Medicine: Physical examination of the cranial nerves
1/43
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
44 Terms
describe CN I exam
ask patient if they have had any decrease in ability to smell
ask patient to close eyes and pinch 1 nostril shut and put a familiar scent (coffee, cinnamon, etc.) underneath nose and ask to identify
repeat for opposite nostril with different scent
positive test for CN I exam
inability to identify scent
what is CN I?
olfactory nerve
what is CN II?
optic nerve
sensory for vision receives sensory stimuli to the _______
retina
there are several different exams that can be done to test CN II. what are they?
pupillary constriction
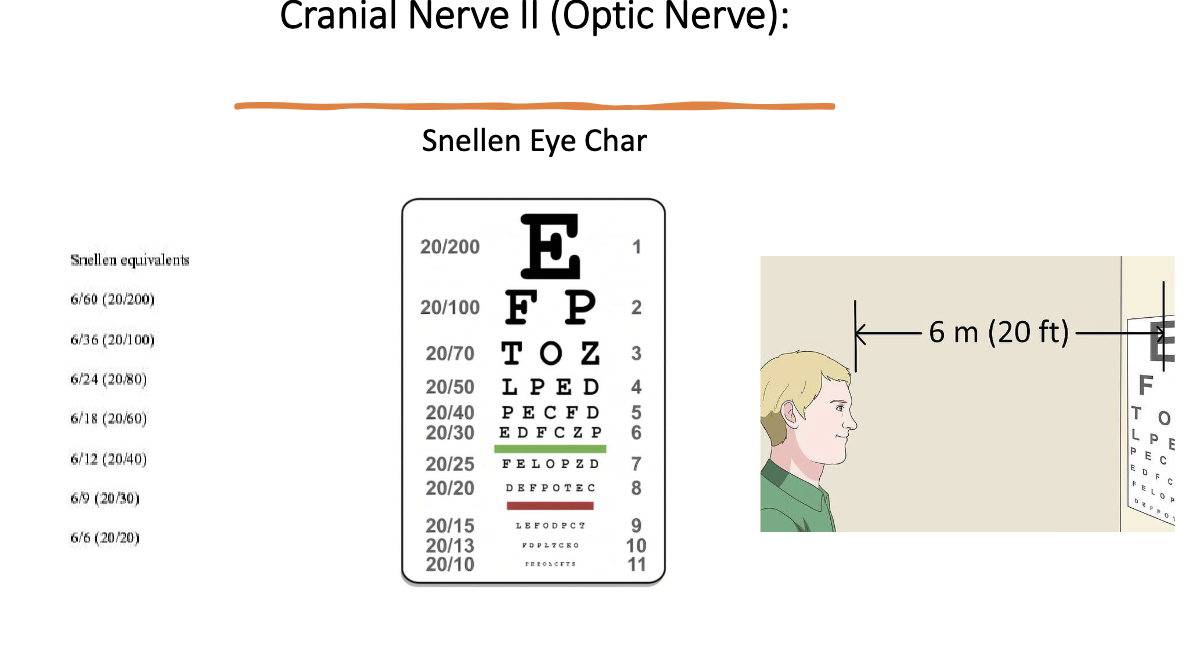
Snellen Eye Chart
visual field test for peripheral vision
describe CN II exam for pupillary constriction
shine a light in patient’s eye while blocking other eye and observe for pupil constriction on same side
repeat same pupil for accommodation reflex (pupil constriction on opposite side)
what’s a positive CN II exam for pupillary constriction?
loss of pupil constriction bilaterally
describe CN II exam using Snellen Eye Chart
patient stand 20 ft from eye chart and read smallest line they can read easily
progress down chart until they reach a line where at least 2 errors are made
compare number on that line with the 20 ft where they stand
20/30 = stood 20 fee but could only read a line that a normal eye can read from 30 ft
describe CN II exam for visual field (peripheral vision)
use hand to see where patient can begin seeing in all fields

what is CN III? what does it innervate?
occulomotor
rest of intrinsice muscles that move eyeball in directions (excluding superior oblique and lateral rectus)
what is CN IV? what does it innervate?
trochlear
superior oblique muscle (move eyeball infero-medially)
what is CN VI? what does it innervate?
abducens
lateral rectus m. (moves eyeball laterally)
which CNs are responsible for motor to eyeball movement?
CN III, IV, VI
describe CN III, IV, and VI exam
ask patient to watch tip of finger with eyes only while u trace an H-pattern in the air
what is a positive exam for CN III, IV, or VI?
inability to move eyeball in respective directions (ipsilateral lesion)
what is CN V? what does it innervate?
trigeminal n.
sensory to face
motor to muscles of mastication
describe sensory CN V exam. positive result?
ask patient to close eyes and distinguish between sharp and soft touch on maxilla and mandible
positive = inability to distinguish or feel
right/left side of forehead → opthalmic branch
right/left side of cheek area → maxillary branch
right/left side of jaw → mandibular branch
describe motor CN V exam. positive result?
put fingers on bilateral temporalis muscles and ask patient to bite down. put fingers on bilateral masseter muscles and ask patient to move jaw side to side.
positive = unequal tension bilaterally in muscles
sensory limb of CN V has how many major branches?
3 (each covers 1/3 of face)
opthalmic
maxillary
mandibular
The Ophthalmic branch of CN 5 also receives sensory input from the surface of the eye. To assess this component:
• Pull out a wisp of cotton.
