NPTE FF Nmeumonics and Study Strategies
1/337
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
338 Terms
Stages of Lymphedema (numbers) vs Grading of Edema (numbers)
Lymphedema 0-3 (lymph03dema)
Grading is from 1-4
Lymphedema vs Lipedema
Lymph: Unilateral or asymmetrical, cellulitis, not painful, distal edema, + Stemmer
Lip: Bilateral and symmetrical, cellulitis RARE, painful and bruise easily, absent stemmer
Anthopometric Measurements (Girth, Volumetric, Bioimpedance, Lymphoscintigraphy)
Girth→ Proximal areas
Volumetric→ Distal Areas
Bioimpedance→ Pre/post surgery
Lymphoscintigraphy→ Lymphatic Insufficiency
What is abnormal palpation of lymph nodes
tender, hard, and immobile
Indicative of malignancy!! → REFER TO PHYSICIAN
Lymphangitis vs Lymphadenitis vs Lymphadenopathy
Angitis → Vessels inflamed due to infection, present with red streaks, pain, fever
Adenitis→ Nodes inflamed, enlarged, painful due to infection
Adenopathy→ Enlargement of nodes, non tender and fixed = malignancy whereas tender = infection
What is the most efficient lymphedema PT management?
Exercise combined with external forces of compression
Complete Decongestive Therapy 2 Stages
Phase 1 → Intensive
Phase 2→ Maintenance
What all is involved in phase 1 of complete decongestive therapy?
MLD (Proximal to distal AREAS, distal to proximal STROKES)
Multiple layer compression bandaging
Skin and nail care
Exercise
What all is involved in phase 2 of complete decongestive therapy?
Self MLD
Compression therapy
Skin and nail care
Exercise
Contraindications to Manual Lymphatic Drainage (7)
Acute infection → don’t wanna spread it
Cardiac Failure → can create system overload
Renal Failure → can create system overload
Active Malignancy → May spread it
Uncontrolled Hypertension → System overload
Acute DVT → May spread it
Severe asthma → fluid could trigger bronchospasm
What bandage do we use for lymphedema and why?
Short stretch because it has low resting pressure and high working pressure → we WANT patient being active
more resistance = more muscle pumps fluid = more fluid return
Wrap distal to proximal with most pressure being distally
How should exercise choice be ordered lymphedema?
Proximal to distal to CLEAR THE TRAFFIC JAM
Imaging for UMN vs LMN
UMN → MRI and CT
LMN → EMG and nerve conduction velocity
Cardinal Signs for PD (TRAP)
PD →
Tremors (Intention)
Rigidity
Akinesia
Postural Instability (due to thoracic kyphosis)
Cogwheel vs Lead Pipe Rigidity
Cogwheel → Smooth and consistent
Lead Pipe → Ratchet like and jerky (rigid tremor)
Signs/Symptoms PD
Anosmia (Smell→ one of first symptoms)
Freezing gait
Dec arm swing
Inc steps per turn
Micrographia
Constipation (decreased movement of muscles)
Hypophonia
OH, Fatigue, Weakness
Flat Affect
Restrictive Lung Disease (due to dec ROM w dec movement and also due to posture)
Hoehn and Yahr PD Scale
1→ Unilateral
2→ Bilateral
3→ Balance impaired BUT INDEPENDENT
4→ standing and walking with AD, all symptoms present (walker has 4 legs)
5→ Confined to bed or WC
What will be seen during on/off phases of levidopa/carbidopa treatment?
On → dyskinesia (snake like, repetitive, large mm groups, involuntary)
Off → dystonia (prolonged contraction/spasms, a specific group)
schedule PT during ON PHASE
High protein diet can block effectiveness of medication
Signs/Symptoms of MS
UMN
Optic neuritis
Trigeminal Neuralgia
Cerebellar symptoms
Pseudobulbar affect
Unique Signs and Symptoms of MS (Ms Lucc Sin is 85)
Multiple Sclerosis
Lhermitte’s
Uthoff’s
Cranial Nerve 2 → Optic Neuritis → Marcus Gunn
Charcot’s Triad
Scanning speech
Intention Tremor
Nystagmus
85 degrees for water
Will also have trigeminal neuralgia
Types of MS
Relapse Remitting → Short attacks w full or partial recovery, may or may not leave deficits
Primary Progressive → Steady inc in disability without attacks
Secondary Progressive → Starts off as RR then turns into primary progressive
Progressive Relapsing (WORST) steady increased disability with attacks
ALS affects…
ALS leaves sensation intact
Attacks motor neurons
Is an upper and lower motor neuron condition
Signs/Symptoms of ALS..
