a house, pressure at work, driving test, etc.
Social Stressor
Social stressors stem from relationships and interactions with society.
E.g. peer pressure and conflicts with family and friends.
Cultural Stressor
Stressors thta emerge from cultural identity, value and and cultural norms.
E.g. discrimination due to cultural beleifs/practices.
There are 3 characteristics of stressors:
Nature: Type of stressor (4 types)
Duration: Time frame: short-term (acute) or long-term (chronic)
Strength: The severity/intensity of the stressor
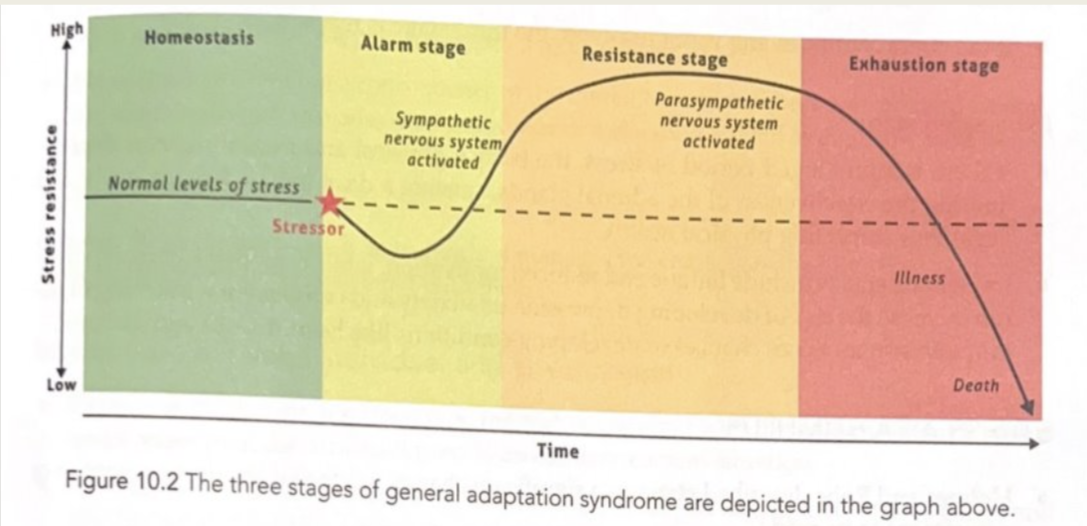
GAS model (Selye, 1936,1983)
The General Adaption Syndrome (GAS) 1983 model is used to describe the physiological changes that the body automatically goes through when it responds to stress.
When initially exposed to a stressor and experience stress, 2 physiological changes occur:
→ Heart rate increases
→ Breathing rate increases
The GAS model consists of 3 stages:
Alarm
Resistance
Exhaustion
Alarm
→ This is an initial response to a stressor (4 types)
→ The alarm stage has 2 sub-stages:
1. Shock: When we first perceive a threats, we go into a state of shock, the bodys resistance drops below normal. It responds as if it has been injured. → these physical effects of shock reduce the individuals ability to deal with the stressor (feeling helpless). After shock comes countershock.
2. Countershock: The sympathetic nervous system (SNS) activastes to prepare for “fight or flight”.
→The amygdala detects threat and signals the hypothalamus to initiate the SNS.
→ A signal is sent to the adrenal glands which triggers the release of adrenaline, nonadrenaline and cortisol.
*The first stage occurs 6-48 hours after initial stress is detected (counter-shock).
Resistance
→ If the stressor remains, the body enters a resistance stage as it attempts to restablises, its internal systems and fight the stressor.
→ The parasympathetic nervous system (PNS) begins to counter act the heightened arousal.
→ Stress hormones (adrenaline, noradrenaline, cortisol) continue to be secreted to help the body cope.
→ Energy is directed to managing the stress.
Exhaustion:
→ Occurs if the stressor continues for a prolonged period.
→ The bodys resources become depleted, leading to:
-Fatigue
-Low motivation
-Impaired immunity
-Increased risk of mental illness and physical illness.
→ The adrenal glands lose effectiveness, blood sugar drops and physical health declines.
GAS Model Diagram:
How did Holmes and Rahe (1967) describe stress?