• While the patient is looking straight ahead, gently brush the wisp against the lateral aspect of the sclera (outer white area of the eye ball).
• This should cause the patient to blink. Blinking also requires that CN 7 function normally, as it controls eye lid closure.
what is CN VII? what does it innervate?
facial n.
sensory to cornea + taste
motor to muscles of facial expression
describe sensory CN VII exam. what’s a positive result?
ask patient to open eye, touch cornea w cotton wisp for corneal reflex
positive = not blinking in response (patients who wear contacts may have lost this reflex)
too much overlap of CNs to use taste as assessment technique
describe motor CN VII exam. what’s a positive result?
ask patient to frown, smile → both corners should rise to same height and equal amounts of teeth visible
puff out cheeks (both sides should puff equally, no air leakage from mouth)
wrinkle eyebrows and close eyes tightly
VII = close lids
III = open lids
positive = inability/asymmetrical facial expression
what is CN VIII? what does it innervate?
vestibulocochlear n.
sensory for hearing
motor for balance
describe exams for CN VIII.
hearing → whisper something while occluding opposite ear
Weber and Rinne test (conductive vs snsorineural hearing loss)
t/f: Any suspected loss should prompt formal audiologic testing to confirm findings and help differentiate conductive hearing loss from sensorineural hearing loss.
true
describe the Weber test.
CN VIII lateralization
wrap tuning fork strongly on palm and press butt of instrument on top of head in midline and ask where they hear the sound
should be heard in center/equally in both ears
conductive hearing loss = vibration louder on side with hearing loss
no vibration heard at all, attempt again and press butt harder on head
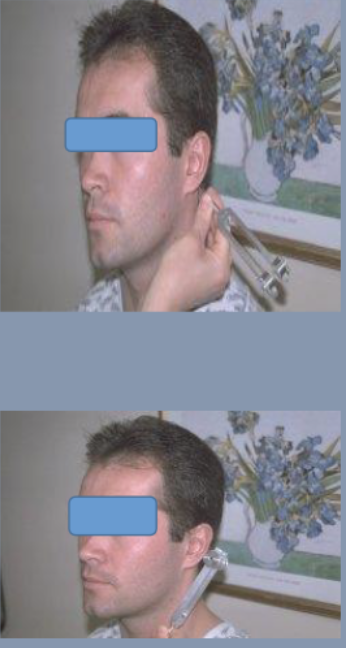
describe the Rinne test.
compares air conduction to bone conduction
wrap tuning fork firmly on palm and place butt on mastoid eminence firmly
ask patient to say “now” when they can no longer hear the vibration
when patient says “now”, remove butt from mastoid process and place U of tuning fork near the ear without touching it
The vestibular division of CN VIII detects changes in the position of the head relative to gravity: our sense of _________
balance and equilibrium
Vestibular function can be evaluated by testing for _______-
nystagmus. ... If patients have acute vertigo during the examination, nystagmus is usually apparent during inspection.
what is CN IX? what does it innervate?
glossopharyngeal n.
motor to muscles of pharynx and larynx
sensory to taste
the motor portion of gag reflex is due to CN ___. describe the exam.
CN IX
touch back of patient’s throat w tongue depressor (not gagging is positive)
what is CN X? what does it innervate?
vagus n.
sensory to taste
motor to soft palate and vocal cords (observe for hoarseness of voice)
describe CN X exam.
observe for hoarseness of voice
shine light in mouth and ask patient to say Ahhhh
check to see if uvula is deviated to one side
uvula will deviate away from side of CN X lesion
which nerves are responsible for raising the soft palate of the mouth and the gag reflex, a protective mechanism which prevents food or liquid from traveling into the lungs. As both CNs contribute to these functions, they are tested together.
CN IX and X
testing elevation of the soft palate is used for CN IX and X. describe the steps.
ask patient to open mouth and say AHhhh (soft palate will rise upward)
look for uvula (use tongue depressor if necessary)
uvula should rise up straight and in the midline
left CN IX dysfunction will result in what clinical presentation?
uvula pulled over towards right (often in post-stroke patients but other processes can cause deviation as well like peritonsilar abscess)

describe steps for testing gag reflex
ask patient to widely open mouth
identify posterior pharynx (use tongue depressor if necessary)
take tongue depressor or cotton tipped applicator and gently brush it against posterior pharynx or uvula and observe for gag
small percent of normal population has minimal or non-existent gag reflex
what is CN XI? what does it innervate?
accessory spinal n.
trapezius m. (permit shrugging of shoulders) and SCM m. (turn head laterally)
describe CN XI exam. positive result?
place hands on top of either shoulder and cheek and ask patient to shrug and turn head into hand (repeat on other side) while u provide resistance
positive = weakness/absence of movement on affected side
what is CN XII? what does it innervate?
hypoglossal n.
motor to tongue muscles (each CN XII innervates ½ of tongue)
describe CN XII exam.
ask patient to stick tongue straight out of mouth
look for deviation to one side/weakness and direct them to push tip of tongue into either cheek while u provide counter pressure from outside
tongue will deviate toward side of CN XII lesion
if the right CN XII is dysfunctional, the tongue will deviate to the right/left.
right
because the normally functioning left half will dominate as it no longer has opposition from the right. Similarly, the tongue would have limited or absent ability to resist against pressure applied from outside the left cheek