UMN/LMN
Pseudobulbar affect (SAME AS MS)
Muscles → extensor weakness causes neck flexion
Respiratory mm weakness will lead to death
Signs and Symptoms of GBS
Distal to proximal LMN damage
Rapid and progressive
Glove and stocking pattern
Bilateral, symmetrical
CN 7, 9, 10, 11, 12 effected
Functions of Frontal Lobe
A CEO
Aphasia (Brocas)
Controls plans, programming, movement
Emotional, behavior, personality → executive function
Olfaction (Smell)
Functions of Temporal Lobe
Hearing and language comprehension
Wernicke’s Aphasia when affected
BEN has Broca
Broken speech
Expressive Aphasia
Non Fluent Aphasia
FRONTAL LOBE, ask yes/no questions
Wernicke’s Aphasia
Word Salad, Receptive Aphasia, Fluent Aphasia
TEMPORAL LOBE, gestures/demonstrations
Deficits seen L Parietal Lobe vs R Parietal Lobe
Left = Language
Right = Perceptual
Nmeumonic to remember cranial nerves and if they’re sensory/motor
Some- Oh - Olfactory (ONE nose)
Say- Oh- Optic (TWO eyes)
Marry- Oh- Oculomotor
Money- To- Trochlear (Cute shoes)
But- Touch- Trigeminal
My- And- Abducens (Lateral)
Brother- Feel- Facial
Says- Very- Vestibulocochlear
Big- Good- Glossopharyngeal
Brains- Velvet- Vagus
Matter- Ah- Accessory Spinal
More- Heaven- Hypoglossal
How to remember location of cranial nerves?
CE → 1,2
MI → 3,4
PONS → 5,6,7,8
MEDU → 9,10,11,12
Describe Pupillary Light Reflex, What CN involved?
When you shine a light into someones eyes, CN2 receives the info, integrates it and sends info to BILATERAL CN3 to constrict pupils (protect the eye)
BOTH should constrict if normally working
What will be seen if cranial nerve 3 is affected?
Strabismus (lateral deviation- CN3 can’t adduct so CN6 will laterally pull eye)
Ptosis
Pupillary Dilation
CN 5 and CN 7 functions, what reflex are they involved in
CN 5- SENSATION to face (5 feels) and anterior 2/3 of tongue, Jaw Jerk Reflex
CN 7- MOVEMENT of face and TASTE of anterior 2/3 of tongue, lacrimation and salivation
Both dampen sound
CN5 is afferent and CN7 is efferent to corneal reflex
Tests for Hearing loss
RINNE tells you type (sensorineural vs conductive)
WEBER tells you side
What is normal for Rinne test, what indicates sensorineural vs conduction
Normal AC > BC
Sensorineural AC > BC
Conduction BC > AC
How to determine which ear experiencing loss with Weber
CANS
Conductive → affected ear is heard louder
Sensorineural → Normal ear heard louder
What reflex are CN 9 and 10 involved in?
Gag
9 → afferent (posterior tongue sensation and taste)
10 → efferent (deviation of uvula)
CN 12 lesions seen as?