Holmes and Rahe (1967) described stress as a significant change in life that requires a response or an adjustment to be made.
What did Holmes and Rahe create?
Holmes and Rahe created the Social Readjustment Scale (SRS) also known as Holmes and Rahe Stress Scale.
What is the SRS?
This scale assesses the amount of stress that has been experienced by an individual in the past year.
It is comprised of 43 life events and a score of 1 to 100 has been allocated to each event.
The score is called a life change unit (LCU). It estimates the amount of response and readjustment required if the event is experienced.
The individual receives a score based on their total stress readjustment (subjective).
Strengths of SRS:
→ Quantitative data is collected, easy to statistically analyse.
Limitations of SRS:
→ Responses rely on subjectively and honesty from participants.
→ No reasoning for responses/rich data. (common limitation in collecting quantitative data).
What did Lazarus and Folkman (1984) suggest?
They suggested that individuals urtalise their perception of a stressful situation and their their subjective past experiences to help them cope.
*stress responses are directed by our cognitive appraisal of the stressor as either a challenge or a threat and also by our assessment of the personal and social resources we have to cope with the stressor.
*Stress response depends on emotions and psychologicl factors that are unique to the individual.
Role of cognitive appraisal
-individuals make judgements on the environment event via cognitive appraisal - the cognitive abilities used to asses situations.
-Psychological stress comes from how a person thinks about and interprets a situation in their environment. Whether the situation feels stressful or not depends upon this cognitive appraisal (how they judge it).
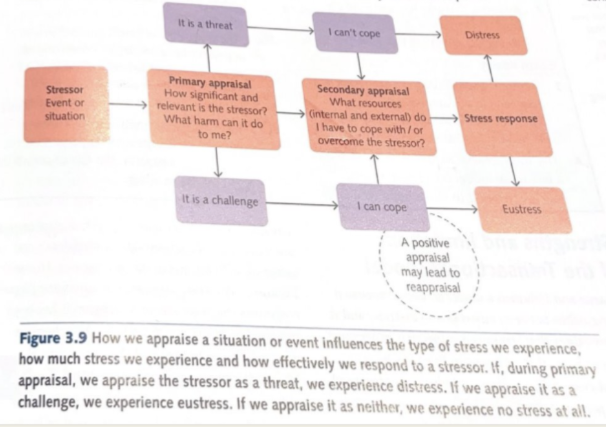
What are the two stages within the transactional model of stress?
Primary Appraisal
Secondary Appraisal
Primary Appraisal:
Primary appraisal involves an initial assessment of the situation to determine whether the situation is a potential threat, challenge or may cause harm.
(summary - Notice a stressor in the environment, decide if it’s irrelevant, a challenge or threat/loss risk.)
Primary appraisal involves two steps:
individual appraises the severity of the stressor:
-If the person appraises the stimulus as stressful, then the next step of primary appraisal occurs
To determine the way in which the stressor is stressful:
This involves evaluating whtehr the stressor is - harm/loss, threat or challenge.
Secondary Appraisal:
When an individual assesses whether they could cope with the stressor.
Assess both the internal and external resources that are available and evaluate whether they can meet the demands of the stressor.
*It occurs alongsde primary appraisal - lazarus and folkman explained hat the name ‘secondary’ does not infer it occurs after primary appraisal.