LICK YOUR LESION
Tongue deviates toward affected side
Muscles innervated by CN 11
SCM and traps
Characteristics of UMN
Spasticity, inc tone, inc reflexes, pathological reflexes, dec sensation, spasms, synergies
Characteristics of LMN
hypotonia, hyporeflexia or areflexia, dec sensation, fasiculations, weak or absent voluntary movement
Characteristics of Basal Ganglia involvement
Rigidity, resting tremors, brady or akinesia
Dec or normal tone, normal sensation
Characteristics of cerebellar involvement
hypotonia, dec or normal reflexes, normal sensation, ataxia, nystagmus, dec coordination, intention tremor
ACA CVA deficits
ABCD = Kid/Baby → “child-like” symptoms
Urinary incontinence, problems with imitation, problems with bimanual tasks, apraxia, slow/delayed motor, contralateral grasp reflex, sucking reflex
Affects contralateral LE
MCA CVA Deficits
MPH
Mouth
Perceptual Disorders
Homonymous Hemianopsia
Will affect contralateral UE/face
Unilateral Neglect…
More commonly as L sided (R Lesion)
Encourage awareness of and use of hemiparetic side
Active visual scanning
Homonymous Hemianopsia…
Will affect contralateral side
EX R lesion will affect L sides of visual field
R lesion will affect L temporal and R nasal
PCA CVA Deficits (Peripheral vs Central)
Peripheral → CL homonymous hemianopsia, visual agnosia, dyslexia WITHOUT agraphia, memory deficits, topographical disorientation
Central→ THALAMIC PAIN SYNDROME
Differences between R and L sided strokes
R→ Child Like
Perceptual issues, Impulsive, Quick, Safety Risk, Rigid thinking, very positive
L→ Elderly Like
Language deficits, slow and cautious, distractible, depressed
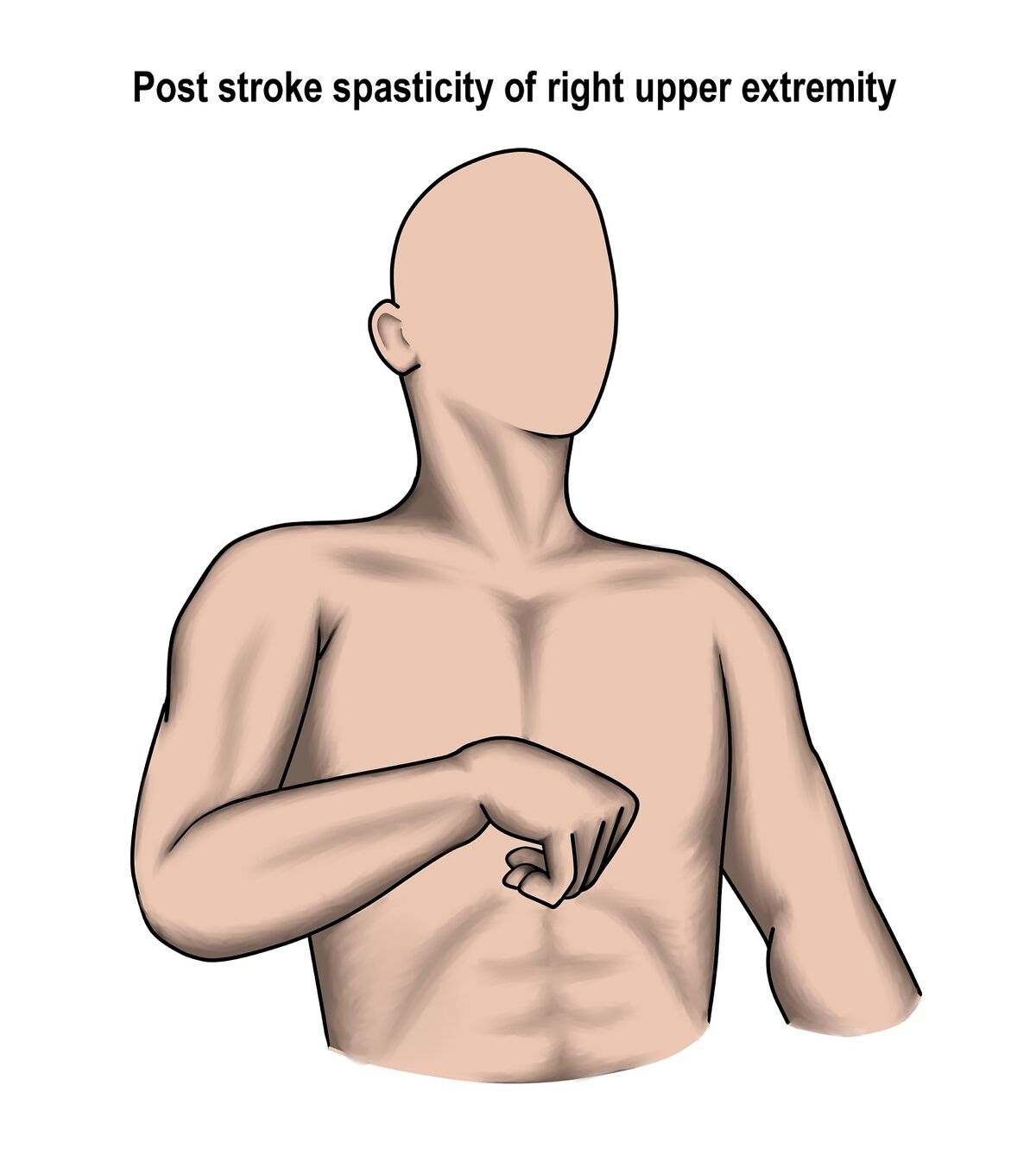
UE Spasticity Pattern
CHICKEN DANCE
Shoulder Retraction and downward rotation
Humeral adduction, IR, depression
Elbow and wrist flexion/adduction
Forearm Pronation
Hand/finger flexion, clenched/adducted thumb in palm