Stress as a transaction Diagram
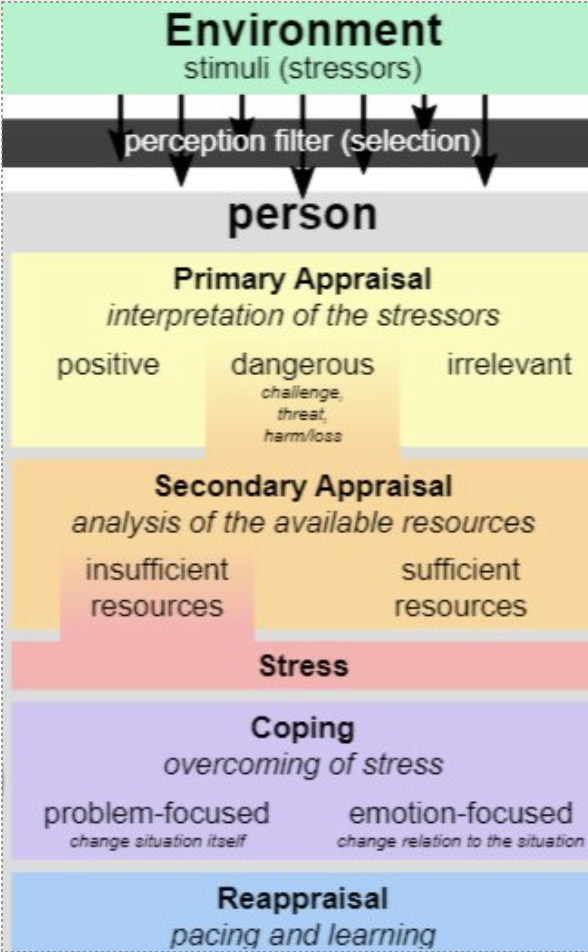
There are two methods of coping:
Emotion-Focused Coping
Problem-Focused Coping
Emotion-focused Coping:
The goal is to manage emotiona reactions to stress. This will be used when an individual perceives that they do not have the resources to deal with the stressor.
E.g. meditation, relaxation techniques, talk therapy, etc.
(Making ourselves feel better)
e.g. Year 12’s use make up at the end of the day for photo day.
Problem-Focused Coping:
The goal is to address the root cause of the stress. This will be used when an individual perceives that they do have the resources to deal with the stressor.
E.g. Pitch at work, quitting a job, etc.
(Addressing the issue by the root and removing it)
e.g. School photos - change it to Year 12’s in mornign and Year 7’s Last.
Stress as a Transaction Diagram - Lazarus and Folkman (1984):
There are two types of coping for stress:
Maladaptive Coping
Adaptive Coping
Maladaptive Coping:
Coping strategies that involve harmful and unhealthy stress management that exacerbates its adverse effects.
These strategies avoid dealing with the stressors that are causing problems.
Examples:
-Negative self talk
-Denial
-Substance abuse
-Withdrawing from society
-Rumination (repetitive thoughts)
-Self-blame
-Procrastination
Adaptive Coping:
Adaptive coping strategies are beneficial and productive methods for managing stress that can decrease the adverse impacts of stress.
Examples:
-Meditation
-Exercise
-Positive reframing
-Planning
-Acceptance
-Humour
-Emotional support by talking to others
What is the ‘Evolutionary Purpose of Sleep’?
A theory stating that sleep serves as a means to increase an animal’s or human’s chance of survival in its environment.
Early humans used the daytime rather than the nighttime to eat, drink and reproduce as there was greater risk of injury in the dark, as well as predators at night that could threaten their survival.
Sleep depends on an animal’s vulnerability to predators.
Sleep depends on the need to find food.
Sleeping at night allowed for energy to be conserved.
What is the ‘Restorative Purpose of sleep’?
A theory stating that sleep allows us to rechanrge our bodues, and recover from the physical and psychological work during the day; it also allows our body’s growth processes to occur.
Recuperation theories of sleep claim that homeostasis of the body (ability to balance internal physiological functioning) is disrupted when humans are awake and that sleep acts to restore it).
Sleeping allows the energy levels that decline during wakefullness to be restored:
-Repairs adn replenishes the body
-Increases alertness
-Increases immunity to disease
-Activates growth hormone
-Enhances mood
Summary comparison of Evolutionary Theory and Restorative Theory:
Theory of Sleep | Purpose | Function |
Evolutionary Theory |
|
|
Restoration Theory |
|
|
Functions of sleep:
Energy Conservation: less muscle tension, lower heart-rate, reduced metabolic activity.
Adaption: evolutionary perspective - what is the most beneficial sleep/wake cycle for humans versus otehr mammals.
Physical Restoration: build and restore materials, growth hormones are released during slow wave, sleep helps to ‘clean’ the brain out.
Memory Consolidation: REM and slow wave (deep) sleep are imortant for memory.
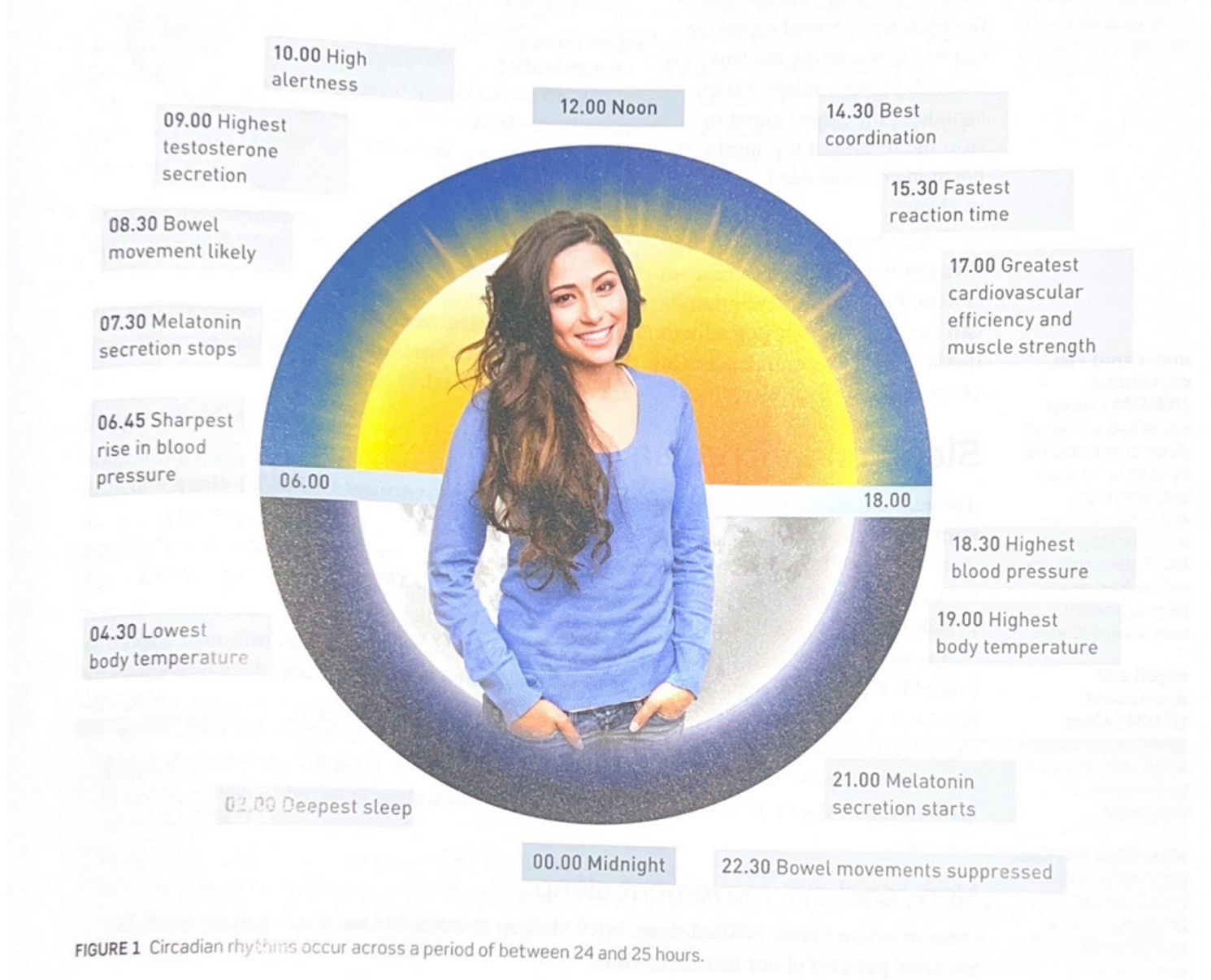
What is the Sleep-Wake Cycle?
The sleep-wake cycle is the reccuring pattern of wakefullness and sleep that individuals undergo on a daily basis.
The sleep-wake cycle is usually measured by recording the times of regular events like when we eat and go to sleep.
This cycle is regulated by the circadian rhythm and is regulated by body temperature, metabolic rate and the release of hormones including melatonin.