LE Spasticity Pattern
BALLERINA
Pelvic retraction
Hip adduction, IR, Extension
Knee extension
Plantarflexion, Inversion, Equinovarus, Toes Claw→ TMT ext, MTP flex
Toes Curl TMT and MTP flexion
UE Flexion Synergy
Johnny Bravo
Shoulder retraction/elevation
Shoulder abduction and ER
Elbow flexion
Wrist and finger flexion
LE Flexion Synergy
Sitting with leg crossed over the other
Hip flexion, abduction, ER
Knee flexion
Ankle DF and inversion, toe DF
UE Extension Synergy
Scap protraction
Shoulder adduction/IR
Elbow extension
Forearm pronation, wrist and finger flexion
LE Extension Synergy
BALLERINA
Hip extension, adduction, IR
Knee extension
Ankle PF and inversion
Toe PF
Brunnstrom Stages of Stroke Recovery
Stage 1: Flacid
Stage 2: Beginning of minimal voluntary mvmt, synergy and tone
Stage 3: PEAK Spasticity and Synergies
Stage 4: Movement outside of synergy, tone starting to decrease
Stage 5: Inc complex movements
Stage 6: Individual Joint movement, coordinated movement
Stage 7: Normal movement
Stages 1-3 RLA
1→ COMA, NO response
2→ Generalized response, non purposeful whole body movement, inconsistent
3→ Local Response, purposeful and local, specific, inconsistent (FOLLOW SIMPLE COMMANDS, CLOSE EYES)
Stages 4-6 RLA
4→ Confused Agitated (DOES NOT COOPERATE) no selective attention, no memory
5→ Confused Inappropriate (will begin to be able to socialize S=5) consistently respond to simple commands
6→ Confused Appropriate (Goal oriented behavior develops G=6) more carryover of skills
Stages 7-8 RLA
7→ Automatic Appropriate
8→ Purposeful Appropriate (judgement is impaired in emergency or stressful situations)
7,8 ready to graduate! → Work on home, school, community reintegration
How do vitals change with incremental exercise?
Heart rate and cardiac output increase linearly
BP
MAP increases linearly
SBP increases
DBP SHOULD REMAIN FAIRLY CONSTANT
What are the BP guidelines?