Our internal biological clock (or circadian clock) is found in the hypothalamus and is called suprachiasmatic nucleus (SCN).
Circadium Rhythum:
the biological cycle that lasts around 24 hours and controls the nocturnal release of hormones including melatonin.
Melatonin:
the hormone that regulates the sleep-wake cycle.
Sleep-Wake Cycle Diagram:
What does a night’s sleep consist of?
A night's sleep consists of four to six sleep cycles lasting approximately 90 minutes each, however the sleep cycles alter in length throughout the night as does the time spent within the different stages.
The sleep cycle is made up of four distinct stages, three non-REM and one REM stage. REM is an abbreviation for 'rapid eye movement', while NREM stands for 'non-rapid eye movement'.
There is evidence that NREM sleep (stage 3) is mostly involved with restoring the body and physical energy, while REM sleep is most important for restoring brain function such as memory and concentration.
Why is sleep important?
Sleep is important for general physical health, restoring energy, recovering from injuries or illness, growth, psychological wellbeing and mood, concentration, memory, work performance, getting along with others and the ability to regulate our emotions.
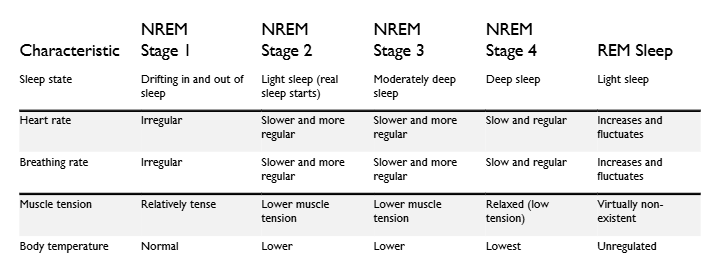
There are 4 stages of sleep:
Non-Rapid Eye Movement
Non-Rapid Eye Movement
Non-Rapid Eye Movement
Rapid Eye Movement
Non-Rapid Eye Movement
Characteristics:
Sleep state: transitional period between wakefulness and sleep
Heart rate decreases
Eye movements are a slow rolling movement (once asleep they stop moving)
Muscles relax
Length of Stage:
1-7 minutes
If uninterrupted, individuals quickly move into NREM 2 and minimal time is spent in this stage.
Non-Rapid Eye Movement
Characteristics:
Sleep state: light non-rem sleep
Heart rate slows down
Eye movement stops
Muscles continue to relax and there are occasional muscle twitches
Length of Stage:
10-25 minutes
The first time this stage occurs in the night it lasts 10-25 minutes, then increases in length with each repetition
Non-Rapid Eye Movement
Characteristics:
Sleep state: deep non-rem sleep
Heart rate continues to slow down
Minimal eye movement
Muscles are at their most relaxed state
Length of Stage:
20-40 minutes
Time spent in this stage is 20-40 minutes for the first few sleep cycles and then reduces in length
Rapid Eye Movement
Characteristics:
Sleep state: dreams occur during this stage
Heart rate increases to match the rate when awake (varies based on dream content)
Rapid eye movement, visual information is not transmitted to the brain
Muscles are temporarily paralysed (except for breathing and eye movement)
Involves a high level of brain activity
Length of Stage:
10-60 minutes
Stage increases in duration over the night ranging from a few minutes to one hour
4 stages table:
Sleep Stage | Characteristics | Length of Stage |
|
| 1-7 minutes
If uninterrupted, individuals quickly move into NREM 2 and minimal time is spent in this stage. |
|
| 10-25 minutes
The first time this stage occurs in the night it lasts 10-25 minutes, then increases in length with each repetition |
|
| 20-40 minutes
Time spent in this stage is 20-40 minutes for the first few sleep cycles and then reduces in length |
|
| 10-60 minutes |
summary table of sleep stages:
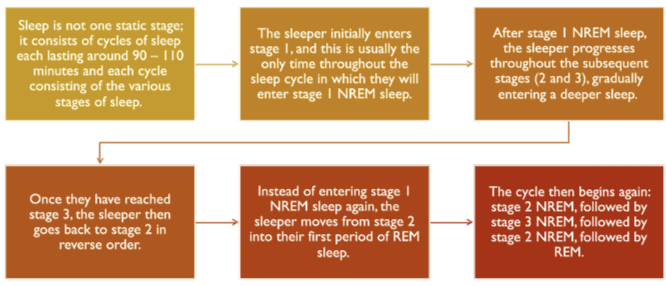
what is each night of sleep made up of
sleep cycles
How long do these sleep cycles last?