Normal→ less than 120/80
Elevated→ 120-129 AND less than 80
Stage 1→ 130-139 or diastolic 80-89
Stage 2→ 140 or 90
HYPERTENSIVE CRISIS→ 180 and/or over 120
PPP Pronation of PRUJ
Pronation
PRUJ
Posterior Glide
Opposite for supination, Supination = Anterior Glide
Changes that INITIALLY occur with altitude changes
HR inc
BP inc
CO inc
SV no change
Changes that occur with altitude acclimation
HR inc (ex you still get excited to see your significant other even after years)
BP and CO normalize
SV decreases
Buoyancy affect on WB at C7, Xiphoid, and ASIS
C7= 10%
Xiphoid= 33%
ASIS= 50%
Decreased swelling and improved circulation due to hydrostatic pressure exerted by water
Aquatic therapy effect on vitals
@ beach, heart is happy
HR, BP, and VO2 decrease
CO and SV have to increase to makeup for HR dec
Trick to remember RPE levels
RPE= 6=20
SHVEM (13 somewhat hard, 15 hard, 17 very hard, 19 extremely hard, 20 max exercion)
and reverse for light
Auscultation Sounds Heart
R 2 ICS→ Aortic
L 2 ICS → Pulmonic
L 3 ICS → Erb
L 4 ICS → Tricuspid (sternal border)
L 5 ICS → Mitral (midclavicular line)
Lub = What closing
“Primary” valves closing→ mitral and tricuspid
Dub = What closing
“Secondary” valves closing → pulmonary and aortic
S3 and S4 associated with…
S3→ Ventricular gallop, heart failure
S4→ Atrial gallop, atrial contraction
Tight and weak muscles→ UPPER CROSSED SYNDROME
Tight muscles PUTS on stress
Pecs
Upper traps
Top corner of scap- Levator Scap
SCM
Weak Drink Mango Lassi
DNF
Mid Trap
Low Trap
Serratus
TOLL for Screw Home Mechanism
Tibia Open Chain- Lateral for locking (extension)
(closed chain→ femur has to move has → will do the opposite (ex: extension femur will medially move)
Shoulder UR and DR
UR→ serratus, upper and lower traps
DR→ levator, rhomboids, pecs
Thumb flexion/extension R/G
Same R/G
Flexion→ radial Adduction → ulnar glide
Extension → radial Abduction → radial glide
Thumb abd/add R/G
Opposite R+G
Abduction → volar roll, dorsal glide
Adduction → dorsal roll, volar glide
SC joint roll and glides
Elevation/Depression→ opposite R + G
Protraction/Retraction → same R+G
TMJ Arthrokinematics
Elevation= Closing = rolls anterior and slides posterior
Depression= Opening = rolls posterior and slides anterior (EARLY PHASE)
Condyle and disc slide together in forward and inferior direction
Protrusion = Mandibular condyle and disc translate anteriorly
Retrusion = Mandibular condyle and disc translate posteriorly
Lateral Excursion = Ipsilateral pivot point and contralateral rotates anteriorly and medially
Anatomical Directions for OKC and CKC Pronation and Supination
OKC
Pronation EDAB
Supination IPAD
CKC
Pronation EPAD
Supination IDAB
Supine ALPS test for SIJ
When in supine
Anterior Longer Posterior Shorter
If the leg is long it is anteriorly rotated, if the leg is short it is posteriorly rotated
Difference in lung volume changes restrictive vs obstructive
Everything decreases except OLD FART
o- obstructive
F- FRC (RESIDUAL- CANNOT GET AIR OUT)
a
R- RV (RESIDUAL- CANNOT GET AIR OUT)
T- TLC (air not getting out, total capacity increases)
T- TV
Ways to remember Gold’s Classification for COPD Diagnosis
FEV1/FVC fraction will always be less than 70% with any level of COPD
Mild - 80%
Moderate- 50-80%
Severe- 30-50%
Very Severe- <30%
Huffing is used mainly for what condition?
COPD- allows glottis to remain open to allow for secretions to expel
How to remember pitch and intensity of each lung sound
Closer to neck → higher pitch and intensity
Further down in lungs → softer and lower pitch
Tracheal: High pitch and intensity
Bronchial: Loud intensity and high pitch
Bronchovesicular: Intermediate pitch and intensity
Vesicular: Soft intensity and low pitch
Duration of lung sounds (exp vs insp)
Bronchovesicular and tracheal→ same duration
Vesicular→ Longer inspiratory (takes LONGER for air to get to bottom of lung)
Bronchial→ Longer expiratory (closer to mouth, expiratory sounds “take over”)
Descriptions of ABnormal lung sounds
Rhonchi→ snoring (low pitch, continuous)
COPD, pneumonia, cystic fibrosis, bronchiectasis, chronic bronchitis
Wheeze→ whistle (high pitch)
Asthma, COPD
Crackles (Rales)→ high pitched, not continuous POPPING
Pleural Rub→ Rubbing 2 papers together, heard in lateral lower chest
Which abnormal lung sound is indicative of cardiac condition? What heart sound is heard with CHF
Crackles (C= Cardiac = Crackles)
S3 Heart sound indicative of CHF (CHF= 3 Letters = S3 sound)
What are voice sounds with lung auscultation?
ABNORMAL, indicative of secretions which create consolidation in lungs
Bronchophony (99)
Egophony (E sounds like A)
Whispered Pectoriloquy (increased loudness of whispering)
Erb vs Klumpke’s Palsy
ERB (5r6) → C5-6 affected
head stretches downward
loss of abduction and ER (waiter tip deformity)
Klumpke (81umpke) → C8-T1
stretching of arm OH
paralysis of hand intrinsics
claw hand
Scheuermann Disease
SH SH SH
Schmorl nodes, scheuermann, schroth (treatment)
An extension bias condition, will have inc thoracic kyphosis and lumbar lordosis
Pain w extension and rotation
Need to stretch pecs, strengthen thoracic extensors and scapular stabilizers
Key Points about Pediatric Outcome Measures
PEDI → will mention caregiver assistance and social function
WeeFIM → adaptation of FIM, includes cognition
Both span 6 months to 7 years
GMFCS
1- Walk without restrictions, limitation in advance gross motor
2- Walk without AD, with limitations walking within community
3- AD> WC limitations walking outdoors and in community
4- WC > AD self mobility severely limited, transported outdoors or use power WC
5- Patient self mobility severely limited, even with AD requires caregiver
Plagiocephaly and Torticollis
Occur on opposite sides
L torticollis will be R plagiocephaly
Torticollis is named after SCM affected
Plagiocephaly named after flat side (occipital bossing will be contralateral side)
Reflex Integration
1-2 Mon: Flex, extend, flexor withdrawal, crossed extension
3: Rooting reflex (^3^) → lips look like a 3, rooting integrates at 3 months
2-5: traction (cervical traction max is 25lbs)
6: PAMS TP
Plantar grasp
ATNR
Moro
Sucking
TLR
Positive Support
9: Plantar (need WB to integrate)
12: Babinski and STNR
When do grasps develop?
Pincer → 3 Jaw Chuck → Fine Pincer/Precision
10-15 months
Developmental Milestones Poem
3 I lift my head (POE, Cervical Extension)
4 Lay on my side (Supine → SL)
5 Prone to supine (babies hate tummy time, will try to get out of it, sup → prone develops right after at 6-7)
6 I sit upright (ring sit, supported, UE)
7 quadruped
At 8 i cant wait to cruise (9)
Creep, cruise, and stand alone at 9
Then walk (12) and stack 2 cubes (10-15, need control of release)
APGAR stands for, how is it graded, what are norms
Appearance (blue, blue extremities, pink)
Pulse (absent, <100, 100-140)
Grimace (no response, grimace, flexor withdrawl or cry)
Activity (flaccid, some flexion, active movement of extremities)
Respiration (absent, weak cry, strong cry)
Normal is 8-10
Check at 1 min, 5 min, 10 min only if needed
Compensation in gait for LLD with stance phase
Long limb will DF in late stance to try to even out
Short limb will PF in stance to try to reach ground
Mechanical Traction Contraindications
H-P-H
Uncontrolled hypertension
Immobilization
Peripheralization of symptoms
Acute Injury or Inflammation
Joint hypermobility or instability