90-110 minutes
Sleep cycle in action
The sleeper enters Stage 1 NREM sleep, this usually only happens once per night.
After Stage 1, the sleeper then progresses through Stages 2 and 3, reaching deeper sleep. They then reverse back to Stage 2 befroe entering REM sleep.
E.g. NREM Stage 1 → Stage 2 → Stage 3 → Stage 2 → REM.
The first NREM → REM cycle lasts ~90 mins
In later cycles Stage 1 NREM is often skipped.
The sequence typically becomes: Stage 2 → Stage 3 → REM.
*These cycles can be visualised in a hypnogram.
From the third cycle onwards, Stage 2 NREM lasts longer, less time in Stage 3 NREM and more time in REM.
In the fourth, fifth and sometimes sixth cycle, Stage 3 NREM becomes rare and more time is spent in REM.
Sleep cycle Stages
Define Sleep Depravation
The condition of not getting sufficient sleep.
There are several causes of sleep deprivation:
-Shift work
-Drugs
-Sleep environment
-Stressors
Shift work:
Humans have hormones, such as melatonin, that help to regulate the sleep-wake cycle and circadian rhythum.
Shift-work involves altering the sleep-wake cycle and consequently reducing the amount and quality of sleep.
Trouble sleeping is caused by the disruption of hormones and lack of sleep cues.
Drugs:
Some drugs impact sleep stage progression/quality, reducing NREM sleep and affecting REM sleep.
Caffeine is a stimulant drug, it speeds up the CNS.
Alcohol is a depressant, it slows down the CNS.
Alcohol and caffeine both negatively impact sleep.
Sleep Environment:
A bright environment and/or loud environment can disrupt the sleep/wake cycle.
Stressors:
Stressors cause anxiety and anxiety can cause issues falling and staying asleep.
E.g. test/exam, headahce (illness), school, etc.
The types of Sleep Deprivation:
Partial/Acute Sleep Deprivation
Chronic Sleep Deprivation
Partial/Acute Sleep Deprivation:
The severe reduction or complete lack of sleep over a short-period of time.
Usually less than 5 hours over a 24 hour period
The effects are reversed once adequate sleep returns.
E.g. Studying, illness, all-nighter, jet-lag, stress, etc.
Chronic Sleep Deprivation:
The persistant reduction of sleep over a long period of time.
Spans from more than a few weeks to years.
The effects are harder to reverse, sometimes leading to negative health outcomes.
E.g. Sleep disorders, work-life balance, health conditions.
The effects of Partial Sleep Deprivation:
Attention: Lapses in attention increase when sleep deprived.
Mood: Decreases mood and increases irritability. Emotional processing is affected.
Reflex Speed: Reaction times increase, taking us longer to react to stimuli.
Vision: Vision can become blurry, eye twitches may occur and eyes become sensitive to light.
*Reversable once adequate sleep is acheived.
The effects of Chronic Sleep Deprivation:
Heart disease: Increases blood pressure and high cholestral which can lead to heart disease.
Obesity: Increases the intake of high-energy food as well as the overall amount of food intake.
Insomnia: Difficulties falling asleep and staying asleep (low sleep latency)
Anxiety: Emotional regulation is negatively impacted. This can increase anxiety.
*Cycle of anxiety → trouble sleeping → anxiety, etc.
*Typically hard to reverse.
Sleep Hygiene
The behaviour and sleep environment that result in a healthy sleep.
Zeitgebers:
Zeitgebers (German word for time givers) are cues in the environment that provide signals to our brains to do things at certain times.
E.g. Light is an example of a zeiteber = when out eues receive lower levels of light, such as when it is getting dark in the environment, the SCN signals to the pineal gland to release melatonin and this makes us feel drowsy and promotes the onset of sleep.
E.g. if you brush your teeth, put pyjamas on and read a book just prior to sleep every ight, this routine will be a signal to your brain that it is time for sleep.
There are three techniques to improve sleep hygeine:
Management of electronic devices
Consistent sleep patterns
Sleep environment
Management of electronic devices:
It is recommended that electronic devise use is ceased one hour prior to bedtime.
It emits blue light that prevents melatonin production and disrupts the circadium rhythum.
It results in brain stimulation that reduces both sleep quality and duration and increases sleep latency.
Consistent sleep patterns:
Critical for circadium rhythum to have a consistent bedtime routine and sleep hygiene.
Consistent bedtime and wake time helps the body clock, helps to prevent sleep deprivation.
Sleep environment:
Bed should be used for sleeping and intimacy only, this creates a cognitrive link between the bed and sleep.
*minimal, including electronic devices
Sleep latency = time taken to fall asleep
Who created the study that involves restricting bedtime mobile phone use?
He at el., 2020
Aim:
to determine how limiting the use of mobile phones before bedtime affects mood, working memory, pre-sleep arousal, sleep quality and sleep habits.
Participants:
38 university students who had the habit of using their mobile phone before bed as well as experiencing poor sleep quality.
Materials:
Positive and Negative Affect Schedule (PANSAS), n-back task, Pre-Sleep Arousal Scale (PSAS), Pittsburgh Sleep Quality Index (PSQI) and an online sleep diary.
Design:
IV: the use of mobile phones before bedtime versus no mobile phone use for 30 minutes before bedtime.
DV: Mood, working memory, pre-sleep arousal, sleep quality and sleep habits.
Procedure:
Researchers obtained approval from ethics comitee. Participants volunteered and singed online consent sheets.
Participants completed all tests to gain a baseline of results.
Participants were randomly assinged to either the experimental or the control group (19 in each)
Participants in the experimental group did not use their mobile phones for 30 minutes before bedtime. Participants in the control group continued with their normal mobile phone use.
At the four-week mark, participants completed the same tests and results were compared.
Key Findings:
Participants who did not use their mobile phone 30 minutes before bedtime were shown to take less time to fall asleep, stayed asleep for longer, had an improved quality of sleep, reduced pre-sleep arousal, improved positive affect, reduced negative affect and showed an improvement in their working memory.
Contributions:
Recent study that uses well established measures, allowing it to be replicated by other researchers.
With replication comes the ability to assess reliability.
Criticisms/Limitations:
The sample size was small, limiting the ability to generalise results to the population that the sample was taken from.
All measures, except for the n-back test, gathered subjective data from participants as they included self-report measures and online diary entries.
Subjective measures should ideally be used in combination with physiological measures as these collect objective data that is likely to be less biased.
What are the 5 measurement tools for measuring sleep?
Positive and Negative Affect Schedule (PANSAS)
n-BackTask
Pre-Sleep Arousal Scale (PSAS)
Pittrburgh Sleep Quality Index (PSQI)
Online Sleep Diary
Positive and Negative Affect Schedule (PANSAS):
Self-report measure
20 statements each requiring the completion of a 5-point Likert scale
Positive and negative emotions over the past week were assessed.
n-BackTask:
Working memory is tested
Computer program used where the participants are presented with a series of numbers and are required to respond when a specific number is presented, when two identical numbers are presented one after the other, and finally, when a number is identical to the one that appeared two numbers prior.
Pre-Sleep Arousal Scale (PSAS):
Self-report measure
5-point Likert scale for each of the 16 statements that pertain to cognitive and somatic arousal experienced when trying to fall asleep in bed.
Cognitive arousal refers to thoughts (e.g. worrying about falling asleep).
Somatic arousal refers to physiological symptoms (e.g. increased heart rate)
Pittrburgh Sleep Quality Index (PSQI):
Self-report measure
19 items that assess sleep quality and disturbances over the past month where a high score of 21, indicates poor sleep quality. A score of above 5 indicates sleep disturbances.
Online Sleep Diary:
Self-report measure
Daily record including bedtime, time taken to fall asleep, wake time, time arisen from bed, sleep duration, length of time mobile phone was used during the day and length of time mobile phone was used between 9pm and sleep time.